
Postpartum Depression Epidemiology, Risk Factors, Diagnosis, and Management: An Appraisal of the Current Knowledge and Future Perspectives
 , , ,
, , ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
3. Definition and Epidemiology of Postpartum Depression
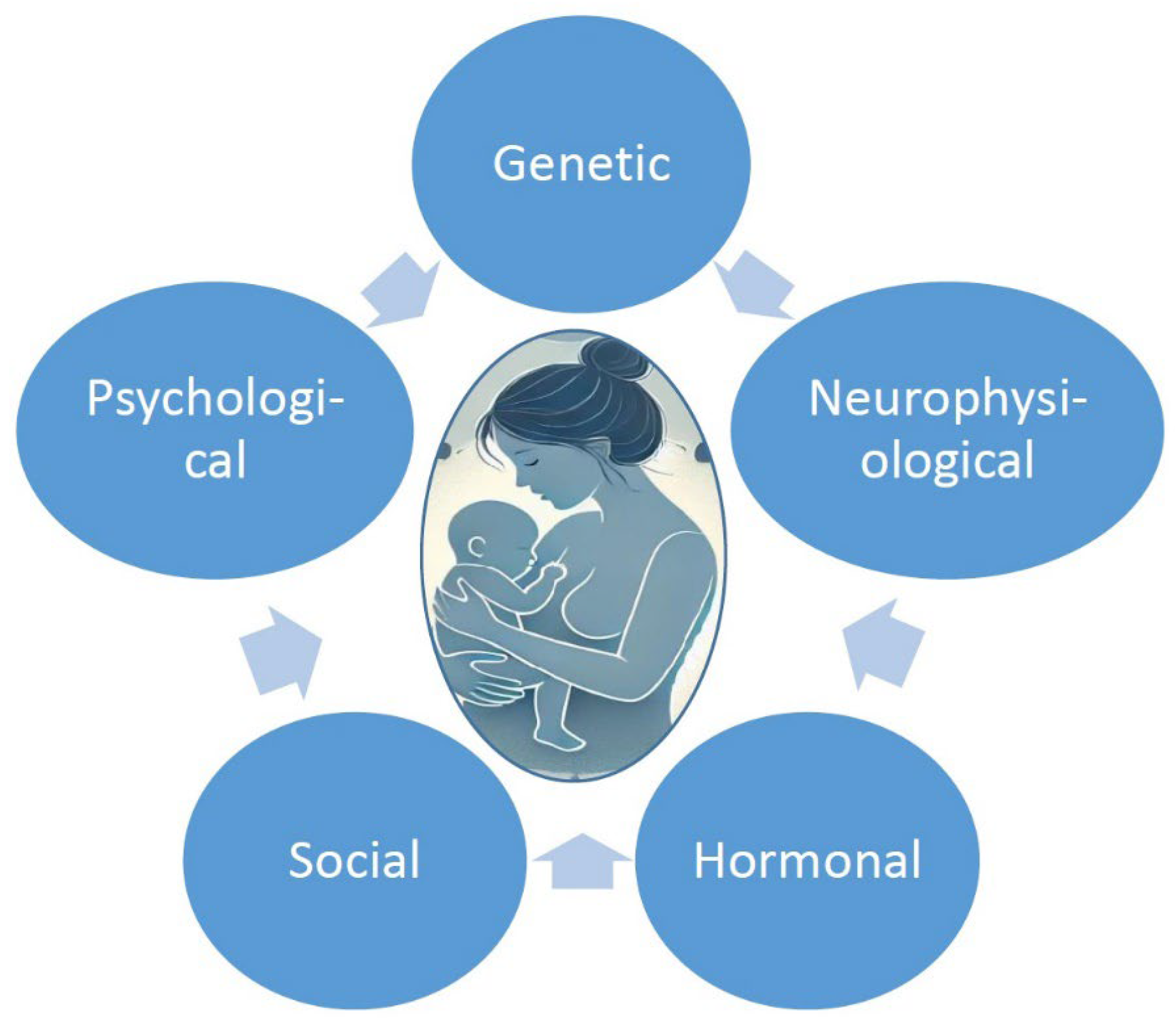
4. Pathophysiology and Risk Factors of Postpartum Depression
5. Symptoms and Diagnosis of Postpartum Depression
6. Association of Maternal Postpartum Depression with Children’s Development
7. Management of Postpartum Depression
8. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- O’Hara, M.W.; McCabe, J.E. Postpartum depression current status and future directions. Annu. Rev. Clin. Psychol. 2013, 9, 379–407. [Google Scholar] [PubMed]
- O’Hara, M.W.; Wisner, K.L. Perinatal mental illness: Definition, description and aetiology. Best Pract. Res. Clin. Obstet. Gynaecol. 2014, 28, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Tosto, V.; Ceccobelli, M.; Lucarini, E.; Tortorella, A.; Gerli, S.; Parazzini, F.; Favilli, A. Maternity Blues: A Narrative Review. J. Pers. Med. 2023, 13, 154. [Google Scholar] [CrossRef] [PubMed]
- Stewart, D.E.; Vigod, S.N. Postpartum Depression: Pathophysiology, Treatment, and Emerging Therapeutics. Annu. Rev. Med. 2019, 70, 183–196. [Google Scholar] [CrossRef]
- Radoš, S.N.; Akik, B.K.; Žutić, M.; Rodriguez-Muñoz, M.F.; Uriko, K.; Motrico, E.; Moreno-Peral, P.; Apter, G.; den Berg, M.L. Diagnosis of peripartum depression disorder: A state-of-the-art approach from the COST Action Riseup-PPD. Compr. Psychiatry 2024, 130, 152456. [Google Scholar]
- Dominiak, M.; Antosik-Wojcinska, A.Z.; Baron, M.; Mierzejewski, P.; Swiecicki, L. Recommendations for the prevention and treatment of postpartum depression. Ginekol. Pol. 2021, 92, 153–164. [Google Scholar] [CrossRef]
- World Health Organization. Thinking Healthy: A Manual for Psychosocial Management of Perinatal Depression; WHO Generic Field-trial Version 1.0; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Lindahl, V.; Pearson, J.L.; Colpe, L. Prevalence of suicidality during pregnancy and the postpartum. Arch. Womens Ment. Health 2005, 8, 77–87. [Google Scholar] [CrossRef] [PubMed]
- Yahya, N.F.S.; Teng, N.I.M.F.; Das, S.; Juliana, N. Nutrition and physical activity interventions to ameliorate postpartum depression: A scoping review. Asia Pac. J. Clin. Nutr. 2021, 30, 662–674. [Google Scholar] [CrossRef]
- Halligan, S.L.; Murray, L.; Martins, C.; Cooper, P.J. Maternal depression and psychiatric outcomes in adolescent offspring: A 13-year longitudinal study. J. Affect. Disord. 2007, 97, 145–154. [Google Scholar]
- Righetti-Veltema, M.; Bousquet, A.; Manzano, J. Impact of postpartum depressive symptoms on mother and her 18-month-old infant. Eur. Child Adolesc. Psychiatry 2003, 12, 75–83. [Google Scholar]
- Righetti-Veltema, M.; Conne-Perréard, E.; Bousquet, A.; Manzano, J. Postpartum depression and mother–infant relationship at 3 months old. J. Affect. Disord. 2002, 70, 291–306. [Google Scholar] [CrossRef] [PubMed]
- Moore Simas, T.A.; Whelan, A.; Byatt, N. Screening Recommendations and Treatments for Postpartum Depression. JAMA 2024, 331, 1300–1301. [Google Scholar] [CrossRef] [PubMed]
- Faravelli, C.; Alessandra Scarpato, M.; Castellini, G.; Lo Sauro, C. Gender differences in depression and anxiety: The role of age. Psychiatry Res. 2013, 210, 1301–1303. [Google Scholar] [CrossRef]
- Sadat, Z.; Abedzadeh-Kalahroudi, M.; Atrian, M.K.; Karimian, Z.; Sooki, Z. The impact of postpartum depression on quality of life in women after child’s birth. Iran. Red. Crescent Med. J. 2014, 16, e14995. [Google Scholar] [CrossRef]
- Gress-Smith, J.L.; Luecken, L.J.; Lemery-Chalfant, K.; Howe, R. Postpartum depression prevalence and impact on infant health, weight, and sleep in low-income and ethnic minority women and infants. Matern. Child. Health J. 2012, 16, 887–893. [Google Scholar] [CrossRef]
- O’Brien, A.P.; McNeil, K.A.; Fletcher, R.; Conrad, A.; Wilson, A.J.; Jones, D.; Chan, S.W. New fathers’ perinatal depression and anxiety—Treatment options: An integrative review. Am. J. Mens. Health 2016, 2016, 1557988316669047. [Google Scholar] [CrossRef]
- Beck, C.T. Predictors of postpartum depression: An update. Nurs. Res. 2001, 50, 275–285. [Google Scholar] [CrossRef]
- Gavin, I.N.; Gaynes, N.B.; Lohr, N.K.; Meltzer-Brody, N.S.; Gartlehner, N.G.; Swinson, N.T. Perinatal depression a systematic review of prevalence and incidence. Obstet. Gynecol. 2005, 106 Pt 1, 1071–1083. [Google Scholar] [CrossRef]
- Wang, Z.; Liu, J.; Shuai, H.; Cai, Z.; Fu, X.; Liu, Y.; Xiao, X.; Zhang, W.; Krabbendam, E.; Liu, S.; et al. Mapping global prevalence of depression among postpartum women. Transl. Psychiatry 2021, 11, 543. [Google Scholar] [CrossRef]
- Li, Y.; Zhao, Q.; Cross, W.M.; Chen, J.; Qin, C.; Sun, M. Assessing the quality of mobile applications targeting postpartum depression in China. Int. J. Ment. Health Nurs. 2020, 29, 772–785. [Google Scholar] [CrossRef]
- Sohr-Preston, S.L.; Scaramella, L.V. Implications of timing of maternal depressive symptoms for early cognitive and language development. Clin. Child Fam. Psychol. Rev. 2006, 9, 65–68. [Google Scholar] [CrossRef] [PubMed]
- Sainuddin, S.S.; Norhayati, M.N.; Abdul Kadir, A.; Zakaria, R. A 10-year systematic review and meta-analysis of determinants of postpartum depression in the Association of Southeast Asian Nations countries. Med. J. Malays. 2023, 78, 675–686. [Google Scholar]
- Liu, X.; Wang, S.; Wang, G. Prevalence and Risk Factors of Postpartum Depression in Women: A Systematic Review and Meta-analysis. J. Clin. Nurs. 2022, 31, 2665–2677. [Google Scholar] [CrossRef] [PubMed]
- Gelaye, B.; Rondon, M.B.; Araya, R.; Williams, M.A. Epidemiology of maternal depression, risk factors, and child outcomes in low-income and middle-income countries. The lancet. Psychiatry 2016, 3, 973–982. [Google Scholar] [CrossRef] [PubMed]
- Parsons, C.E.; Young, K.S.; Rochat, T.J.; Kringelbach, M.L.; Stein, A. Postnatal depression and its effects on child development: A review of evidence from low- and middle-income countries. Br. Med. Bull. 2012, 101, 57–79. [Google Scholar] [CrossRef]
- Fisher, J.; de Mello, M.C.; Patel, V.; Rahman, A.; Tran, T.; Holton, S.; Holmes, W. Prevalence and determinants of common perinatal mental disorders in women in low- and lower-middle-income countries: A systematic review/Prevalence et determinants des troubles mentaux perinataux communs chez les femmes des pays a revenu faible et moyen: Une etude systematique/Prevalencia y determinantes de los trastornos mentales perinatales frecuentes en mujeres en paises de ingresos bajos y medios-bajos: Examen sistematico. Bull. WHO 2012, 90, 139. [Google Scholar] [CrossRef]
- Chechko, N.; Losse, E.; Frodl, T.; Nehls, S. Baby blues, premenstrual syndrome and postpartum affective disorders: Intersection of risk factors and reciprocal influences. BJPsych Open 2023, 10, e3. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chen, J.; Cross, W.M.; Plummer, V.; Lam, L.; Tang, S. A systematic review of prevalence and risk factors of postpartum depression in Chinese immigrant women. Women Birth J. Aust. Coll. Midwives 2019, 32, 487–492. [Google Scholar] [CrossRef]
- Abdollahi, F.; Lye, M.-S.; Zain, A.M.; Ghazali, S.S.; Zarghami, M. Postnatal Depression and Its Associated Factors in Women From Different Cultures. Iran. J. Psychiatry Behav. Sci. 2011, 5, 5–11. [Google Scholar]
- Ishikawa, N.; Goto, S.; Murase, S.; Kanai, A.; Masuda, T.; Aleksic, B.; Usui, H.; Ozaki, N. Prospective study of maternal depressive symptomatology among Japanese women. J. Psychosom. Res. 2011, 71, 264–269. [Google Scholar] [CrossRef]
- Suzuki, S. Prevention of Postpartum Depression by Multidisciplinary Collaboration in Japan. JMA J. 2024, 7, 600–602. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Shafiei, T.; Small, R.; McLachlan, H. Immigrant Afghan women’s emotional well-being after birth and use of health services in Melbourne, Australia. Midwifery 2015, 31, 671–677. [Google Scholar] [CrossRef] [PubMed]
- Canada Statistics. Immigrant Population in Canada, 2016 Census of Population. Available online: https://www150.statcan.gc.ca/n1/pub/11-627-m/11-627-m2017028-eng.htm (accessed on 25 February 2025).
- Zhao, X.H.; Zhang, Z.H. Risk factors for postpartum depression: An evidence-based systematic review of systematic reviews and meta-analyses. Asian J. Psychiatry 2020, 53, 102353. [Google Scholar] [CrossRef]
- Agrawal, I.; Mehendale, A.M.; Malhotra, R. Risk Factors of Postpartum Depression. Cureus 2022, 14, e30898. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Guintivano, J.; Sullivan, P.F.; Stuebe, A.M.; Penders, T.; Thorp, J.; Rubinow, D.R.; Meltzer-Brody, S. Adverse life events; psychiatric history, and biological predictors of postpartum depression in an ethnically diverse sample of postpartum women. Psychol. Med. 2018, 48, 1190–1200. [Google Scholar]
- Maguire, J.; Mody, I. Behavioral Deficits in Juveniles Mediated by Maternal Stress Hormones in Mice. Neural Plast. 2016, 2016, 2762518. [Google Scholar]
- Murgatroyd, C.A.; Taliefar, M.; Bradburn, S.; Carini, L.M.; Babb, J.A.; Nephew, B.C. Social stress during lactation, depressed maternal care, and neuropeptidergic gene expression. Behav. Pharmacol. 2015, 26, 642–653. [Google Scholar]
- Baird, H.; Harris, R.A.; Santos, H.P., Jr. The Effects of Maternal Perinatal Depression on Child IQ: A Systematic Review. Matern. Child Health J. 2023, 27, 1489–1502. [Google Scholar] [CrossRef] [PubMed]
- Horsch, A.; Garthus-Niegel, S.; Ayers, S.; Chandra, P.; Hartmann, K.; Vaisbuch, E.; Lalor, J. Childbirth-related posttraumatic stress disorder: Definition, risk factors, pathophysiology, diagnosis, prevention, and treatment. Am. J. Obstet. Gynecol. 2024, 230, S1116–S1127. [Google Scholar] [CrossRef] [PubMed]
- Forty, L.; Jones, L.; Macgregor, S.; Caesar, S.; Cooper, C.; Hough, A.; Dean, L.; Dave, S.; Farmer, A.; McGuffin, P.; et al. Familiality of Postpartum Depression in Unipolar Disorder: Results of a Family Study. Am. J. Psychiatry 2006, 163, 1549–1553. [Google Scholar]
- Murphy-Eberenz, K.; Zandi, P.P.; March, D.; Crowe, R.R.; Scheftner, W.A.; Alexander, M.; McInnis, M.G.; Adams, P.; DePaulo, J.R.; Miller, E.B.; et al. Is perinatal depression familial? J. Affect. Disord. 2006, 90, 49–55. [Google Scholar] [PubMed]
- Payne, J.L.; Maguire, J. Pathophysiological mechanisms implicated in postpartum depression. Front. Neuroendocr. 2019, 52, 165–180. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mehta, D.; Newport, D.J.; Frishman, G.; Kraus, L.; Rex-Haffner, M.; Ritchie, J.C.; Lori, A.; Knight, B.T.; Stagnaro, E.; Ruepp, A.; et al. Early predictive biomarkers for postpartum depression point to a role for estrogen receptor signaling. Psychol. Med. 2014, 44, 2309–2322. [Google Scholar]
- Binder, E.B.; Newport, D.J.; Zach, E.B.; Smith, A.K.; Deveau, T.C.; Altshuler, L.L.; Cohen, L.S.; Stowe, Z.N.; Cubells, J.F. A serotonin transporter gene polymorphism predicts peripartum depressive symptoms in an at-risk psychiatric cohort. J. Psychiatr. Res. 2010, 44, 640–646. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pinheiro, R.T.; Coelho, F.M.; Silva, R.A.; Pinheiro, K.A.; Oses, J.P.; Quevedo Lde, Á.; Souza, L.D.; Jansen, K.; Zimmermann Peruzatto, J.M.; Manfro, G.G.; et al. Association of a serotonin transporter gene polymorphism (5-HTTLPR) and stressful life events with postpartum depressive symptoms: A population-based study. J. Psychosom. Obs. Gynaecol. 2013, 34, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Fang, M.; Du, X.; Hu, Z. Lucky gene 5-HTTLPR and postpartum depression: A systematic review. Neuro Endocrinol. Lett. 2017, 38, 316–320. [Google Scholar] [PubMed]
- Landoni, M.; Missaglia, S.; Tavian, D.; Ionio, C.; Di Blasio, P. Influence of 5-HTTLPR polymorphism on postpartum depressive and posttraumatic symptoms. Psychiatr. Genet. 2022, 32, 9–14. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Doornbos, B.; Dijck-Brouwer, D.A.J.; Kema, I.P.; Tanke, M.A.C.; van Goor, S.A.; Muskiet, F.A.J.; Korf, J. The development of peripartum depressive symptoms is associated with gene polymorphisms of MAOA, 5-HTT and COMT. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2009, 33, 1250–1254. [Google Scholar] [CrossRef]
- Sacher, J.; Rekkas, P.V.; Wilson, A.A.; Houle, S.; Romano, L.; Hamidi, J.; Rusjan, P.; Fan, I.; Stewart, D.E.; Meyer, J.H. Relationship of monoamine oxidase-A distribution volume to postpartum depression and postpartum crying. Neuropsychopharmacology 2015, 40, 429–435. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ma, J.; Huang, Z.; Wang, S.; Zheng, S.; Duan, K. Postpartum depression: Association with genetic polymorphisms of noradrenaline metabolic enzymes and the risk factors. Nan Fang Yi Ke Da Xue Xue Bao 2019, 39, 57–62. (In Chinese) [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pariante, C.M.; Lightman, S.L. The HPA axis in major depression: Classical theories and new developments. Trends Neurosci. 2008, 31, 464–468. [Google Scholar] [PubMed]
- Chai, Y.; Li, Q.; Wang, Y.; Tao, E.; Asakawa, T. The Value of HPA Axis Hormones as Biomarkers for Screening and Early Diagnosis of Postpartum Depression: Updated Information About Methodology. Front. Endocrinol. 2022, 13, 916611. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dennis, C.L.; Ross, L.E.; Herxheimer, A. Oestrogens and progestins for preventing and treating postpartum depression. Cochrane Database Syst. Rev. 2008, 2008, Cd001690. [Google Scholar] [PubMed]
- Kettunen, P.; Koistinen, E.; Hintikka, J.; Perheentupa, A. Oestrogen therapy for postpartum depression: Efficacy and adverse effects. A double-blind, randomized, placebo-controlled pilot study. Nord. J. Psychiatry 2022, 76, 348–357. [Google Scholar] [CrossRef]
- Sundström-Poromaa, I.; Comasco, E.; Sumner, R.; Luders, E. Progesterone-Friend or foe? Front. Neuroendocrinol. 2020, 59, 100856. [Google Scholar] [CrossRef]
- Henshaw, E.J. Breastfeeding and Postpartum Depression: A Review of Relationships and Potential Mechanisms. Curr. Psychiatry Rep. 2023, 25, 803–808. [Google Scholar] [CrossRef] [PubMed]
- Bell, A.F.; Erickson, E.N.; Carter, C.S. Beyond labor: The role of natural and synthetic oxytocin in the transition to motherhood. J. Midwifery Women’s Health 2014, 59, 35–42. [Google Scholar]
- Thul, T.A.; Corwin, E.J.; Carlson, N.S.; Brennan, P.A.; Young, L.J. Oxytocin and postpartum depression: A systematic review. Psychoneuroendocrinology 2020, 120, 104793. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pedersen, C.A.; Johnson, J.L.; Silva, S.; Bunevicius, R.; Meltzer-Brody, S.; Hamer, R.M.; Leserman, J. Antenatal thyroid correlates of postpartum depression. Psychoneuroendocrinology 2007, 32, 235–245. [Google Scholar]
- Bloch, M.; Schmidt, P.J.; Danaceau, M.; Murphy, J.; Nieman, L.; Rubinow, D.R. Effects of Gonadal Steroids in Women with a History of Postpartum Depression. Am. J. Psychiatry 2000, 157, 924–930. [Google Scholar]
- Bloch, M.; Daly, R.C.; Rubinow, D.R. Endocrine factors in the etiology of postpartum depression. Compr. Psychiatry 2003, 44, 234–246. [Google Scholar] [CrossRef] [PubMed]
- Schiller, C.E.; Meltzer-Brody, S.; Rubinow, D.R. The role of reproductive hormones in postpartum depression. CNS Spectr. 2015, 20, 48–59. [Google Scholar] [CrossRef] [PubMed]
- Stuebe, A.M.; Grewen, K.; Meltzer-Brody, S. Association Between Maternal Mood and Oxytocin Response to Breastfeeding. J. Women’s Health 2013, 22, 352–361. [Google Scholar] [CrossRef]
- Mah, B.L.; Van Ijzendoorn, M.H.; Out, D.; Smith, R.; Bakermans-Kranenburg, M.J. The Effects of Intranasal Oxytocin Administration on Sensitive Caregiving in Mothers with Postnatal Depression. Child Psychiatry Hum. Dev. 2017, 48, 308–315. [Google Scholar] [CrossRef]
- Whitley, J.; Wouk, K.; Bauer, A.E.; Grewen, K.; Gottfredson, N.C.; Meltzer-Brody, S.; Propper, C.; Mills-Koonce, R.; Pearson, B.; Stuebe, A. Oxytocin during breastfeeding and maternal mood symptoms. Psychoneuroendocrinology 2020, 113, 104581. [Google Scholar] [CrossRef]
- Cheng, B.; Hu, X.; Roberts, N.; Zhao, Y.; Xu, X.; Zhou, Y.; Tan, X.; Chen, S.; Meng, Y.; Wang, S.; et al. Prolactin mediates the relationship between regional gray matter volume and postpartum depression symptoms. J. Affect. Disord. 2022, 301, 253–259. [Google Scholar] [CrossRef]
- Wiciński, M.; Malinowski, B.; Puk, O.; Socha, M.; Słupski, M. Methyldopa as an inductor of postpartum depression and maternal blues: A review. Biomed. Pharmacother. Biomed. Pharmacother. 2020, 127, 110196. [Google Scholar] [CrossRef]
- Ikeda, M.; Kamibeppu, K. Measuring the risk factors for postpartum depression: Development of the Japanese version of the Postpartum Depression Predictors Inventory-Revised (PDPI-R-J). BMC Pregnancy Childbirth 2013, 127, 112. [Google Scholar] [CrossRef]
- Beck, C.T.; Gable, R.K. Postpartum depression screening scale: Development and psychometric testing. Nurs. Res. 2000, 49, 272–282. [Google Scholar] [CrossRef]
- Mirsalimi, F.; Ghofranipour, F.; Noroozi, A.; Montazeri, A. The postpartum depression literacy scale (PoDLiS): Development and psychometric properties. BMC Pregnancy Childbirth 2020, 20, 13. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Alves, S.; Fonseca, A.; Canavarro, M.C.; Pereira, M. Preliminary Psychometric Testing of the Postpartum Depression Predictors Inventory-Revised (PDPI-R) in Portuguese Women. Matern. Child Health J. 2018, 22, 571–578. [Google Scholar] [CrossRef] [PubMed]
- Records, K.; Rice, M.; Beck, C.T. Psychometric assessment of the postpartum depression predictors inventory-revised. J. Nurs. Meas. 2007, 15, 189–202. [Google Scholar] [PubMed]
- Bagheri, P.; Rostami, M. Postpartum depression and suicide in Iran. Womens Health 2021, 17, 17455065211043994. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lee, Y.L.; Tien, Y.; Bai, Y.S.; Lin, C.K.; Yin, C.S.; Chung, C.H.; Sun, C.A.; Huang, S.H.; Huang, Y.C.; Chien, W.C.; et al. Association of Postpartum Depression with Maternal Suicide: A Nationwide Population-Based Study. Int. J. Environ. Res. Public. Health 2022, 19, 5118. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Huang, R.S.; Spence, A.R.; Abenhaim, H.A. Non-Obstetric Maternal Mortality Trends by Race in the United States. Matern. Child Health J. 2024, 28, 895–904. [Google Scholar] [CrossRef] [PubMed]
- Moya, E.; Larson, L.M.; Stewart, R.C.; Fisher, J.; Mwangi, M.N.; Phiri, K.S. Reliability and validity of depression anxiety stress scale (DASS)-21 in screening for common mental disorders among postpartum women in Malawi. BMC Psychiatry 2022, 22, 352. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Braverman, J.; Roux, J. Screening for the patient at risk for postpartum depression. Obs. Gynecol. 1978, 52, 731–736. [Google Scholar]
- Beck, C.T. Revision of the postpartum depression predictors inventory. J. Obs. Gynecol. Neonatal Nurs. 2002, 31, 394–402. [Google Scholar]
- Beck, C.T. A meta-analysis of predictors of postpartum depression. Nurs. Res. 1996, 45, 297–303. [Google Scholar]
- Beck, A.T.; Steer, R.A. Manual for the Beck Anxiety Inventory; Psychological Corporation: San Antonio, TX, USA, 1990. [Google Scholar]
- Conradt, E.; Manian, N.; Bornstein, M.H. Screening for Depression in the Postpartum using the Beck Depression Inventory-II: What Logistic Regression Reveals. J. Reprod. Infant. Psychol. 2012, 30, 427–435. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Su, K.P.; Chiu, T.H.; Huang, C.L.; Ho, M.; Lee, C.C.; Wu, P.L.; Lin, C.Y.; Liau, C.H.; Liao, C.C.; Chiu, W.C.; et al. Different cutoff points for different trimesters? The use of Edinburgh Postnatal Depression Scale and Beck Depression Inventory to screen for depression in pregnant Taiwanese women. Gen. Hosp. Psychiatry 2007, 29, 436–441. [Google Scholar] [CrossRef] [PubMed]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [PubMed]
- Oliveira, T.A.; Luzetti, G.G.; Rosalém, M.M.; Neto, C.M. Screening of Perinatal Depression Using the Edinburgh Postpartum Depression Scale. Rev. Bras. De Ginecol. E Obs./RBGO Gynecol. Obstet. 2022, 44, 452–457. [Google Scholar] [CrossRef]
- Park, S.H.; Kim, J.I. Predictive validity of the Edinburgh postnatal depression scale and other tools for screening depression in pregnant and postpartum women: A systematic review and meta-analysis. Arch. Gynecol. Obstet. 2023, 307, 1331–1345. [Google Scholar] [CrossRef]
- Levis, B.; Negeri, Z.; Sun, Y.; Benedetti, A.; Thombs, B.D. Accuracy of the Edinburgh Postnatal Depression Scale (EPDS) for screening to detect major depression among pregnant and postpartum women: Systematic review and meta-analysis of individual participant data. BMJ 2020, 371, m4022. [Google Scholar] [CrossRef]
- Adouard, F.; Glangeaud-Freudenthal, N.M.C.; Golse, B. Validation of the Edinburgh postnatal depression scale (EPDS) in a sample of women with high-risk pregnancies in France. Arch. Womens Ment. Health 2005, 8, 89–95. [Google Scholar]
- Kubota, C.; Okada, T.; Aleksic, B.; Nakamura, Y.; Kunimoto, S.; Morikawa, M.; Shiino, T.; Tamaji, A.; Ohoka, H.; Banno, N.; et al. Factor structure of the Japanese version of the Edinburgh postnatal depression scale in the postpartum period. PLoS ONE 2014, 9, e103941. [Google Scholar]
- Small, R.; Lumley, J.; Yelland, J.; Brown, S. The performance of the Edinburgh postnatal depression scale in english speaking and non-English speaking populations in Australia. Soc. Psychiatry Psychiatr. Epidemiol. 2007, 42, 70–78. [Google Scholar]
- Kotz, J.; Marriott, R.; Reid, C. The EPDS and Australian Indigenous women: A systematic review of the literature. Women Birth J. Aust. Coll. Midwives 2021, 34, e128–e134. [Google Scholar] [CrossRef]
- Chávez-Tostado, M.; Chávez-Tostado, K.V.; Cervantes-Guevara, G.; Cervantes-Cardona, G.; Hernandez-Corona, D.M.; González-Heredia, T.; Méndez-del Villar, M.; Corona-Meraz, F.I.; Guzmán-Ornelas, M.O.; Barbosa-Camacho, F.J.; et al. Breastfeeding Practices and Postpartum Depression in Mexican Women during the COVID-19 Pandemic: A Cross-Sectional Study. Medicina 2023, 59, 1330. [Google Scholar] [CrossRef]
- King, P.A.L. Replicability of structural models of the Edinburgh Postnatal Depression Scale (EPDS) in a community sample of postpartum African American women with low socioeconomic status. Arch. Womens Ment. Health 2012, 15, 77–86. [Google Scholar] [PubMed]
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [PubMed]
- Price DA, M.; Middleton, M.M.; Matthey AA, P.S.; Goldfeld, P.S.; Kemp, P.L.; Orsini, M.F. A comparison of two measures to screen for mental health symptoms in pregnancy and early postpartum: The Matthey Generic Mood Questionnaire and the Depression, Anxiety, Stress Scales short-form. J. Affect. Disord. 2021, 281, 824–833. [Google Scholar] [CrossRef]
- Maxwell, D.; Robinson, S.R.; Rogers, K. “I keep it to myself”: A qualitative meta-interpretive synthesis of experiences of postpartum depression among marginalised women. Health Soc. Care Community 2018, 27, e23–e36. [Google Scholar] [CrossRef]
- Luoma, I.; Tamminen, T.; Kaukonen, P.; Laippala, P.; Puura, K.; Salmelin, R.; Almqvist, F. Longitudinal study of maternal depressive symptoms and child well-being. J. Am. Acad. Child. Adolesc. Psychiatry 2001, 40, 1367–1374. [Google Scholar]
- Schechter, J.C.; Brennan, P.A.; Smith, A.K.; Stowe, Z.N.; Newport, D.J.; Johnson, K.C. Maternal prenatal psychological distress and preschool cognitive functioning: The protective role of positive parental engagement. J. Abnorm. Child. Psychol. 2016, 45, 249–260. [Google Scholar] [CrossRef]
- Evans, J.; Melotti, R.; Heron, J.; Ramchandani, P.; Wiles, N.; Murray, L.; Stein, A. The timing of maternal depressive symptoms and child cognitive development: A longitudinal study. J. Child. Psychol. Psychiatry 2011, 53, 632–640. [Google Scholar] [CrossRef]
- Faleschini, S.; Rifas-Shiman, S.; Tiemeier, H.; Oken, E.; Hivert, M.F. Associations of prenatal and postnatal maternal depressive symptoms with ofspring cognition and behavior in Mid-Childhood: A prospective cohort study. Int. J. Environ. Res. Public Health 2019, 16, 1007. [Google Scholar] [CrossRef]
- Walker, L.O. Maternal postpartum health and its impact on health and development of young children. Womens Health Nurs. 2024, 30, 96–100. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Murray, L.; Arteche, A.; Fearon, P.; Halligan, S.; Croudace, T.; Cooper, P. The efects of maternal postnatal depression and child sex on academic performance at age 16 years: A developmental approach. J. Child. Psychol. Psychiatry 2010, 51, 1150–1159. [Google Scholar] [CrossRef]
- Amani, B.; Merza, D.; Savoy, C.; Streiner, D.; Bieling, P.; Ferro, M.A.; Van Lieshout, R.J. Peer-Delivered Cognitive-Behavioral Therapy for Postpartum Depression: A Randomized Controlled Trial. J. Clin. Psychiatry 2021, 83, 21m13928. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Laplante, D.P.; Paquin, V.; Lafortune, S.; Elgbeili, G.; King, S. Effectiveness of cognitive behavioral therapy for perinatal maternal depression, anxiety and stress: A systematic review and meta-analysis of randomized controlled trials. Clin. Psychol. Rev. 2022, 92, 102129. [Google Scholar] [CrossRef] [PubMed]
- Spelke, M.B.; Paul, R.; Blette, B.S.; Meltzer-Brody, S.; Schiller, C.E.; Ncheka, J.M.; Kasaro, M.P.; Price, J.T.; Stringer, J.S.A.; Stringer, E.M. Interpersonal therapy versus antidepressant medication for treatment of postpartum depression and anxiety among women with HIV in Zambia: A randomized feasibility trial. J. Int. AIDS Soc. 2022, 25, e25959. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Guille, C.; Newman, R.; Fryml, L.D.; Lifton, C.K.; Epperson, C.N. Management of postpartum depression. J. Midwifery Womens Health 2013, 58, 643–653. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Treatment and Management of Mental Health Conditions During Pregnancy and Postpartum: ACOG Clinical Practice Guideline No. 5. Obstet. Gynecol. 2023, 141, 1262–1288. [CrossRef] [PubMed]
- Kroska, E.B.; Stowe, Z.N. Postpartum Depression: Identification and Treatment in the Clinic Setting. Obs. Gynecol. Clin. N. Am. 2020, 47, 409–419. [Google Scholar] [CrossRef] [PubMed]
- Pettman, D.; O’Mahen, H.; Blomberg, O.; Svanberg, A.S.; von Essen, L.; Woodford, J. Effectiveness of cognitive behavioural therapy-based interventions for maternal perinatal depression: A systematic review and meta-analysis. BMC Psychiatry 2023, 23, 208. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dennis, C.L.; Ravitz, P.; Grigoriadis, S.; Jovellanos, M.; Hodnett, E.; Ross, L.; Zupancic, J. The effect of telephone-based interpersonal psychotherapy for the treatment of postpartum depression: Study protocol for a randomized controlled trial. Trials 2012, 13, 38. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Prevatt, B.S.; Lowder, E.M.; Desmarais, S.L. Peer-support intervention for postpartum depression: Participant satisfaction and program effectiveness. Midwifery 2018, 64, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Dennis, C.L. Postpartum depression peer support: Maternal perceptions from a randomized controlled trial. Int. J. Nurs. Stud. 2010, 47, 560–568. [Google Scholar] [CrossRef] [PubMed]
- Cornett, E.M.; Rando, L.; Labbé, A.M.; Perkins, W.; Kaye, A.M.; Kaye, A.D.; Viswanath, O.; Urits, I. Brexanolone to Treat Postpartum Depression in Adult Women. Psychopharmacol. Bull. 2021, 51, 115–130. [Google Scholar] [PubMed] [PubMed Central]
- Deligiannidis, K.M.; Meltzer-Brody, S.; Maximos, B.; Peeper, E.Q.; Freeman, M.; Lasser, R.; Bullock, A.; Kotecha, M.; Li, S.; Forrestal, F.; et al. Zuranolone for the Treatment of Postpartum Depression. Am. J. Psychiatry 2023, 180, 668–675, Erratum in: Am. J. Psychiatry 2024, 182, 3. [Google Scholar] [CrossRef] [PubMed]
- Hutcherson, T.C.; Cieri-Hutcherson, N.E.; Gosciak, M.F. Brexanolone for postpartum depression. Am. J. Health Syst. Pharm. 2020, 77, 336–345. [Google Scholar] [CrossRef] [PubMed]
- Suryawanshi, O., 4th; Pajai, S. A Comprehensive Review on Postpartum Depression. Cureus 2022, 14, e32745. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]



{kind=link}
{kind=link}
{kind=link}
| Prevalence/Incidence | Population/Region | Socioeconomic/Clinical Context | Clinical Insights | Socioeconomic/Healthcare Factors | Study/Source |
|---|---|---|---|---|---|
| 10–17% | Global | Mixed (high- and low-income countries) | General prevalence of PPD | Potential underdiagnosis in low-resource settings | [19] |
| 7% to 40% | Developed countries (including Japan and China) | High-income, better mental health support | Variation in PPD prevalence due to healthcare access | Differences in mental health support and social services | [23] |
| 20% | Low- and middle-income countries | Limited mental health resources, high stigma | High prevalence of non-psychotic postpartum mental disorders | Barriers to accessing care and societal stigma | [27] |
| 3.5% to 63.3% | Asian countries (including China) | Diverse cultural and socioeconomic backgrounds | Cultural beliefs and economic factors influencing PPD | Significant healthcare disparities within the region | [23] |
| 55% | European women | High-income, specific regional contexts | Exceptionally high PPD prevalence in specific populations | Possible influence of cultural and regional stressors | [28] |
| 30% | Afghan immigrant women in Australia | Immigrant group, socio-cultural challenges | Increased PPD risk due to resettlement stress | Potential lack of culturally sensitive support systems | [29] |
| Up to 60% | Various regions | Mixed (extreme cases in vulnerable groups) | Highest reported PPD prevalence | Often seen in underrepresented or high-risk populations | [21] |
| Factor/Mechanism | Specific Elements | Clinical Impact | Study/Source |
|---|---|---|---|
| Genetic Factors | Estrogen receptor α gene, serotonin transporter gene, MAOA gene polymorphisms | Increased vulnerability to PPD, particularly after childbirth | [44,45,51,52] |
| Neuroendocrine Factors |
| Dysregulation of stress response, impact on mood, emotion regulation contribute to PPD symptoms | [35,53,54,55,56,57,58,59,60,61] |
| Neuroinflammatory Changes | Hormonal withdrawal (ovarian-steroid-withdrawal hypothesis) | Association with mood disorders and increased PPD risk | [62,63] |
| Psychological and Social Factors | Previous negative life events, stress, anxiety, depression history, marital/financial challenges | Increased risk of PPD, impaired mother–child bonding | [37,38,39,40,41] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khamidullina, Z.; Marat, A.; Muratbekova, S.; Mustapayeva, N.M.; Chingayeva, G.N.; Shepetov, A.M.; Ibatova, S.S.; Terzic, M.; Aimagambetova, G. Postpartum Depression Epidemiology, Risk Factors, Diagnosis, and Management: An Appraisal of the Current Knowledge and Future Perspectives. J. Clin. Med. 2025, 14, 2418. https://doi.org/10.3390/jcm14072418
Khamidullina Z, Marat A, Muratbekova S, Mustapayeva NM, Chingayeva GN, Shepetov AM, Ibatova SS, Terzic M, Aimagambetova G. Postpartum Depression Epidemiology, Risk Factors, Diagnosis, and Management: An Appraisal of the Current Knowledge and Future Perspectives. Journal of Clinical Medicine. 2025; 14(7):2418. https://doi.org/10.3390/jcm14072418
Chicago/Turabian StyleKhamidullina, Zaituna, Aizada Marat, Svetlana Muratbekova, Nagima M. Mustapayeva, Gulnar N. Chingayeva, Abay M. Shepetov, Syrdankyz S. Ibatova, Milan Terzic, and Gulzhanat Aimagambetova. 2025. "Postpartum Depression Epidemiology, Risk Factors, Diagnosis, and Management: An Appraisal of the Current Knowledge and Future Perspectives" Journal of Clinical Medicine 14, no. 7: 2418. https://doi.org/10.3390/jcm14072418
APA StyleKhamidullina, Z., Marat, A., Muratbekova, S., Mustapayeva, N. M., Chingayeva, G. N., Shepetov, A. M., Ibatova, S. S., Terzic, M., & Aimagambetova, G. (2025). Postpartum Depression Epidemiology, Risk Factors, Diagnosis, and Management: An Appraisal of the Current Knowledge and Future Perspectives. Journal of Clinical Medicine, 14(7), 2418. https://doi.org/10.3390/jcm14072418