
Biportal Endoscopic Decompression with Maximized Facet Joint Preservation for Central to Extraforaminal Lumbar Stenosis
 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Surgical Procedure
2.2.1. Interlaminar Approach
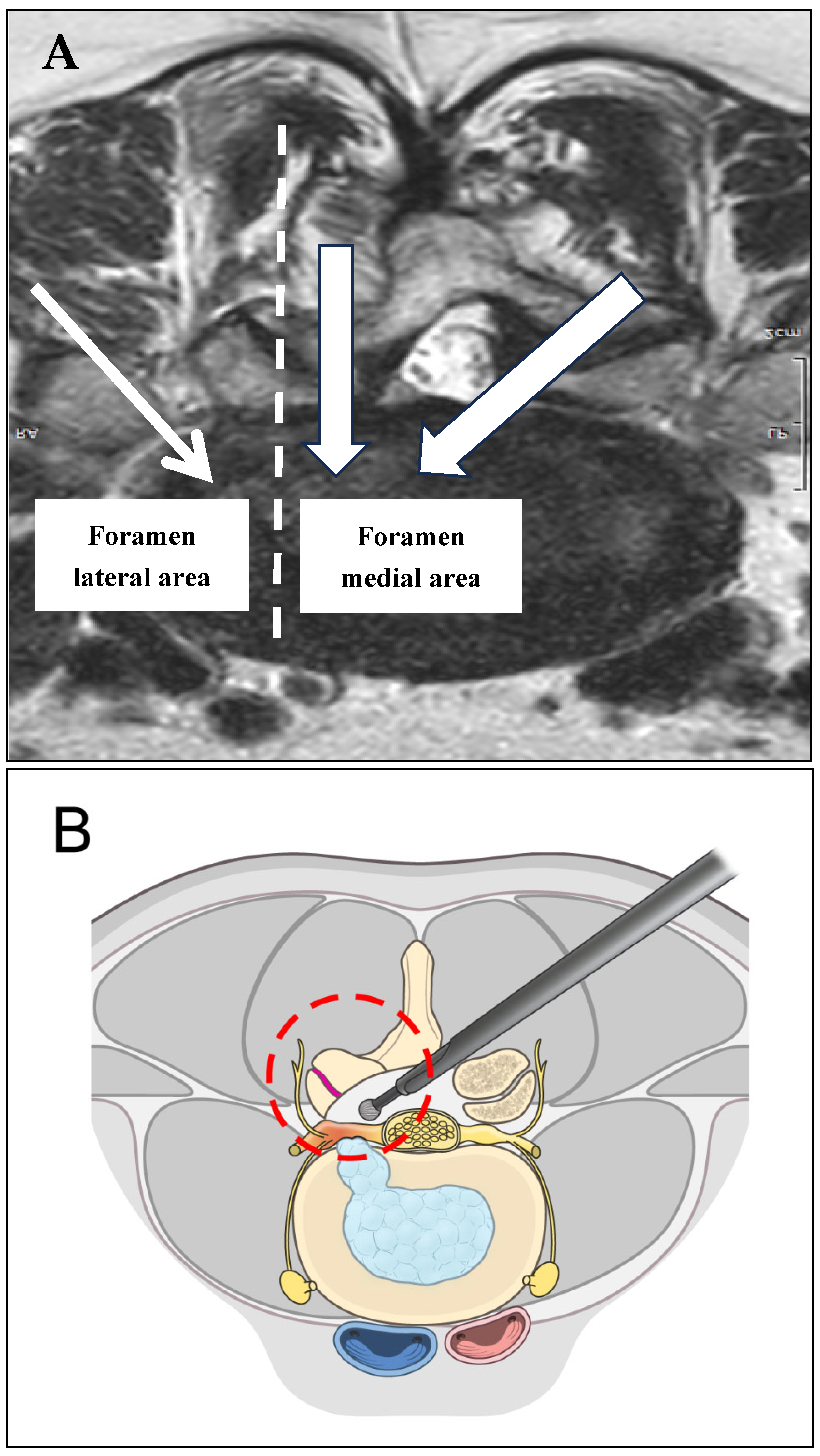
2.2.2. Extraforaminal Approach
2.3. Outcome Evaluation
2.4. Statistical Analyses
3. Results
3.1. Patient Demographics
3.2. Surgical Outcomes
3.3. Evaluation of Radiological Outcomes
3.4. Clinical Outcomes
3.5. Case Report
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kwon, J.W.; Moon, S.H.; Park, S.Y.; Park, S.J.; Park, S.R.; Suk, K.S.; Kim, H.S.; Lee, B.H. Lumbar Spinal Stenosis: Review Update 2022. Asian Spine J. 2022, 16, 789–798. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lee, W.M.; You, K.H.; Kang, M.S.; Kim, J.H.; Park, H.J. Oblique Lumbar Interbody Fusion with Selective Biportal Endoscopic Posterior Decompression for Multilevel Lumbar Degenerative Diseases. Asian Spine J. 2023, 17, 392–400. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ahn, J.S.; Lee, H.J.; Choi, D.J.; Lee, K.Y.; Hwang, S.J. Extraforaminal approach of biportal endoscopic spinal surgery: A new endoscopic technique for transforaminal decompression and discectomy. J. Neurosurg. Spine 2018, 28, 492–498. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.E.; Choi, D.J. Clinical and Radiological Outcomes of Unilateral Biportal Endoscopic Decompression by 30° Arthroscopy in Lumbar Spinal Stenosis: Minimum 2-Year Follow-up. Clin. Orthop. Surg. 2018, 10, 328–336. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kim, J.E.; Choi, D.J.; Park, E.J. Clinical and Radiological Outcomes of Foraminal Decompression Using Unilateral Biportal Endoscopic Spine Surgery for Lumbar Foraminal Stenosis. Clin. Orthop. Surg. 2018, 10, 439–447. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Junjie, L.; Jiheng, Y.; Jun, L.; Haixiong, L.; Haifeng, Y. Comparison of Unilateral Biportal Endoscopy Decompression and Microscopic Decompression Effectiveness in Lumbar Spinal Stenosis Treatment: A Systematic Review and Meta-analysis. Asian Spine J. 2023, 17, 418–430. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tian, D.; Zhu, B.; Liu, J.; Chen, L.; Sun, Y.; Zhong, H.; Jing, J. Contralateral inclinatory approach for decompression of the lateral recess and same-level foraminal lesions using unilateral biportal endoscopy: A technical report. Front. Surg. 2022, 9, 959390. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wangsawatwong, P.; de Andrada Pereira, B.; Lehrman, J.N.; Sawa, A.G.U.; O'Neill, L.K.; Turner, J.D.; Uribe, J.S.; Kelly, B.P. Biomechanical Effects of Facet Joint Violation After Single-Level Lumbar Fusion with Transpedicular Screw and Rod Instrumentation. Spine 2023, 48, 1033–1040. [Google Scholar] [CrossRef] [PubMed]
- Sharma, M.; Langrana, N.A.; Rodriguez, J. Role of ligaments and facets in lumbar spinal stability. Spine 1995, 20, 887–900. [Google Scholar] [CrossRef] [PubMed]
- Haher, T.R.; O'Brien, M.; Dryer, J.W.; Nucci, R.; Zipnick, R.; Leone, D.J. The role of the lumbar facet joints in spinal stability. Identification of alternative paths of loading. Spine 1994, 19, 2667–2670; discussion 2671. [Google Scholar] [CrossRef] [PubMed]
- Yeung, Y.K.; Park, C.W.; Jun, S.G.; Park, J.H.; Tse, A.C. Comparative Cohort Study for Expansion of Lateral Recess and Facet Joint Injury after Biportal Endoscopic Ipsilateral Decompression and Contralateral Decompression. Asian Spine J. 2022, 16, 560–566. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kim, J.E.; Choi, D.J.; Park, E.J.J.; Lee, H.J.; Hwang, J.H.; Kim, M.C.; Oh, J.S. Biportal Endoscopic Spinal Surgery for Lumbar Spinal Stenosis. Asian Spine J. 2019, 13, 334–342. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Song, K.S.; Lee, C.W.; Moon, J.G. Biportal endoscopic spinal surgery for bilateral lumbar foraminal decompression by switching surgeon’s position and primary 2 portals: A report of 2 cases with technical note. Neurospine 2019, 16, 138–147. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Kim, H.S.; Oh, S.W.; Adsul, N.M.; Singh, R.; Kashlan, O.N.; Noh, J.H.; Jang, I.T.; Oh, S.H. Evolution of Spinal Endoscopic Surgery. Neurospine 2019, 16, 6–14. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kim, H.S.; Patel, R.; Paudel, B.; Jang, J.S.; Jang, I.T.; Oh, S.H.; Park, J.E.; Lee, S. Early Outcomes of Endoscopic Contralateral Foraminal and Lateral Recess Decompression via an Interlaminar Approach in Patients with Unilateral Radiculopathy from Unilateral Foraminal Stenosis. World Neurosurg. 2017, 108, 763–773. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Heo, D.H. Contralateral sublaminar approach for decompression of the combined lateral recess, foraminal, and extraforaminal lesions using biportal endoscopy: A technical report. Acta Neurochir. 2021, 163, 2783–2787. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Kang, H.S.; Choi, G.; Kong, B.J.; Ahn, Y.; Kim, J.S.; Lee, H.Y. Foraminoplastic ventral epidural approach for removal of extruded herniated fragment at the L5-S1 level. Neurol. Med. Chir. 2010, 50, 1074–1078. [Google Scholar] [CrossRef] [PubMed]
- Eun, D.C.; Lee, Y.H.; Park, J.O.; Suk, K.S.; Kim, H.S.; Moon, S.H.; Park, S.Y.; Lee, B.H.; Park, S.J.; Kwon, J.W.; et al. A Comparative Analysis of Bi-Portal Endoscopic Spine Surgery and Unilateral Laminotomy for Bilateral Decompression in Multilevel Lumbar Stenosis Patients. J. Clin. Med. 2023, 12, 1033. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Yang, H.S.; Lee, N.; Park, J.Y. Current status of biportal endoscopic decompression for lumbar foraminal stenosis: Endoscopic partial facetectomy and outcome factors. J. Minim Invasive Spine Surg. Tech. 2021, 6 (Suppl. S1), S157–S163. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean ± SD | |
|---|---|
| Age | 71.40 ± 6.90 |
| Sex | |
| F | 34 (73.91%) |
| M | 12 (26.06%) |
| Surgical level | |
| L3-4 | 6 (13.04%) |
| L4-5 | 18 (39.13%) |
| L5-S1 | 22 (47.83%) |
| Operation time (min) | 98.04 ± 10.08 |
| Estimated blood loss (mL) | 64.13 ± 10.47 |
| HOD (day) | 2.78 ± 0.64 |
| Follow-up period (month) | 16.35 ± 2.58 |
| Pre-op | Post-op | Expansion Ratio (%) | p-Value | |
|---|---|---|---|---|
| Mean ± SD | Mean ± SD | |||
| CSA-SC (mm2) | 1.27 ± 0.23 | 2.27 ± 0.27 | 178.74% | <0.0001 |
| CSA-IVF (mm2) | 0.46 ± 0.13 | 1.13 ± 0.16 | 245.65% | <0.0001 |
| Pre-op | Post-op | Maintenance Ratio (%) | |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| CSA-FJ (mm2) | 2.37 ± 0.44 | 2.07 ± 0.46 | 87.34% |
| Facet joint length (mm) | 13.57 ± 1.34 | 12.22 ± 1.48 | 90.05% |
| SAP length (mm) | 11.74 ± 1.14 | 8.87 ± 1.25 | 75.55% |
| Disc height (mm) | 8.39 ± 1.24 | 8.29 ± 1.24 | 98.81% |
| Segmental lordosis (°) | 11.52 ± 3.76 | 11.34 ± 3.70 | 98.44% |
| Pre-op | 1 Month | 3 Months | 6 Months | 12 Months | Overall p-Value | |
|---|---|---|---|---|---|---|
| Back VAS Estimated mean (SE) | 4.74 (0.24) | 2.44 (0.20) | 2.04 (0.17) | 1.39 (0.14) | 1.17 (0.15) | <0.0001 |
| Leg VAS Estimated mean (SE) | 7.52 (0.18) | 3.44 (0.16) | 2.78 (0.19) | 2.17 (0.15) | 1.96 (0.15) | <0.0001 |
| Pregabalin (mg) Estimated mean (SE) | 247.83 (15.23) | 102.17 (7.36) | 63.04 (8.30) | 33.70 (5.80) | 18.48 (4.22) | <0.0001 |
| Grade | Pre-op | 1 Month | 3 Months | 6 Months | 12 Months | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Poor | 12 | 52.2% | - | 0% | - | 0% | - | 0% | - | 0% |
| Fair | 11 | 47.8% | 9 | 39.1% | 4 | 17.4% | 2 | 8.7% | - | 0% |
| Good | - | 0% | 14 | 60.9% | 16 | 69.6% | 16 | 69.6% | 9 | 39.1% |
| Excellent | - | 0% | - | 0% | 3 | 13.0% | 5 | 21.7% | 14 | 60.9% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S.-R.; Choi, S.-R.; Kim, N.-H.; Kim, H.-S.; Kwon, J.-W.; Suk, K.-S.; Moon, S.-H.; Park, S.-Y.; Shin, J.-W.; Lee, B.-H.; et al. Biportal Endoscopic Decompression with Maximized Facet Joint Preservation for Central to Extraforaminal Lumbar Stenosis. J. Clin. Med. 2025, 14, 2725. https://doi.org/10.3390/jcm14082725
Park S-R, Choi S-R, Kim N-H, Kim H-S, Kwon J-W, Suk K-S, Moon S-H, Park S-Y, Shin J-W, Lee B-H, et al. Biportal Endoscopic Decompression with Maximized Facet Joint Preservation for Central to Extraforaminal Lumbar Stenosis. Journal of Clinical Medicine. 2025; 14(8):2725. https://doi.org/10.3390/jcm14082725
Chicago/Turabian StylePark, Sub-Ri, Sung-Ryul Choi, Nam-Hoo Kim, Hak-Sun Kim, Ji-Won Kwon, Kyung-Soo Suk, Seong-Hwan Moon, Si-Young Park, Jae-Won Shin, Byung-Ho Lee, and et al. 2025. "Biportal Endoscopic Decompression with Maximized Facet Joint Preservation for Central to Extraforaminal Lumbar Stenosis" Journal of Clinical Medicine 14, no. 8: 2725. https://doi.org/10.3390/jcm14082725
APA StylePark, S.-R., Choi, S.-R., Kim, N.-H., Kim, H.-S., Kwon, J.-W., Suk, K.-S., Moon, S.-H., Park, S.-Y., Shin, J.-W., Lee, B.-H., & Park, J.-O. (2025). Biportal Endoscopic Decompression with Maximized Facet Joint Preservation for Central to Extraforaminal Lumbar Stenosis. Journal of Clinical Medicine, 14(8), 2725. https://doi.org/10.3390/jcm14082725