Abstract
Veno-venous extracorporeal membrane oxygenation (vvECMO) is a life-saving intervention for severe respiratory failure unresponsive to conventional therapies. However, managing refractory hypoxemia in morbidly obese patients poses significant challenges due to the unique physiological characteristics of this population, including hyperdynamic circulation, elevated cardiac output, and increased oxygen consumption. These factors can limit the effectiveness of vvECMO by diluting arterial oxygen content and complicating oxygen delivery. Refractory hypoxemia in obese patients supported by vvECMO often stems from an imbalance between ECMO blood flow and cardiac output. Hyperdynamic circulation exacerbates the recirculation of oxygenated blood and impairs the efficiency of oxygen transfer. To address these challenges, a stepwise, individualized approach is essential. Strategies to reduce oxygen consumption include deep sedation, neuromuscular blockade, and temperature control. Cardiac output modulation can be achieved through beta-blockers and cautious therapeutic hypothermia. Optimizing oxygen delivery involves improving residual lung function; high positive end-expiratory pressure ventilation guided by esophageal pressure monitoring; prone positioning; and adjustments to the ECMO circuit, such as using dual oxygenators, larger membranes, or additional drainage cannulas. This review highlights the interplay of physiological adaptations and technical innovations required to overcome the challenges of managing refractory hypoxemia in obese patients during vvECMO. By addressing the complexities of high cardiac output and obesity, clinicians can enhance the effectiveness of vvECMO and improve outcomes for this high-risk population.
1. Introduction
Veno-venous extracorporeal membrane oxygenation (vvECMO) has emerged as a life-saving intervention for patients with acute respiratory distress syndrome (ARDS) [1] with severe respiratory failure who are unresponsive to conventional therapies. Emerging data (EOLIA [2] and CESAR [3] trial) and the COVID-19 pandemic are changing mentalities toward vvECMO use in ARDS. As obesity prevalence has risen in the general population over the past decades, including among critically ill patients—now accounting for up to 20% of intensive care unit (ICU) cases [4]—ICU physicians considering ECMO should enhance their understanding of the specific challenges and considerations associated with this technique in obese and super-obese patients. Current guidelines recommend that clinicians consider vvECMO cannulation when EOLIA criteria are met [5]. Table 1 summarize the EOLIA criteria for ECMO initiation and the classical contraincations.

Table 1.
EOLIA criteria for ECMO initiation [2] and classical contraindications of vvECMO [5].
Although obesity is associated with an overall increased risk of morbidity and mortality in the general population, critically ill obese and super-obese patients (body mass index [BMI] > 40 kg/m2) are not showing increases in mortality during ICU stay [6] but might be associated with longer ICU stay and longer duration of mechanical ventilation [6,7] among survivors. These contradictory findings have been referred to as “the obesity paradox” [4,8]. Similar findings for ARDS obese patients [9] underscore the resilience of this population in severe respiratory failure. Concerns regarding the use of ECMO in obese patients include difficult vascular access for percutaneous cannulation technique, high cardiac output and blood volume, and an increased risk of cannula-related infections. However, despite these concerns, recent studies have shown that—consistent with previous data—obesity in patients on vv-ECMO may be associated with an increased survival rate [10,11]. Nonetheless, in the EOLIA study, patients with a BMI greater than 45 kg/m2 were excluded [2]. Despite the small sample size (12 patients) in their study, Swol et al. [12] further demonstrated the feasibility of using vv-ECMO in obese and super-obese patients. Their study included surgical patients with hypercapnic respiratory failure associated with a mean BMI of 47.9 kg/m2, with the highest BMI reaching 88 kg/m2. They also confirmed the feasibility of percutaneous cannulation and reported a 50% survival rate, which was comparable to the outcomes in the EOLIA and CESAR trials. Consequently, the use of vvECMO in that population can no longer be viewed as a contraindication or predictor of poor outcomes and may even be strongly considered. Nevertheless, in this particular population, the application of vvECMO requires particular management and technical nuances [9,13].
In obese patient, ARDS is frequently characterized by elevated cardiac output (CO) [14], elevated total blood volume [15], increased oxygen consumption [16], and impaired pulmonary mechanic resulting in high rates of atelectasis [17]. All of these factors can contribute to the development of refractory hypoxemia during vvECMO support. The hyperdynamic circulation and elevated blood volume necessary in obese patients in response both to the need to perfuse the additional mass and to increase baseline oxygen consumption dilutes arterial oxygen content, creating a scenario where even maximal ECMO flow may fail to meet metabolic demand [16].
This review explores the physiological rationale, clinical strategies, and technical innovations involved in optimizing vvECMO for morbidly obese patients. As a practical reference, a flowchart summarizing the clinical strategies and providing a stepwise management approach is included to guide the implementation of these techniques in clinical practice (Figure 1). By understanding the interplay of these factors, clinicians can better navigate the challenges of managing refractory hypoxemia in this high-risk population and ensure that the promise of vvECMO is fully realized.
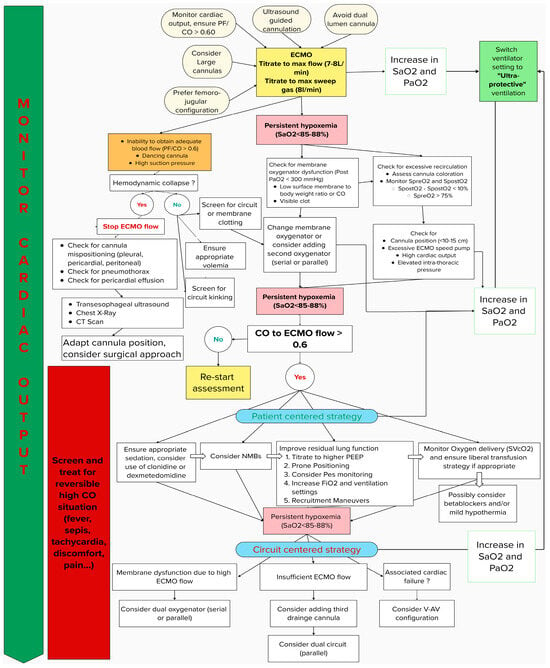
Figure 1.
Flowchart of stepwise management for refractory hypoxemia in ARDS vvECMO among obese patients.
2. Data Collection
A comprehensive literature search was conducted using PubMed, Google Scholar, and Scopus to identify relevant articles on managing refractory hypoxemia in obese patients with ARDS using veno-venous extracorporeal membrane oxygenation (VV-ECMO). The research did not impose a date restriction; however, emphasis was placed on the most recent studies, and the language was limited to English and French articles.
The inclusion criteria were as follows: studies and/or systematic reviews/meta-analyses involving patients with ARDS receiving vvECMO that included obese patients. Use of veno-arterial ECMO was included only if no data were found for vvECMO. When such studies were unavailable, those examining ARDS in obese patients, regardless of ECMO use, were considered. If no data were found on obesity in ARDS, general ARDS studies were selected, and subgroup analyses of obese patients were extracted when possible. Reviews and expert opinions were excluded except for validated guidelines from scientific society. Finally, “Similar articles” and “Cited by” sections in PubMed Central as well as the references of included papers were screened for additional material not found in the initial literature research.
This approach ensured the inclusion of the most relevant and comprehensive data on the topic.
3. Physiological Explanation of Refractory Hypoxemia in vvECMO: Inadequacy of ECMO Blood Flow and Cardiac Output (CO)
Although permissive hypoxemia was initially thought to improve survival [18], recent studies have shown that lower is not always better. Refractory hypoxemia can be defined as the impossibility to achieve an SpO2 of 88–95% [19] or PaO2 > 60 mmHg [20]. This can occur immediately after cannulation or at any time during vvECMO support. These cutoff values are commonly used and recommended [1,21], as lower oxygen saturation has been linked to increased mortality and/or morbidity (e.g., mesenteric ischemia) [22] in critically ill patients with ARDS. Conversely, higher SpO2 levels have not been linked to improved survival [23,24], even in COVID-19-induced ARDS [25].
Before diagnosing refractory hypoxemia during vvECMO, technical issues such as a kinked circuit, recirculation, cannula misplacement, or membrane and pump dysfunction must be ruled out first. Once these factors are addressed, refractory hypoxemia can generally be attributed to an imbalance between ECMO flow and the patient’s CO, where the oxygen delivery capacity of the circuit fails to meet the physiological demands of the patient. In vvECMO, part of the venous return goes through the ECMO circuit and is oxygenated to 100%, then returned to the right atrium. The rest (patient venous return), with 60–80% of venous saturation, passes through the pulmonary circulation unaltered. These flows (ECMO and patient’s flow) mix in the right atrium and ventricle, move through the lungs, and determine arterial blood saturation, which is typically 80–90%. ECMO flow must be adjusted relative to total venous return (cardiac output) to optimize systemic oxygen delivery [5].
This can be synthesized in a formula determining arterial oxygen saturation (SaO2) associated with vvECMO [26]:
where:
SaO2~SPAO2 = (EF/CO)SmO2 + (1 − EF/CO)SvO2
+ 0.01PmO2 + RLF
where EF = (1 − R)PF
- SPAO2 is oxygen saturation in the pulmonary artery (%);
- EF is effective flow, the fraction of pump flow oxygenated by ECMO (L/min);
- SmO2 is oxygen saturation in the blood exiting the oxygenator (membrane; %);
- CO is cardiac output (L/min);
- SvO2 is oxygen saturation in mixed venous blood (%);
- PmO2 is partial pressure of oxygen in the blood exiting the oxygenator (membrane; %);
- RLF is residual lung function;
- R is recirculation rate;
- PF is pump flow.
- The term 0.01PmO2 (in %) is a numerical estimation of the increase in SaO2 due to dissolved oxygen in the blood exiting the oxygenator.
This formula indicates that higher ECMO flow results in higher arterial saturation (SaO2), while higher cardiac output results in decreased SaO2. High recirculation also reduces SaO2, and improved residual lung function will improve SaO2. This has been demonstrated in clinical studies. In ARDS cases, Schmidt et al. [27] showed that ECMO flow below 60% of the patient’s cardiac output usually results in SaO2 inferior to 90%.
Thus, central to this issue is the inadequacy of ECMO blood flow relative to the patient’s cardiac output, a dynamic interplay with significant physiological implications.
Patients may exhibit a hyperdynamic circulatory state with elevated CO in conditions like obesity but also liver failure, pregnancy, hyperthyroidism, fever, systemic inflammatory responses (SIRS) or septic shock, arteriovenous malformations, Paget’s disease, myeloproliferative disorders, or even general agitation [28]. These conditions can exacerbate the imbalance, as the fraction of deoxygenated blood bypassing the ECMO circuit increases unless the ECMO flow is proportionally escalated. Screening for these conditions throughout the ECMO course is essential and should prompt a thorough assessment of cardiac output.
Additionally, elevated CO in hyperdynamic states makes it even more challenging to match ECMO blood flow to metabolic demands. Conditions associated with high cardiac output often coincide with increased metabolic demands, heightened oxygen consumption [29], and greater CO2 production, which can ultimately lead to tissue hypoxia and lactic acidosis.
4. Clinical Management
Assessment of hypoxemia should start directly upon cannulation. Initially, the sweep gas flow should be carefully titrated over ECMO blood flow (usually up to 7–8 L/min), and the membrane fraction of oxygen (FmO2) should initially be set to 100% to ensure optimal oxygenation [26]. Before escalating therapy to improve oxygen saturation, clinicians should address common pitfalls of vvECMO management. If inadequate resaturation or if desaturation occurs immediately after cannulation, the ECMO team must screen for complications linked to ECMO cannulation such as hemothorax, pneumothorax, or derecruitment causing atelectasis. Therefore, chest X-ray should be performed directly after cannulation in order to rule out these complications and to additionally address the position of the cannulas [30]. Meanwhile, clinicians should follow a stepwise approach, as most cases of persistent hypoxemia post-ECMO cannulation are due to technical issues that can be easily evaluated. Key parameters to evaluate sequentially include assessment of ECMO blood flow, recirculation, and membrane dysfunction.
Technical Issues
ECMO blood flow: ECMO blood flow should be titrated until optimal oxygen saturation or maximal ECMO capacity (usually up to 7–8 L depending on manufacturer) is obtained. If up titration of ECMO blood flow cannot be obtained, clinicians should raise concerns about cannulation misplacement (sus-hepatic vein, retroperitoneum in case of femoral cannulation, and pleural or pericardial space in case of jugular cannulation). This will often result in rapid hemodynamic deterioration and may ultimately lead to patient death. In such cases, the ECMO circuit should be stopped, and the ECMO cannula position should be assessed through adequate imaging (transesophageal ultrasound, chest X-ray, or CT scan depending on the severity of the patient and availability), and the surgical team should be advised if necessary. If adequate position of the cannulas is confirmed, the clinician should assess for hypovolemia and promptly initiate fluid resuscitation. Furthermore, kinking of the circuit can be a classic cause of inappropriate ECMO flow and should be ruled out quickly. Finally, inappropriate cannula purging during placement may result in massive clotting of the cannulas, prompting immediate replacement to avoid a massive pulmonary or air embolism.

Recirculation: At high ECMO flows, the return of oxygenated blood through the ECMO circuit can inadvertently mix with the drainage blood at the cannula site. This reduces the effective oxygen transfer of the circuit, as already oxygenated blood is reoxygenated, leaving systemic venous blood inadequately addressed. This can be easily and rapidly assessed by first examining the blood color in both cannulas [31]; a similar reddish color could indicate significant recirculation. This can be evaluated also by arterial gas samples from the venous and arterial cannulas.
Excessive recirculation can be detected based on high SvO2 (usually > 75%) and minimal saturation difference (less than 10%) between pre-membrane saturation and post-membrane saturation. Additionally, recirculation fraction can be calculated upon this formula and should be less than 20–30% [32].
SpréOx − SVO2/SPostOx − SVO2
In a study by Pooth et al. [33], the authors showed that excessive recirculation often occurs due to the close proximity of the drainage and return cannulas, high ECMO blood flow, and low cardiac output [32]. BMI was not associated with a high recirculation ratio [32]. Certain configurations of cannulation (femoro-femoral) were associated with more recirculation than femoro-jugular or dual lumen cannulas and thus probably need to be avoided. The ideal range between the cannulas should be between 10 to 15 cm [26]. Dual lumen cannulas (e.g., Avalon cannulas) are known to reduce the risk of recirculation [33] due to their placement, with drainage orifices positioned in both superior and inferior vena cava, while the orifice reinjection jet is oriented directly toward the tricuspid valve. As illustrated, this precise placement requires an experienced clinician, as there is a steep learning curve associated with this technique [34]. Moreover, dual lumen cannulas do not permit high flow rates [35]; therefore, they should not be considered a viable alternative in cases of refractory hypoxemia due to high cardiac output. Other factors influencing recirculation are a high-speed pump, high CO to QECMO ratio, and high intrathoracic pressure [32].

Inadequate ECMO membrane efficiency or membrane dysfunction: At 100% FmO2 and max sweep gas, post-membrane PaO2 should normally be higher than 300 mmHg [31]. If this is not the case, clinicians should assess for membrane dysfunction. First, screening for membrane clotting due to inappropriate cannulation is essential, followed by regular monitoring for increased pre-membrane pressure, visible blood clots, and altered post-membrane PaO2 [5,31]. Additionally, ECMO oxygenators have a limited capacity for oxygen transfer, which depends on the surface area of the oxygenator and the blood’s transit time through it. At high flow rates, the reduced transit time can limit oxygen diffusion, worsening the mismatch between oxygen supply and demand. The appropriate surface membrane should be chosen according to the patient’s morphology and CO. ECMO membrane surfaces vary from 0.75 m2 to 2.5 m2; a high surface membrane might be necessary in cases of morbidly obese patients or patients with hyperdynamic states.

5. Standardized Protocol
Initiation of shared guidelines and standardized protocols has been largely associated with higher quality of care [36]. Implementing local protocols for the management of refractory hypoxemia in vvECMO patients could be beneficial. Several studies [37,38] have shown that implementing such guidelines may improve survival, reduce ICU length of stay, and increase ventilator-free days. Zhou et al. [37] conducted a single-center, retrospective cohort study of patients undergoing vvECMO and found that after implanting a local protocol for refractory hypoxemia, compliance with protective ventilation strategies during ECMO support improved. They observed lower mean plateau pressure, driving pressure, and tidal volume during ECMO course. Additionally, there was a statistically significant increase in the number of patients undergoing prone positioning and a significant reduction in the use of high-frequency oscillation ventilation [37]. Gallo de Moraes et al. [38] demonstrated comparable results in non-ECMO ARDS with the evidence of shorter time to prone positioning as well as reduced ICU and hospital length of stay.
6. Patient-Centered Strategy
6.1. Residual Lung Function
In ARDS, protective ventilation (6 mL/kg of ideal body weight [IBW]) has been shown to improve mortality and increase ventilator-free days [39]. This strategy has thus been widely adopted and recommended by guidelines on ARDS [1,19,40]. The rationale for vvECMO use is therefore to deepen this strategy by applying “ultra-protective ventilation” (3–4 mL/kg of IBW, low plateau and driving pressure, high PEEP, and low respiratory rate (RR) [5,6,7,8,9,10]) to put the lung at maximum rest in order to further improve lung regeneration and potentially improve survival.
Comparison of both ventilation strategies are summarized in Table 2.
Table 2.
Comparison of protective and ultra-protective ventilation strategies.
Despite the pathophysiological rationale for ultra-protective ventilation, data on its impact on barotrauma or survival outcomes remain controversial [41,42]. Two studies conducted by Li et al. [43] and Nishikimi et al. [44] looking at ultra-protective ventilation in vaECMO and vvECMO might add some evidence to current knowledge. Therefore, optimizing residual lung function by titrating the ventilator to higher PEEP, plateau pressure (PPlat), RR, and FiO2 may be necessary, especially in the obese population.

Use of concomitant vvECMO with prone positioning, optimal PEEP with recruitment maneuvers, and utilization of an esophageal probe as well as with inhaled nitric oxide are discussed further.
Recruitment maneuvers: Recruitment maneuvers (RMs) are sustained but temporary increases in transpulmonary pressure aimed at reopening collapsed alveoli (incremental increases in PEEP to achieve airway pressures ≥35 cm H2O) [1], enhancing the lung volume involved in gas exchange and ultimately improving oxygenation [45]. Their routine use has been controversial in the literature due to concerns about hemodynamic collapse, barotrauma, and ventilator-induced injury [46]. Several methods exist, including the Staircase Recruitment Maneuver (SRM) described in the ART study [47], the sustained inflation recruitment maneuver [48], or a gradual increase in continuous airway pressure (CPAP 40 cm H2O) [49]. However, recent meta-analyses of non-ECMO ARDS [45,50,51] failed to prove increased survival. Among obese patients, the PHARLAP study (mean BMI of 31 kg/m2) [52] and De Santis Santiago et al. (mean BMI of 57 kg/m2) [53] did not demonstrate improved survival despite good hemodynamic tolerance. Although, among survivors, obese patients showed more ventilator-free days and less need for adjunctive therapies (vvECMO and inhaled nitric oxide). Based on this evidence, recruitment maneuvers appear to be a reasonable technique for optimizing ventilation in obese patients who require improvement in their residual lung function.

Higher titration PEEP and use of esophageal probe: A low driving pressure (less than 15 mmHg) may be associated with lower mortality in ARDS [54]. Ultra-protective ventilation with very low respiratory rates and very low tidal volumes can cause progressive derecruitment of lungs, induce atelectasis, worsen gas exchange, and increase shear stress to the alveoli. To minimize this phenomenon, an open lung strategy has been proposed involving the use of a higher PEEP combined with low tidal volume. This approach leads to low driving pressure and therefore hypoventilation. vvECMO facilitates this strategy by efficiently removing the CO2 from the blood. While some animal studies have suggested that ultra-protective ventilation may help to reduce lung inflammation, Deniel et al. [55] showed that low tidal volume, PEEP titrated to a maximum of 20–25 cmH2O of PPlat, and low RR (5/min) were associated with less lung inflammation. Similarly, a randomized controlled trial conducted by Hermann et al. [56] showed that low RR (4–5/min) associated with high PEEP (14-16 cmH2O) was associated with higher ventilator-free days than conventional ventilation. Mortality was lower in the ultra-protective group but did not reach statistical significance.
In obese patients, PEEP is often underestimated [10,57,58], although higher PEEP levels may be necessary due to increased abdominal pressure and chest wall weight, with some studies suggesting a survival benefit [10,52,59]. Moreover, experimental studies have shown that pleural pressure and transpulmonary pressure were not directly correlated with PPlat in the obese population [60,61]. Consequently, esophageal pressure (PES) monitoring has been considered a potential tool in obese and super-obese patients on vvECMO. However, the EPVent-2 study [62] found no superiority of PES monitoring, despite higher PEEP in the PES group and a high prevalence of obesity in their population. In a post hoc reanalysis of the EPVent-2 study [63], the authors demonstrated the lowest mortality when end expiratory transpulmonary pressure was equal to 0 cmH20. Conversely, studies by De Jong et al. [61] and Terry et al. [64] found that in an obese population, elevated driving pressure and plateau pressure were not correlated with higher mortality in ARDS.
Given the lack of certainty, these measures could serve as a valid adjunctive therapy to guide ventilation in the obese vvECMO population. Nonetheless, these practices should be individualized based on patient-specific data, clinical relevance, and institutional practices.

Prone positioning: Prone positioning (PP) improves oxygenation by enhancing ventilation–perfusion matching by providing a more homogenous distribution of transpulmonary pressure across the lungs [10]. PP has been demonstrated to increase survival in severe ARDS (when PaO2 to FiO2 ratio drop under 150) [65], and current ARDS guidelines [1,20,40] strongly recommend PP in these cases. Several studies have shown the feasibility of PP in both obese [66] and ECMO patients [67]. However, evidence supporting the routine use of PP during vvECMO remains controversial. An early retrospective trial by Petit et al. [67] suggested improved survival with PP and vvECMO. Other small retrospective studies showed possible trends toward improved survival with PP, especially if applied early (less than 24 h after cannulation) [68,69]. Additionally, a recent prospective observational trial from patients with non-COVID-19 ARDS conducted by Wang et al. [70] showed improvement in weaning from ECMO and sixty-day mortality. Patients all underwent PP before ECMO implementation. Finally, a pooled individual patient data analysis of European cohort studies conducted by Giani et al. [71] showed improvement in ICU mortality, but this did not reach statistical significance. However, when patients were matched on baseline characteristics using a propensity score, those in the prone group had a lower 60-day mortality. Despite these encouraging findings, the first multicenter prospective study PRONECMO [72] published in 2023 by Schmidt et al. did not demonstrate a significant benefit of PP in ECMO weaning time and mortality. The study involved patients with a mean BMI of 33 kg/m2, reflecting the high prevalence of obesity in their population. Several limitations may have influenced the results, including prior use of PP before ECMO initiation, the COVID-19 pandemic, the small sample size, and the study design. Nevertheless, given its safety and feasibility, use of PP during ECMO could still be a viable option for obese patients with low pulmonary compliance.

Inhaled nitric oxide: Inhaled nitric oxide (InhNO) enhances oxygenation and gas exchange through the dilation of alveolar vessels receiving oxygen, thereby reducing ventilation–perfusion mismatch and improving oxygen capture by ventilated alveoli [73]. This mechanism allows for improved oxygenation without altering ventilator settings, offering an elegant alternative in patients with high ventilator pressures. Despite this encouraging pathophysiological approach, the literature has failed to demonstrate the superiority of InhNO in ARDS [74,75], and a meta-analysis even showed the potential harmful effect of InhNO. The harmful effect of InhNO can be explained by the formation of peroxynitric acid in the situation of high FiO2, which is a highly pulmonary toxic substance [76]. As a result, use of InhNO was mostly abandoned. The COVID-19 pandemic, however, renewed interest in the technique, and InhNO was widely used to treat refractory hypoxemia in patients with COVID-19-related ARDS, with studies reporting the use of InhNO in approximately 20–25% of ARDS patients [77,78]. While research in both COVID-19 and non-COVID-19 ARDS showed improved oxygenation, no survival benefit was demonstrated [79,80,81,82]. One study suggested that patients with vvECMO criteria might benefit from InhNO [80], though further research is needed to confirm this finding. In a small recent observational study conducted by Muensters et al. [83], ECMO with InhNO in COVID-19 ARDS was associated with a poorer outcome, but InhNO responders had better survival. Therefore, nitric oxide cannot be routinely recommended to treat vvECMO ARDS with refractory hypoxemia and should be used as a last resort if deemed appropriate.

6.2. Reducing Oxygen Consumption and Carbon Dioxide Production
One way to minimize tissue hypoxia and improve oxygenation is by reducing the body’s overall oxygen consumption, which can be achieved through simple approaches. Common causes of elevated oxygen utilization (VO2) include sepsis, fever, agitation, movements, and shivering. All these causes should be considered in cases of worsening hypoxemia in vvECMO, where other previous complications have been ruled out. Optimizing sedation, favoring a completely controlled ventilation strategy, and ultimately using an intermittent or continuous neuromuscular blockade can help achieve lower oxygen consumption targets. This can also decrease CO2 production. Multimodal use of sedation may be necessary in obese patients, as they often require a higher dose of sedatives to obtain the sedation goal. The adsorption or sequestration of sedative drugs within the ECMO circuit further complicates the situation [84]. Sedative agents include morphine derivatives, propofol, benzodiazepines, ketamine, clonidine, and occasionally neuroleptic or anti-epileptic drugs [84]. Fever, although rare in the vvECMO setting, is also a trigger for increased oxygen consumption; consequently, strict temperature control needs to be performed throughout the ECMO circuit.
Neuromuscular blockade: The neuromuscular blockade (NMB) plays a nuanced role in the management of ARDS. Neuromuscular blocking agents (NMBAs) have been shown to decrease oxygen consumption by eliminating muscular activity and improving systemic oxygenation, particularly in muscles involved in respiratory function. This mechanism reduces respiratory demand and cardiac output, leading to increased mixed venous oxygen partial pressure and arterial oxygen partial pressure. By reducing the work of breathing during mechanical ventilation, NMBAs can significantly lower whole-body oxygen consumption, with reports of up to a 25% reduction [85]. Additionally, this redistribution of blood flow to the splanchnic and other non-vital vascular beds contributes to sparing oxygen for vital organs. NMBAs may also mitigate ventilator-induced lung injury (VILI) by reducing high minute ventilation and excessive patient effort. However, the impact of NMBAs on mortality remains controversial, especially in the ECMO population, for whom data are lacking. De Grado et al. studied current practice among ECMO patients, and they showed that only 12 percent of ECMO patients receive continuous NMBs [86], emphasizing the uncertainty regarding this practice. Kressin et al. [87] reported no change in ECMO free days, ICU length of stay, or mortality in a small single-center, retrospective observational cohort study involving 47 ECMO patients. In the ECMObesity trial [11], which showed improved survival of obese patients with vvECMO compared to non-obese populations, 68% of obese patients received NMBs compared to 59% of non-obese. No randomized controlled trials exist regarding the use of NMBs in the ECMO population; therefore, current evidence is based on the non-ECMO ARDS population. Key studies have reported conflicting outcomes: the Early Neuromuscular Blockade in the Acute Respiratory Distress Syndrome (ROSE) [88] trial found no survival benefit from early NMBs, whereas the Neuromuscular Blockers in Early Acute Respiratory Distress Syndrome (ACURASYS) [89] trial demonstrated improved survival rates. Neither study provided an indication of BMI in their population, but the ROSE study excluded super-obese patients from their protocol. Finally, a recent meta-analysis reported increased survival among non-ECMO ARDS patients treated with NMBAs [90]. Clinical evidence supporting the use of NMBAs in vvECMO are lacking. Integrating data from non-ECMO ARDS might provide an indication on use in the vvECMO setting in addition to pathophysiological data.
6.3. Optimizing Oxygen Delivery and Transfusion Strategy
Hunsicker et al. [91] demonstrated that a restrictive transfusion strategy (<8 g/dL) in ECMO and non-ECMO ARDS patients resulted in similar survival as a liberal strategy (<10 g/dL). For patients with severe ARDS treated with vv-ECMO, the optimal hemoglobin level has not been well defined. The Extracorporeal Life Support Organization (ELSO) guidelines [5] recommend maintaining a normal hematocrit level during ECMO treatment; however, some small retrospective studies [92,93,94] have shown a trend toward similar survival, with a transfusion threshold of 7 g/dL of hemoglobin. Additionally, the PROTECMO observational study [95] showed no sign of improved survival when the transfusion threshold was set higher than 7 g/dL of hemoglobin. Thus, the routine hemoglobin level of a vv-ECMO course could be set at 7g/dL if appropriate tissue oxygenation is provided.
That being said, and on top of previous strategies, in cases of tissue hypoxia despite previous measures ensuring adequate oxygen delivery, higher hemoglobin level and therefore liberal transfusion strategy might be employed reasonably, especially since Schmidt et al. showed improvement in SaO2 and PaO2 with higher hemoglobin levels [27].

6.4. Optimizing ECMO Blood Flow to Patient Blood Flow Ratio (QECMO/QCO Ratio)
When managing refractory hypoxemia and when considering vvECMO in cases of ARDS, the clinician should primarily monitor the patient’s CO and calculate the ECMO blood flow to patient’s CO ratio (QECMO/QCO). The optimal ratio has been shown to be set at >60% [27]. If the ratio is too low (meaning there will be significant shunting into the dysfunctioning patient’s lungs, resulting in hypoxemia), strategies involving optimizing the CO accordingly to ECMO blood flow might be employed.
General strategy: The classical approach involves the previous strategies discussed above (optimizing sedation and use of NMBs as decreased metabolic demands often result in decreased CO). If not sufficient, the addition or up titration of clonidine or dexmedetomidine to existing sedation might be employed to benefit from their mechanism of action (stimulating the presynaptic alpha-2 adrenoceptors, thereby decreasing norepinephrine release from both central and peripheral sympathetic nerve terminals) [96] allowing for decreased CO in addition to their sedative effect [97]. Similarly, sinus rhythm should be maintained, and rapid ventricular response atrial fibrillation should be avoided. Vasopressor therapy should be titrated to the minimal acceptable mean pressure to avoid the inotropic effect of norepinephrine and induced arrythmia. Ultimately, cautious use of beta-blockers or, in some cases, therapeutic hypothermia might be considered.

Beta-blockers: The rationale for using beta-blockers (BB) is their negative inotropic effect, which can effectively reduce CO and therefore increase the QECMO/QCO ratio above 0.6 [27]. Their ability to decrease CO may be of interest in the context of refractory hypoxemia in vv-ECMO due to a low QECMO/QCO ratio. Despite these considerations, there are concerns regarding the safety of BB use in this setting.
Since tissue oxygenation (which remains the primary goal when considering vvECMO) ultimately relies on oxygen delivery (DO2), BB must demonstrate evidence of improved tissue oxygenation to support their routine use. The pathophysiology regarding BB use in vv-ECMO includes an understanding of the determinants of DO2 and arterial oxygen content (CaO2).
DO2 and CaO2 can be calculated using the following equations:
DO2 = CO × CaO2
CaO2 = 1.34[Hb](SaO2/100) + 0.003PaO2
These formulas indicate that even if BB may improve SaO2 and consequently CaO2, by optimizing QECMO/QCO, they achieve that goal at the cost of a lowered CO, thereby diminishing DO2. If high cardiac output is driven by high oxygen demands, a BB-induced reduction in CO is associated with a lower DO2.
In their articles, Staudacher et al. [98] and Bommiasamy et al. [99] (in response to Staudacher et al.) demonstrated that despite improving SaO2, BB use was associated with lower CO and resulted in decreased DO2 in patients with ARDS who where totally dependent on vvECMO for tissue oxygenation. In their original article [98], Staudacher et al. concluded that BB might only be advisable in situations where CO is inappropriately increased and not driven by oxygen demand and that simpler measures, such as discussed above, should be prioritized.
If, despite these concerns, clinicians still decide to use BB, esmolol might be the first-line agent. Esmolol is a short-acting cardio-selective BB administered via continuous infusion. A few small studies have investigated the safety and feasibility of esmolol during the vvECMO course in select tachycardic patients [100,101,102]. They all showed improvements in SaO2. Another case series by Kim et al. [103] further confirmed the improvement in SaO2 but also the decrease in DO2. Krupnik et al. [104] studied the effect of metoprolol in forty-two vvECMO patients with COVID-19 ARDS. They experienced only mild improvement in SaO2, and metoprolol was associated with a high rate (47.6%) of adverse events, including hypotension, increased lactate levels, and bradycardia. Therefore, as there is still insufficient to no data to support the routine use of BB in vvECMO in cases of a low QECMO/QCO ratio, clinicians should use BB very cautiously. One valid indication could be the use of BB in cases of rapid response supra-ventricular tachycardia.

Therapeutic induced hypothermia: Hypothermia is associated with bradycardia and low CO with a 7% drop in CO per °C [105]. Considering this, decreasing temperature via the heat exchanger of the ECMO circuit might increase QECMO/QCO. Moreau et al. [106] summarized the body of evidence in induced hypothermia for high CO patients undergoing vvECMO. The current literature relies on small studies and cases reports, introducing selection and publication biases to the available literature. The optimal target temperature for this population remains unknown due to significant heterogeneity in the available studies. The authors conclude that induced hypothermia is a feasible and relatively safe intervention in the setting of the high CO vv-ECMO population; however, its effects on clinical outcomes remain uncertain.

7. ECMO Circuit-Centered Strategy
When previous measures become insufficient, modifications to the ECMO circuit can become critical. Modifications involve alterations to the ECMO circuit in order to improve QECMO/QCO or to maximize oxygen transfer from the oxygenator to the patient’s blood. Available options include the addition of a third drainage cannula to enhance venous drainage in cases of insufficient ECMO flow, the use of dual oxygenators in parallel or in a series to increase oxygen transfer efficiency, or even transitioning to more complex configurations such as veno-arterio-venous ECMO (v-avECMO) or dual independent (parallel) vvECMO circuits. Although these strategies might seem attractive, they remain purely experimental, as the literature rely only on case series or reports. Such interventions require careful consideration of risks linked to ECMO circuit manipulation, particularly in patients completely dependent on ECMO support. Potential complications include catastrophic hemorrhage, massive air embolism, hemolysis, thrombosis, and mechanical stress on the ECMO system. These measures also place additional pressure on the nursing and/or perfusion teams by increasing the workload required to manage these patients. Given the risks mentioned earlier, these considerations should be implemented in expert centers. However, despite these challenges, such measures can be lifesaving in cases of extreme refractory hypoxemia. When considering these strategies, clinicians should follow a stepwise approach, starting with minimally invasive methods and progressing to more complex ones. Since neither technique has shown clear superiority over the other, the final decision should be based on the clinician’s and ECMO team’s experience, integrating the resources available at their center.
7.1. Enhancing QECMO/QCO by Employing Large Cannulas or Adding Additional Cannulas
The preferred site of cannulation should be the femoro-jugular configuration, as it decreases the risk of recirculation [33,107] and allows for large-diameter cannulas, effectively providing higher flow. Other cannulation sites include the bi-femoral configuration or supra- or (more rarely) sub-clavian cannulation, which has been described to be a safe alternative in cases of limited venous access [108]. Double lumen cannulation should be avoided in obese patients as it provides only limited flow [107,109,110] (max 4–5 L/min).
Cannula diameters usually range from 17 French to 31 French depending on the manufacturer. Inserting large-diameter cannulas can lead to fear of vessel injury. However, large cannulas are often necessary to achieve high flow in vvECMO [5]. Mauri et al. [111] demonstrated that large-diameter cannulas allowing for a higher ECMO flow were associated with improved survival in COVID-19 ARDS and did not increase the risk of vessel injury. Spinelli et al. [112] further demonstrated positive physiological changes associated with high QECMO, showing improved SvO2, decreased CO, and decreased pulmonary pressure and right ventricle workload, highlighting the need for larger cannulas. Additionally, larger cannulation provides less recirculation [113]. Thus, in the obese population or high-cardiac-output population, it is strongly recommended the cannula diameter be tailored to the patient’s anatomy [109].
A third drainage cannula might be necessary if a high QECMO remains difficult to achieve despite the use of a large-diameter cannula. A supplemental cannula can be inserted into the contralateral femoral vein, creating a femoro-femoro-jugular configuration. During the COVID-19 pandemic, two retrospective and observational studies [113,114] demonstrated the feasibility of this technique. This configuration allowed for improved QECMO with an identical speed pump but showed no change in post-oxygenator SvO2 and no impact on survival.

7.2. Optimizing ECMO Oxygen Transfer Efficiency
The addition of a second oxygenator, either in parallel or in a series, can improve post-membrane SvO2 or PaO2. This has only been poorly described in the literature through limited case reports. Miyazato et al. [115] used two oxygenators in parallel in a patient with severe obesity and COVID-19 ARDS. In their case, placement was triggered by persistently low post-membrane PaO2 despite several oxygenator changes. The addition of a second oxygenator significantly improved post-membrane PaO2 with no further decline, ultimately allowing for vvECMO withdrawal. They demonstrated that a shunt can be induced in the vvECMO circuit if QECMO is high, reducing the transit time through the oxygenator and providing insufficient time for oxygen transfer. Hurtado et al. [116] described a three-patient series with severe ARDS secondary to COVID-19 and refractory hypoxemia during ECMO support successfully treated with this approach. On the other hand, Leloup et al. [117] used two oxygenators in a series for refractory hypercapnia in a patient (with a body surface area of 2.77 m2) with ARDS following traumatic brain injury. This approach allowed for protective ventilation and restoration of normal PaCO2 for brain protection. They did not demonstrate any effect on systemic PaO2, as post-membrane oxygenation was already satisfactory. Seadler and al. [118], on their side, conducted an observational study in patients with refractory hypoxemia and hypercapnia on vvECMO during the COVID-19 pandemic using an additional oxygenator placed in parallel. Their approach increased post-membrane PaO2 and systemic PaO2 while reducing PaCO2 and FiO2, thereby enabling (ultra)protective ventilation.
In porcine models, Melro et al. [119] studied the efficacy and systemic implications of serial or parallel oxygenators (Jostra–Quadrox D, Maquet, surface membrane: 1.8 m2) with max QECMO of 5.5 L/min. They showed that both oxygenator configurations resulted in minors changes in circuit blood pressures and systemic oxygenation and modest changes in decarboxylation efficacy. The results observed may be attributed to the lack of data on ECMO flow rates above 7L associated with smaller membrane surfaces, meaning their method could not determine whether it would be effective in this configuration. In their study, they showed that a parallel oxygenator configuration in contrast to the serial configuration offers the advantage of not increasing the ECMO flow resistance. CO2 removal was slightly higher in the parallel configuration compared to the serial one. Additionally, Omlor et al. [120] performed an experimental study on a mock ECMO circuit, testing for serial and parallel oxygenation in the context of refractory hypoxemia. In contrast, Melro et al. found that a serial configuration may provide better oxygenation and decarboxylation. They explain this phenomenon using the concept of a “boundary layer”, which is a stationary fluid layer on the outside of the gas fibers that oxygen molecules need to pass via diffusion. The higher blood flow achieved in the serial configuration allowed for thinning of the boundary layer and therefore better oxygen transfer [121]. Thus, the use of two oxygenators in parallel or in a series might offer a safe and relatively simple alternative in cases of refractory hypoxemia induced by shunting through the ECMO circuit when a high QECMO is needed.

7.3. The Use of Additional Circuits
If hypoxemia persists despite previous measures, and QECMO/QCO remains below 0.6, an alternative to previous vvECMO modifications is the use of a complete additional circuit, either in series or in parallel. This configuration requires the separation of two independent vvECMOs and necessitates appropriate volemia for additional cannula insertion, as it can lead to severe vascular injury due to the requirement of the placement of two cannulas in the inferior vena cava. Although the parallel configuration is more common (allowing for better improvement in total QECMO), the serial configuration has also been used. Kang et al. [122] described the use of two serial extra corporeal membrane oxygenators, allowing for weaning of the ECMO support in an obese patient during the COVID-19 pandemic. Several cases reports demonstrated the feasibility of this approach [123,124,125]. Kwon et al. [123] used two parallel vv-ECMO circuits in a burn patient with acute lung injury in order to palliate the high cardiac output of the patient. In their configuration, they used two separate ECMO circuits with two separate drainage cannulas going through two different pumps and oxygenators, which were then reunited in a “Y” shape configuration in the jugular vein. Patel et al. described a case series of five patients treated with parallel vvECMO circuits with relatively successful results [126]. They further demonstrated the effectiveness and feasibility of the approach with four out of five patients surviving until ICU discharge. They also showed that the duration of ECMO support could be prolonged up to 73 days in this configuration without a high rate of complications. Another observational study [127] described the routine use of two parallel vvECMO circuits for refractory hypoxemia in 22 obese patients (mean body weight of 122 kg), further demonstrating the feasibility and need for higher QECMO in the obese population with a high CO (mean CO of 14 L/min). Among their cohort, 16 patients out of 22 survived, with a mean ECMO support duration of 40 days. They experienced very few cannulation problems, but their patients required a mean of two changes in ECMO circuit during ECMO support, demonstrating the high workload for these patients. A limitation of their study was that none of their patients underwent PP before or during ECMO support, despite its proven safety and effectiveness in both obese and ECMO populations [65,66,67,68,69,70]. Although Patel et al. [126,127] reported only a few cannulation complications, the technique still requires a high nursing workload, two additional cannulations with two cannulas in the inferior vena cava, and one cannula in each jugular vein, doubling the risk of potential complications. Therefore, while technically feasible, potentially safe, and capable of significantly improving the QECMO/QCO ratio, leading to better systemic oxygenation in obese patients with high CO, double-circuit vvECMO should be used as a last resort in experienced centers when other techniques have failed.
7.4. Other Techniques (V-AV, VA, or VV-VA ECMO)
Switching from vvECMO to vaECMO: Extracorporeal membrane oxygenation provides a variable content of oxygen to the blood that is directly related to the hemoglobin × blood flow rate. Delivery of that oxygen content to the arterial system achieves little or no increase in systemic oxygen delivery over vvECMO [5], with an increase in meaningful complications [128]. In the case of severe ARDS treated with vaECMO, as the heart recovers, patients can have upper body (and cerebral) hypoxemia; this is known as “Differential hypoxemia”, “Harlequin” [129], or “North/South syndrome”. Therefore, this approach cannot be recommended to manage refractory hypoxemia in high cardiac output patients [5].
V-AV configuration: In cases of refractory hypoxemia during vaECMO and the occurrence of Harlequin syndrome due to the association of heart and lung failure, the addition of a jugular return cannula (v-avECMO) might be required [130,131]. V-avECMO allows for bypassing the native lung to oxygenate the upper body. This configuration is only used in cases of concomitant heart and lung failure and cannot be recommended for refractory hypoxemia due to high CO during the vaECMO course due to flow competition, where classical vvECMO would be sufficient.
More complex strategies: Navas Blanco et al. [132] described a case of management of refractory hypoxemia with a double va and vvECMO circuit in an obese patient. In their case, due to high CO, requiring high QECMO, they switched from classical vvECMO to a v-vvECMO configuration. Later, they needed to add a va-ECMO circuit in parallel due to cardiovascular collapse. They justified the use of the VA and VV circuits by the high flow required in their obese patient and the shear stress potentially caused by high flow through the oxygenators and pumps required to provide sufficient QECMO. The need for this technique may have been driven by the high hemodynamic support required to meet the elevated metabolic demands associated with the patient’s size (BMI of 54 kg/m2 and BSA of 3.27 m2). Ka et al. [133] also described a case of using a double VV and VA circuit in parallel. Contrary to Navas Blanco et al., their patient was not obese and did not experience a high cardiac output. Their rationale for implementing VV and VA circuits in parallel was driven by the fact that the V-AV configuration would require a temporary pause in ECMO support (risking catastrophic complications) and the low blood flow provided by their machine (maximum 4 L/min). These few case reports cannot provide enough evidence to support the routine use of this configuration in situations of refractory hypoxemia associated with heart failure.

Additional strategies exist, including the use of Impella [134] or Pulmonary artery ECMO (paECMO) [135], mixing support in case of associated heart and lung failure. These associations are outside the scope of this article and are not discussed further.
7.5. Resource and Cost Effectiveness
ECMO patients require highly specific needs and an increased nursing workload. Lucchini et al. [136] demonstrated in their study that the nursing activity score (NAS) was significantly higher in the ECMO population and recommended, in alignment with current guidelines, a patient to nurse ratio of 1 with highly trained nurses [137]. The implementation of a second ECMO circuit, whether in parallel or in a series, significantly increased the demand on healthcare resources, particularly in terms of nursing workload [138], perfusionist involvement, and overall medical resource allocation. Standard patient care, including repositioning, hygiene, and routine interventions, becomes exceedingly complex, often necessitating the involvement of multiple nurses or caregivers to safely execute even basic tasks. This added complexity can lead to increased staff fatigue, higher rates of burnout, and a greater risk of complications due to potential lapses in protocol adherence [139].
From a financial perspective, studies evaluating the cost of ECMO demonstrated that patients receiving ECMO had significant higher costs compared to non-ECMO ICU patients [140]. These advanced strategies contribute, consequently, to a marked increase in healthcare costs, primarily due to prolonged ICU length of stay, heightened consumable usage, and the need for multiple ECMO circuit exchanges [127]. Patients with refractory hypoxemia requiring such advanced configurations often experience longer durations of ECMO support, with studies reporting median ECMO runs exceeding 40–70 days in certain cohorts [126]. Each ECMO circuit change represents a substantial financial burden, depending on institutional pricing and regional healthcare policies ranging from tens of thousands to hundreds of thousands of USD [140,141,142]. On average, 82% of costs for the total hospital stay were related to personnel use. Blood products constituted 7%, laboratory and radiology 2.5%, disposable items 3%, and medication 1.5% [141]. Potential complications such as vascular injury and infection further prolong hospital stays, compounding both direct and indirect costs. Finally, in addition to the high costs and significant workload demands, advanced ECMO strategies can exacerbate resource depletion, placing further strain on ECMO-capable centers, especially during periods of heightened demand, such as the COVID-19 pandemic.
8. Conclusions
Veno-venous extracorporeal membrane oxygenation has evolved into a crucial intervention for patients with severe ARDS and refractory respiratory failure, particularly in cases where conventional therapies have failed. While obesity presents unique physiological and technical challenges, emerging evidence suggests that it should not be viewed as a contraindication to vvECMO. Contrary to initial concerns, obese and even super-obese patients appear to exhibit comparable or even improved survival rates during ECMO support, reinforcing the concept of the “obesity paradox”.
However, the management of vvECMO in this population requires careful consideration of distinct pathophysiological factors, including increased cardiac output, elevated blood volume, and heightened oxygen consumption, all of which may influence oxygen delivery and ECMO efficiency. Technical challenges such as percutaneous cannulation, infection risk, and anticoagulation strategies must be addressed to optimize patient outcomes.
Given the increasing prevalence of obesity in critical care settings, ICU clinicians must enhance their expertise in vvECMO strategies tailored to this high-risk group. Further studies are needed to refine best practices and determine the optimal management protocols for obese patients requiring ECMO support. Nevertheless, current data indicate that when appropriately managed, vvECMO remains a life-saving intervention that should be strongly considered in the obese population with severe ARDS. However, the implementation of advanced ECMO strategies in this population comes with significant challenges, including increased costs, heightened resource utilization, and a substantial burden on ICU staff, particularly the nursing team, which must be carefully weighed when considering these interventions.
Author Contributions
Conceptualization, A.R.; Methodology, A.R., P.B., and I.M.; Validation, A.R., P.B., and I.M.; Investigation, A.R.; Resources, A.R.; Writing—Original Draft Preparation, A.R.; Writing—Review & Editing, A.R., P.B., P.M.H., and I.M.; Supervision, A.R., P.B., P.M.H., and I.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Qadir, N.; Sahetya, S.; Munshi, L.; Summers, C.; Abrams, D.; Beitler, J.; Bellani, G.; Brower, R.G.; Burry, L.; Chen, J.-T.; et al. An Update on Management of Adult Patients with Acute Respiratory Distress Syndrome: An Official American Thoracic Society Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2024, 209, 24–36. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Combes, A.; Hajage, D.; Capellier, G.; Demoule, A.; Lavoué, S.; Guervilly, C.; Da Silva, D.; Zafrani, L.; Tirot, P.; Veber, B.; et al. Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2018, 378, 1965–1975. [Google Scholar] [CrossRef] [PubMed]
- Peek, G.J.; Mugford, M.; Tiruvoipati, R.; Wilson, A.; Allen, E.; Thalanany, M.M.; Hibbert, C.L.; Truesdale, A.; Clemens, F.; Cooper, N.; et al. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): A multicentre randomised controlled trial. Lancet 2009, 374, 1351–1363. [Google Scholar] [CrossRef] [PubMed]
- Schetz, M.; De Jong, A.; Deane, A.M.; Druml, W.; Hemelaar, P.; Pelosi, P.; Pickkers, P.; Reintam-Blaser, A.; Roberts, J.; Sakr, Y.; et al. Obesity in the critically ill: A narrative review. Intensiv. Care Med. 2019, 45, 757–769. [Google Scholar] [CrossRef]
- Tonna, J.E.; Abrams, D.; Brodie, D.; Greenwood, J.C.; Mateo-Sidron, J.A.R.; Usman, A.; Fan, E. Management of Adult Patients Supported with Venovenous Extracorporeal Membrane Oxygenation (VV ECMO): Guideline from the Extracorporeal Life Support Organization (ELSO). ASAIO J. 2021, 67, 601–610. [Google Scholar] [CrossRef] [PubMed]
- Martino, J.L.; Stapleton, R.D.; Wang, M.; Day, A.G.; Cahill, N.E.; Dixon, A.E.; Suratt, B.T.; Heyland, D.K. Extreme Obesity and Outcomes in Critically Ill Patients. Chest 2011, 140, 1198–1206. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wardell, S.; Wall, A.; Bryce, R.; Gjevre, J.A.; Laframboise, K.; Reid, J.K. The Association between Obesity and Outcomes in Critically Ill Patients. Can. Respir. J. 2015, 22, 23–30. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Decruyenaere, A.; Steen, J.; Colpaert, K.; Benoit, D.D.; Decruyenaere, J.; Vansteelandt, S. The obesity paradox in critically ill patients: A causal learning approach to a casual finding. Crit. Care 2020, 24, 485. [Google Scholar] [CrossRef]
- De Jong, A.; Verzilli, D.; Jaber, S. ARDS in Obese Patients: Specificities and Management. Crit. Care 2019, 23, 74. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Javidfar, J.; Zaaqoq, A.M.; Yamashita, M.H.; Eschun, G.; Jacobs, J.P.; Heinsar, S.; Hayanga, J.W.; Peek, G.J.; Arora, R.C. Venovenous extracorporeal membrane oxygenation in obese patients. JTCVS Tech. 2021, 10, 335–348. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rudym, D.; Pham, T.; Rackley, C.R.; Grasselli, G.; Anderson, M.; Baldwin, M.R.; Beitler, J.; Agerstrand, C.; Serra, A.; Winston, L.A.; et al. Mortality in Patients with Obesity and Acute Respiratory Distress Syndrome Receiving Extracorporeal Membrane Oxygenation: The Multicenter ECMObesity Study. Am. J. Respir. Crit. Care Med. 2023, 208, 685–694. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Swol, J.; Buchwald, D.; Dudda, M.; Strauch, J.; Schildhauer, T.A. Veno-venous extracorporeal membrane oxygenation in obese surgical patients with hypercapnic lung failure. Acta Anaesthesiol. Scand. 2014, 58, 534–538. [Google Scholar] [CrossRef] [PubMed]
- Kon, Z.N.; Dahi, S.; Evans, C.F.; Byrnes, K.A.; Bittle, G.J.; Wehman, B.; Rector, R.P.; McCormick, B.M.; Herr, D.L.; Sanchez, P.G.; et al. Class III Obesity is Not a Contraindication to Venovenous Extracorporeal Membrane Oxygenation Support. Ann. Thorac. Surg. 2015, 100, 1855–1860. [Google Scholar] [CrossRef] [PubMed]
- Stelfox, H.T.; Ahmed, S.B.; Ribeiro, R.A.; Gettings, E.M.; Pomerantsev, E.; Schmidt, U. Hemodynamic monitoring in obese patients: The impact of body mass index on cardiac output and stroke volume. Crit. Care Med. 2006, 34, 1243–1246. [Google Scholar] [CrossRef]
- Lemmens, H.J.M.; Bernstein, D.P.; Brodsky, J.B. Estimating Blood Volume in Obese and Morbidly Obese Patients. Obes. Surg. 2006, 16, 773–776. [Google Scholar] [CrossRef]
- Shashaty, M.G.S.; Stapleton, R.D. Physiological and Management Implications of Obesity in Critical Illness. Ann. Am. Thorac. Soc. 2014, 11, 1286–1297. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pelosi, P.; Croci, M.; Ravagnan, I.; Tredici, S.; Pedoto, A.; Lissoni, A.; Gattinoni, L. The Effects of Body Mass on Lung Volumes, Respiratory Mechanics, and Gas Exchange During General Anesthesia. Anesth. Analg. 1998, 87, 654–660. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, N.D. Oxygen in the ICU: Too much of a good thing? JAMA 2016, 316, 1553–1554. [Google Scholar] [CrossRef]
- ARDSnet. NIH NHLBI ARDS Clinical Network Mechanical Ventilation Protocol Summary. Available online: http://www.ardsnet.org/files/ventilator_protocol_2008-07.pdf (accessed on 25 February 2025).
- Duan, E.H.; Adhikari, N.K.J.; D’aragon, F.; Cook, D.J.; Mehta, S.; Alhazzani, W.; Goligher, E.; Charbonney, E.; Arabi, Y.M.; Karachi, T.; et al. Management of Acute Respiratory Distress Syndrome and Refractory Hypoxemia. A Multicenter Observational Study. Ann. Am. Thorac. Soc. 2017, 14, 1818–1826. [Google Scholar] [CrossRef] [PubMed]
- Tasaka, S.; Ohshimo, S.; Takeuchi, M.; Yasuda, H.; Ichikado, K.; Tsushima, K.; Egi, M.; Hashimoto, S.; Shime, N.; Saito, O.; et al. ARDS Clinical Practice Guideline 2021. J. Intensiv. Care 2022, 10, 32. [Google Scholar] [CrossRef] [PubMed]
- Barrot, L.; Asfar, P.; Mauny, F.; Winiszewski, H.; Montini, F.; Badie, J.; Quenot, J.-P.; Pili-Floury, S.; Bouhemad, B.; Louis, G.; et al. Liberal or Conservative Oxygen Therapy for Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2020, 382, 999–1008. [Google Scholar] [CrossRef] [PubMed]
- Panwar, R.; Hardie, M.; Bellomo, R.; Barrot, L.; Eastwood, G.M.; Young, P.J.; Capellier, G.; Harrigan, P.W.J.; Bailey, M. Conservative versus Liberal Oxygenation Targets for Mechanically Ventilated Patients. A Pilot Multicenter Randomized Controlled Trial. Am. J. Respir. Crit. Care Med. 2016, 193, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Girardis, M.; Busani, S.; Damiani, E.; Donati, A.; Rinaldi, L.; Marudi, A.; Morelli, A.; Antonelli, M.; Singer, M. Effect of conservative vs. conventional oxygen therapy on mortality among patients in an intensive care unit: The oxygen-ICU randomized clinical trial. JAMA. 2016, 316, 1583–1589. [Google Scholar] [CrossRef]
- Nielsen, F.M.; Klitgaard, T.L.; Siegemund, M.; Laake, J.H.; Thormar, K.M.; Cole, J.M.; Aagaard, S.R.; Bunzel, A.-M.G.; Vestergaard, S.R.; Langhoff, P.K.; et al. Lower vs Higher Oxygenation Target and Days Alive Without Life Support in COVID-19: The HOT-COVID Randomized Clinical Trial. JAMA 2024, 331, 1185–1194. [Google Scholar] [CrossRef]
- Messaï, E.; Bouguerra, A.; Harmelin, G.; Di Lascio, G.; Cianchi, G.; Bonacchi, M. A new formula for determining arterial oxygen satura-tion during venovenous extracorporeal oxygenation. Intensive Care Med. 2013, 39, 327–334. [Google Scholar] [CrossRef]
- Schmidt, M.; Tachon, G.; Devilliers, C.; Muller, G.; Hekimian, G.; Bréchot, N.; Merceron, S.; Luyt, C.E.; Trouillet, J.-L.; Chastre, J.; et al. Blood oxygenation and decarboxylation determinants during venovenous ECMO for respiratory failure in adults. Intensiv. Care Med. 2013, 39, 838–846. [Google Scholar] [CrossRef] [PubMed]
- Reddy, Y.N.; Melenovsky, V.; Redfield, M.M.; Nishimura, R.A.; Borlaug, B.A. High-Output Heart Failure: A 15-Year Experience. J. Am. Coll. Cardiol. 2016, 68, 473–482. [Google Scholar] [CrossRef] [PubMed]
- Straaten, H.M.O.-V.; Jansen, P.G.M.; Velthuis, H.T.; Beenakkers, I.C.M.; Stoutenbeek, C.P.; van Deventer, S.J.H.; Sturk, A.; Eysman, L.; Wildevuur, C.R.H. Increased oxygen consumption after cardiac surgery is associated with the inflammatory response to endotoxemia. Intensiv. Care Med. 1996, 22, 294–300. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Chaturvedi, A. Imaging adults on extracorporeal membrane oxygenation (ECMO). Insights Into Imaging 2014, 5, 731–742. [Google Scholar] [CrossRef]
- Gajkowski, E.F.; Herrera, G.; Hatton, L.; Antonini, M.V.; Vercaemst, L.; Cooley, E. ELSO Guidelines for Adult and Pediatric Extracorporeal Membrane Oxygenation Circuits. ASAIO J. 2022, 68, 133–152. [Google Scholar] [CrossRef]
- Gehron, J.; Bandorski, D.; Mayer, K.; Böning, A. The Impact of Recirculation on Extracorporeal Gas Exchange and Patient Oxygenation during Veno-Venous Extracorporeal Membrane Oxygenation—Results of an Observational Clinical Trial. J. Clin. Med. 2023, 12, 416. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pooth, J.; Förster, J.K.; Benk, C.; Diel, P.; Brixius, S.J.; Maier, S.; Supady, A.; Wengenmayer, T.; Staudacher, D.L.; Haimerl, G.; et al. Impact of Cannulation Strategy and Extracorporeal Blood Flow on Recirculation During Veno-Venous Extracorporeal Membrane Oxygenation. Artif. Organs, 2025; online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Parker, L.P.; Marcial, A.S.; Brismar, T.B.; Broman, L.M.; Wittberg, L.P. Hemodynamic and recirculation performance of dual lumen cannulas for venovenous extracorporeal membrane oxygenation. Sci. Rep. 2023, 13, 7472. [Google Scholar] [CrossRef]
- Schoeberl, A.-K.; Staudacher, D.; Kawashima, M.; Fischer, C.; Cypel, M.; Buchtele, N.; Staudinger, T.; Aigner, C.; Hoetzenecker, K.; Schweiger, T. Al-ternative venous access sites for dual-lumen extracorporeal membrane oxygenation cannulation. Interdiscip. Cardio-Vasc. Thorac. Surg. 2024, 38, ivae060. [Google Scholar]
- Morgan, M.; Hopwood, M.J.; Dunbar, J.A. Shared guidelines and protocols to achieve better health outcomes for people living with serious mental illness. Med. J. Aust. 2022, 217 (Suppl. S7), S34–S35. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zhou, Y.; Holets, S.R.; Li, M.; Meyer, T.J.; Latuche, L.J.R.; Oeckler, R.A.; Bohman, J.K. The Impact of a Standardized Refractory Hypoxemia Protocol on Outcome of Subjects Receiving Venovenous Extracorporeal Membrane Oxygenation. Respir. Care 2021, 66, 837–844. [Google Scholar] [CrossRef] [PubMed]
- De Moraes, A.G.; Holets, S.R.; Tescher, A.N.; Elmer, J.; Arteaga, G.M.; Schears, G.; Patch, R.K.; Bohman, J.K.; Oeckler, R.A. The Clinical Effect of an Early, Protocolized Approach to Mechanical Ventilation for Severe and Refractory Hypoxemia. Respir. Care 2020, 65, 413–419. [Google Scholar] [CrossRef] [PubMed]
- Acute Respiratory Distress Syndrome Network; Brower, R.G.; Matthay, M.A.; Morris, A.; Schoenfeld, D.; Thompson, B.T.; Wheeler, A. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N. Engl. J. Med. 2000, 342, 1301–1308. [Google Scholar] [CrossRef] [PubMed]
- Grasselli, G.; Calfee, C.S.; Camporota, L.; Poole, D.; Amato, M.B.P.; Antonelli, M.; Arabi, Y.M.; Baroncelli, F.; Beitler, J.R.; Bellani, G.; et al. ESICM guidelines on acute respiratory distress syndrome: Definition, phenotyping and respiratory support strategies. Intensiv. Care Med. 2023, 49, 727–759. [Google Scholar] [CrossRef] [PubMed]
- Guervilly, C.; Fournier, T.; Chommeloux, J.; Arnaud, L.; Pinglis, C.; Baumstarck, K.; Boucekine, M.; Valera, S.; Sanz, C.; Adda, M.; et al. Ultra-lung-protective ventilation and biotrauma in severe ARDS patients on veno-venous extracorporeal membrane oxygenation: A randomized controlled study. Crit. Care 2022, 26, 383. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rozencwajg, S.; Guihot, A.; Franchineau, G.; Lescroat, M.; Bréchot, N.; Hékimian, G.; Lebreton, G.; Autran, B.; Luyt, C.-E.; Combes, A.; et al. Ultra-Protective Ventilation Reduces Biotrauma in Patients on Venovenous Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome. Crit. Care Med. 2019, 47, 1505–1512. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Chen, C.; Hu, D.; Sun, F.; Zhang, G.; Zhang, Z.; Dong, Y.; Lv, J.; Mei, Y.; Chen, X. Randomized controlled trial of ultra-protective vs. protective ventilation strategy in veno-arterial extracorporeal membrane oxygenation patients with refractory cardiogenic shock: A study protocol for the ultra-ECMO trial. Front. Cardiovasc. Med. 2023, 10, 1092653. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nishikimi, M.; Ohshimo, S.; Hamaguchi, J.; Fujizuka, K.; Hagiwara, Y.; Anzai, T.; Ishii, J.; Ogata, Y.; Aokage, T.; Ikeda, T.; et al. High versus low positive end-expiratory pressure setting in patients receiving veno-venous extracorporeal membrane oxygenation support for severe acute respiratory distress syndrome: Study protocol for the multicentre, randomised ExPress SAVER Trial. BMJ Open 2023, 13, e072680. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pensier, J.; de Jong, A.; Hajjej, Z.; Molinari, N.; Carr, J.; Belafia, F.; Chanques, G.; Futier, E.; Azoulay, E.; Jaber, S. Effect of lung recruitment maneuver on oxygenation, physiological parameters and mortality in acute respiratory distress syndrome patients: A systematic review and meta-analysis. Intensiv. Care Med. 2019, 45, 1691–1702. [Google Scholar] [CrossRef] [PubMed]
- Dianti, J.; Tisminetzky, M.; Ferreyro, B.L.; Englesakis, M.; Del Sorbo, L.; Sud, S.; Talmor, D.; Ball, L.; Meade, M.; Hodgson, C.; et al. Association of Positive End-Expiratory Pressure and Lung Recruitment Selection Strategies with Mortality in Acute Respiratory Distress Syndrome: A Systematic Review and Network Meta-analysis. Am. J. Respir. Crit. Care Med. 2022, 205, 1300–1310. [Google Scholar] [CrossRef] [PubMed]
- Writing Group for the Alveolar Recruitment for Acute Respiratory Distress Syndrome Trial (ART) Investigators. Effect of lung recruitment and titrated positive end-expiratory pressure (PEEP) vs. low PEEP on mortality in patients with acute respiratory distress syndrome: A randomized clinical trial. JAMA 2017, 318, 1335–1345. [Google Scholar] [CrossRef] [PubMed]
- Arnal, J.-M.; Paquet, J.; Wysocki, M.; Demory, D.; Donati, S.; Granier, I.; Corno, G.; Durand-Gasselin, J. Optimal duration of a sustained inflation recruitment maneuver in ARDS patients. Intensiv. Care Med. 2011, 37, 1588–1594. [Google Scholar] [CrossRef] [PubMed]
- Riva, D.; Contador, R.; Baez-Garcia, C.; Xisto, D.; Cagido, V.; Martini, S.; Morales, M.; Rocco, P.; Faffe, D.; Zin, W. Recruitment maneuver: RAMP versus CPAP pressure profile in a model of acute lung injury. Respir. Physiol. Neurobiol. 2009, 169, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Hodgson, C.; Goligher, E.C.; Young, M.E.; Keating, J.L.; Holland, A.E.; Romero, L.; Bradley, S.J.; Tuxen, D. Recruitment manoeuvres for adults with acute respiratory distress syndrome receiving mechanical ventilation. Cochrane Database Syst. Rev. 2016, 2018, CD006667. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cui, Y.; Cao, R.; Wang, Y.; Li, G. Lung Recruitment Maneuvers for ARDS Patients: A Systematic Review and Meta-Analysis. Respiration 2019, 99, 264–276. [Google Scholar] [CrossRef] [PubMed]
- Hodgson, C.L.; Cooper, D.J.; Arabi, Y.; King, V.; Bersten, A.; Bihari, S.; Brickell, K.; Davies, A.; Fahey, C.; Fraser, J.; et al. Maximal Recruitment Open Lung Ventilation in Acute Respiratory Distress Syndrome (PHARLAP). A Phase II, Multicenter Randomized Controlled Clinical Trial. Am. J. Respir. Crit. Care Med. 2019, 200, 1363–1372. [Google Scholar] [CrossRef] [PubMed]
- Santiago, R.D.S.; Droghi, M.T.; Fumagalli, J.; Marrazzo, F.; Florio, G.; Grassi, L.G.; Gomes, S.; Morais, C.C.A.; Ramos, O.P.S.; Bottiroli, M.; et al. High Pleural Pressure Prevents Alveolar Overdistension and Hemodynamic Collapse in Acute Respiratory Distress Syndrome with Class III Obesity. A Clinical Trial. Am. J. Respir. Crit. Care Med. 2021, 203, 575–584. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Amato, M.B.P.; Meade, M.O.; Slutsky, A.S.; Brochard, L.; Costa, E.L.V.; Schoenfeld, D.A.; Stewart, T.E.; Briel, M.; Talmor, D.S.; Mercat, A.; et al. Driving Pressure and Survival in the Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2015, 372, 747–755. [Google Scholar] [CrossRef] [PubMed]
- Deniel, G.; Dhelft, F.; Lancelot, S.; Orkisz, M.; Roux, E.; Mouton, W.; Benzerdjeb, N.; Richard, J.-C.; Bitker, L. Pulmonary inflammation decreases with ultra-protective ventilation in experimental ARDS under VV-ECMO: A positron emission tomography study. Front. Med. 2024, 11, 1338602. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hermann, M.; König, S.; Laxar, D.; Krall, C.; Kraft, F.; Krenn, K.; Baumgartner, C.; Tretter, V.; Maleczek, M.; Hermann, A.; et al. Low-Frequency Ventilation May Facilitate Weaning in Acute Respiratory Distress Syndrome Treated with Extracorporeal Membrane Oxygenation: A Randomized Controlled Trial. J. Clin. Med. 2024, 13, 5094. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pirrone, M.; Fisher, D.; Chipman, D.; Imber, D.A.E.; Corona, J.; Mietto, C.; Kacmarek, R.M.; Berra, L. Recruitment Maneuvers and Positive End-Expiratory Pressure Titration in Morbidly Obese ICU Patients. Crit. Care Med. 2016, 44, 300–307. [Google Scholar] [CrossRef] [PubMed]
- Mezidi, M.; Daviet, F.; Chabert, P.; Hraiech, S.; Bitker, L.; Forel, J.-M.; Yonis, H.; Gragueb, I.; Dhelft, F.; Papazian, L.; et al. Transpulmonary pressures in obese and non-obese COVID-19 ARDS. Ann. Intensiv. Care 2020, 10, 129. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bime, C.; Fiero, M.; Lu, Z.; Oren, E.; Berry, C.E.; Parthasarathy, S.; Garcia, J.G. High Positive End-Expiratory Pressure Is Associated with Improved Survival in Obese Patients with Acute Respiratory Distress Syndrome. Am. J. Med. 2016, 130, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Spina, S.; Mantz, L.; Xin, Y.; Moscho, D.C.; Santiago, R.R.D.S.; Grassi, L.; Nova, A.; Gerard, S.E.; Bittner, E.A.; Fintelmann, F.J.; et al. The pleural gradient does not reflect the superimposed pressure in patients with class III obesity. Crit. Care 2024, 28, 306. [Google Scholar] [CrossRef] [PubMed]
- De Jong, A.; Cossic, J.; Verzilli, D.; Monet, C.; Carr, J.; Conseil, M.; Monnin, M.; Cisse, M.; Belafia, F.; Molinari, N.; et al. Impact of the driving pressure on mortality in obese and non-obese ARDS patients: A retrospective study of 362 cases. Intensiv. Care Med. 2018, 44, 1106–1114. [Google Scholar] [CrossRef] [PubMed]
- Beitler, J.R.; Sarge, T.; Banner-Goodspeed, V.M.; Gong, M.N.; Cook, D.; Novack, V.; Loring, S.H.; Talmor, D. Effect of Titrating Positive End-Expiratory Pressure (PEEP) With an Esophageal Pressure–Guided Strategy vs an Empirical High PEEP-Fio2 Strategy on Death and Days Free from Mechanical Ventilation Among Patients With Acute Respiratory Distress Syndrome: A Randomized Clinical Trial. JAMA 2019, 321, 846–857. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sarge, T.; Baedorf-Kassis, E.; Banner-Goodspeed, V.; Novack, V.; Loring, S.H.; Gong, M.N.; Cook, D.; Talmor, D.; Beitler, J.R.; EPVent-2 Study Group. Effect of Esophageal Pressure–guided Positive End-Expiratory Pressure on Survival from Acute Respiratory Distress Syndrome: A Risk-based and Mechanistic Reanalysis of the EPVent-2 Trial. Am. J. Respir. Crit. Care Med. 2021, 204, 1153–1163. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Terry, C.M.; Brinton, D.; Simpson, A.N.; Kirchoff, K.; Files, D.C.; Carter, G.; Ford, D.W.M.; Goodwin, A.J.M. Elevated Driving Pressure and Elastance Does Not Increase In-Hospital Mortality Among Obese and Severely Obese Patients with Ventilator Dependent Respiratory Failure. Crit. Care Explor. 2022, 4, e0811. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Guérin, C.; Reignier, J.; Richard, J.-C.; Beuret, P.; Gacouin, A.; Boulain, T.; Mercier, E.; Badet, M.; Mercat, A.; Baudin, O.; et al. Prone Positioning in Severe Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2013, 368, 2159–2168. [Google Scholar] [CrossRef]
- De Jong, A.; Molinari, N.; Sebbane, M.; Prades, A.; Fellow, N.; Futier, E.; Jung, B.; Chanques, G.; Jaber, S. Feasibility and Effectiveness of Prone Position in Morbidly Obese Patients With ARDS: A case-control clinical study. Chest 2013, 143, 1554–1561. [Google Scholar] [CrossRef] [PubMed]
- Petit, M.; Fetita, C.; Gaudemer, A.; Treluyer, L.; Lebreton, G.; Franchineau, G.; Hekimian, G.; Chommeloux, J.; de Chambrun, M.P.; Brechot, N.; et al. Prone-Positioning for Severe Acute Respiratory Distress Syndrome Requiring Extracorporeal Membrane Oxygenation. Crit. Care Med. 2021, 50, 264–274. [Google Scholar] [CrossRef] [PubMed]
- Rilinger, J.; Zotzmann, V.; Bemtgen, X.; Schumacher, C.; Biever, P.M.; Duerschmied, D.; Kaier, K.; Stachon, P.; Mühlen, C.v.Z.; Zehender, M.; et al. Prone positioning in severe ARDS requiring extracorporeal membrane oxygenation. Crit. Care 2020, 24, 397. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tong, H.; Pan, F.; Zhang, X.; Jia, S.; Vashisht, R.; Chen, K.; Wang, Q. Effect of prone positioning on survival in adult patients receiving venovenous extracorporeal membrane oxygenation for acute respiratory distress syndrome: A prospective multicenter randomized controlled study. J. Thorac. Dis. 2024, 16, 1368–1377. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wang, R.; Tang, X.; Li, X.; Li, Y.; Liu, Y.; Li, T.; Zhao, Y.; Wang, L.; Li, H.; Li, M.; et al. Early reapplication of prone position during venovenous ECMO for acute respiratory distress syndrome: A prospective observational study and propensity-matched analysis. Ann. Intensiv. Care 2024, 14, 127. [Google Scholar] [CrossRef] [PubMed]
- Giani, M.; Rezoagli, E.; Guervilly, C.; Rilinger, J.; Duburcq, T.; Petit, M.; Textoris, L.; Garcia, B.; Wengenmayer, T.; Grasselli, G.; et al. Prone positioning during venovenous extracorporeal membrane oxygenation for acute respiratory distress syndrome: A pooled individual patient data analysis. Crit. Care 2022, 26, 8. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.; Hajage, D.; Lebreton, G.; Dres, M.; Guervilly, C.; Richard, J.C.; Sonneville, R.; Winiszewski, H.; Muller, G.; Beduneau, G.; et al. Prone Positioning During Extracorporeal Membrane Oxygenation in Patients with Severe ARDS: The PRONECMO Randomized Clinical Trial. JAMA 2023, 330, 2343–2353, Erratum in JAMA 2024, 331, 446. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Afshari, A.; Brok, J.; Møller, A.M.; Wetterslev, J. Inhaled Nitric Oxide for Acute Respiratory Distress Syndrome and Acute Lung Injury in Adults and Children: A systematic review with meta-analysis and trial sequential analysis. Anesth. Analg. 2011, 112, 1411–1421. [Google Scholar] [CrossRef] [PubMed]
- Troncy, E.; Collet, J.-P.; Shapiro, S.; Guimond, J.-G.; Blair, L.; Ducruet, T.; Francoeur, M.; Charbonneau, M.; Blaise, G. Inhaled Nitric Oxide in Acute Respiratory Distress Syndrome: A pilot randomized controlled study. Am. J. Respir. Crit. Care Med. 1998, 157, 1483–1488. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.W.; Zimmerman, J.L.; Dellinger, R.P.; Straube, R.C.; Criner, G.J.; Davis, J.K.; Kelly, K.M.; Smith, T.C.; Small, R.J. Low-Dose Inhaled Nitric Oxide in Patients with Acute Lung InjuryA Randomized Controlled Trial. JAMA 2004, 291, 1603–1609. [Google Scholar] [CrossRef] [PubMed]
- Narula, P.; Xu, J.; Kazzaz, J.A.; Robbins, C.G.; Davis, J.M.; Horowitz, S.; Sparkman, L.; Boggaram, V.; Salinas, D.; Berhane, K.; et al. Synergistic cytotoxicity from nitric oxide and hyperoxia in cultured lung cells. Am. J. Physiol. Cell. Mol. Physiol. 1998, 274, L411–L416. [Google Scholar] [CrossRef] [PubMed]
- Stoll, S.E.; Böttiger, B.W.; Dusse, F.; Leister, N.; Leupold, T.; Menzel, C.; Overbeek, R.; Mathes, A. Impact of Inhaled Nitric Oxide (iNO) on the Outcome of COVID-19 Associated ARDS. J. Clin. Med. 2024, 13, 5981. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Isha, S.; Balasubramanian, P.; Hanson, A.J.; Jonna, S.; Raavi, L.; Khadka, S.; Vasudhar, A.; De Frias, J.S.; Jenkins, A.; Balavenkataraman, A.; et al. Impact of low dose inhaled nitric oxide treatment in spontaneously breathing and intubated COVID-19 patients: A retrospective propensity-matched study. Crit. Care 2024, 28, 344. [Google Scholar] [CrossRef] [PubMed]
- Alqahtani, J.S.; Aldhahir, A.M.; Al Ghamdi, S.S.; AlBahrani, S.; AlDraiwiesh, I.A.; Alqarni, A.A.; Latief, K.; Raya, R.P.; Oyelade, T. Inhaled Nitric Oxide for Clinical Management of COVID-19: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 12803. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dessap, A.M.; Papazian, L.; Schaller, M.; Nseir, S.; Megarbane, B.; Haudebourg, L.; Timsit, J.-F.; Teboul, J.-L.; Kuteifan, K.; Gainnier, M.; et al. Inhaled nitric oxide in patients with acute respiratory distress syndrome caused by COVID-19: Treatment modalities, clinical response, and outcomes. Ann. Intensiv. Care 2023, 13, 57. [Google Scholar] [CrossRef] [PubMed]
- Di Fenza, R.; Shetty, N.S.; Gianni, S.; Parcha, V.; Giammatteo, V.; Fakhr, B.S.; Tornberg, D.; Wall, O.; Harbut, P.; Lai, P.S.; et al. High-Dose Inhaled Nitric Oxide in Acute Hypoxemic Respiratory Failure Due to COVID-19: A Multicenter Phase II Trial. Am. J. Respir. Crit. Care Med. 2023, 208, 1293–1304. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gebistorf, F.; Karam, O.; Wetterslev, J.; Afshari, A. Inhaled nitric oxide for acute respiratory distress syndrome (ARDS) in children and adults. Cochrane Database Syst. Rev. 2016, 2016, CD002787. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Muenster, S.; Nadal, J.; Schewe, J.-C.; Ehrentraut, H.; Kreyer, S.; Putensen, C.; Ehrentraut, S.F. Analysis of Patients with Severe ARDS on VV ECMO Treated with Inhaled NO: A Retrospective Observational Study. J. Clin. Med. 2024, 13, 1555. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Crow, J.; Lindsley, J.; Cho, S.-M.; Wang, J.; Lantry, J.H.I.; Kim, B.S.; Tahsili-Fahadan, P. Analgosedation in Critically Ill Adults Receiving Extracorporeal Membrane Oxygenation Support. ASAIO J. 2022, 68, 1419–1427. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Marik, P.E.; Kaufman, D. The effects of neuromuscular paralysis on systemic and splanchnic oxygen utilization in mechanically ventilated patients. Chest 1996, 109, 1038–1042. [Google Scholar] [CrossRef]
- DeGrado, J.R.; Hohlfelder, B.; Ritchie, B.M.; Anger, K.E.; Reardon, D.P.; Weinhouse, G.L. Evaluation of sedatives, analgesics, and neuromuscular blocking agents in adults receiving extracorporeal membrane oxygenation. J. Crit. Care 2017, 37, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Kressin, C.; Bastin, M.T.; Ather, A.; Gopinath, A.; Srour, H.; Schadler, A.; Pandya, K. Cisatracurium Continuous Infusion Versus No Neuromuscular Blockade for Acute Respiratory Distress Syndrome on Venovenous Extracorporeal Membrane Oxygenation. J. Clin. Pharmacol. 2021, 61, 1415–1420. [Google Scholar] [CrossRef] [PubMed]
- National Heart, Lung, and Blood Institute PETAL Clinical Trials Network; Moss, M.; Huang, D.T.; Brower, R.G.; Ferguson, N.D.; Ginde, A.A.; Gong, M.N.; Grissom, C.K.; Gundel, S.; Hayden, D.; et al. Early Neuromuscular Blockade in the Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2019, 380, 1997–2008. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Papazian, L.; Forel, J.-M.; Gacouin, A.; Penot-Ragon, C.; Perrin, G.; Loundou, A.; Jaber, S.; Arnal, J.-M.; Perez, D.; Seghboyan, J.-M.; et al. Neuromuscular Blockers in Early Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2010, 363, 1107–1116. [Google Scholar] [CrossRef] [PubMed]
- Savoie-White, F.H.; Tremblay, L.; Menier, C.A.; Duval, C.; Bergeron, F.; Tadrous, M.; Tougas, J.; Guertin, J.R.; Ugalde, P.A. The use of early neuromuscular blockage in acute respiratory distress syndrome: A systematic review and meta-analyses of randomized clinical trials. Heart Lung 2022, 57, 186–197. [Google Scholar] [CrossRef] [PubMed]
- Hunsicker, O.; Materne, L.; Bünger, V.; Krannich, A.; Balzer, F.; Spies, C.; Francis, R.C.; Weber-Carstens, S.; Menk, M.; Graw, J.A. Lower versus higher hemoglobin threshold for transfusion in ARDS patients with and without ECMO. Crit. Care 2020, 24, 697. [Google Scholar] [CrossRef] [PubMed]
- Voelker, M.T.; Busch, T.; Bercker, S.; Fichtner, F.; Kaisers, U.X.; Laudi, S. Restrictive Transfusion Practice During Extracorporeal Membrane Oxygenation Therapy for Severe Acute Respiratory Distress Syndrome. Artif. Organs 2014, 39, 374–378. [Google Scholar] [CrossRef] [PubMed]
- Agerstrand, C.L.; Burkart, K.M.; Abrams, D.C.; Bacchetta, M.D.; Brodie, D. Blood conservation in extracorporeal membrane oxygenation for acute res-piratory distress syndrome. Ann. Thorac. Surg. 2015, 99, 590–595. [Google Scholar] [CrossRef] [PubMed]
- Doyle, A.J.M.; Richardson, C.M.; Sanderson, B.B.; Wong, K.M.; Wyncoll, D.M.; Camporota, L.; Barrett, N.A.M.; Hunt, B.J.; Retter, A.M. Restrictive Transfusion Practice in Adults Receiving Venovenous Extracorporeal Membrane Oxygenation: A Single-Center Experience. Crit. Care Explor. 2020, 2, e0077. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Martucci, G.; Schmidt, M.; Agerstrand, C.; Tabatabai, A.; Tuzzolino, F.; Giani, M.; Ramanan, R.; Grasselli, G.; Schellongowski, P.; Riera, J.; et al. Transfusion practice in patients receiving VV ECMO (PROTECMO): A prospective, multicentre, observational study. Lancet Respir. Med. 2022, 11, 245–255. [Google Scholar] [CrossRef] [PubMed]
- Jamadarkhana, S.; Gopal, S. Clonidine in adults as a sedative agent in the intensive care unit. J. Anaesthesiol. Clin. Pharmacol. 2010, 26, 439–445. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- McRaven, D.R.; Kroetz, F.W.; Kioschos, J.; Kirkendall, W.M. The effect of clonidine on hemodynamics in hypertensive patients. Am. Heart J. 1971, 81, 482–489. [Google Scholar] [CrossRef] [PubMed]
- Staudacher, D.L.; Wengenmayer, T.; Schmidt, M. Beta-blockers in refractory hypoxemia on venovenous extracorporeal membrane oxygenation: A double-edged sword. Crit. Care 2023, 27, 360. [Google Scholar] [CrossRef]
- Bommiasamy, A.K.; Zakhary, B.; Ran, R. Beta-blockade in V-V ECMO. Crit. Care 2024, 28, 139. [Google Scholar] [CrossRef]
- Pappalardo, F.; Zangrillo, A.; Pieri, M.; Landoni, G.; Morelli, A.; Stefani, M.; Guarracino, F. Esmolol administration in patients with VV ECMO: Why not? J. Cardiothorac. Vasc. Anesth. 2013, 27, e40. [Google Scholar] [CrossRef] [PubMed]
- Bunge, J.J.; Diaby, S.; Valle, A.L.; Bakker, J.; Gommers, D.; Vincent, J.-L.; Creteur, J.; Taccone, F.S.; Miranda, D.R. Safety and efficacy of beta-blockers to improve oxygenation in patients on veno-venous ECMO. J. Crit. Care 2019, 53, 248–252. [Google Scholar] [CrossRef] [PubMed]
- Guarracino, F.; Zangrillo, A.; Ruggeri, L.; Pieri, M.; Calabrò, M.G.; Landoni, G.; Stefani, M.; Doroni, L.; Pappalardo, F. β-Blockers to Optimize Peripheral Oxygenation During Extracorporeal Membrane Oxygenation: A Case Series. J. Cardiothorac. Vasc. Anesth. 2012, 26, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.S.; Keller, S.P.; Dodd-O, J.M. A case series evaluating the effect of esmolol therapy to treat hypoxemia in COVID-19 patients on VV-ECMO. Int. J. Artif. Organs 2023, 46, 381–383. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Krupnik, A.; Dhaliwal, J.; Hatton, K.; Harris, A.; White, A.; Schadler, A.; Ather, A. 121: Safety and Efficacy of Metoprolol Use to Improve Oxygenation in COVID-19 Patients on Venovenous Extracorporeal Membrane Oxygenation. ASAIO J. 2023, 69 (Suppl. S3), 31. [Google Scholar] [CrossRef]
- Wood, T.; Thoresen, M. Physiological responses to hypothermia. Semin. Fetal Neonatal Med. 2015, 20, 87–96. [Google Scholar] [CrossRef] [PubMed]
- Moreau, A.; Levy, B.; Annoni, F.; Lorusso, R.; Su, F.; Belliato, M.; Taccone, F.S. The use of induced hypothermia in extracorporeal membrane oxygenation: A narrative review. Resusc. Plus 2023, 13, 100360. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Napp, L.C.; Kühn, C.; Hoeper, M.M.; Vogel-Claussen, J.; Haverich, A.; Schäfer, A.; Bauersachs, J. Cannulation strategies for percutaneous extracorporeal membrane oxygenation in adults. Clin. Res. Cardiol. 2015, 105, 283–296. [Google Scholar] [CrossRef] [PubMed]
- Bojic, A.; Steiner, I.; Gamper, J.; Schellongowski, P.; Lamm, W.; Hermann, A.; Riss, K.; Robak, O.; Staudinger, T. Supraclavicular Approach to the Subclavian Vein as an Alternative Venous Access Site for ECMO Cannulae? A Retrospective Comparison. ASAIO J. 2017, 63, 679–683. [Google Scholar] [CrossRef] [PubMed]
- Gothner, M.; Buchwald, D.; Strauch, J.T.; Schildhauer, T.A.; Swol, J. The use of double lumen cannula for veno-venous ECMO in trauma patients with ARDS. Scand. J. Trauma Resusc. Emerg. Med. 2015, 23, 30. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Banfi, C.; Pozzi, M.; Siegenthaler, N.; Brunner, M.-E.; Tassaux, D.; Obadia, J.-F.; Bendjelid, K.; Giraud, R. Veno-venous extracorporeal membrane oxygenation: Cannulation techniques. J. Thorac. Dis. 2016, 8, 3762–3773. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mauri, T.; Spinelli, E.; Ibrahim, Q.; Rochwerg, B.; Lorusso, R.; Tonna, J.E.; Price, S.; MacLaren, G.; Pesenti, A.; Slutsky, A.S.; et al. Impact of Drainage Cannula Size and Blood Flow Rate on the Outcome of Patients Receiving Venovenous Extracorporeal Membrane Oxygenation for Acute Respiratory Distress Syndrome: An ELSO Registry Analysis. Am. J. Respir. Crit. Care Med. 2023, 208, 105–107. [Google Scholar] [CrossRef] [PubMed]
- Spinelli, E.; Giani, M.; Slobod, D.; Pavlovsky, B.; di Pierro, M.; Crotti, S.; Lissoni, A.; Foti, G.; Grasselli, G.; Mauri, T. Physiologic Effects of Extracorporeal Membrane Oxygenation in Patients with Severe Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2024, 210, 629–638. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Szułdrzyński, K.; Kowalewski, M.; Jankowski, M.; Staromłyński, J.; Prokop, J.; Pasierski, M.; Chudziński, K.; Drobiński, D.; Martucci, G.; Lorusso, R.; et al. Effects of adding the second drainage cannula in severely hypoxemic patients supported with VV ECMO due to COVID-19-associated ARDS. Artif. Organs 2023, 47, 1622–1631. [Google Scholar] [CrossRef] [PubMed]
- Dave, S.B.; Leiendecker, E.; Creel-Bulos, C.; Miller, C.F.; Boorman, D.W.; Javidfar, J.; Attia, T.; Daneshmand, M.; Jabaley, C.S.; Caridi-Schieble, M. Outcomes following additional drainage during veno-venous extracorporeal membrane oxygenation: A single-center retrospective study. Perfusion 2024, 02676591241249609. [Google Scholar] [CrossRef] [PubMed]
- Miyazato, A.; Kondo, Y.; Seki, K.; Kumakawa, Y.; Ishihara, T.; Sueyoshi, K.; Okamoto, K.; Tanaka, H. Use of two parallel oxygenators during veno-venous extracorporeal membrane oxygenation in a patient with severe obesity and COVID-19 pneumonia. Perfusion 2022, 38, 1738–1741. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hurtado, S.; Sepulveda, V.; Godoy, C.; Bahamondes, R.; Kattan, E.; Mendez, M.; Besa, S. Parallel oxygenators in the same circuit for refractory hypoxemia on veno-venous extracorporeal membrane oxygenation. A 3-patient series. Perfusion 2023, 39, 1715–1721. [Google Scholar] [CrossRef]
- Leloup, G.; Rozé, H.; Calderon, J.; Ouattara, A. Use of two oxygenators during extracorporeal membrane oxygenator for a patient with acute respiratory distress syndrome, high-pressure ventilation, hypercapnia, and traumatic brain injury. Br. J. Anaesth. 2017, 107, 1014–1015. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Seadler, B.; Alagoa, K.; Zelten, J.; Ubert, H.A.; Durham, L. 1510: Dual oxygenators for refractory hypercapnia and hypoxia on ecmo: An underutilized therapy? Crit. Care Med. 2023, 52, S726. [Google Scholar] [CrossRef]
- Melro, L.M.G.; Santos, Y.d.A.P.d.; Júnior, L.C.M.C.; Besen, B.A.M.P.; Zigaib, R.; Forte, D.N.; Mendes, P.V.; Park, M. Exploring the association of two oxygenators in parallel or in series during respiratory support using extracorporeal membrane oxygenation. Rev. Bras. Ter. Intensiv. 2022, 34, 402–409. [Google Scholar] [CrossRef]
- Omlor, A.J.; Caspari, S.; Omlor, L.S.; Jungmann, A.M.; Krawczyk, M.; Schmoll, N.; Mang, S.; Seiler, F.; Muellenbach, R.M.; Bals, R.; et al. Comparison of Serial and Parallel Connections of Membrane Lungs against Refractory Hypoxemia in a Mock Circuit. Membranes 2023, 13, 809. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Madhani, S.P.; May, A.G.; Frankowski, B.J.; Burgreen, G.W.; Federspiel, W.J. Blood Recirculation Enhances Oxygenation Ef-ficiency of Artificial Lungs. ASAIO J. 2020, 66, 565–570. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.H.; Kim, J.W.; Kim, S.H.; Moon, S.H.; Yang, J.H.; Jung, J.J.; Cha, H.J.; Choi, J.Y.; Lee, C.E.; Heo, W.; et al. The serial connection of two extracorporeal membrane oxygenators for patient with refractory hypoxemia. Heart Lung 2021, 50, 853–856. [Google Scholar] [CrossRef] [PubMed]
- Kwon, O.J.; Rojo, M.; Dobaria, V.; Tedesco, J.; Schwartz, J.P. The utility of parallel venovenous extracorporeal membrane oxygenation circuits for refractory hypoxemia in severely burned patients: A case report. JTCVS Tech. 2022, 15, 126–129. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Malik, A.; Shears, L.L.; Zubkus, D.; Kaczorowski, D.J. Parallel circuits for refractory hypoxemia on venovenous extracorporeal membrane oxygenation. J. Thorac. Cardiovasc. Surg. 2016, 153, e49–e51. [Google Scholar] [CrossRef]
- Shoni, M.; Lazar, S.; Jackson, A.; Tonetti, M.K.; Horak, J.; Gutsche, J.; Augoustides, J.G.; Marchant, B.E.; Fernando, R.J.; Jelly, C.A.; et al. Parallel Venovenous Extracorporeal Membrane Oxygenation Circuits for Refractory Hypoxemia in a Super-Super-Obese Patient. J. Cardiothorac. Vasc. Anesth. 2023, 37, 1304–1314. [Google Scholar] [CrossRef] [PubMed]
- Patel, Y.J.; Stokes, J.W.; Gannon, W.D.; Francois, S.A.; Wu, W.K.; Rice, T.W.; Bacchetta, M. Extracorporeal Membrane Oxygenation Circuits in Parallel for Refractory Hypoxemia in COVID-19: A Case Series. ASAIO J. 2022, 68, 1002–1009. [Google Scholar] [CrossRef] [PubMed]
- Patel, Y.J.; Gannon, W.D.; Francois, S.A.; Stokes, J.W.; Tipograf, Y.; Landsperger, J.S.; Semler, M.W.; Casey, J.D.; Rice, T.W.; Bacchetta, M. Extracorporeal membrane oxygenation circuits in parallel for refractory hypoxemia in patients with COVID-19. J. Thorac. Cardiovasc. Surg. 2022, 167, 746–754.e1. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Aubron, C.; Cheng, A.C.; Pilcher, D.; Leong, T.; Magrin, G.; Cooper, D.J.; Scheinkestel, C.; Pellegrino, V. Factors associated with outcomes of patients on extracorporeal membrane oxygenation support: A 5-year cohort study. Crit. Care 2013, 17, R73. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Falk, L.; Sallisalmi, M.; Lindholm, J.A.; Lindfors, M.; Frenckner, B.; Broomé, M.; Broman, L.M. Differential hypoxemia during venoarterial extracorporeal membrane oxygenation. Perfusion 2019, 34 (Suppl. S1), 22–29. [Google Scholar] [CrossRef] [PubMed]
- Saxena, A.; Curran, J.; Ahmad, D.; Nasher, N.; Miyamoto, T.; Brailovsky, E.; Shah, M.K.; Rajapreyar, I.N.; Rame, J.E.; Loforte, A.; et al. Utilization and outcomes of V-AV ECMO: A systematic review and meta-analysis. Artif. Organs 2023, 47, 1559–1566. [Google Scholar] [CrossRef] [PubMed]
- Cha, H.J.; Kim, J.W.; Kang, D.H.; Moon, S.H.; Kim, S.H.; Jung, J.J.; Yang, J.H.; Byun, J.H. Conversion to Veno-arteriovenous Extracorporeal Membrane Oxygenation for Differential Hypoxia. J. Chest Surg. 2023, 56, 274–281. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Navas-Blanco, J.R.; Lifgren, S.A.; Dudaryk, R.; Scott, J.; Loebe, M.; Ghodsizad, A. Parallel veno-venous and veno-arterial extracorporeal membrane circuits for coexisting refractory hypoxemia and cardiovascular failure: A case report. BMC Anesthesiol. 2021, 21, 77. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ka, E.S.; Lee, J.; Ahn, S.; Kim, Y.H. Parallel Venovenous and Venoarterial Extracorporeal Membrane Oxygenation for Respiratory Failure and Cardiac Dysfunction in a Patient with Coronavirus Disease 2019: A Case Report. J. Chest Surg. 2024, 57, 225–229. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kluis, A.; Rawitscher, D.; Afzal, A.M.; DiMaio, J.M.; George, T.J. Impella 5.5 and venovenous extracorporeal membrane oxygenation as a bridge to ventricular assist device in cardiopulmonary failure. Bayl. Univ. Med. Cent. Proc. 2023, 36, 208–210. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Encarnación-Martínez, U.; Torres-Pulido, A.; Lazcano-Díaz, E.A.; Manzur-Sandoval, D.; Baeza-Herrera, L.A.; González-Ruiz, F.J.; Jiménez-Rodríguez, G.M.; Rojas-Velasco, G. Circulatory support with triple cannulation V-PaA ECMO in a patient with acute right ventricular failure and refractory hypoxemia secondary to diffuse alveolar hemorrhage: A case report. Respir. Med. Case Rep. 2024, 50, 102064. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lucchini, A.; Elli, S.; De Felippis, C.; Greco, C.; Mulas, A.; Ricucci, P.; Fumagalli, R.; Foti, G. The evaluation of nursing workload within an Italian ECMO Centre: A retrospective observational study. Intensiv. Crit. Care Nurs. 2019, 55, 102749. [Google Scholar] [CrossRef] [PubMed]
- Combes, A.; Brodie, D.; Bartlett, R.; Brochard, L.; Brower, R.; Conrad, S.; De Backer, D.; Fan, E.; Ferguson, N.; Fortenberry, J.; et al. Position Paper for the Organization of Extracorporeal Membrane Oxygenation Programs for Acute Respiratory Failure in Adult Patients. Am. J. Respir. Crit. Care Med. 2014, 190, 488–496. [Google Scholar] [CrossRef] [PubMed]
- Ross, P.; Sheldrake, J.; Ilic, D.; Watterson, J.; Berkovic, D.; Pilcher, D.; Udy, A.; Hodgson, C.L. An exploration of intensive care nurses’ perceptions of workload in providing extracorporeal membrane oxygenation (ECMO) support: A descriptive qualitative study. Aust. Crit. Care 2024, 37, 585–591. [Google Scholar] [CrossRef] [PubMed]
- Jones, T.L.; Hamilton, P.; Murry, N. Unfinished nursing care, missed care, and implicitly rationed care: State of the science review. Int. J. Nurs. Stud. 2015, 52, 1121–1137. [Google Scholar] [CrossRef] [PubMed]
- Harvey, M.J.; Gaies, M.G.; Prosser, L.A. US and International In-Hospital Costs of Extracorporeal Membrane Oxygenation: A Systematic Review. Appl. Health Econ. Health Policy 2015, 13, 341–357. [Google Scholar] [CrossRef] [PubMed]
- Mishra, V.; Svennevig, J.L.; Bugge, J.F.; Andresen, S.; Mathisen, A.; Karlsen, H.; Khushi, I.; Hagen, T.P. Cost of extracorporeal membrane oxygenation: Evidence from the Rikshospitalet University Hospital, Oslo, Norway. Eur. J. Cardio-Thorac. Surg. 2009, 37, 339–342. [Google Scholar] [CrossRef] [PubMed]
- Uwumiro, F.; Otabor, N.; Okpujie, V.; Osiogo, E.O.; Osemwota, O.F.; Abesin, O.; Utibe, M.A.; Ekeh, N.; Onyekwe, A.E.; Fasoranti-Sowemimo, O.F.; et al. Rates, Outcomes, and Resource Burden of Extracorporeal Membrane Oxygenation Use in Hospitalizations in the United States During the Pandemic. Cureus 2024, 16, e54081. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
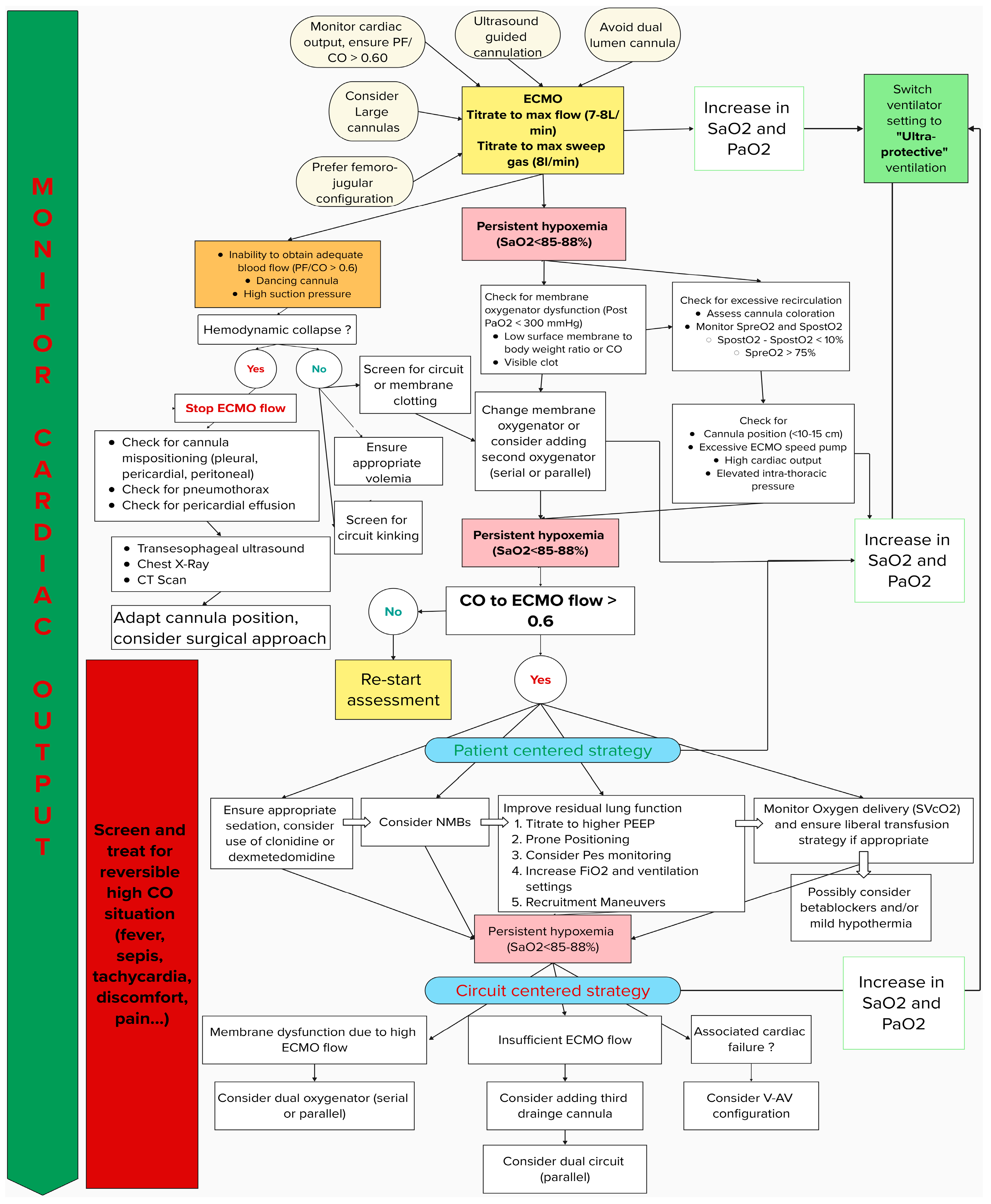
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).