

Prevalence and Cardiopulmonary Characteristics of Post-COVID Syndrome at a Hungarian Tertiary Referral Hospital

 , ,
, ,  ,
,  , , , , , ,
, , , , , ,
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Population Characteristics
3.2. Post-COVID Symptoms
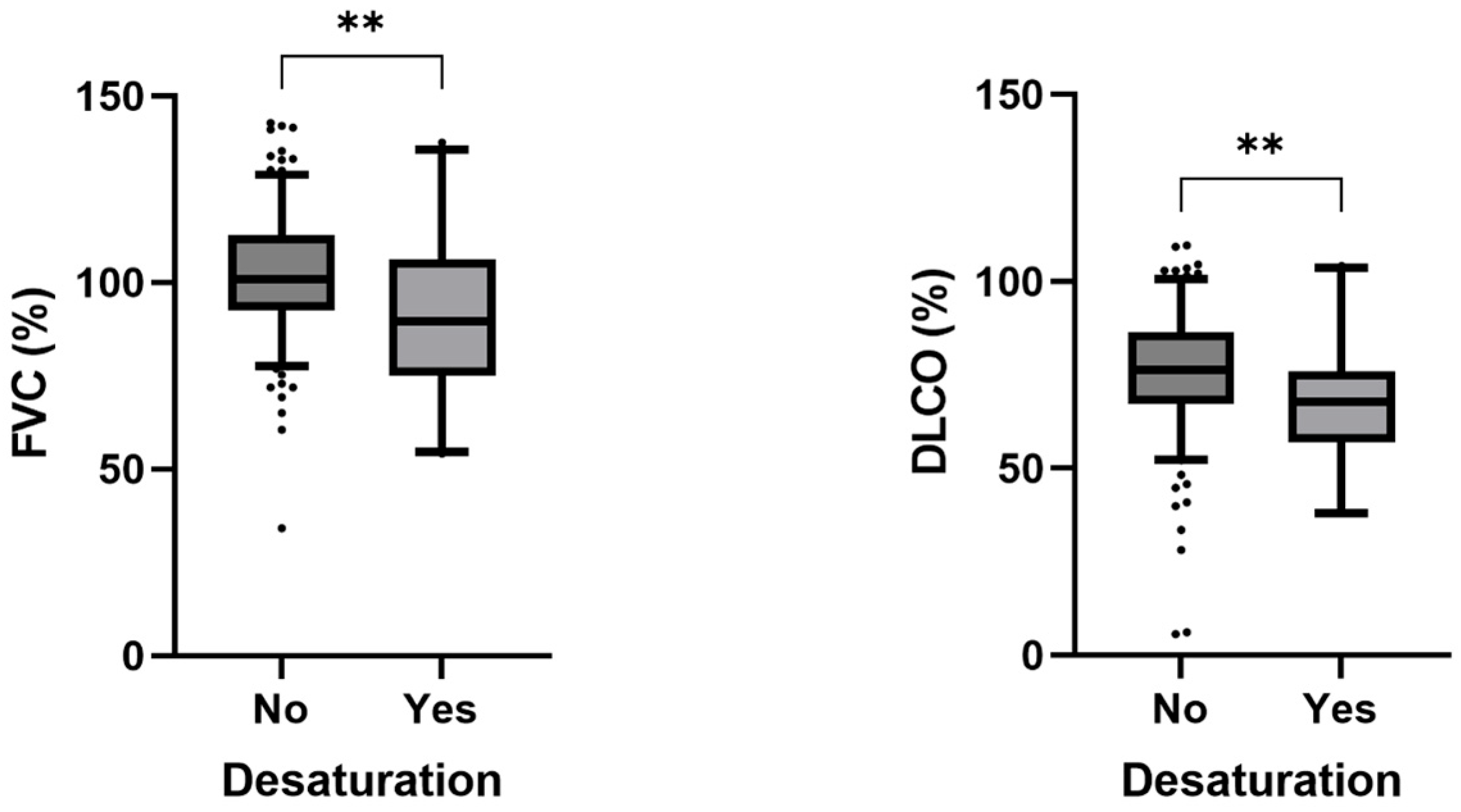
3.3. Clinical Testing
3.4. Laboratory Testing
3.5. Length of Hospital Stay
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| 6MWT | 6-Minute Walk Test |
| BMI | Body Mass Index |
| BNP | Brain Natriuretic Peptide |
| CAC | COVID-19-Associated Coagulopathy |
| COPD | Chronic Obstructive Pulmonary Disease |
| COVID | Coronavirus Disease |
| CRP | C-Reactive Protein |
| DLCO | Diffusion Lung Capacity for Carbon Monoxide |
| DM | Diabetes Mellitus |
| ECG | Electrocardiogram |
| ERS | European Respiratory Society |
| ESC | European Society of Cardiology |
| FEV1 | Forced Expiratory Volume in the First Second |
| FVC | Forced Vital Capacity |
| GE | General Electric |
| GP | General Practitioner |
| hs | High Sensitivity |
| HT | Hypertension |
| ICU | Intensive Care Unit |
| Ig | Immunoglobulin |
| IL | Interleukin |
| IHME | Institute for Health Metrics and Evaluation |
| LA | Lupus Anticoagulant |
| LV | Left Ventricular |
| LVEF | Left Ventricular Ejection Fraction |
| LVIDd | Left Ventricular Internal Diameter in Diastole |
| LVIDs | Left Ventricular Internal Diameter in Systole |
| OR | Odds Ratio |
| NTproBNP | N-terminal proBNP |
| PACS | Post-Acute COVID-19 Syndrome |
| rt-PCR | Real time-Polymerase Chain Reaction |
| SARS-CoV-2 | Severe Acute Respiratory Syndrome-Coronavirus-2 |
| SEM | Standard Error of the Mean |
| TTE | Transthoracic Echocardiography |
References
- COVID—Coronavirus Statistics—Worldometer. Available online: https://www.worldometers.info/coronavirus/ (accessed on 23 May 2024).
- COVID-19—Institute for Health Metrics and Evaluation. Available online: https://www.healthdata.org/research-analysis/diseases-injuries/covid (accessed on 23 May 2024).
- Oke, J.; Heneghan, C. Global COVID-19 Case Fatality Rates. Available online: http://cebm.net/covid-19/global-covid-19-case-fatality-rates/ (accessed on 23 May 2024).
- Chams, N.; Chams, S.; Badran, R.; Shams, A.; Araji, A.; Raad, M.; Mukhopadhyay, S.; Stroberg, E.; Duval, E.J.; Barton, L.M.; et al. COVID-19: A Multidisciplinary Review. Front. Public Health 2020, 8, 383. [Google Scholar] [CrossRef] [PubMed]
- Ahirwar, A.K.; Takhelmayum, R.; Sakarde, A.; Rathod, B.D.; Jha, P.K.; Kumawat, R.; Gopal, N. The study of serum hsCRP, ferritin, IL-6 and plasma D-dimer in COVID-19: A retrospective study. Horm. Mol. Biol. Clin. Investig. 2022, 43, 337–344. [Google Scholar] [CrossRef]
- Chen, C.; Haupert, S.R.; Zimmermann, L.; Shi, X.; Fritsche, L.G.; Mukherjee, B. Global Prevalence of Post-Coronavirus Disease 2019 (COVID-19) Condition or Long COVID: A Meta-Analysis and Systematic Review. J. Infect. Dis. 2022, 226, 1593–1607. [Google Scholar] [CrossRef] [PubMed]
- Sk Abd Razak, R.; Ismail, A.; Abdul Aziz, A.F.; Suddin, L.S.; Azzeri, A.; Sha’ari, N.I. Post-COVID syndrome prevalence: A systematic review and meta-analysis. BMC Public Health 2024, 24, 1785. [Google Scholar] [CrossRef]
- Scholkmann, F.; May, C.A. COVID-19, post-acute COVID-19 syndrome (PACS, “long COVID”) and post-COVID-19 vaccination syndrome (PCVS, “post-COVIDvac-syndrome”): Similarities and differences. Pathol. Res. Pract. 2023, 246, 154497. [Google Scholar] [CrossRef]
- Turner, S.; Khan, M.A.; Putrino, D.; Woodcock, A.; Kell, D.B.; Pretorius, E. Long COVID: Pathophysiological factors and abnormalities of coagulation. Trends Endocrinol. Metab. 2023, 34, 321–344. [Google Scholar] [CrossRef] [PubMed]
- Castanares-Zapatero, D.; Chalon, P.; Kohn, L.; Dauvrin, M.; Detollenaere, J.; Maertens de Noordhout, C.; Primus-de Jong, C.; Cleemput, I.; Van den Heede, K. Pathophysiology and mechanism of long COVID: A comprehensive review. Ann. Med. 2022, 54, 1473–1487. [Google Scholar] [CrossRef]
- Davis, H.E.; McCorkell, L.; Vogel, J.M.; Topol, E.J. Long COVID: Major findings, mechanisms and recommendations. Nat. Rev. Microbiol. 2023, 21, 133–146. [Google Scholar] [CrossRef]
- van Kessel, S.A.M.; Olde Hartman, T.C.; Lucassen, P.L.B.J.; van Jaarsveld, C.H.M. Post-acute and long-COVID-19 symptoms in patients with mild diseases: A systematic review. Fam. Pract. 2022, 39, 159–167. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–270. [Google Scholar] [CrossRef]
- Stanojevic, S.; Kaminsky, D.A.; Miller, M.R.; Thompson, B.; Aliverti, A.; Barjaktarevic, I.; Cooper, B.G.; Culver, B.; Derom, E.; Hall, G.L.; et al. ERS/ATS technical standard on interpretive strategies for routine lung function tests. Eur. Respir. J. 2022, 60, 2101499. [Google Scholar] [CrossRef] [PubMed]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef]
- 6 Minute Walk Test Calculator. Available online: https://www.omnicalculator.com/health/6-minute-walk-test (accessed on 13 July 2024).
- Anaya, J.M.; Rojas, M.; Salinas, M.L.; Rodríguez, Y.; Roa, G.; Lozano, M.; Rodríguez-Jiménez, M.; Montoya, N.; Zapata, E.; Post-COVID Study Group; et al. Post-COVID syndrome. A case series and comprehensive review. Autoimmun. Rev. 2021, 20, 102947. [Google Scholar] [CrossRef]
- Duggal, P.; Penson, T.; Manley, H.N.; Vergara, C.; Munday, R.M.; Duchen, D.; Linton, E.A.; Zurn, A.; Keruly, J.C.; Mehta, S.H.; et al. Post-sequelae symptoms and comorbidities after COVID-19. J. Med. Virol. 2022, 94, 2060–2066. [Google Scholar] [CrossRef]
- Puntmann, V.O.; Shchendrygina, A.; Bolanos, C.R.; Madjiguène Ka, M.; Valbuena, S.; Rolf, A.; Escher, F.; Nagel, E. Cardiac Involvement Due to COVID-19: Insights from Imaging and Histopathology. Eur. Cardiol. 2023, 18, e58. [Google Scholar] [CrossRef] [PubMed]
- Baum, P.; Do, L.; Deterding, L.; Lier, J.; Kunis, I.; Saur, D.; Classen, J.; Wirtz, H.; Laufs, U. Cardiac function in relation to functional status and fatigue in patients with post-COVID syndrome. Sci. Rep. 2022, 12, 19575. [Google Scholar] [CrossRef]
- Wen, H.; Huapaya, J.A.; Kanth, S.M.; Sun, J.; Matthew, B.P.; Lee, S.C.; Do, M.; Chen, M.Y.; Malayeri, A.A.; Suffredini, A.F. Quantitative CT Metrics Associated with Variability in the Diffusion Capacity of the Lung of Post-COVID-19 Patients with Minimal Residual Lung Lesions. J. Imaging 2023, 9, 150. [Google Scholar] [CrossRef] [PubMed]
- Torres-Castro, R.; Vasconcello-Castillo, L.; Alsina-Restoy, X.; Solis-Navarro, L.; Burgos, F.; Puppo, H.; Vilaró, J. Respiratory function in patients post-infection by COVID-19: A systematic review and meta-analysis. Pulmonology 2021, 27, 328–337. [Google Scholar] [CrossRef]
- Sonnweber, T.; Sahanic, S.; Pizzini, A.; Luger, A.; Schwabl, C.; Sonnweber, B.; Kurz, K.; Koppelstätter, S.; Haschka, D.; Petzer, V.; et al. Cardiopulmonary recovery after COVID-19: An observational prospective multicentre trial. Eur. Respir. J. 2021, 57, 2003481. [Google Scholar] [CrossRef]
- Tanni, S.E.; Fabro, A.T.; de Albuquerque, A.; Ferreira, E.V.M.; Verrastro, C.G.Y.; Sawamura, M.V.Y.; Ribeiro, S.M.; Baldi, B.G. Pulmonary fibrosis secondary to COVID-19: A narrative review. Expert Rev. Respir. Med. 2021, 15, 791–803. [Google Scholar] [CrossRef]
- Dotan, A.; Muller, S.; Kanduc, D.; David, P.; Halpert, G.; Shoenfeld, Y. The SARS-CoV-2 as an instrumental trigger of autoimmunity. Autoimmun. Rev. 2021, 20, 102792. [Google Scholar] [CrossRef] [PubMed]
- Rasool, Z.S.; Tiwari, V. Biochemistry, Lupus Anticoagulant. Available online: https://www.ncbi.nlm.nih.gov/books/NBK544357/ (accessed on 23 May 2024).
- Zlatković-Švenda, M.; Rašić, M.; Ovuka, M.; Pavlov-Dolijanović, S.; Atanasković Popović, M.; Ogrič, M.; Žigon, P.; Sodin-Šemrl, S.; Zdravković, M.; Radunović, G. The New Occurrence of Antiphospholipid Syndrome in Severe COVID-19 Cases with Pneumonia and Vascular Thrombosis Could Explain the Post-COVID Syndrome. Biomedicines 2025, 13, 516. [Google Scholar] [CrossRef] [PubMed]
- Kuniyoshi, Y. Persistent Lupus Anticoagulant Positivity and Long-Term Sequelae Following Mild COVID-19. Cureus 2024, 16, e72668. [Google Scholar] [CrossRef]
- Emmenegger, M.; Emmenegger, V.; Shambat, S.M.; Scheier, T.C.; Gomez-Mejia, A.; Chang, C.C.; Wendel-Garcia, P.D.; Buehler, P.K.; Buettner, T.; Roggenbuck, D.; et al. Antiphospholipid antibodies are enriched post-acute COVID-19 but do not modulate the thrombotic risk. Clin. Immunol. 2023, 257, 109845. [Google Scholar] [CrossRef] [PubMed]
- Pisareva, E.; Badiou, S.; Mihalovičová, L.; Mirandola, A.; Pastor, B.; Kudriavtsev, A.; Berger, M.; Roubille, C.; Fesler, P.; Klouche, K.; et al. Persistence of neutrophil extracellular traps and anticardiolipin auto-antibodies in post-acute phase COVID-19 patients. J. Med. Virol. 2023, 95, e28209. [Google Scholar] [CrossRef]
- Bertin, D.; Kaphan, E.; Weber, S.; Babacci, B.; Arcani, R.; Faucher, B.; Ménard, A.; Brodovitch, A.; Mege, J.L.; Bardin, N. Persistent IgG anticardiolipin autoantibodies are associated with post-COVID syndrome. Int. J. Infect. Dis. 2021, 113, 23–25. [Google Scholar] [CrossRef]
- Cimolai, N. Untangling the Intricacies of Infection, Thrombosis, Vaccination, and Antiphospholipid Antibodies for COVID-19. SN Compr. Clin. Med. 2021, 3, 2093–2108. [Google Scholar] [CrossRef]
- Smoking of Tobacco Products by Sex, Age and Country of Citizenship. Available online: https://ec.europa.eu/eurostat/databrowser/view/hlth_ehis_sk1c$defaultview/default/table?lang=en (accessed on 23 May 2024).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Comorbidity | Total | Treated at Home | Hospitalized | OR a | p-Value a |
|---|---|---|---|---|---|
| Diabetes mellitus | 15.1% | 11.4% | 23.7% | 2.42 | 0.012 |
| Hypertension | 42.8% | 35.2% | 60.5% | 2.82 | <0.001 |
| COPD | 1.2% | 0.6% | 2.6% | 3.93 | 0.22 |
| Bronchial asthma | 8.7% | 8.5% | 9.2% | 1.09 | 0.81 |
| Thromboembolic events | 5.9% | 5.7% | 6.6% | 1.17 | 0.78 |
| Symptom/Complaint | Frequency |
|---|---|
| Fatigue, weakness, or reduced exercise tolerance | 74 (29.4%) |
| Dyspnea | 48 (19.1%) |
| Chest pain | 27 (10.7%) |
| Dry cough | 27 (10.7%) |
| Arrhythmias or palpitation | 15 (5.9%) |
| Musculoskeletal symptoms | 14 (5.6%) |
| Neurological symptoms | 14 (5.6%) |
| High or unstable blood pressure | 7 (2.8%) |
| Other (hair loss, urticaria, fever, gastro-intestinal symptoms) | 9 (3.6%) |
| Baseline | Month 3 | p-Value a | |
|---|---|---|---|
| LVEF (%) | 62 (58–66) | 64 (60–66) | 0.28 |
| LVIDd (mm) | 45 (42–49) | 44 (42–50) | 0.48 |
| LVIDs (mm) | 27 (26–32) | 28 (25–30) | 0.43 |
| Mitral e’ | 0.08 (0.07–0.11) | 0.09 (0.07–0.12) | 0.52 |
| Mitral E/e’ | 7.88 (6.14–9.25) | 7.64 (5.65–11.61) | 0.53 |
| FVC (% of expected) | 101 (92–112) | 99 (91–108) | 0.37 |
| FEV1 (% of expected) | 99 (89–108) | 96 (90–105) | 0.12 |
| Tiffeneau-index (% of expected) | 81 (78–85) | 81 (77–84) | 0.19 |
| DLCO (% of expected) | 72 (64–86) | 74 (66–86) | 0.028 |
| Baseline Value | Abnormal (%) | 3 Months | Abnormal (%) | p-Value a | |
|---|---|---|---|---|---|
| D-dimer (ug/L) | 435 (310–719) | 37.7 | 388 (274–593) | 34.8 | <0.01 |
| Ferritin (ug/L) | 113 (50–248) | 18.1 | 106 (48–218) | 10.9 | <0.01 |
| Fibrinogen (g/L) | 3.4 (2.9–3.8) | 24.2 | 3.3 (2.8–4.0) | 25.6 | 0.96 |
| hs-CRP (mg/L) | 1.7 (1–3.1) | 19.1 | 1.8 (0.8–4.4) | 17.9 | 0.27 |
| hs-Troponin-T (ng/L) | 6.1 (3.5–9.0) | 11.2 | 5.2 (3.7–7.6) | 8.4 | <0.001 |
| IL-6 (pg/mL) | 40 (10–320) | n.a. | 73 (6–376) | n.a. | 0.49 |
| IL-33 (pg/mL) | 200 (107–1064) | n.a. | 279 (99–719) | n.a. | 0.75 |
| NT-proBNP (pg/mL) | 70 (33–129) | 5.0 | 72 (34–112) | 4.4 | 0.36 |
| Severity Categories | Patients ≤ 52 Years | Patients > 52 Years |
|---|---|---|
| Treated at home | 109 (82.6%) | 67 (55.8%) |
| Hospitalized without respiratory failure | 9 (6.8%) | 4 (3.3%) |
| Hospitalized with respiratory failure | 10 (7.6%) | 40 (33.3%) |
| Intensive care admission | 4 (3.0%) | 9 (7.5%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fekete, K.; Sándor, B.; Kacsó, A.; Pálfi, A.; Tóth, S.; Deres, L.; Szabados, E.; Czopf, L.; Rábai, M.; Gál, R.; et al. Prevalence and Cardiopulmonary Characteristics of Post-COVID Syndrome at a Hungarian Tertiary Referral Hospital. J. Clin. Med. 2025, 14, 2604. https://doi.org/10.3390/jcm14082604
Fekete K, Sándor B, Kacsó A, Pálfi A, Tóth S, Deres L, Szabados E, Czopf L, Rábai M, Gál R, et al. Prevalence and Cardiopulmonary Characteristics of Post-COVID Syndrome at a Hungarian Tertiary Referral Hospital. Journal of Clinical Medicine. 2025; 14(8):2604. https://doi.org/10.3390/jcm14082604
Chicago/Turabian StyleFekete, Krisztina, Barbara Sándor, Anita Kacsó, Anita Pálfi, Szilard Tóth, László Deres, Eszter Szabados, László Czopf, Miklós Rábai, Roland Gál, and et al. 2025. "Prevalence and Cardiopulmonary Characteristics of Post-COVID Syndrome at a Hungarian Tertiary Referral Hospital" Journal of Clinical Medicine 14, no. 8: 2604. https://doi.org/10.3390/jcm14082604
APA StyleFekete, K., Sándor, B., Kacsó, A., Pálfi, A., Tóth, S., Deres, L., Szabados, E., Czopf, L., Rábai, M., Gál, R., Alexy, T., Habon, T., Tóth, K., Alizadeh, H., Soós, S., & Halmosi, R. (2025). Prevalence and Cardiopulmonary Characteristics of Post-COVID Syndrome at a Hungarian Tertiary Referral Hospital. Journal of Clinical Medicine, 14(8), 2604. https://doi.org/10.3390/jcm14082604