
Safety and Efficacy of Ritlecitinib for the Treatment of Patients with Alopecia Areata: A Systematic Review and Meta-Analysis of Controlled Trials


Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy
2.3. Study Selection
2.4. Data Extraction and Management
2.5. Methodological Quality Assessment of Included Studies
2.6. Statistical Analysis
3. Results
3.1. Current Study Characteristics
3.2. Quality Assessment of Included Studies
3.3. Meta-Analysis
3.3.1. Efficacy of Ritlecitinib on SALT Score
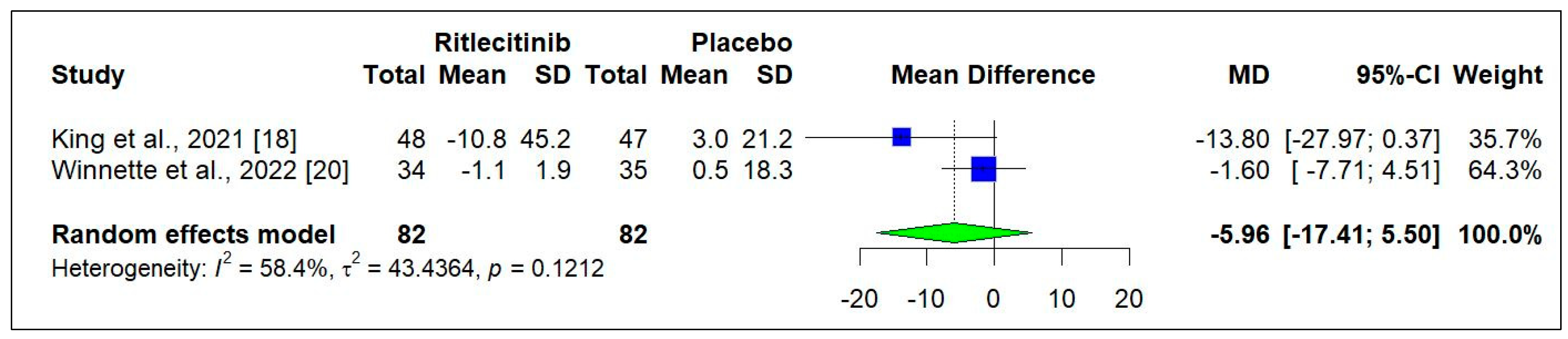
3.3.2. Efficacy of Ritlecitinib on AASIS Score
3.3.3. Efficacy of Ritlecitinib on PGIC Score
3.3.4. Safety of Ritlecitinib
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AA | Alopecia areata |
| AU | Alopecia universalis |
| AT | Alopecia totalis |
| RCTs | Randomized controlled trials |
| PRISMA | Preferred Reporting Items for Systematic Review |
| PICOS | Population, intervention, comparison, outcome, and study design |
| FPS | First-pass screening |
| RoB | Risk of bias |
| CI | Confidence interval |
| SD | Standard deviations |
| AASIS | Alopecia Areata Symptom Impact Scale |
| PGIC | Patient Global Impression of Change |
| US | United States |
| JAK | Janus kinase |
| NSV | Non-segmental vitiligo |
| AAPPO | Alopecia Areata Patient Priority Outcomes |
References
- Dhurat, R.; Sharma, R. A practical approach to the treatment of alopecia areata. Indian Dermatol. Online J. 2022, 13, 725–728. [Google Scholar] [PubMed]
- Fukumoto, T.; Fukumoto, R.; Magno, E.; Oka, M.; Nishigori, C.; Horita, N. Treatments for alopecia areata: A systematic review and network meta-analysis. Dermatol. Ther. 2021, 34, e14916. [Google Scholar] [CrossRef] [PubMed]
- Kwon, O.; Senna, M.M.; Sinclair, R.; Ito, T.; Dutronc, Y.; Lin, C.Y.; Yu, G.; Chiasserini, C.; McCollam, J.; Wu, W.S.; et al. Efficacy and safety of baricitinib in patients with severe alopecia areata over 52 weeks of continuous therapy in two phase III trials (BRAVE-AA1 and BRAVE-AA2). Am. J. Clin. Dermatol. 2023, 24, 443–451. [Google Scholar] [CrossRef]
- Lintzeri, D.A.; Constantinou, A.; Hillmann, K.; Ghoreschi, K.; Vogt, A.; Blume-Peytavi, U. Alopecia areata-Current understanding and management. J. Dtsch. Dermatol. Ges. 2022, 20, 59–90. [Google Scholar] [CrossRef]
- Vu, B.K.; Tuson, H.; Harricharan, S.; Law, E.H.; Wosik, K.; Tran, H.; Wolk, R.; Neary, M.P. Epidemiology of Alopecia Areata Across Global Regions-A Systematic Literature Review. Value Health 2022, 25, S202. [Google Scholar] [CrossRef]
- Wang, H.; Pan, L.; Wu, Y. Epidemiological trends in alopecia areata at the global, regional, and national levels. Front. Immunol. 2022, 13, 874677. [Google Scholar] [CrossRef]
- Sibbald, C.; Castelo-Soccio, L. Review of global epidemiology data for alopecia areata highlights gaps and a call for action. Br. J. Dermatol. 2024, 191, 315–316. [Google Scholar] [CrossRef]
- Darwin, E.; Hirt, P.A.; Fertig, R.; Doliner, B.; Delcanto, G.; Jimenez, J.J. Alopecia areata: Review of epidemiology, clinical features, pathogenesis, and new treatment options. Int. J. Trichology 2018, 10, 51–60. [Google Scholar] [CrossRef]
- King, B.A.; Senna, M.M.; Ohyama, M.; Tosti, A.; Sinclair, R.D.; Ball, S.; Ko, J.M.; Glashofer, M.; Pirmez, R.; Shapiro, J. Defining severity in alopecia areata: Current perspectives and a multidimensional framework. Dermatol. Ther. 2022, 12, 825–834. [Google Scholar] [CrossRef]
- Villasante Fricke, A.C.; Miteva, M. Epidemiology and burden of alopecia areata: A systematic review. Clin. Cosmet. Investig. Dermatol. 2015, 8, 397–403. [Google Scholar]
- Alsantali, A. Alopecia areata: A new treatment plan. Clin. Cosmet. Investig. Dermatol. 2011, 4, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Fernando, T.; Goldman, R.D. Corticosteroids for alopecia areata in children. Can. Fam. Physician 2020, 66, 499–501. [Google Scholar] [PubMed]
- Seetharam, K.A. Alopecia areata: An update. Indian J. Dermatol. Venereol. Leprol. 2013, 79, 563–575. [Google Scholar] [CrossRef]
- Wang, E.C.; Dai, Z.; Christiano, A.M. Novel therapies for alopecia areata: The era of rational drug development. J. Allergy Clin. Immunol. 2018, 141, 499–504. [Google Scholar] [CrossRef]
- Guttman-Yassky, E.; Pavel, A.B.; Diaz, A.; Zhang, N.; Del Duca, E.; Estrada, Y.; King, B.; Banerjee, A.; Banfield, C.; Cox, L.A.; et al. Ritlecitinib and brepocitinib demonstrate significant improvement in scalp alopecia areata biomarkers. J. Allergy Clin. Immunol. 2022, 149, 1318–1328. [Google Scholar] [CrossRef]
- Hordinsky, M.; Hebert, A.A.; Gooderham, M.; Kwon, O.; Murashkin, N.; Fang, H.; Harada, K.; Law, E.; Wajsbrot, D.; Takiya, L.; et al. Efficacy and safety of ritlecitinib in adolescents with alopecia areata: Results from the ALLEGRO phase 2b/3 randomized, double-blind, placebo-controlled trial. Pediatr. Dermatol. 2023, 40, 1003–1009. [Google Scholar] [CrossRef]
- Hordinsky, M.K.; Hebert, A.; Gooderham, M. Efficacy and safety of the oral JAK3/TEC inhibitor ritlecitinib in adolescents with alopecia areata: Results from the ALLEGRO Phase 2b/3 randomized, double-blind, placebo-controlled trial. J. Am. Acad. Dermatol. 2022, 87, AB51. [Google Scholar] [CrossRef]
- King, B.; Guttman-Yassky, E.; Peeva, E.; Banerjee, A.; Sinclair, R.; Pavel, A.B.; Zhu, L.; Cox, L.A.; Craiglow, B.; Chen, L.; et al. A phase 2a randomized, placebo-controlled study to evaluate the efficacy and safety of the oral Janus kinase inhibitors ritlecitinib and brepocitinib in alopecia areata: 24-week results. J. Am. Acad. Dermatol. 2021, 85, 379–387. [Google Scholar] [CrossRef]
- King, B.; Szepietowski, J.C.; Farrant, P. Safety of the oral JAK3/TEC inhibitor ritlecitinib (PF-06651600) in patients with alopecia areata: Results from the ALLEGRO phase 2b/3, randomized, double-blind, placebo-controlled trial. J. Am. Acad. Dermatol. 2022, 87, AB106. [Google Scholar] [CrossRef]
- Winnette, R.; Banerjee, A.; Sikirica, V.; Peeva, E.; Wyrwich, K. Characterizing the relationships between patient-reported outcomes and clinician assessments of alopecia areata in a phase 2a randomized trial of ritlecitinib and brepocitinib. J. Eur. Acad. Dermatol. Venereol. 2022, 36, 602–609. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Cumpston, M.; Li, T.; Page, M.J.; Chandler, J.; Welch, V.A.; Higgins, J.P.; Thomas, J. Updated guidance for trusted systematic reviews: A new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst. Rev. 2019, 10, ED000142. [Google Scholar] [CrossRef] [PubMed]
- ClinicalTrials.gov. Placebo-Controlled Safety Study of Ritlecitinib (PF-06651600) in Adults with Alopecia Areata [Study Record]. 2020. Available online: https://classic.clinicaltrials.gov/ct2/show/NCT04517864 (accessed on 11 April 2024).
- King, B.; Zhang, X.; Harcha, W.G.; Szepietowski, J.C.; Shapiro, J.; Lynde, C.; Mesinkovska, N.A.; Zwillich, S.H.; Napatalung, L.; Wajsbrot, D.; et al. Efficacy and safety of ritlecitinib in adults and adolescents with alopecia areata: A randomised, double-blind, multicentre, phase 2b–3 trial. Lancet 2023, 401, 1518–1529. [Google Scholar] [CrossRef]
- Mesinkovska, N.; King, B.; Zhang, X.; Guttman-Yassky, E.; Magnolo, N.; Sinclair, R.; Mizuashi, M.; Shapiro, J.; Peeva, E.; Banerjee, A.; et al. Efficacy of the oral JAK3/TEC inhibitor ritlecitinib (PF-06651600) in patients with alopecia areata over 48 weeks: Results from the ALLEGRO Phase 2b/3 randomized, double-blind, placebo-controlled trial. J. Am. Acad. Dermatol. 2022, 87, AB54. [Google Scholar] [CrossRef]
- Piliang, M.; Lynde, C.; King, B.; Mirmirani, P.; Sinclair, R.; Senna, M.; Forman, S.; Bordone, L.; De La Cueva Dobao, P.; Wolk, R.; et al. Sustained scalp, eyebrow, and eyelash hair regrowth with ritlecitinib through Week 48 in patients with alopecia areata: Post hoc analysis of the ALLEGRO phase 2b/3 study. J. Am. Acad. Dermatol. 2023, 89, AB91. [Google Scholar] [CrossRef]
- Senna, M.; Forman, S.; Bordone, L.; De La Cueva Dobao, P.; Wolk, R.; Zwillich, S.H.; Wajsbrot, D.; Ahmed, H.M.; Takiya, L. Scalp, eyebrow, and eyelash hair regrowth with continued ritlecitinib treatment among patients with alopecia areata without target efficacy response at Week 24: Post hoc analysis of the ALLEGRO phase 2b/3 study. J. Am. Acad. Dermatol. 2023, 89, AB221. [Google Scholar] [CrossRef]
- Sinclair, R.; Mesinkovska, N. Improvement in patient-reported hair loss outcome measures in patients with alopecia areata treated with ritlecitinib: 48-week results from the ALLEGRO phase 2B/3 randomized, double-blind, placebo-controlled trial. J. Am. Acad. Dermatol. 2022, 87, AB69. [Google Scholar] [CrossRef]
- King, B.; Soung, J.; Tziotzios, C.; Rudnicka, L.; Joly, P.; Gooderham, M.; Sinclair, R.; Mesinkovska, N.A.; Paul, C.; Gong, Y.; et al. Integrated safety analysis of ritlecitinib in adolescent patients with alopecia areata from the randomized, placebo-controlled ALLEGRO phase 2b/3 and ongoing open-label phase 3 ALLEGRO-LT studies. Am. J. Clin. Dermatol. 2024, 25, 689. [Google Scholar] [CrossRef]
- Thaçi, D.; Tziotzios, C.; Ito, T.; Ko, J.; Karadağ, A.S.; Fang, H.; Edwards, R.A.; Bonfanti, G.; Wolk, R.; Tran, H.; et al. Hair Loss Profiles and Ritlecitinib Efficacy in Patients with Alopecia Areata: Post Hoc Analysis of the ALLEGRO Phase 2b/3 Study. Dermatol. Ther. 2023, 13, 2621–2634. [Google Scholar] [CrossRef]
- Ramírez-Marín, H.A.; Tosti, A. Evaluating the Therapeutic Potential of Ritlecitinib for the Treatment of Alopecia Areata. Drug Des. Devel. Ther. 2023, 16, 363–374. [Google Scholar] [CrossRef] [PubMed]
- Guttman-Yassky, E.; Del Duca, E.; Da Rosa, J.C.; Bar, J.; Ezzedine, K.; Ye, Z.; He, W.; Hyde, C.; Hassan-Zahraee, M.; Yamaguchi, Y.; et al. Improvements in immune/melanocyte biomarkers with JAK3/TEC family kinase inhibitor ritlecitinib in vitiligo. J. Allergy. Clin. Immunol. 2024, 153, 161–172.e8. [Google Scholar] [CrossRef] [PubMed]
- King, B.; Soung, J.; Tziotzios, C.; Rudnicka, L.; Joly, P.; Gooderham, M.; Sinclair, R.; Mesinkovska, N.A.; Paul, C.; Gong, Y.; et al. Integrated safety analysis of Ritlecitinib, an oral JAK3/TEC family kinase inhibitor, for the treatment of alopecia areata from the ALLEGRO clinical trial program. Am. J. Clin. Dermatol. 2024, 25, 299–314. [Google Scholar] [CrossRef] [PubMed]
- Anderson, S.; Cavaletti, G.; Hood, L.J.; Polydefkis, M.; Herrmann, D.N.; Rance, G.; King, B.; McMichael, A.J.; Senna, M.M.; Kim, B.S.; et al. A phase 2a study investigating the effects of ritlecitinib on brainstem auditory evoked potentials and intraepidermal nerve fiber histology in adults with alopecia areata. Pharmacol. Res. Perspect. 2024, 12, e1204. [Google Scholar] [CrossRef]
- ClinicalTrials.gov. Pre-Approval Single-Patient Expanded Access for Ritlecitinib (PF-06651600) [Study Record]. 2024. Available online: https://clinicaltrials.gov/study/NCT05522556?intr=ritlecitinib&cond=Alopecia%20Areata&rank=1 (accessed on 11 April 2024).









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author ID | Year | Type of Publication | NCT ID | Study Design | Dose of Ritlecitinib # | Blinded/Open | Study Duration | Total Number of Participants |
|---|---|---|---|---|---|---|---|---|
| Guttman-Yassky et al., 2022 [15] | 2022 | Journal article | NCT02974868 | RCT | NR | Blinded | 24 weeks | 46 |
| Hordinsky et al., 2023 [16] | 2023 | Journal article | NCT03732807 | RCT | 10 or 30 or 50 mg | Blinded | 24 weeks | 105 |
| King et al., 2021 [18] | 2021 | Journal article | NCT03732807 | RCT | 50 mg | Blinded | 24 weeks | 95 |
| King et al., 2023 [25] | 2023 | Journal article | NCT03732807 | RCT | 50 mg | Blinded | 24 weeks | 718 |
| Hordinsky et al., 2022 * [17] | 2022 | Abstract | NCT03732807 | RCT | 10 or 30 or 50 mg | Blinded | 24 weeks | 105 |
| King et al., 2022 * [19] | 2022 | Abstract | NCT03732807 | RCT | 10 or 30 or 50 mg | Blinded | 48 weeks | 715 |
| Mesinkovska et al., 2022 * [26] | 2022 | Abstract | NCT03732807 | RCT | 10 or 30 or 50 mg | Blinded | 24 weeks | 718 |
| Piliang et al., 2023 * [27] | 2023 | Abstract | NCT03732807 | RCT | 10 or 30 or 50 mg | Blinded | 24 weeks | 111 |
| Senna et al., 2023 * [28] | 2023 | Abstract | NCT03732807 | RCT | 10 or 30 or 50 mg | Blinded | 48 weeks | 359 |
| Sinclair et al., 2022 * [29] | 2022 | Abstract | NCT03732807 | RCT | 10 or 30 or 50 mg | Blinded | 48 weeks | 718 |
| Soung et al., 2023 * [30] | 2023 | Abstract | NCT03732807 | RCT | 50 mg | Blinded | 48 weeks | 105 |
| NCT04517864., 2020 [24] | 2020 | Clinical trial document | NCT04517864 | RCT | 50 mg | Blinded | 24 weeks | 71 |
| Winnette et al., 2022 [20] | 2022 | Journal article | NCT04517864 | RCT | 50 mg | Blinded | 24 weeks | 95 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alfahl, S.O.A.; Alzolibani, A. Safety and Efficacy of Ritlecitinib for the Treatment of Patients with Alopecia Areata: A Systematic Review and Meta-Analysis of Controlled Trials. J. Clin. Med. 2025, 14, 1817. https://doi.org/10.3390/jcm14061817
Alfahl SOA, Alzolibani A. Safety and Efficacy of Ritlecitinib for the Treatment of Patients with Alopecia Areata: A Systematic Review and Meta-Analysis of Controlled Trials. Journal of Clinical Medicine. 2025; 14(6):1817. https://doi.org/10.3390/jcm14061817
Chicago/Turabian StyleAlfahl, Samah Omar Ali, and Abdullateef Alzolibani. 2025. "Safety and Efficacy of Ritlecitinib for the Treatment of Patients with Alopecia Areata: A Systematic Review and Meta-Analysis of Controlled Trials" Journal of Clinical Medicine 14, no. 6: 1817. https://doi.org/10.3390/jcm14061817
APA StyleAlfahl, S. O. A., & Alzolibani, A. (2025). Safety and Efficacy of Ritlecitinib for the Treatment of Patients with Alopecia Areata: A Systematic Review and Meta-Analysis of Controlled Trials. Journal of Clinical Medicine, 14(6), 1817. https://doi.org/10.3390/jcm14061817