Abstract
Background/Objectives: This systematic review and meta-analysis aimed to determine the effectiveness of different aspirin dosages in preventing preeclampsia and its effect on other pregnancy-associated conditions. Methods: A comprehensive search of three databases (Pubmed, Embase, and Cochrane Library) was conducted for randomized controlled trials without time interval criteria, comparing aspirin at various doses with placebo or no specific preeclampsia prophylaxis. Eligible randomized controlled trials (RCTs) examined pregnant women receiving aspirin at any dose and time during their pregnancy, while the control group received a placebo, or placebo and a different dose of aspirin, or no specific preeclampsia prevention. No exclusion criteria were established regarding the population, study size, study site, or length of aspirin prophylaxis. Studies examining additional preventive medication (such as low-molecular-weight heparin) compared to aspirin without a placebo group were excluded. For all outcomes, the risk ratios (RRs) and mean differences (MDs) with 95% confidence intervals (CIs) were calculated. Meta-regression was performed to examine the relation between aspirin dosage and preeclampsia. Results: Based on the analysis of 31 studies involving 28,318 pregnancies and 20 studies involving 26,551 pregnancies, the early initiation of aspirin significantly reduced the overall incidence of preeclampsia (RR = 0.63, CI: 0.47–0.84) and perinatal death risk (RR = 0.82, CI: 0.72–0.93), respectively. Based on our meta-regression model, we could not establish a dose-dependent correlation between aspirin dosage and the risk of preeclampsia. Conclusions: Early-initiated aspirin prophylaxis is effective in preventing preeclampsia, without raising the incidence of placental abruption or increasing the amount of peripartum bleeding. No specific dose was superior to others; thus, further research should explore higher doses and focus on preterm preeclampsia, maternal–fetal complications, and bleeding.
1. Introduction
Preeclampsia is a pregnancy-related condition defined by new onset hypertension and significant proteinuria or end-organ dysfunction without proteinuria, after 20 weeks of gestation or postpartum, and is associated with different fetal and maternal complications [1].
Preeclampsia is the leading cause of maternal morbidity and mortality among all pregnancy-associated hypertensive disorders [1,2]. By affecting 5% to 7% of all pregnancies, it is responsible for over 70,000 maternal and 500,000 fetal deaths annually. Furthermore, preeclampsia is also the leading cause of cesarean section and prematurity in the United States [3,4,5].
Aspirin is a widely available and affordable medication with the potential to safely help pregnant women and neonates during pregnancy by preventing preeclampsia and its complications [6]. The first study examining aspirin as a possible preeclampsia prevention remedy was carried out in 1985 by Beaufils et al. [7], and since then, several randomized trials have investigated the prophylactic use of aspirin in preventing preeclampsia. However, over the years, different doses of aspirin from 25 mg to 150 mg were assessed in numerous well-designed trials with different baseline characteristics, examining different safety and efficacy outcomes, but the optimal dose still remains unclear. Based on the data provided, the timing of initiation for preeclampsia prevention is suggested at ≥12 weeks of gestation and ideally before 16 weeks [8]. Although the United States Preventive Services Taskforce (USPSTF) and the American College of Obstetricians and Gynecologists (ACOG) also recommend 81 mg of aspirin daily based on statistical analyses, recent meta-analyses [9,10] suggest that higher doses may be more efficient without elevating the risk of maternal and fetal adverse outcomes [11]. Likewise, for women identified as high risk, the recommendation delivered by The International Federation of Gynecology and Obstetrics (FIGO) in 2020 also suggests aspirin prophylaxis commencing at 11–14 weeks plus 6 days of gestation at a dose of ~150 mg until 36 weeks of gestation, when delivery occurs, or when preeclampsia is diagnosed [12].
In light of the controversies, our primary objective was to determine the effect of different aspirin doses on the incidence of preeclampsia. Additionally, we aimed to assess its impact on several secondary outcomes, including intrauterine growth restriction, preterm birth, gestational age at delivery, actual birth weight (neonate’s recorded weight at delivery explicitly excluding common alternative weight estimates, such as ultrasound-based fetal weight estimations, modeled projections, or retrospective estimations), placental abruption, peripartum bleeding, neonatal intensive care admission, and perinatal death, in which we did not separate intrauterine demise from early neonatal death. We hypothesized that higher doses of aspirin are more effective in preventing preeclampsia without raising the risk of fetal–maternal complications.
2. Materials and Methods
We reported our meta-analysis based on the recommendation of the PRISMA 2020 guideline [13] (see Supplementary Table S1), while we followed the Cochrane Handbook [14]. The study protocol was registered on PROSPERO (registration number CRD42021287369). In comparison to the original protocol, instead of a network meta-analysis, we performed a meta-analysis with a dose–response analysis to characterize the dose-dependent effect of aspirin on preeclampsia incidence.
2.1. Search Strategy
We conducted our systematic search in three databases (Pubmed, Embase, and Cochrane Library) on 3 November 2021 and updated on 29 January 2023, with the following search key: (aspirin OR “acetylsalicylic acid” OR ASA) AND (pregnancy OR pregnant OR gravidity OR preeclampsia OR eclampsia OR “preterm delivery” OR “preterm birth” OR “premature delivery” OR “premature birth” OR “fetal growth restriction” OR FGR OR “intrauterine growth restriction” OR IUGR OR “small for gestational age” OR SGA) AND random*. We did not use language, study type, or other filters during the search.
2.2. Selection Process
For the selection process, we used the Endnote v20 reference manager software (Clarivate Analytics, Philadelphia, PA, USA). After automatic and manual duplicate removal, we screened each entry based on title and abstract and then based it on the full text. The selection was made on each level by two independent review authors, while a third independent review author resolved disagreements.
2.3. Eligibility Criteria
Eligible randomized controlled trials (RCTs) examined pregnant women receiving aspirin at any dose and time during their pregnancy, while the control group received a placebo, a different dose of aspirin, or no specific preeclampsia prevention. Our primary outcome was preeclampsia, while we analyzed numerous secondary outcomes (see details below). No exclusion criteria were established regarding the population, study size, study site, or length of aspirin prophylaxis. We did not exclude studies due to initiation time differences. In addition, studies examining more doses of aspirin compared to placebo were also included. Studies examining additional preventive medication (such as low-molecular-weight heparin) compared to aspirin without a placebo group were excluded.
2.4. Data Collection Process and Data Items
Using a predefined datasheet, the following data were extracted: first author, year of publication, study population, gestational age at randomization, eligibility criteria, time and dosage of aspirin, type of control, and the total number of patients and events in the intervention and control groups.
2.5. Outcome Definitions
We checked each study’s outcome definitions and categorized them accordingly. Studies were included only if they explicitly reported outcome definitions, ensuring consistency in data extraction and analysis. For preeclampsia, we accepted definitions that included significant proteinuria or end-organ dysfunction without proteinuria [15]. For intrauterine growth restriction (IUGR), outcomes were classified based on different birth weight percentile thresholds, specifically evaluating below the 10th, 5th, and 3rd percentiles separately. Studies that did not specify a precise IUGR definition were included in the overall analysis. For preterm births, we applied a cut-off of delivery before 37 weeks. Birth weights were reported in grams, and gestational age was recorded in weeks. When studies originally reported gestational age in days, values were converted into weeks with two-decimal precision for consistency. Placental abruption was defined based on clinical symptoms or the pathological examination of the placenta. For perinatal death, we included both intrauterine fetal demise and neonatal mortality, defined as death within the first 28 days after delivery. Additionally, postpartum hemorrhage was analyzed as a separate safety outcome. These outcome definitions were applied consistently across all included studies to maintain methodological rigor and comparability.
2.6. Risk of Bias Assessment
Two authors independently assessed the risk of bias by utilizing the Cochrane risk-of-bias tool for randomized trials (RoB 2) tool [16]. A third review author resolved disagreements.
2.7. Synthesis Methods
All statistical analyses were made with R (R Core Team 2020, v4.0.3) using the meta (v5.2.0) package [17]. We calculated risk ratios (RRs) with 95% confidence intervals (CIs) for categorical variables, while for continuous variables, we calculated mean differences (MDs) with 95% CIs. The restricted maximum likelihood (REML) method was applied with a random-effects model [18]. We used forest plots to represent pooled and individual study results. I2 and χ2 tests assessed the statistical heterogeneity with a p-value < 0.1 as a threshold for a statistically significant difference. If at least ten studies were involved in the analysis, Egger’s test was used to assess publication bias. In addition to heterogeneity, a p-value < 0.05 was considered statistically significant in our analysis. We performed a meta-regression using a random-effects model to test the effects of different aspirin doses on the effect size. We used scatter plots to present individual study estimates and calculated the residual heterogeneity (I2 and χ2) and regression coefficients with a 95% CI. Subgroup analyses were carried out for all the different doses of daily aspirin. Furthermore, we divided the included studies based on the treatment’s start.
2.8. Evidence Synthesis
We followed the recommendation of the Grades of Recommendation, Assessment, Development, and Evaluation (GRADE) workgroup to evaluate the quality of evidence [19].
3. Results
3.1. Search and Selection
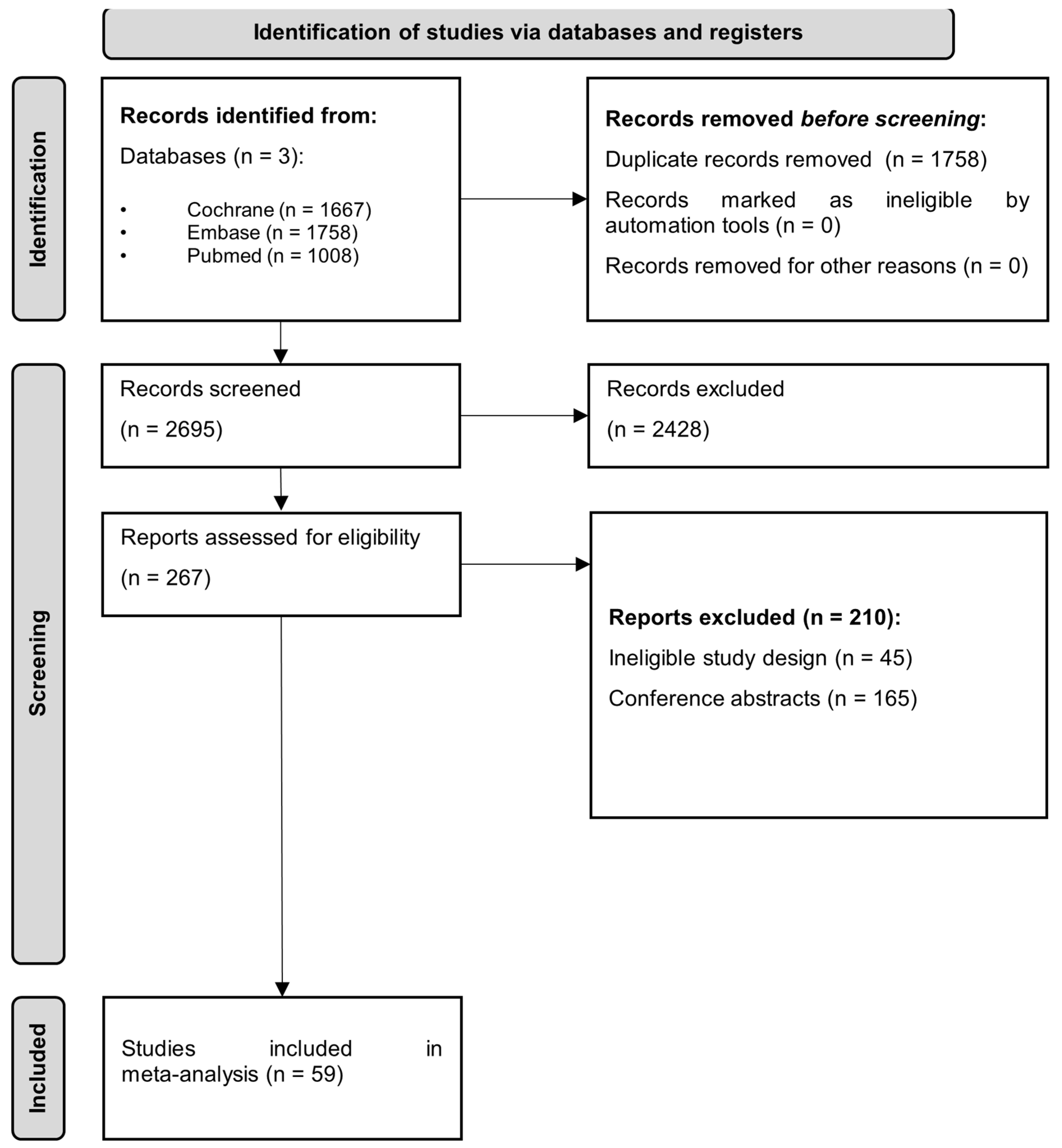
Using our search key, we identified 4433 studies. After duplicate removal, we screened 2675 articles based on title and abstract. Finally, we found 59 full-text articles eligible out of the 267 full-text studies assessed (Figure 1).
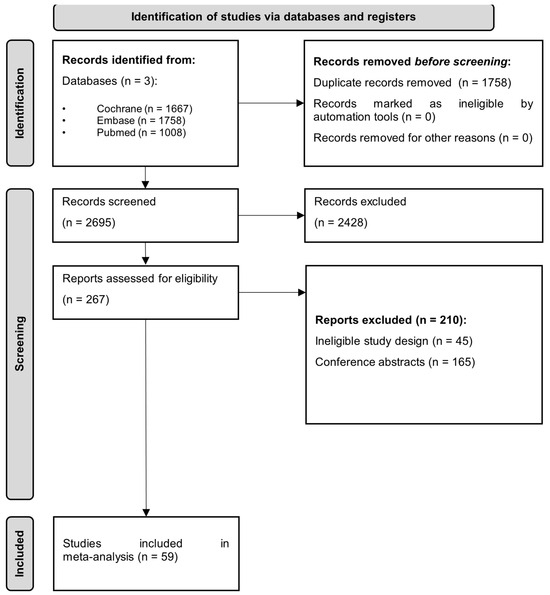
Figure 1.
PRISMA 2020 flowchart representing the study selection process.
3.2. Basic Characteristics of Included Studies
The baseline characteristics of the enrolled studies are detailed in Table 1. All the RCTs identified by our systematic search were involved, in which aspirin doses between 25 and 150 mg were compared to a placebo or the absence of any prophylaxis, and the initiation of aspirin varied from preconception to the third trimester. Among all involved articles, fifty-four examined moderate-to-high-risk preeclampsia pregnancies; three examined patients with unexplained recurring pregnancy loss; one examined patients with Alpha Fetoprotein levels below 2.5 without fetal anomalies; and one did not set up additional inclusion criteria for pregnancy for the examined population. Supplementary Tables S1 and S2 summarize the inclusion and exclusion criteria for the eligible studies.

Table 1.
Basic characteristics of included studies.
3.3. Primary Outcomes
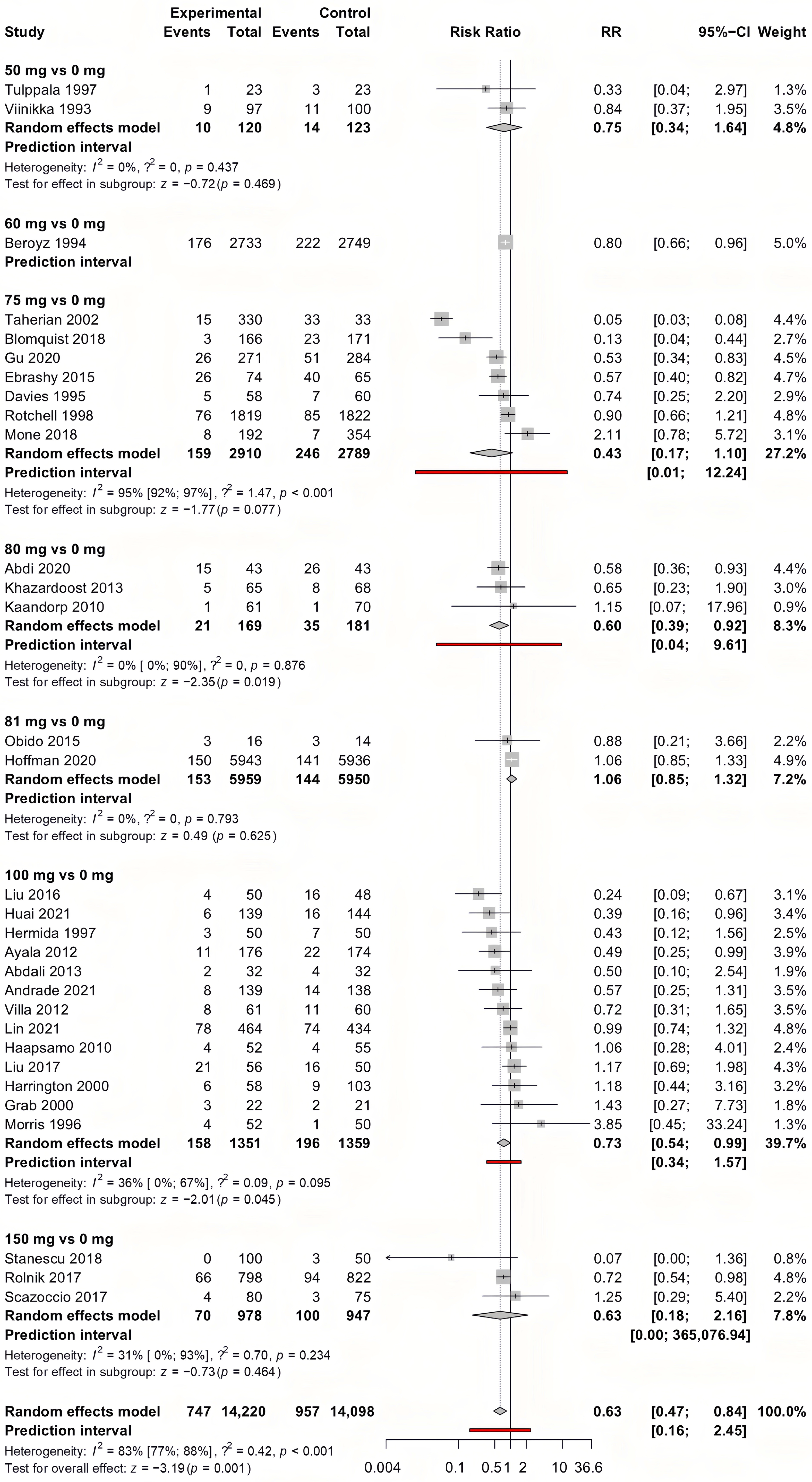
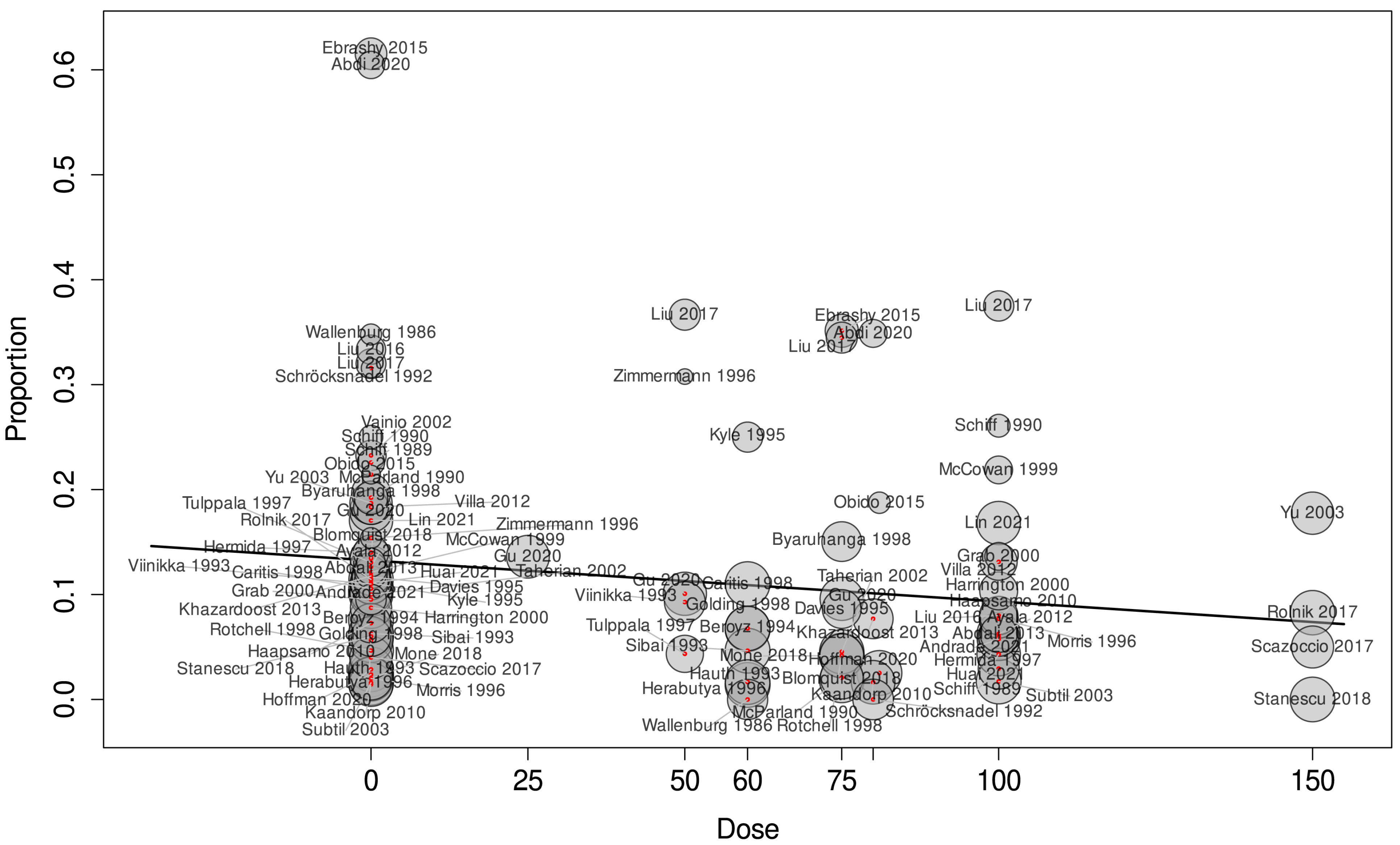
We summarized our results in Table 2. The detailed analysis for each analysis can be found in Supplementary Figures S2–S26. For the outcome of preeclampsia, early-initiated aspirin showed the most convincing results. As a result of the analysis of 31 studies involving 28,318 pregnancies, early-initiated aspirin significantly lowered the risk of preeclampsia (RR = 0.63, CI: 0.47–0.84) (Figure 2). As a result of the meta-regression analysis between the different aspirin doses and diagnosed preeclampsia (Figure 3), the correlation coefficient was −0.0006 (CI: −0.0012, 0, p = 0.049), with a high residual heterogeneity (I2 = 99.53%, p < 0.001), which means that the effect of the dose is insignificant. Aspirin initiated after the 20th week of gestation did not have a significant effect on preeclampsia prevention (RR = 0.67, CI: 0.35–1.28).
Table 2.
Summary of findings of aspirin prophylaxis at any dose.
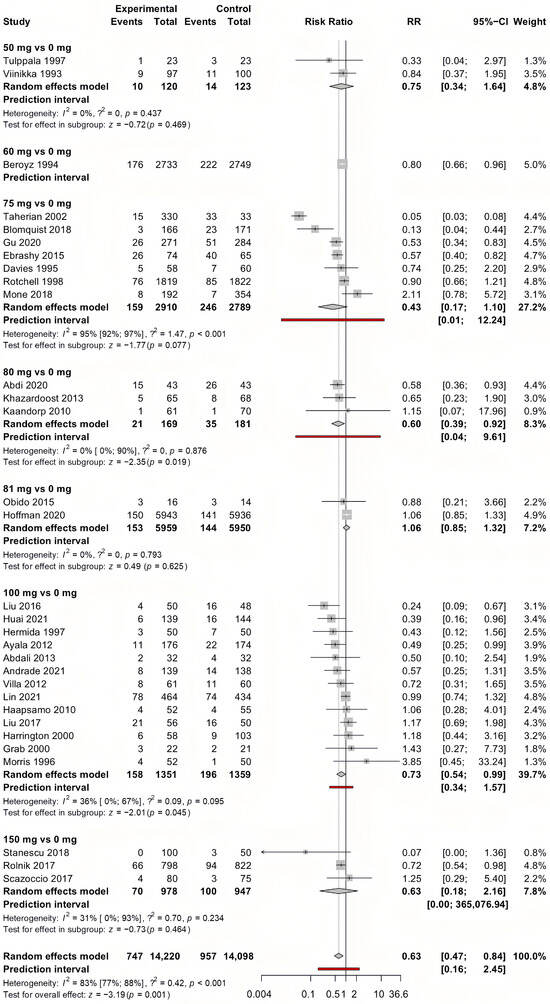
Figure 2.
Forest plot of the outcome preeclampsia with early-initiated (<week 20) aspirin. The experimental group received the indicated aspirin dose (e.g., “100 vs. 0” refers to 100 mg of aspirin vs. placebo or no aspirin). The control group consists of participants who received either a placebo or no specific preeclampsia prevention. Each row represents an individual study, with the number of events and total participants in both groups. The risk ratio (RR) and 95% confidence interval (CI) for each study are displayed, with the summary effect estimated using a random-effects model. Prediction intervals indicate the expected range of effects in future studies. Statistical heterogeneity is quantified using I2 and τ2 values [20,21,24,25,30,31,34,36,37,38,39,40,44,45,46,48,49,50,52,53,54,56,60,62,63,65,66,74].
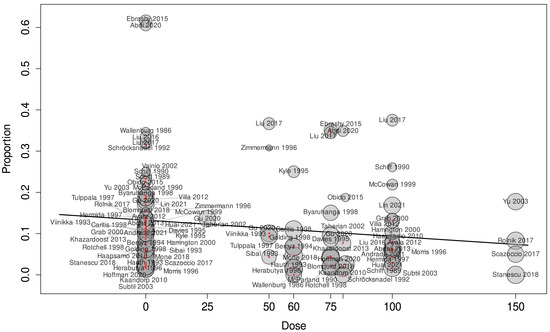
Figure 3.
Meta-regression between the administered dosage and the effect size of each individual study for the outcome of preeclampsia started at any time during pregnancy [20,21,22,24,25,26,30,31,33,34,35,36,37,38,39,40,44,45,46,48,49,50,52,53,54,55,56,57,58,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,77,78].
3.4. Secondary Outcomes
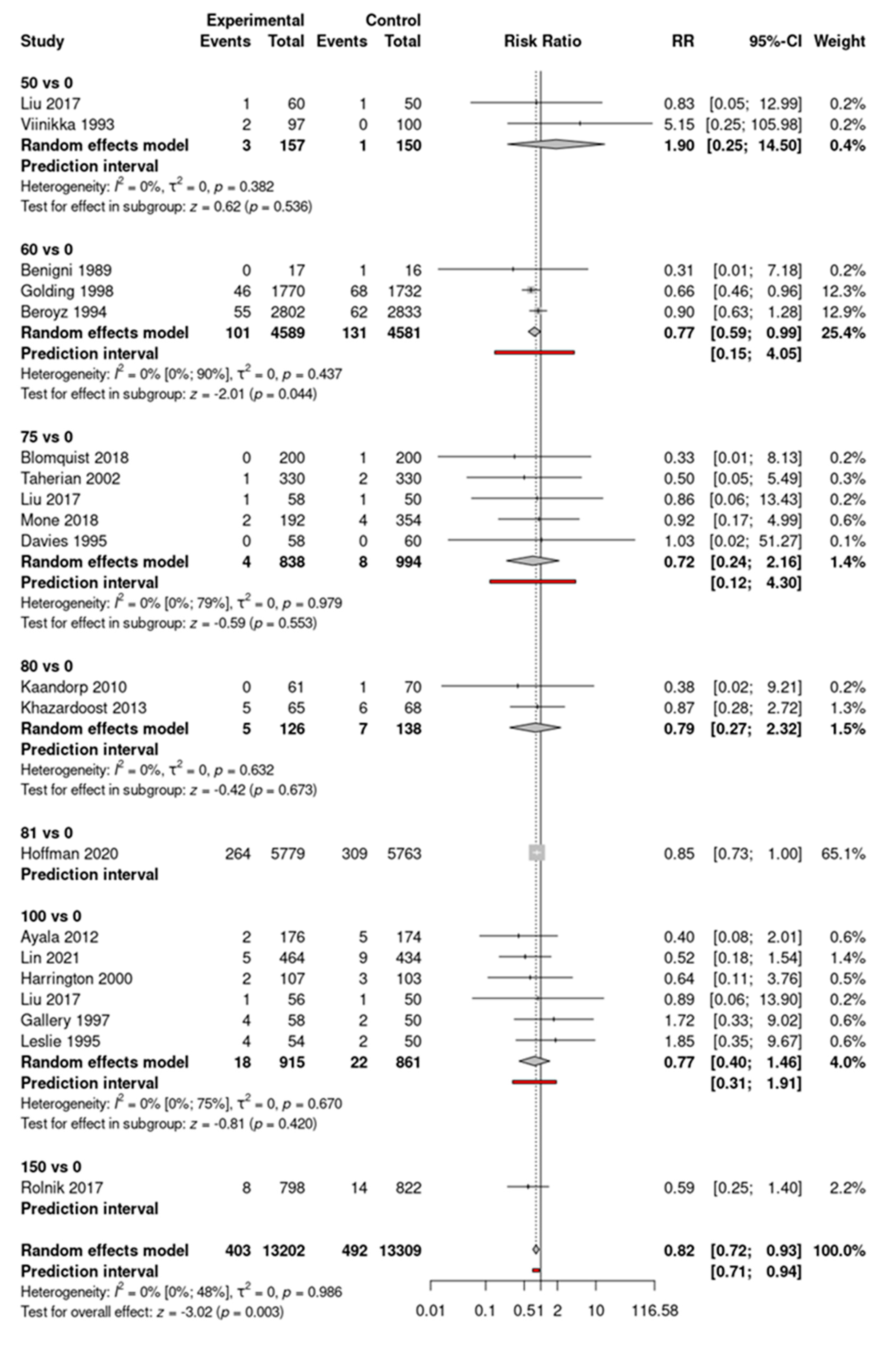
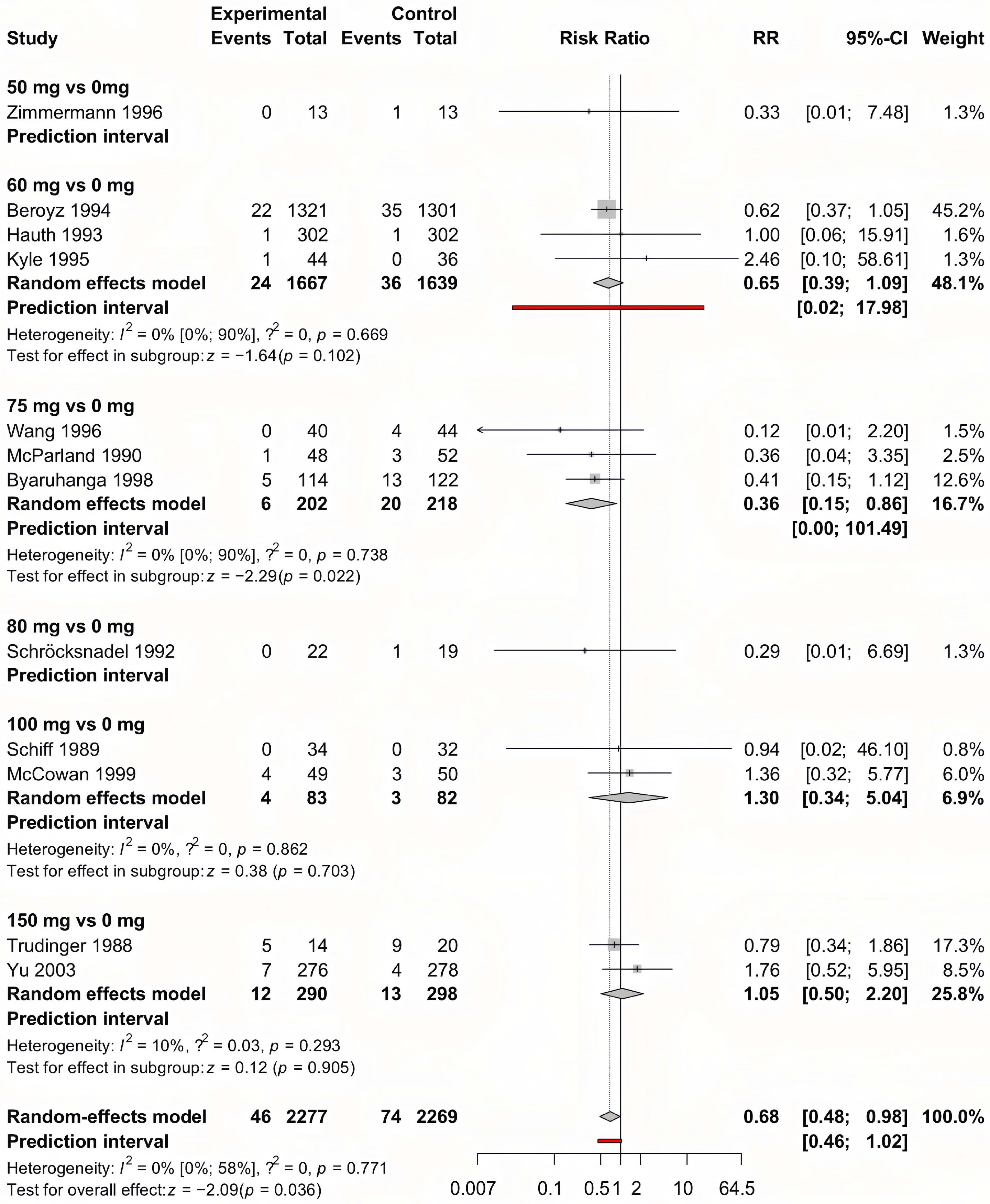
In the overall analysis, no significant risk reduction for IUGR was found in the aspirin group compared to the control group. In the case of early-initiated aspirin, lower rates were found (RR = 0.91, CI: 0.083–1.00, p = 0.055), but the significance level was not reached. Based on subgroup analyses, only 150 mg of aspirin was associated with significant risk reduction (RR = 0.72, CI 0.55–0.96 and RR = 0.83, CI: 0.70–0.99) in cases of fetal weight below the 10th and 5th percentile, respectively. No significant effect was described for the outcome of more severe IUGR (<3rd percentile). Although for the outcome of preterm birth <37 weeks, there were no significant differences in the risks between the two groups (RR = 0.82, CI: 0.65–1.03), and patients receiving aspirin carried their pregnancies significantly longer by an average of 0.26 weeks and gave birth to a significantly—averagely 27.56 g—heavier child than patients receiving no prophylaxis (MD = 0.26, CI: 0.05–0.46, and MD = 27.56, CI: 5.09–50.04, respectively). On the other hand, in the set up of late aspirin initiation (>week 20), a significant reduction was described in the rates of preterm birth (RR = 0.79, CI: 0.70–0.91), without a significant effect on birth weight (MD = 0.25, CI: −0.38–0.87) or gestational age (MD = 42.37, CI: −15.96–100.70). No significant difference in the incidence of placental abruption or postpartum hemorrhage was described between the two groups (RR = 1.13, CI: 0.92–1.39) and (RR = 1.13, CI: 0.95–1.34), respectively. Although the necessity of the neonatal intensive care unit admission of newborns was not influenced by prophylactic aspirin usage (RR = 0.96, CI: 0.86–1.06), newborns of those who were allocated to receive aspirin had a significantly reduced risk for perinatal death (RR = 0.86, CI: 0.77–0.96). For the outcome of perinatal death, significantly reduced risks can also be noted in patients who started aspirin before or after the 20th week (RR = 0.82, CI: 0.72–0.93 and RR = 0.68, CI: 0.48–0.98, respectively) (Figure 4 and Figure 5).
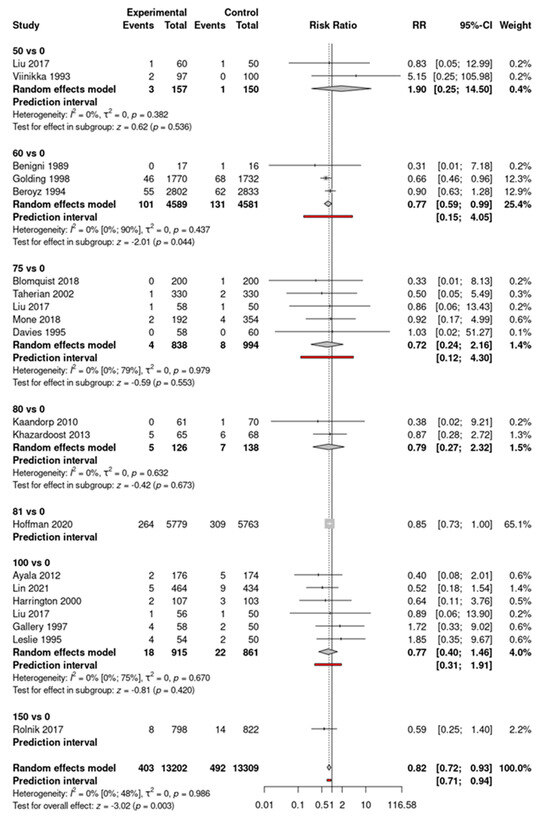
Figure 4.
Forest plot of the perinatal death outcome with early-initiated (<week 20) aspirin [20,21,24,25,30,31,34,36,37,38,39,40,44,45,46,48,49,50,52,53,54,56,60,62,63,65,66,74].
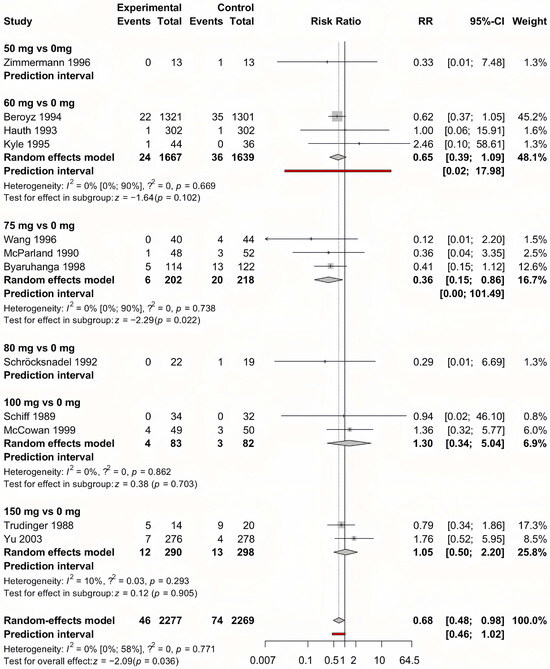
Figure 5.
Forest plot of the perinatal death outcome with late-initiated (>week 20) aspirin [24,59,64,67,68,69,70,71,73,76,77,78].
3.5. Publication Bias
Egger’s test showed a significant publication bias for overall birth weight (p = 0.043), overall IUGR (p = 0.023), and gestational age for aspirin started before 20 weeks (p = 0.019).
3.6. Risk of Bias Assessment and Evidence Synthesis
Overall, no studies were deemed to have a high risk for bias, six studies were rated to raise some concerns, and the remaining fifty-three studies were evaluated to have a low risk of bias. The results of the risk of bias assessment are presented in Supplementary Table S3. Evidence certainty of all our examined outcomes was graded as high evidence (Table 2 and Supplementary Table S4).
4. Discussion
4.1. Main Findings
In correlation with prior meta-analyses [10,11,79], we found that aspirin started before the 20th week significantly reduced the risk of preeclampsia and perinatal death [79] in both low- and high-risk pregnancies. This effect was consistent across various study populations and remained robust even in sensitivity analyses. Based on the meta-regression analyses, the dose of aspirin was not significantly associated with the risk of preeclampia. The observed reduction in preeclampsia risk aligns with the hypothesis that early aspirin initiation counteracts placental dysfunction, a key pathophysiological mechanism underlying the disease. As placentation is largely completed by the end of the first trimester, initiating aspirin prophylaxis before the 20th week may enhance trophoblastic invasion and improve uteroplacental perfusion. This mechanistic basis is supported by studies demonstrating that aspirin modulates thromboxane–prostacyclin balance, mitigates oxidative stress, and restores angiogenic homeostasis in high-risk pregnancies.
Despite the clear benefits of early initiation, our findings indicate no significant dose–response relationship, reinforcing the idea that lower doses may be equally effective in preeclampsia prevention when administered at the optimal time. This is consistent with prior clinical recommendations that emphasize initiation timing over dose escalation. However, residual heterogeneity across studies highlights the need for further research to identify potential subgroups that might benefit from higher doses or alternative risk stratification methods.
4.2. Additional Findings
Regarding secondary outcomes, we found different effects with a wide variety of significant and non-significant results (see Supplementary Figures S2–S24). For the outcome of IUGR, a significant risk reduction was only described in the overall group if IUGR was defined as below the 5th percentile. We found that aspirin prophylaxis does not affect the incidence rate of severe IUGR (IUGR below the 3rd percentile) and the intensive care admission of newborns. These data are not supported by previous meta-analyses, which suggest aspirin as a potential prophylaxis for IUGR [6,79]. However, the ASPIRIN trial [38] linked early-initiated aspirin prophylaxis with significant preterm birth reduction, and it has been strengthened by the meta-analysis of Yeo et al. 2021 [79]; we did not find a significant correlation between aspirin prophylaxis and preterm birth incidence only in the subgroup of late-initiated aspirin. These beneficial effects of late initiation should be evaluated carefully by considering that spontaneous and iatrogenic preterm births were not distinguished in the analysis of the involved trials. Prophylaxis significantly prolonged pregnancies by 0.26 weeks, and the actual birth weight of newborns was significantly higher, with 27.56 g on average. This correlates with the findings of an earlier-mentioned meta-analysis [80], with the difference being that the effect on gestational age did not reach the significance level earlier.
During the peer review process, a new randomized controlled trial by Mirzamoradi et al. was published, investigating low-dose aspirin (80 mg) for preterm delivery (PTD) prevention in women with a history of spontaneous PTD. While aspirin did not significantly reduce overall PTD rates, it showed a protective effect in a high-risk subgroup experiencing spontaneous labor (p = 0.022). These findings further highlight the heterogeneous effects of aspirin on PTD, suggesting a potential role in targeted prophylaxis.
4.3. Safety
With all these beneficial effects, we have to take safety into account. At doses more than 100 mg/day, aspirin irreversibly inhibits COX-1 and COX-2. Although blocking prostaglandin production, suppressing the immune system, and diminishing oxidative stress might restore the angiogenic imbalance associated with preeclampsia [80,81], safety considerations must always be considered. In the case of placental abruption, which has been attributed to ischemia–reperfusion injury in maternal uteroplacental vessels as a possible complication of aspirin intake, increased risk ratios were found in the aspirin group, but it did not reach the level of significance. Referring to a prior meta-analysis—examining low-risk nulliparous women with singleton pregnancies—conducted by Man et al. in 2021 [11], our study showed similar results for postpartum bleeding, which did not reach the level of significance. We did not examine the amount of blood loss during delivery. Due to a lack of quantified information, we did not perform a statistical analysis of antepartum bleeding.
4.4. Strengths and Limitations
Regarding the strengths of our study, this assessment was the first meta-regression analysis of aspirin for preeclampsia prevention, evaluating a large sample size. Subgroup analyses were also conducted to determine the optimal dose of prophylactic aspirin. The limitations of this work include heterogeneity in outcome definitions, which may introduce some inconsistency in the findings. Additionally, some studies did not provide clearly defined outcomes, further contributing to variability. We did not separately evaluate preterm preeclampsia (preeclampsia before the 34th week of pregnancy) or preterm birth before the 34th week of gestation. Due to limited data and inconsistent reporting, antepartum bleeding was not assessed. In our study, iatrogenic and spontaneous preterm births were not distinguished, and the risk factors for preterm birth were not evaluated, which likely varied across study sites. In studies where multiple aspirin doses were compared to placebo, to prevent the distortion of outcomes, we excluded additional dose groups beyond the first comparison to avoid counting the same placebo group multiple times. The selection of which dose to include in such cases was randomized. Additionally, the moderate risk of bias in some domains represents another limitation. Despite these constraints, aspirin prophylaxis was effective in preventing preeclampsia and significantly lowered the incidence of perinatal death, especially when initiated before 20 weeks of pregnancy. Different doses showed effectiveness for various outcomes, but no clear dose dependency was observed across the examined endpoints.
4.5. Implications for Practice and Research
In agreement with the leading professional societies [82,83,84], we suggest aspirin prophylaxis at a dose of 81 g to 150 mg for high-risk pregnancies [85] with the initiation before 16 but not earlier than 11 weeks of gestation, until 36 weeks of gestation, when delivery occurs, or when preeclampsia is diagnosed. We encourage clinicians to screen for high-risk pregnancies available to start aspirin prophylaxis with a dose preferably between 81 mg and 150 mg. Based on these findings, preeclampsia and perinatal mortality can be successfully reduced. By taking into account the international guidelines [82,83,84], and the examined dose–response correlation between aspirin dose and preeclampsia incidence, we suggest further RCTs with higher doses of aspirin compared to the widely accepted 81 mg, focusing on preterm preeclampsia, fetal–maternal complications, and bleeding. We suggest involving pediatricians to evaluate fetal hemorrhagic conditions, and for the clinical obstetricians to set up a reliable measurement method for evaluating peripartum bleeding in both vaginal and abdominal delivery cases.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/jcm14072134/s1, Figure S1: PRISMA Flowchart of article selection; Figure S2: Forest plot of the outcome preeclampsia regardless of aspirin initiation time; Figure S3: Forest plot of the outcome intrauterine growth restriction below the 10 percentile regardless of aspirin initiation time; Figure S4: Forest plot of the outcome intrauterine growth restriction below the 5 percentile regardless of aspirin initiation time; Figure S5: Forest plot of the outcome intrauterine growth restriction below the 3 percentile regardless of aspirin initiation time; Figure S6: Forest plot of the outcome preterm birth before week 37 regardless of aspirin initiation time; Figure S7: Forest plot of the outcome gestational age at delivery (in weeks) regardless of aspirin initiation time; Figure S8: Forest plot of the outcome actual birth weight (in grams) regardless of aspirin initiation time; Figure S9: Forest plot of the outcome placental abruption regardless of aspirin initiation time; Figure S10: Forest plot of the outcome neonatal intensive care unit admission regardless of aspirin initiation time; Figure S11: Forest plot of the outcome perinatal death regardless of aspirin initiation time; Figure S12: Forest plot of the outcome postpartum hemorrhage regardless of aspirin initiation time; Figure S13: Forest plot of the outcome preeclampsia with early initiated (<week 20) aspirin; Figure S14: Forest plot of the outcome intrauterine growth restriction below the 10 percentile with early initiated (<week 20) aspirin; Figure S15: Forest plot of the outcome intrauterine growth restriction below the 5 percentile with early initiated (<week 20) aspirin; Figure S16: Forest plot of the outcome intrauterine growth restriction below the 3 percentile regardless of aspirin initiation time; Figure S17: Forest plot of the outcome preterm birth before week 37 with early initiated (<week 20) aspirin; Figure S18: Forest plot of the outcome gestational age at delivery (in weeks) with early initiated (<week 20) aspirin; Figure S19: Forest plot of the outcome actual birth weight (in grams) with early initiated (<week 20) aspirin; Figure S20: Forest plot of the outcome preeclampsia with late initiated (>week 20) aspirin; Figure S21: Forest plot of the outcome intrauterine growth restriction below the 10 percentile with late initiated (>week 20) aspirin; Figure S22: Forest plot of the outcome preterm birth before week 37 with late initiated (>week 20) aspirin; Figure S23: Forest plot of the outcome gestational age at delivery (in weeks) with late initiated (>week 20) aspirin; Figure S24: Forest plot of the outcome actual birth weight (in grams) with late initiated (>week 20) aspirin; Figure S25: Forest plot of the outcome perinatal death with late initiated (>week 20) aspirin; Table S1: PRISMA 2020 checklist; Table S2: Detailed search strategy; Table S3: Eligibility criteria in each included article; Table S4: Outcomes and outcome definitions in the included studies; Table S5: Risk of bias assessment of each individual study and outcome; Table S6: Certainty of evidence using the GRADEPro tool.
Author Contributions
B.K.: conceptualization, data curation, formal analysis, and writing—original draft; S.V.: conceptualization, project administration, methodology, and writing—review and editing; A.V.: conceptualization, formal analysis, visualization, and writing—review and editing; P.H.: conceptualization and writing—review and editing; V.V.: conceptualization, data curation, and writing—review and editing; I.B.: conceptualization, data curation, and writing—review and editing; A.S.: conceptualization, data curation, and writing—review and editing; P.N.: conceptualization and writing—review and editing; Z.B.: conceptualization, supervision, and writing—original draft; N.Á.: conceptualization, supervision, funding acquisition, and writing—original draft. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study did not require ethical approval because it is a systematic review and meta-analysis that involved the synthesis and analysis of previously published data. All included studies had already obtained ethical approval from their respective institutional review boards or ethics committees. No new data were collected directly from human participants or animals, and no identifying or sensitive information was accessed during this study. Therefore, the research complies with ethical standards for secondary data analysis as outlined by the Declaration of Helsinki.
Informed Consent Statement
Not applicable, as this study is a systematic review and meta-analysis using previously published data, with no new data collected from human participants.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article, as it is based on a systematic review and meta-analysis of previously published studies. For further details, refer to the MDPI Research Data Policies at https://www.mdpi.com/ethics, accessed on 3 December 2024.
Acknowledgments
The authors have no additional acknowledgments to declare.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Rana, S.; Lemoine, E.; Granger, J.P.; Karumanchi, S.A. Preeclampsia. Circ. Res. 2019, 124, 1094–1112. [Google Scholar] [CrossRef] [PubMed]
- Khan, K.S.; Wojdyla, D.; Say, L.; Gülmezoglu, A.M.; Van Look, P.F. WHO analysis of causes of maternal death: A systematic review. Lancet 2006, 367, 1066–1074. [Google Scholar] [CrossRef]
- Hogan, M.C.; Foreman, K.J.; Naghavi, M.; Ahn, S.Y.; Wang, M.; Makela, S.M.; Lopez, A.D.; Lozano, R.; Murray, C.J.L. Maternal mortality for 181 countries, 1980–2008: A systematic analysis of progress towards Millennium Development Goal 5. Lancet 2010, 375, 1609–1623. [Google Scholar] [CrossRef] [PubMed]
- Wanderer, J.P.; Leffert, L.R.; Mhyre, J.M.; Kuklina, E.V.; Callaghan, W.M.; Bateman, B.T. Epidemiology of Obstetric-Related ICU Admissions in Maryland. Crit. Care Med. 2013, 41, 1844–1852. [Google Scholar] [CrossRef]
- Kuklina, E.V.; Ayala, C.; Callaghan, W.M. Hypertensive Disorders and Severe Obstetric Morbidity in the United States. Obstet. Gynecol. 2009, 113, 1299–1306. [Google Scholar] [CrossRef] [PubMed]
- Duley, L.; Meher, S.; Hunter, K.E.; Seidler, A.L.; Askie, L.M. Antiplatelet agents for preventing pre-eclampsia and its complications. Cochrane Database Syst. Rev. 2019, 2019, CD004659. [Google Scholar] [CrossRef]
- Beaufils, M.; Donsimoni, R.; Uzan, S.; Colau, J.C. Prevention of pre-eclampsia by early antiplatelet therapy. Lancet 1985, 325, 840–842. [Google Scholar] [CrossRef] [PubMed]
- Roberge, S.; Nicolaides, K.H.; Demers, S.; Villa, P.; Bujold, E. Prevention of perinatal death and adverse perinatal outcome using low-dose aspirin: A meta-analysis. Ultrasound Obstet. Gynecol. 2013, 41, 491–499. [Google Scholar] [CrossRef]
- Roberge, S.; Bujold, E.; Nicolaides, K.H. Aspirin for the prevention of preterm and term preeclampsia: Systematic review and metaanalysis. Am. J. Obstet. Gynecol. 2018, 218, 287–293.e1. [Google Scholar] [CrossRef]
- Van Doorn, R.; Mukhtarova, N.; Flyke, I.P.; Lasarev, M.; Kim, K.; Hennekens, C.H.; Hoppe, K.K. Dose of aspirin to prevent preterm preeclampsia in women with moderate or high-risk factors: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0247782. [Google Scholar] [CrossRef]
- Man, R.; Hodgetts Morton, V.; Devani, P.; Morris, R.K. Aspirin for preventing adverse outcomes in low risk nulliparous women with singleton pregnancies: A systematic review and meta-analysis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 262, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Poon, L.C.; Shennan, A.; Hyett, J.A.; Kapur, A.; Hadar, E.; Divakar, H.; McAuliffe, F.; da Silva Costa, F.; von Dadelszen, P.; McIntyre, H.D.; et al. The International Federation of Gynecology and Obstetrics (FIGO) initiative on pre-eclampsia: A pragmatic guide for first-trimester screening and prevention. Int. J. Gynecol. Obstet. 2019, 145 (Suppl. S1), 1–33. [Google Scholar] [CrossRef] [PubMed]
- Tugwell, P.; Tovey, D. PRISMA 2020. J. Clin. Epidemiol. 2021, 134, A5–A6. [Google Scholar] [CrossRef] [PubMed]
- Cumpston, M.; Li, T.; Page, M.J.; Chandler, J.; Welch, V.A.; Higgins, J.P.; Thomas, J. Updated guidance for trusted systematic reviews: A new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst. Rev. 2019, 2019, ED000142. [Google Scholar] [CrossRef]
- Khan, N.; Andrade, W.; De Castro, H.; Wright, A.; Wright, D.; Nicolaides, K.H. Impact of new definitions of pre-eclampsia on incidence and performance of first-trimester screening. Ultrasound Obstet. Gynecol. 2020, 55, 50–57. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Balduzzi, S.; Rücker, G.; Schwarzer, G. How to perform a meta-analysis with R: A practical tutorial. Evid. Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef]
- Viechtbauer, W. Bias and Efficiency of Meta-Analytic Variance Estimators in the Random-Effects Model. J. Educ. Behav. Stat. 2005, 30, 261–293. [Google Scholar] [CrossRef]
- Aguayo-Albasini, J.L.; Flores-Pastor, B.; Soria-Aledo, V. GRADE System: Classification of Quality of Evidence and Strength of Recommendation. Cirugía Española 2014, 92, 82–88. [Google Scholar] [CrossRef]
- Abdali, K.; Taghizadeh, R.; Amoei, S.; Tabatabai, S.H.R. Comparison between aspirin and placebo on the mean of 24 hour blood pressure in pregnant women at preeclampsia risk, a double blind randomized controlled clinical trial. Int. J. Community Based Nurs. Midwifery 2013, 1, 83–89. Available online: https://www.cochranelibrary.com/central/doi/10.1002/central/CN-01995023/full (accessed on 3 December 2024).
- Abdi, N.; Rozrokh, A.; Alavi, A.; Zare, S.; Vafaei, H.; Asadi, N.; Kasraeian, M.; Hessami, K. The effect of aspirin on preeclampsia, intrauterine growth restriction and preterm delivery among healthy pregnancies with a history of preeclampsia. J. Chin. Med. Assoc. 2020, 83, 852–857. [Google Scholar] [CrossRef] [PubMed]
- Andrade, J.; Silva, R.M.D.; Araujo Júnior, E.; Carvalho, F.H.C. Low-dose acetylsalicylic acid does not modify maternal vascular reactivity in nulliparas. J. Matern. Fetal Neonatal Med. 2021, 35, 6029–6035. [Google Scholar] [CrossRef] [PubMed]
- Benigni, A.; Gregorini, G.; Frusca, T.; Chiabrando, C.; Ballerini, S.; Valcamonico, A.; Orisio, S.; Piccinelli, A.; Pinciroli, V.; Fanelli, R.; et al. Effect of low-dose aspirin on fetal and maternal generation of thromboxane by platelets in women at risk for pregnancy-induced hypertension. New Engl. J. Med. 1989, 321, 357–362. Available online: https://www.embase.com/search/results?subaction=viewrecord&id=L19190440&from=export (accessed on 3 December 2024). [CrossRef] [PubMed]
- Beroyz, G.; Casale, R.; Farreiros, A.; Palermo, M.; Margulies, M.; Voto, L.; Fabregues, G.; Ramalingam, R.; Davies, T.; Bryce, R.; et al. CLASP: A randomised trial of low-dose aspirin for the prevention and treatment of pre-eclampsia among 9364 pregnant women. Lancet 1994, 343, 619–629. Available online: https://www.embase.com/search/results?subaction=viewrecord&id=L24087805&from=export (accessed on 3 December 2024).
- Blomqvist, L.; Hellgren, M.; Strandell, A. Acetylsalicylic acid does not prevent first-trimester unexplained recurrent pregnancy loss: A randomized controlled trial. Acta Obstet. Gynecol. Scand. 2018, 97, 1365–1372. [Google Scholar] [CrossRef]
- Caritis, S.; Sibai, B.; Hauth, J.; Lindheimer, M.D.; Klebanoff, M.; Thom, E.; VanDorsten, P.; Landon, M.; Paul, R.; Miodovnik, M.; et al. Low-dose aspirin to prevent preeclampsia in women at high risk. National Institute of Child Health and Human Development Network of Maternal-Fetal Medicine Units. N. Engl. J. Med. 1998, 338, 701–705. Available online: https://www.cochranelibrary.com/central/doi/10.1002/central/CN-00148035/full (accessed on 3 December 2024). [CrossRef]
- Caspi, E.; Raziel, A.; Sherman, D.; Arieli, S.; Bukovski, I.; Weinraub, Z. Prevention of pregnancy-induced hypertension in twins by early administration of low-dose aspirin: A preliminary report. Am. J. Reprod. Immunol. 1994, 31, 19–24. [Google Scholar] [CrossRef]
- Chiaffarino, F.; Parazzini, F.; Paladini, D.; Acaia, B.; Ossola, W.; Marozio, L.; Facchinetti, F.; Del Giudice, A. A small randomised trial of low-dose aspirin in women at high risk of pre-eclampsia. Eur. J. Obstet. Gynecol. Reprod. Biol. 2004, 112, 142–144. [Google Scholar] [CrossRef]
- Dasari, R.; Narang, A.; Vasishta, K.; Garewal, G. Effect of maternal low dose aspirin on neonatal platelet function. Indian Pediatr. 1998, 35, 507–511. [Google Scholar]
- Davies, N.J.; Gazvani, M.R.; Farquharson, R.G.; Walkinshaw, S.A. Low-dose aspirin in the prevention of hypertensive disorders of pregnancy in relatively low-risk nulliparous women. Hypertens. Pregnancy 1995, 14, 49–55. Available online: https://www.embase.com/search/results?subaction=viewrecord&id=L25122276&from=export (accessed on 3 December 2024). [CrossRef]
- Ebrashy, A.; Ibrahim, M.; Marzook, A.; Yousef, D. Usefulness of aspirin therapy in high-risk pregnant women with abnormal uterine artery Doppler ultrasound at 14-16 weeks pregnancy: Randomized controlled clinical trial. Croat Med. J. 2005, 46, 826–831. [Google Scholar] [PubMed]
- Gallery, E.D.M.; Ross, M.R.; Hawkins, M.; Leslie, G.; Györy, Á.Z. Low-dose aspirin in high-risk pregnancy? Hypertens. Pregnancy. 1997, 16, 229–238. [Google Scholar] [CrossRef]
- Golding, J. Jamaica Low Dose Aspirin Study Group. A randomised trial of low dose aspirin for primiparae in pregnancy. Br. J. Obstet. Gynaecol. 1998, 105, 293–299. [Google Scholar] [CrossRef]
- Haapsamo, M.; Martikainen, H.; Tinkanen, H.; Heinonen, S.; Nuojua-Huttunen, S.; Räsänen, J. Low-dose aspirin therapy and hypertensive pregnancy complications in unselected IVF and ICSI patients: A randomized, placebo-controlled, double-blind study. Hum. Reprod. 2010, 25, 2972–2977. [Google Scholar] [CrossRef]
- Herabutya, Y.; Jetsawangsri, T.; Saropala, N. The use of low-dose aspirin to prevent preeclampsia. Int. J. Gynaecol. Obstet. 1996, 54, 177–178. [Google Scholar] [CrossRef]
- Hermida, R.C.; Ayala, D.E.; Iglesias, M.; Mojón, A.; Silva, I.; Ucieda, R.; Fernández, J.R. Time-dependent effects of low-dose aspirin administration on blood pressure in pregnant women. Hypertension 1997, 30 Pt 2, 589–595. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, M.K.; Goudar, S.S.; Kodkany, B.S.; Metgud, M.; Somannavar, M.; Okitawutshu, J.; Lokangaka, A.; Tshefu, A.; Bose, C.L.; Mwapule, A.; et al. Low-dose aspirin for the prevention of preterm delivery in nulliparous women with a singleton pregnancy (ASPIRIN): A randomised, double-blind, placebo-controlled trial. Lancet 2020, 395, 285–293. [Google Scholar] [CrossRef]
- Huai, J.; Lin, L.; Juan, J.; Chen, J.; Li, B.; Zhu, Y.; Yu, M.; Yang, H. Preventive effect of aspirin on preeclampsia in high-risk pregnant women with stage 1 hypertension. J. Clin. Hypertens. 2021, 23, 1060–1067. [Google Scholar] [CrossRef]
- Kaandorp, S.P.; Goddijn, M.; Post Van Der, J.A.M.; Hutten, B.A.; Verhoeve, H.R.; Hamulyak, K.; Mol, B.W.; Folkeringa, N.; Nahuis, M.; Papastonis, D.N.M.; et al. Aspirin alone or combined with low-molecular-weight heparin in women with unexplained recurrent miscarriage, a randomised placebo-controlled trial. Hum. Reprod. 2010, 25, i28–i29. Available online: https://www.embase.com/search/results?subaction=viewrecord&id=L70245484&from=export (accessed on 3 December 2024). [CrossRef]
- Khazardoost, S.; Mousavi, S.; Borna, S.; Hantoushzadeh, S.; Alavi, A.; Khezerlou, N. Effect of aspirin in prevention of adverse pregnancy outcome in women with elevated alpha-fetoprotein. J. Matern.-Fetal Neonatal Med. 2014, 27, 561–565. [Google Scholar] [CrossRef] [PubMed]
- Lambers, M.J.; Hoozemans, D.A.; Schats, R.; Homburg, R.; Lambalk, C.B.; Hompes, P.G.A. Low-dose aspirin in non-tubal IVF patients with previous failed conception: A prospective randomized double-blind placebo-controlled trial. Fertil. Steril. 2009, 92, 923–929. [Google Scholar] [CrossRef]
- Landman, A.; de Boer, M.; Visser, L.; Hemels, M.; Naaktgeboren, C.; Jansen-van der Weide, M.; Mol, B.; van Laar, J.; Papatsonis, D.; Bekker, M.; et al. Low dose aspirin for the prevention of recurrent preterm labor (APRIL): A randomized controlled trial. Am. J. Obstet. Gynecol. 2021, 224, S6. Available online: https://www.embase.com/search/results?subaction=viewrecord&id=L2010868438&from=export (accessed on 3 December 2024). [CrossRef]
- Leslie, G.I.; Gallery, E.D.M.; Arnold, J.D.; Ross, M.R.; Gyory, A.Z. Neonatal outcome in a randomized, controlled trial of low-dose aspirin in high-risk pregnancies. J. Paediatr. Child. Health 1995, 31, 549–552. Available online: https://www.embase.com/search/results?subaction=viewrecord&id=L26019307&from=export (accessed on 3 December 2024). [CrossRef] [PubMed]
- Lin, L.; Huai, J.; Li, B.; Zhu, Y.; Juan, J.; Zhang, M.; Cui, S.; Zhao, X.; Ma, Y.; Zhao, Y.; et al. A randomized controlled trial of low-dose aspirin for the prevention of preeclampsia in women at high risk in China. Am. J. Obstet. Gynecol. 2021, 226, 251.e1–251.e12. Available online: https://www.cochranelibrary.com/central/doi/10.1002/central/CN-02326513/full (accessed on 3 December 2024). [CrossRef] [PubMed]
- Liu, F.M.; Zhao, M.; Wang, M.; Yang, H.L.; Li, L. Effect of regular oral intake of aspirin during pregnancy on pregnancy outcome of high-risk pregnancy-induced hypertension syndrome patients. Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 5013–5016. [Google Scholar]
- Liu, F.; Yang, H.; Li, G.; Zou, K.; Chen, Y. Effect of a small dose of aspirin on quantitative test of 24-h urinary protein in patients with hypertension in pregnancy. Exp. Ther. Med. 2017, 13, 37–40. [Google Scholar] [CrossRef]
- Louden, K.A.; Broughton Pipkin, F.; Symonds, E.M.; Tuohy, P.; O’Callaghan, C.; Heptinstall, S.; Fox, S.; Mitchell, J.R.A. A randomized placebo-controlled study of the effect of low dose aspirin on platelet reactivity and serum thromboxane B2 production in non-pregnant women, in normal pregnancy, and in gestational hypertension. Br. J. Obstet. Gynaecol. 1992, 99, 371–376. [Google Scholar] [CrossRef]
- Mone, F.; Mulcahy, C.; McParland, P.; Downey, P.; Culliton, M.; Maguire, O.; Mooney, E.E.; Clarke, P.; Fitzgerald, D.; Tully, E.; et al. The impact of low dose aspirin on preeclampsia biomarkers and fetal growth in lowrisk women. Am. J. Obstet. Gynecol. 2018, 218, S303. Available online: https://www.embase.com/search/results?subaction=viewrecord&id=L620310171&from=export (accessed on 3 December 2024). [CrossRef]
- Morris, J.; Fay, R.; Ellwood, D.; Cook, C.; Devonald, K. A Randomized Controlled Trial of Aspirin in Patients With Abnormal Uterine Artery Blood Flow. Obstet. Gynecol. 1996, 87, 74–78. [Google Scholar] [CrossRef]
- Odibo, A.O.; Goetzinger, K.R.; Odibo, L.; Tuuli, M.G. Early prediction and aspirin for prevention of pre-eclampsia (EPAPP) study: A randomized controlled trial. Ultrasound Obstet. Gynecol. 2015, 46, 414–418. [Google Scholar] [CrossRef] [PubMed]
- Pattison, N.S.; Chamley, L.W.; Birdsall, M.; Zanderigo, A.M.; Liddell, H.S.; McDougall, J. Does aspirin have a role in improving pregnancy outcome for women with the antiphospholipid syndrome? A randomized controlled trial. Am. J. Obstet. Gynecol. 2000, 183, 1008–1012. [Google Scholar] [CrossRef]
- Rolnik, D.L.; Wright, D.; Poon, L.C.Y.; Syngelaki, A.; O’Gorman, N.; de Paco Matallana, C.; Akolekar, R.; Cicero, S.; Janga, D.; Singh, M.; et al. ASPRE trial: Performance of screening for preterm pre-eclampsia. Ultrasound Obstet. Gynecol. 2017, 50, 492–495. [Google Scholar] [CrossRef]
- Rotchell, Y.E.; Cruickshank, J.K.; Gay, M.P.; Griffiths, J.; Stewart, A.; Farrell, B.; Ayers, S.; Hennis, A.; Grant, A.; Duley, L.; et al. Barbados Low Dose Aspirin Study in Pregnancy (BLASP): A randomised trial for the prevention of pre-eclampsia and its complications. Br. J. Obstet. Gynaecol. 1998, 105, 286–292. [Google Scholar] [CrossRef] [PubMed]
- Scazzocchio, E.; Oros, D.; Diaz, D.; Ramirez, J.C.; Ricart, M.; Meler, E.; de Agüero, R.G.; Gratacos, E.; Figueras, F. Impact of aspirin on trophoblastic invasion in women with abnormal uterine artery Doppler at 11–14 weeks: A randomized controlled study. Ultrasound Obstet. Gynecol. 2017, 49, 435–441. [Google Scholar] [CrossRef] [PubMed]
- Sibai, B.M.; Caritis, S.N.; Thom, E.; Klebanoff, M.; McNellis, D.; Rocco, L.; Paul, R.H.; Romero, R.; Witter, F.; Rosen, M.; et al. Prevention of preeclampsia with low-dose aspirin in healthy, nulliparous pregnant women. The National Institute of Child Health and Human Development Network of Maternal-Fetal Medicine Units. N. Engl. J. Med. 1993, 329, 1213–1218. Available online: https://www.cochranelibrary.com/central/doi/10.1002/central/CN-00096363/full (accessed on 3 December 2024). [CrossRef]
- Stanescu, A.D.; Banica, R.; Sima, R.M.; Ples, L. Low dose aspirin for preventing fetal growth restriction: A randomised trial. J. Perinat. Med. 2018, 46, 776–779. [Google Scholar] [CrossRef]
- Subtil, D.; Goeusse, P.; Puech, F.; Lequien, P.; Biausque, S.; Breart, G.; Uzan, S.; Marquis, P.; Parmentier, D.; Churlet, A.; et al. Aspirin (100 mg) used for prevention of pre-eclampsia in nulliparous women: The Essai Régional Aspirine Mère-Enfant study (Part 1). BJOG Int. J. Obstet. Gynaecol. 2003, 110, 475–484. [Google Scholar] [CrossRef]
- Subtil, D.; Goeusse, P.; Houfflin-Debarge, V.; Puech, F.; Lequien, P.; Breart, G.E.; Uzan, S.; Quandalle, F.; Delcourt, Y.M.; Malek, Y.M.; et al. Randomised comparison of uterine artery Doppler and aspirin (100 mg) with placebo in nulliparous women: The Essai Régional Aspirine Mère-Enfant study (Part 2). BJOG Int. J. Obstet. Gynaecol. 2003, 110, 485–491. Available online: https://www.embase.com/search/results?subaction=viewrecord&id=L36556131&from=export (accessed on 3 December 2024). [CrossRef]
- Trudinger, B.J.; Cook, C.M.; Thompson, R.S.; Giles, W.B.; Connelly, A. Low-dose aspirin therapy improves fetal weight in umbilical placental insufficiency. Am. J. Obstet. Gynecol. 1988, 159, 681–685. [Google Scholar] [CrossRef]
- Tulppala, M.; Marttunen, M.; Söderstrom-Anttila, V.; Foudila, T.; Ailus, K.; Palosuo, T.; Ylikorkala, O. Low-dose aspirin in prevention of miscarriage in women with unexplained or autoimmune related recurrent miscarriage: Effect on prostacyclin and thromboxane A2 production. Hum. Reprod. 1997, 12, 1567–1572. [Google Scholar] [CrossRef] [PubMed]
- Vainio, M.; Kujansuu, E.; Iso-Mustajärvi, M.; Mäenpää, J. Low dose acetylsalicylic acid in prevention of pregnancy-induced hypertension and intrauterine growth retardation in women with bilateral uterine artery notches. BJOG Int. J. Obstet. Gynaecol. 2002, 109, 161–167. [Google Scholar]
- Viinikka, L.; Hartikainen-Sorri, A.L.; Lumme, R.; Hiilesmaa, V.; Ylikorkala, O. Low dose aspirin in hypertensive pregnant women: Effect on pregnancy outcome and prostacyclin-thromboxane balance in mother and newborn. Br. J. Obstet. Gynaecol. 1993, 100, 809–815. [Google Scholar] [CrossRef]
- Villa, P.M.; Kajantie, E.; Räikkönen, K.; Pesonen, A.K.; Hämäläinen, E.; Vainio, M.; Taipale, P.; Laivuori, H.; on behalf of the PREDO Study Group. Aspirin in the prevention of pre-eclampsia in high-risk women: A randomised placebo-controlled PREDO Trial and a meta-analysis of randomised trials. BJOG Int. J. Obstet. Gynaecol. 2013, 120, 64–74. [Google Scholar] [CrossRef] [PubMed]
- Byaruhanga, R.N.; Chipato, T.; Rusakaniko, S. A randomized controlled trial of low-dose aspirin in women at risk from pre-eclampsia. Int. J. Gynaecol. Obstet. 1998, 60, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Grab, D.; Paulus, W.E.; Erdmann, M.; Terinde, R.; Oberhoffer, R.; Lang, D.; Muche, R.; Kreienberg, R. Effects of low-dose aspirin on uterine and fetal blood flow during pregnancy: Results of a randomized, placebo-controlled, double-blind trial. Ultrasound Obstet. Gynecol. 2000, 15, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Harrington, K.; Kurdi, W.; Aquilina, J.; England, P.; Campbell, S. A prospective management study of slow-release aspirin in the palliation of uteroplacental insufficiency predicted by uterine artery Doppler at 20 weeks. Ultrasound Obstet. Gynecol. 2000, 15, 13–18. [Google Scholar] [CrossRef]
- Hauth, J.C.; Goldenberg, R.L.; Parker, C.R.; Philips, J.B.; Copper, R.L.; DuBard, M.B.; Cutter, G.R. Low-dose aspirin therapy to prevent preeclampsia. Am. J. Obstet. Gynecol. 1993, 168, 1083–1093. [Google Scholar] [CrossRef]
- Kyle, P.M.; Buckley, D.; Kissane, J.; De Swiet, M.; Redman, C.W.G. The angiotensin sensitivity test and low-dose aspirin are ineffective methods to predict and prevent hypertensive disorders in nulliparous pregnancy. Am. J. Obstet. Gynecol. 1995, 173, 865–872. Available online: https://www.embase.com/search/results?subaction=viewrecord&id=L25297339&from=export (accessed on 3 December 2024). [CrossRef]
- McCowan, L.M.; Harding, J.; Roberts, A.; Barker, S.; Ford, C.; Stewart, A. Administration of low-dose aspirin to mothers with small for gestational age fetuses and abnormal umbilical Doppler studies to increase birthweight: A randomised double-blind controlled trial. Br. J. Obstet. Gynaecol. 1999, 106, 647–651. [Google Scholar] [CrossRef] [PubMed]
- McParland, P.; Pearce, J.M.; Chamberlain, G.V.P. Doppler ultrasound and aspirin in recognition and prevention of pregnancy-induced hypertension. Lancet 1990, 335, 1552–1555. Available online: https://www.embase.com/search/results?subaction=viewrecord&id=L20189627&from=export (accessed on 3 December 2024).
- Schiff, E.; Peleg, E.; Goldenberg, M.; Rosenthal, T.; Ruppin, E.; Tamarkin, M.; Barkai, G.; Ben-Baruch, G.; Yahal, I.; Blankstein, J.; et al. The use of aspirin to prevent pregnancy-induced hypertension and lower the ratio of thromboxane A2 to prostacyclin in relatively high risk pregnancies. N. Engl. J. Med. 1989, 321, 351–356. [Google Scholar] [CrossRef] [PubMed]
- Schiff, E.; Barkai, G.; Ben-Baruch, G.; Mashiach, S. Low-dose aspirin does not influence the clinical course of women with mild pregnancy-induced hypertension. Obstet. Gynecol. 1990, 76 Pt 1, 742–744. [Google Scholar] [CrossRef] [PubMed]
- Schröcksnadel, H.; Sitte, B.; Alge, A.; Steckel-Berger, G.; Schwegel, P.; Pastner, E.; Daxenbichler, G.; Hansen, H.; Dapunt, O. Low-dose aspirin in primigravidae with positive roll-over test. Gynecol. Obstet. Invest. 1992, 34, 146–150. [Google Scholar] [CrossRef]
- Taherian, A.A.; Taherian, A.; Shirvani, A. Prevention of preeclampsia with low-dose aspirin or calcium supplementation. Arch. Iran Med. 2002, 5, 151–156. Available online: https://www.embase.com/search/results?subaction=viewrecord&id=L35314985&from=export (accessed on 3 December 2024).
- Wallenburg, H.C.S.; Dekker, G.A.; Makovitz, J.W.; Rotmans, P. Low-dose aspirin prevents pregnancy-induced hypertension and pre-eclampsia in angiotensin-sensitive primigravidae. Lancet 1986, 1, 1–3. Available online: https://www.embase.com/search/results?subaction=viewrecord&id=L16182814&from=export (accessed on 3 December 2024). [CrossRef] [PubMed]
- Wang, Z.; Li, W. A prospective randomized placebo-controlled trial of low-dose aspirin for prevention of intra-uterine growth retardation. Chin. Med. J. 1996, 109, 238–242. [Google Scholar]
- Yu, C.K.H.; Papageorghiou, A.T.; Parra, M.; Palma Dias, R.; Nicolaides, K.H. Randomized controlled trial using low-dose aspirin in the prevention of pre-eclampsia in women with abnormal uterine artery Doppler at 23 weeks’ gestation. Ultrasound Obstet. Gynecol. 2003, 22, 233–239. [Google Scholar] [CrossRef]
- Zimmermann, P.; Eiriö, V.; Koskinen, J.; Niemi, K.; Nyman, R.; Kujansuu, E.; Ranta, T. Effect of low-dose aspirin treatment on vascular resistance in the uterine, uteroplacental, renal and umbilical arteries—A prospective longitudinal study on a high risk population with persistent notch in the uterine arteries. Eur. J. Ultrasound 1997, 5, 17–30. Available online: https://www.embase.com/search/results?subaction=viewrecord&id=L27096629&from=export (accessed on 3 December 2024). [CrossRef]
- Choi, Y.J.; Shin, S. Aspirin Prophylaxis During Pregnancy: A Systematic Review and Meta-Analysis. Am. J. Prev. Med. 2021, 61, e31–e45. [Google Scholar] [CrossRef]
- Espinoza, J.; Vidaeff, A.; Pettker, C.M.; Shiman, H. ACOG Committee Opinion No. 202. ACOG. Obstet. Gynecol. 2019, 133, 1. [Google Scholar]
- Mirabito Colafella, K.M.; Neuman, R.I.; Visser, W.; Danser, A.H.J.; Versmissen, J. Aspirin for the prevention and treatment of pre-eclampsia: A matter of COX-1 and/or COX-2 inhibition? Basic Clin. Pharmacol. Toxicol. 2020, 127, 132–141. [Google Scholar] [CrossRef] [PubMed]
- LeFevre, M.L. Low-Dose Aspirin Use for the Prevention of Morbidity and Mortality From Preeclampsia: U.S. Preventive Services Task Force Recommendation Statement. Ann. Intern. Med. 2014, 161, 819. [Google Scholar] [CrossRef] [PubMed]
- Porter, F.T.; Gyamfi-Bannerman, C.; Manuk, T. ACOG Committee Opinion No. 743: Low-Dose Aspirin Use During Pregnancy. Obstet. Gynecol. 2018, 132, e44–e52. [Google Scholar]
- Rolnik, D.L.; Nicolaides, K.H.; Poon, L.C. Prevention of preeclampsia with aspirin. Am. J. Obstet. Gynecol. 2022, 226, S1108–S1119. [Google Scholar] [CrossRef]
- Davidson, K.W.; Barry, M.J.; Mangione, C.M.; Cabana, M.; Caughey, A.B.; Davis, E.M.; Donahue, K.; Doubeni, C.A.; Kubik, M.; Li, L.; et al. Aspirin Use to Prevent Preeclampsia and Related Morbidity and Mortality. JAMA 2021, 326, 1186. [Google Scholar]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).