Abstract
Background/Objectives: Chronic plantar fasciopathy is a degenerative pathology that elicits persistent heel pain, significantly impacting quality of life. When conservative treatments fail to yield satisfactory outcomes, radiofrequency microtenotomy utilizing the Topaz technique presents a minimally invasive alternative with regenerative potential. This study aims to evaluate its efficacy in pain reduction, functional improvement, and complication rate compared to other treatments. Methods: A systematic review was conducted in accordance with the PRISMA guidelines and registered in PROSPERO (CRD4202525648314). PubMed, EBSCOhost, Web of Science, and Scopus (2014–2024) were comprehensively searched to identify studies on the Topaz technique for refractory chronic plantar fasciopathy. Clinical trials, cohort studies, and case series were included, and a meta-analysis was performed using a random-effects model to assess pain, the Visual Analog Scale (VAS), American Orthopaedic Foot & Ankle Society function(AOFAS), and complications. Results: Fifteen studies encompassing 1576 patients were analyzed. The meta-analysis demonstrated a significant reduction in pain of 5.90 points on the VAS scale (95% CI: 5.03 to 6.77, p < 0.001) and a functional improvement of 0.28 points on the AOFAS scale (95% CI: 0.27 to 0.28, p < 0.001). The complication rate was low (3.00%), with high patient satisfaction (90%) and rapid recovery. Conclusions: The findings suggest that the Topaz technique is a safe and effective option for chronic plantar fasciopathy, demonstrating significant improvements and minimal complications.
1. Introduction
Chronic plantar fasciopathy is a degenerative pathology that affects the plantar fascia, a fibrous structure fundamental to foot biomechanics. It is one of the primary causes of heel pain and affects between 3.6% and 7% of the general population, with a high incidence in athletes and individuals who stand for prolonged periods [1,2,3]. Traditionally, it has been considered an inflammatory process known as “plantar fasciitis”. However, recent studies have indicated that its etiology is predominantly degenerative, characterized by fibrosis, thickening, and alterations in the collagen matrix [2].
Plantar fasciitis is one of the most prevalent soft tissue conditions of the foot in adults, particularly among individuals aged 40 to 60 years [4], a population in which a higher incidence has been reported [5]. This condition, associated with factors such as increased body mass index, reduced ankle dorsiflexion, and prolonged weight bearing, rarely affects children [5,6,7]. While it may appear in younger individuals due to repetitive strain, evidence indicates a predominantly adult distribution [4]. Consequently, this review focuses exclusively on adult patients, and studies including pediatric populations were excluded to maintain clinical relevance.
Risk factors include intrinsic causes, such as obesity, pes cavus or pes planus, limited ankle dorsiflexion, and aging, as well as extrinsic factors, such as the use of inappropriate footwear and repetitive impact during athletic activities [1,2,3]. Clinically, the pain is localized to the medial calcaneal tuberosity and is most severe during the initial steps of the day or after extended periods of rest. Diagnosis is based on physical examination and imaging studies. Musculoskeletal ultrasonography can identify fascial thickening and assess its structure, and is a crucial tool for differentiating fasciopathy from other conditions, such as calcaneal fractures or nerve entrapment [8].
Initial treatment is conservative and may include plantar orthoses, physiotherapy, cryotherapy, non-steroidal anti-inflammatory drugs, neuromuscular taping, and physical therapies, such as extracorporeal shock wave therapy [9]. Corticosteroid infiltration, platelet-rich plasma, and hyaluronic acid are also used, depending on the degree of fascial degeneration [10,11,12]. However, approximately 10% of patients do not experience improvement with these interventions and require surgical procedures [13].
Traditional surgical approaches include partial plantar fasciotomy, which aims to reduce fascial tension through partial sectioning. However, this technique can result in complications, such as medial plantar nerve injury, alterations in foot biomechanics, and collapse of the longitudinal arch [13]. As an alternative, the Topaz technique has been developed, a minimally invasive procedure that involves the application of radiofrequency through percutaneous micro-tenotomies, with the objective of stimulating angiogenesis and promoting tissue regeneration [13,14]. Previous studies suggest that the Topaz technique allows for a 70% reduction in pain, a 60% functional improvement, and has low complication rates (<5%) compared with other surgical approaches [15]. Furthermore, its primary advantage lies in its rapid recovery, with a return to daily activities in 2–4 weeks [16,17,18]. Given its safety and efficacy, the Topaz technique is postulated as a viable therapeutic option for patients with chronic plantar fasciopathy refractory to conservative treatments. However, its long-term impact, as well as its combination with other techniques such as gastrocnemius lengthening or Baxter’s nerve decompression, requires further investigation [13].
The effects and characteristics of surgical interventions should be analyzed to develop comprehensive guidelines for these techniques. It is imperative to ensure that the application of this technique adheres to the most effective and safe recommendations tailored to the needs of patients diagnosed with plantar fasciopathy. The primary objective of the present study is to evaluate the efficacy of Topaz coblation radiofrequency in chronic plantar fasciopathy, analyzing its benefits in terms of pain reduction and post-surgical functionality. Furthermore, its effectiveness will be compared with other surgical and non-surgical treatments in order to establish its role in the comprehensive management of this pathology and facilitate the development of more comprehensive and precise specific guidelines [12,13,14].
2. Materials and Methods
2.1. Registry of Systematic Review Protocol
This systematic review was conducted in accordance with the criteria established by the PRISMA Declaration [19]. The PRISMA checklist is detailed in Supplementary File S1, ensuring adherence to the methodological quality standards. The protocol was pre-registered with PROSPERO (identification number CRD42025648314). A systematic computerized literature search was performed using PubMed, EBSCOhost, Web of Science, and Scopus. The search timeframe encompassed the period from 2014 to 2024 (from the inception of indexing until 5 February 2025), utilizing terms related to “plantar fasciopathy”, “radiofrequency”, “coblation”, and “Topaz”, as well as their English equivalents. To enhance the precision of the search, the SR-Accelerator frequency analysis tool was employed, selecting relevant studies published in English, Spanish, and French while excluding literature reviews and individual case studies. To identify pertinent publications that may have been overlooked by the computerized search, the bibliographies of all the selected articles were meticulously examined.
2.2. Eligibility Criteria
2.2.1. Inclusion Criteria
The inclusion criteria were as follows: (a) studies involving patients diagnosed with chronic plantar fasciopathy refractory to conservative treatment for a minimum of six months; (b) studies evaluating the efficacy of radiofrequency coblation utilizing the Topaz technique, either as a sole intervention or in combination with other techniques; (c) studies reporting outcomes such as pain reduction using the Visual analog scale (VAS), American Orthopaedic Foot & Ankle Society (AOFAS) score, postoperative recovery time, and complication rates; (d) randomized clinical trials, cohort studies, case-control studies, or case series with a representative sample size; (e) studies published in peer-reviewed scientific journals between 2014 and 2024; and (f) articles written in English, Spanish, or French.
2.2.2. Exclusion Criteria
The exclusion criteria were as follows: (a) studies conducted in animal models; (b) studies focusing on conditions other than chronic plantar fasciopathy or in pediatric populations; (c) studies that did not explicitly specify the use of the Topaz technique or employed alternative radiofrequency methods; (d) studies that did not include pre- and post-treatment clinical evaluations; (e) narrative reviews, single case reports, expert opinions, or conference abstracts lacking complete data; (f) studies without sufficient quantitative data for extraction and analysis; and (g) articles published in languages other than English, Spanish, or French without an available translation.
2.3. Search Strategy
The primary investigation focused on studies evaluating the efficacy of the radiofrequency Topaz technique in the treatment of chronic plantar fasciopathy, with particular emphasis on its impact on pain reduction, functional improvement, and post-surgical recovery time. Literature searches were conducted in PubMed, EBSCOhost, Web of Science, and Scopus, and articles published within the last decade (2014–2024) were selected. The PICO strategy was employed for the construction of search criteria in the electronic databases, incorporating terms related to coblation radiofrequency intervention in patients with chronic plantar fasciopathy. The search string utilized in MEDLINE/PubMed was: (“fasciitis, plantar”[MeSH Terms] OR “plantar fasciopathy”[Title/Abstract] OR “plantar fasciosis”[Title/Abstract]) AND (“Radiofrequency Therapy”[MeSH Terms] OR “radiofrequency”[Title/Abstract] OR “microtenotomy”[Title/Abstract] OR “Topaz”[Title/Abstract] OR “coblation”[Title/Abstract]). Analogous search strategies were applied in EBSCOhost, Web of Science, and Scopus, with terms and Boolean operators adapted for each database. Search strings for other databases were adapted using the Polyglot Search Translator Tool. These search strings are presented in Appendix A.
2.4. Data Extraction and Summary
The eligibility criteria were independently applied by two reviewers (SD-M and NF-E) to the full texts of articles that passed the initial screening of titles and abstracts. A third researcher (JVM) conducted a secondary review of the studies included in the systematic search and refined the eligibility criteria to narrow the scope of the review. Discrepancies in article selection were resolved through discussion among the reviewers, and in cases of persistent disagreement, a third reviewer (JFT) was consulted for the final decision. To eliminate duplicate references, the online tool SR-Accelerator Deduplicator (https://www.sr-accelerator.com/#/deduplicator accessed on 10 February 2025) was initially employed. Subsequently, a manual removal of duplicates was performed using the Mendeley reference manager.
2.5. Study Coding and Summary
Data extraction was conducted independently by two reviewers for the selected studies. The following data were extracted and coded: (i) study identification, (ii) study design, (iii) sample size, (iv) mean age (range), (v) follow-up, and (vi) intervention. Additionally, outcomes were recorded in terms of (i) pain reduction, (ii) improvement in foot function, and (iii) post-surgical recovery time. Further specific data, such as complication rates, level of evidence of the study, and grade of clinical recommendation, were also collected. All extracted information was organized in an Excel spreadsheet (Table 1), facilitating statistical and comparative analyses to evaluate the efficacy of the procedure for the treatment of recalcitrant plantar fasciopathy. In instances where data were inadequately reported, the authors were contacted via email. If the requested information was not provided by the authors and was not available in tables or text, data were extracted from figures using WebPlot Digitizer (Web Plot Digitizer, V.4.1. Texas, USA) when feasible.

Table 1.
Description of studies: population, interventions, and outcomes.
2.6. Methodological Quality and Risk of Bias
The methodological quality and risk of bias were independently assessed by two investigators (JVM, NFE) using the Oxford Evidence Table developed by the Oxford Centre for Evidence-Based Medicine (OCEBM). This table categorizes the levels of evidence and degrees of recommendation for medical studies, ranging from randomized clinical trials to expert opinions. Aspects such as internal validity and potential biases, including confounding, selection, and reporting biases were evaluated. For the assessment of risk of bias, the Joanna Briggs Institute (JBI) tools were employed for cohort studies, Risk Of Bias In Non-randomized Studies—of Interventions (ROBINS-I) for non-randomized studies, and Risk Of Bias In Randomized Trials (ROB-2) for randomized clinical trials. Subsequently, the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) classification was applied to evaluate the reliability and applicability of the findings of each study.
2.7. Statistical Analysis
To evaluate the efficacy of radiofrequency microtenotomy in chronic plantar fasciopathy, considering pain reduction, functional improvement (AOFAS), patient satisfaction, and complication rates—a meta-analysis was conducted using a random-effects model in JASP software (v.0.19.3, Amsterdam, The Netherlands). The Mean Difference (MD) and corresponding 95% confidence intervals (95% CI) were calculated for each outcome. Given the clinical and methodological heterogeneity among the studies, this model was deemed appropriate. Statistical significance was determined using p-values, with results considered significant at p < 0.05.
Heterogeneity among studies was assessed using the Q statistic and the I2 statistic. A meta-regression analysis was subsequently conducted to explore the potential sources of this heterogeneity. Additionally, prediction intervals (95% PI) were calculated to estimate the expected range of true effects in similar future studies, providing a more nuanced understanding of effect variability across contexts.
3. Results
3.1. Search Results
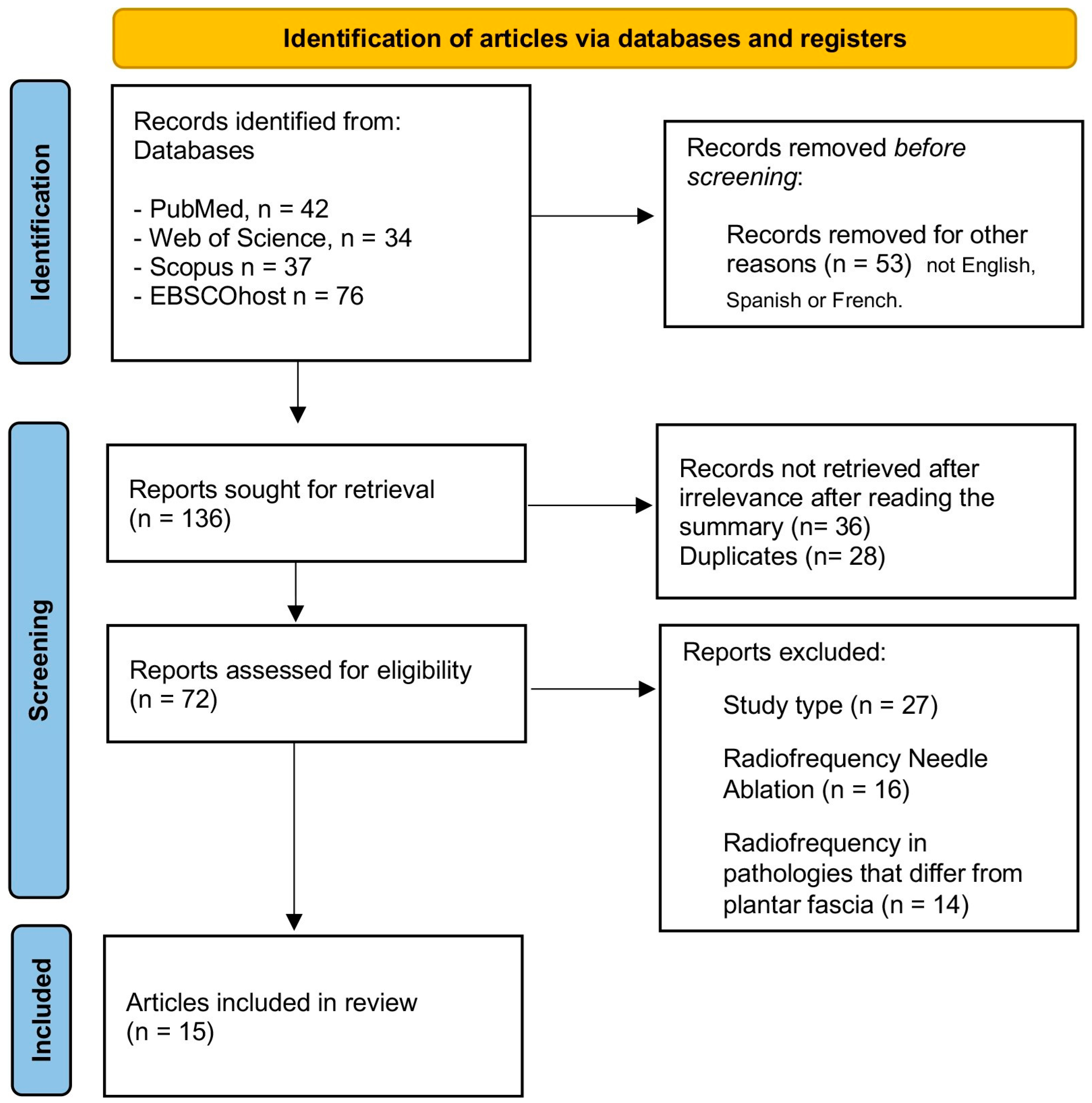
Figure 1 presents a flow diagram detailing the various stages of the literature search and the selection of studies included in this review. The initial search of the electronic databases yielded 189 articles. Prior to the selection process, 53 articles were eliminated due to filters applied for review articles and those not written in English, Spanish, or French. Subsequently, duplicate studies were removed, with 28 articles eliminated automatically and 36 eliminated manually. Subsequently, 27 additional articles were excluded after reviewing the title and abstract. Furthermore, 30 articles were discarded after a full-text evaluation. Ultimately, a total of 15 articles were included in the review.
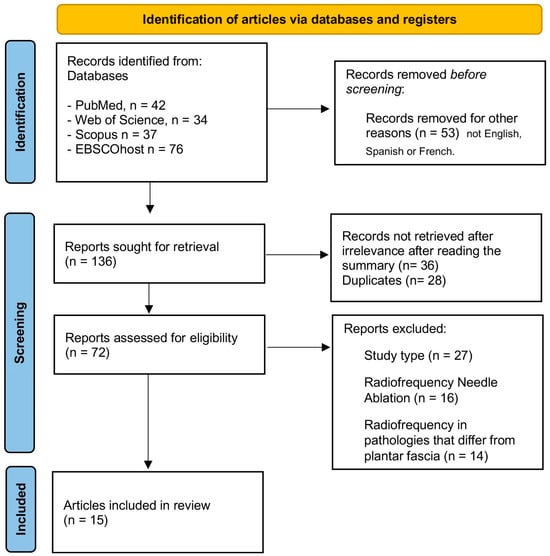
Figure 1.
PRISMA flowchart of the article selection process.
3.2. Participants and Interventions Characteristics
The total number of patients reported was 1576, with a total of 1696 feet, assuming 1 ft per patient when not specified as bilateral. The individual sample sizes ranged from 4 to 460 patients per study. The age of the participants ranged widely from 19 to 77 years, with an overall mean of 45 to 55 years, indicating a predominance of middle-aged individuals. Female sex predominated in most studies, accounting for 60% to 77% of the samples, although in smaller studies, such as the Topaz technique, this trend varied. The average body mass index (BMI) ranged from 27 to 31 kg/m2, suggesting a general overweight profile among participants, with some specific studies presenting a higher average BMI, such as the Eke et al. study, which reported an average of 31.3 kg/m2.
The duration of symptoms prior to treatment exhibited high variability, ranging from 4 months to 11 years, being longer in patients with recalcitrant plantar fasciitis, where the mean duration was 12 to 24 months, reaching up to 178 months (14.8 years) in extreme cases. The laterality of the condition demonstrated an even distribution, with approximately 50% of the cases affecting the right foot and the other 50% affecting the left foot, while bilateral cases represented between 10% and 25% of the samples.
The most common inclusion criteria among the studies encompassed the presence of chronic plantar fasciitis for more than 6 to 9 months, failure of previous conservative treatments, manifestation of characteristic first-step pain after rest, and plantar fascia thickness greater than 4 mm, as measured by ultrasound in some cases. The most frequent exclusion criteria were the presence of systemic diseases, diabetes, previous surgeries, re-occurring treatments such as physiotherapy or cortisone injections, and an extremely high BMI (greater than 35 kg/m2).
3.3. Risk of Bias
A quality and risk of bias assessment was conducted on the included studies, utilizing the methodologically most appropriate scale according to their design. Case series studies (Colberg et al., 2022 [17]; Colberg et al., 2019 [18]; Bagali et al., 2016 [20]; Shah et al., 2016 [14]) were evaluated using the JBI Critical Appraisal tool (See Table 2), which analyzes criteria such as participant inclusion, follow-up, and result reliability. Observational cohort and retrospective studies (Koh et al., 2022 [30]; Yuan et al., 2020 [29]; Eke et al., 2021 [22]; Erden et al., 2020 [23]; Chou et al., 2016 [21]; Lucas et al., 2015 [24]; Ozan et al., 2016 [26]; Wang et al., 2017 [27]; Huang et al., 2018 [16]) were assessed using ROBINS-I (See Table 3), which enables the determination of bias risk in non-randomized studies, considering factors such as confounding, participant selection, and outcome reporting. Randomized clinical trials(Wu et al., 2017 [28]; Møller et al., 2022 [25]) were evaluated using ROB-2, an instrument that analyzes randomization, blinding, and data integrity (See Table 4).
Table 2.
Results for the Joanna Briggs Institute (JBI) critical appraisal tool for case series studies.
Table 3.
Risk of bias in non-randomized studies–of interventions.
Table 4.
ROB-2 (Risk of bias in randomized trials).
3.4. GRADE Quality Assessment
Assessment of study quality according to the GRADE scale [28] demonstrates that there are two randomized controlled trials (RCTs) (Wu et al., 2017 [28] and Møller et al., 2022 [25]) classified as high quality, owing to their low risk of bias, consistency in results, and high precision (see Table 5). Four cohort studies (Koh et al., 2022 [30]; Erden et al., 2020 [23]; Chou et al., 2016 [21]; Ozan et al., 2016 [26]) are classified as moderate quality, exhibiting some risk of bias and certain methodological limitations. Four case series(Colberg et al., 2022 [17]; Colberg et al., 2019 [18]; Bagali et al., 2016 [20]) were of moderate quality due to limitations in variable control and comparability. Lastly, five retrospective studies (Yuan et al., 2020 [29]; Eke et al., 2021 [22]; Lucas et al., 2015 [24]; Wang et al., 2017 [27]; Huang et al., 2018 [16]) are classified as low quality due to their high risk of bias, inconsistency in findings, and potential publication bias. These results indicate that while the overall evidence is favorable, the reliability of the findings varies depending on the study design.
Table 5.
GRADE quality assessment.
3.5. Meta-Analysis Results
The analysis of the 15 studies included in this systematic review evaluated the efficacy of various interventions in the treatment of recalcitrant plantar fasciitis. Two primary variables were analyzed: pain reduction measured using the visual analog scale (VAS) and functional improvement measured with the AOFAS (American Orthopaedic Foot & Ankle Society) scale, in conjunction with additional scales and sub-analyses.
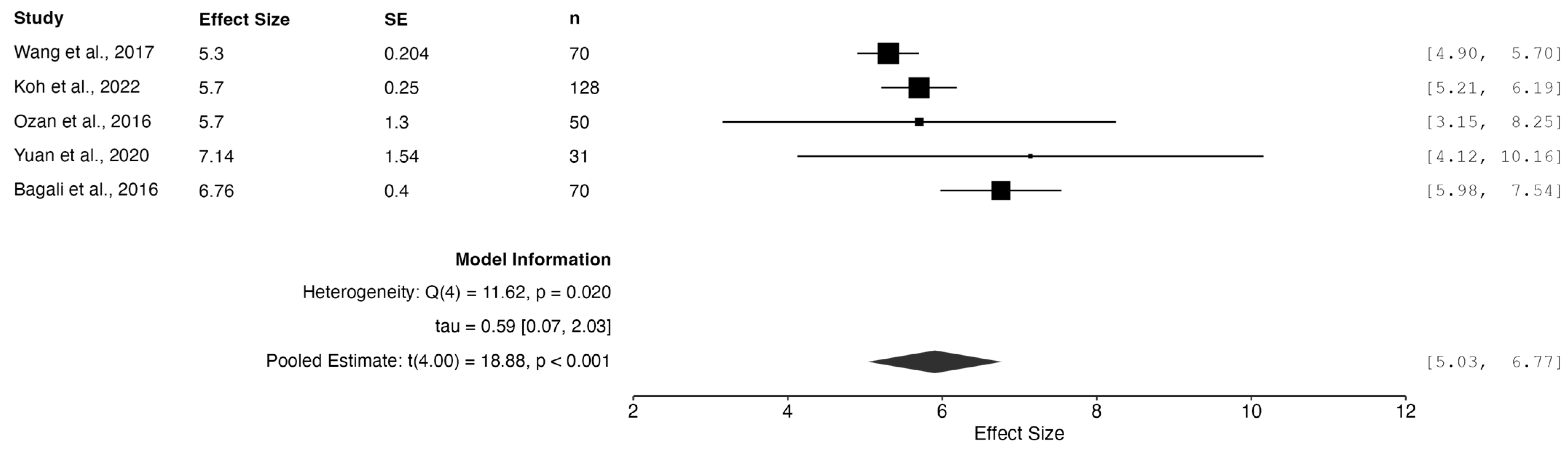
3.5.1. Pain Reduction
The visual analog scale (VAS) is a widely used instrument for quantifying patient-perceived pain, offering a subjective yet standardized method for assessing symptom intensity. Its consistent application across the studies included in this meta-analysis underscores its clinical utility and widespread acceptance as a valid indicator of treatment progress.
A random-effects meta-analysis revealed a combined effect size of 5.90 (95% CI: 5.03 to 6.77, p < 0.001), indicating a statistically and clinically significant reduction in reported pain following the intervention. This outcome highlights the substantial therapeutic impact on pain perception and, consequently, on patients’ health-related quality of life.
Nonetheless, statistically significant heterogeneity was observed (Qe = 11.62, df = 4, p = 0.02), with an I2 of 71.57%, reflecting considerable variability across studies that could not be attributed to chance alone. Such heterogeneity may stem from differences in intervention characteristics, patient populations or pain measurement techniques.
The 95% prediction interval (4.05 to 7.76) indicates that while the overall efficacy of the interventions is robust, the magnitude of benefit may vary depending on the clinical setting, intervention type, or baseline pain severity. This finding emphasizes the value of personalized treatment strategies in clinical practice. (See Figure 2)
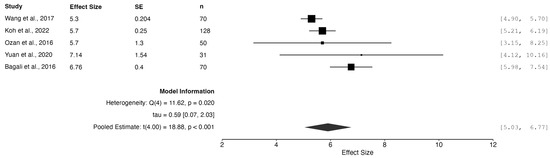
Figure 2.
Meta-analysis of pain reduction measured by VAS. Studies included: Wang et al., 2017 [27]; Koh et al., 2022 [30]; Ozan et al., 2016 [26]; Yuan et al., 2020 [29]; Bagali et al., 2016 [20].
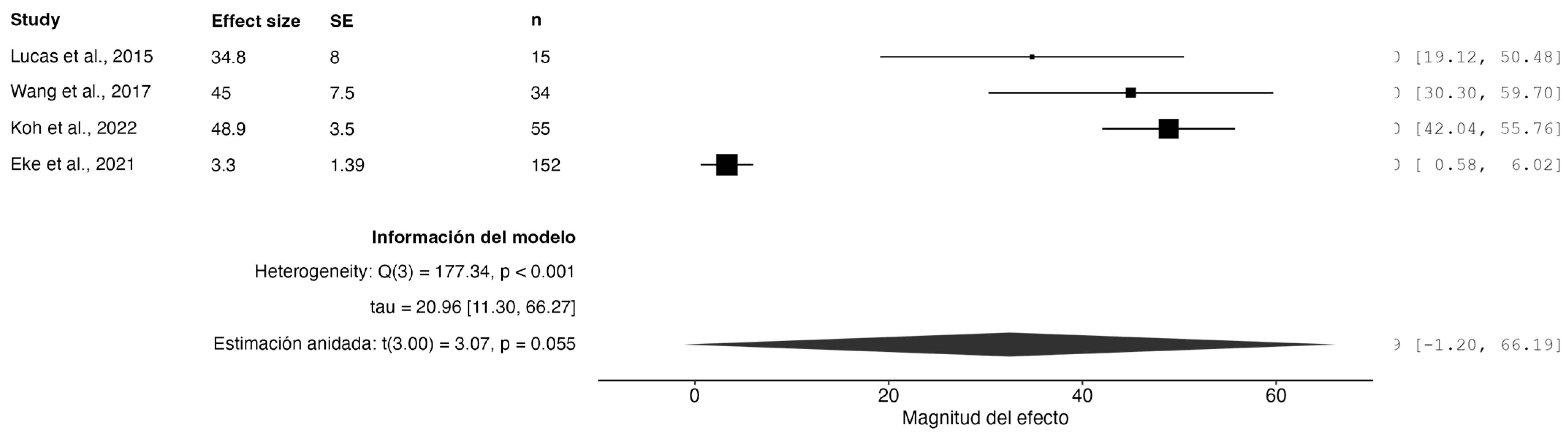
3.5.2. Functional Improvement Assessed with the AOFAS Scale
A random-effects model meta-analysis demonstrated statistically significant functional improvement among patients with plantar fasciitis, as assessed by the AOFAS (American Orthopaedic Foot & Ankle Society) scale. The pooled effect showed a mean functional gain of 32.78 points (95% CI: 14.86 to 50.69, p = 0.0053), highlighting the clinical relevance of the evaluated interventions for functional recovery.
Although the confidence interval is relatively wide, it still suggests a meaningful positive effect. The 95% prediction interval ranged from –13.97 to 79.52, indicating considerable variability in treatment efficacy across similar future studies.
Importantly, the analysis identified substantial heterogeneity (Q = 191.30, df = 5, p < 0.001; I2 = 93.22%), indicating a high inconsistency among the included trials. This heterogeneity may reflect variations in the study populations, intervention protocols, outcome assessment methods, or follow-up durations.
Despite the heterogeneity, the overall effect remains statistically significant, supporting the general effectiveness of the evaluated treatments in improving foot function. (See Figure 3)
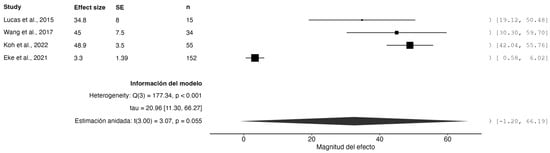
Figure 3.
Forest plot of functional improvement measured using the AOFAS scale. Studies included: Lucas et al., 2015 [24]; Wang et al., 2017 [27]; Koh et al., 2022 [30]; Eke et al., 2021 [22].
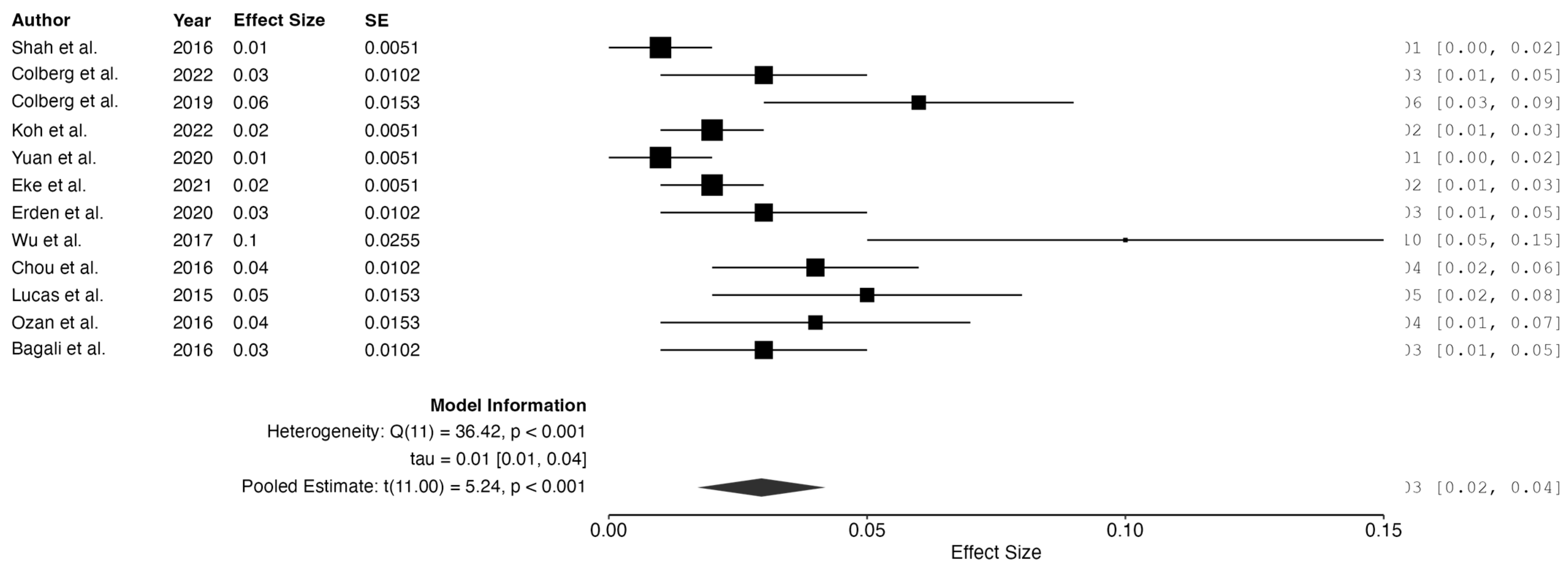
3.5.3. Complication Rate
Evaluating the complications associated with clinical interventions is essential for understanding the safety profile of medical treatments. This meta-analysis provides a quantitative synthesis of complication rates and offer an integrated overview of potential clinical risks.
Using a random-effects model, the pooled effect size was 0.03 (95% CI: 0.02 to 0.04, p < 0.001), indicating a very low overall incidence of complications and supporting the general safety of the interventions under review.
However, significant residual heterogeneity was detected (Qe = 36.42, df = 11, p < 0.001; I2 = 75.36%), suggesting substantial variability in the complication rates. Possible contributors include procedural differences, patient characteristics, and inconsistent definitions of “complication” across the studies.
The 95% prediction interval (−0.0033 to 0.06) further reflects variability in clinical outcomes. While the negative lower bound is a statistical artifact with no clinical meaning, as complication rates cannot be negative, it illustrates uncertainty in future effect estimates.
The interventions appear to be generally safe, though these findings underline the need for standardized definitions and improved reporting of adverse events in future research. (See Figure 4).
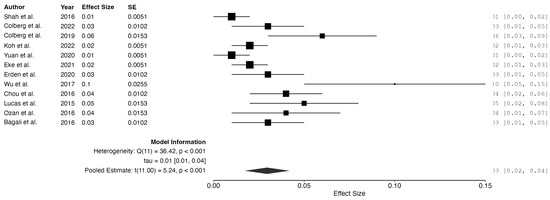
Figure 4.
Meta-analysis: complication rates. Studies included: Shah et al., 2016 [14]; Colberg et al., 2022 [17]; Colberg et al., 2019 [18]; Koh et al., 2022 [30]; Yuan et al., 2020 [29]; Eke et al., 2021 [22]; Erden et al., 2020 [23]; Wu et al., 2017 [28]; Chou et al., 2016 [21]; Lucas et al., 2015 [24]; Ozan et al., 2016 [26]; Bagali et al., 2016 [20].
3.5.4. Follow-Up Time
Random-effects analysis revealed disparities in pain reduction relative to the follow-up duration. For studies with a short follow-up period (<6 months), pain reduction was −3.42 points on the VAS scale (95% CI: −4.06 to −2.78, p < 0.001), exhibiting high heterogeneity (I2 = 97.80%). Conversely, studies with long follow-up (≥12 months) demonstrated a pain reduction of −4.27 points (95% CI: −4.58 to −3.95, p < 0.001), also exhibiting high heterogeneity (I2 = 96.50%). These findings indicate that pain reduction was statistically significant in both groups.
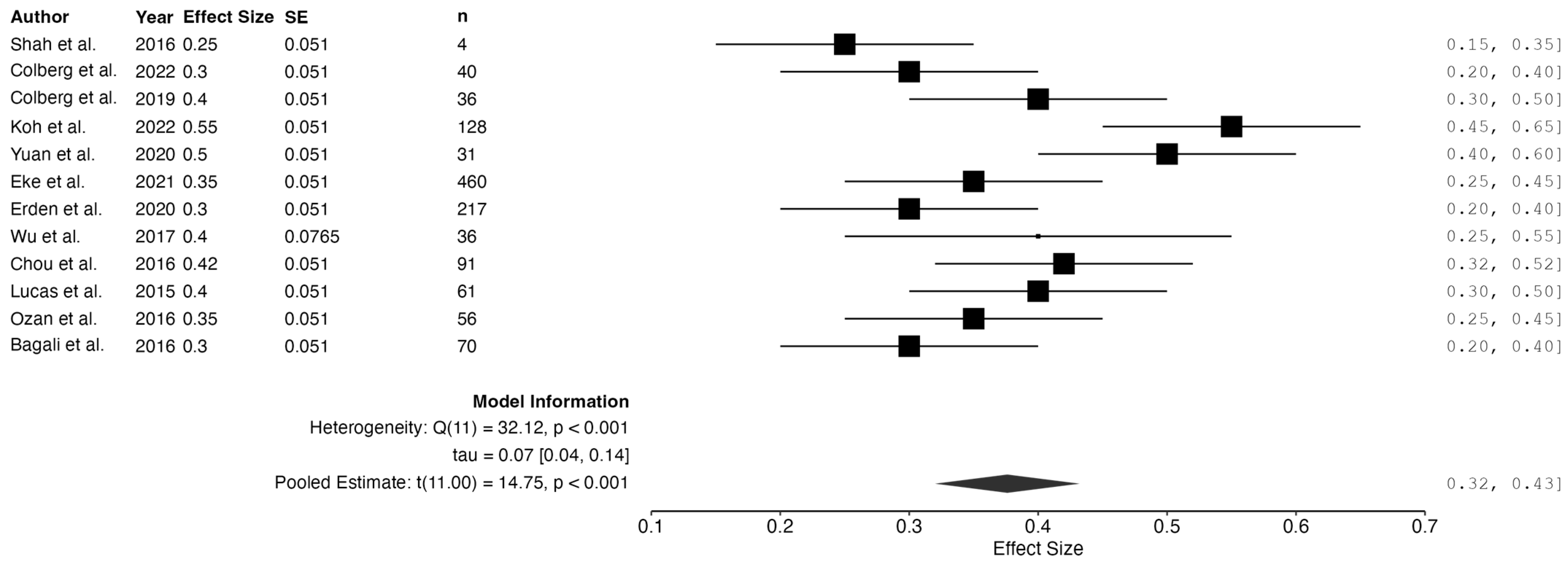
3.5.5. Analysis of the Variable “Use of Adjuvant Therapies”
The studies included in the meta-analysis evaluated various adjuvant therapies for recovery and symptom reduction in patients with plantar fasciitis. Physiotherapy was the most frequently utilized, focusing on biomechanical exercises to enhance foot functionality (Shah et al., 2016 [14]; Wang et al., 2017 [27]). Platelet-rich plasma (PRP) has been administered as a regenerative therapy with favorable outcomes in recalcitrant cases (Colberg et al., 2022 [17]; Lucas et al., 2015 [24]). Extracorporeal Shock Wave Therapy (ESWT) has demonstrated efficacy in pain reduction (Koh et al., 2022 [30]; Yuan et al., 2020 [29]). The utilization of orthoses and specialized footwear contributes to improved load distribution and reduced recurrence (Møller et al., 2022 [25]). Lastly, corticosteroid infiltrations, although less prevalent, provided temporary pain relief, albeit with an increased risk of recurrence (Wu et al., 2017 [28]; Chou et al., 2016 [21]).
A random-effects meta-analysis revealed a pooled effect size of 0.38 (95% CI: 0.32 to 0.43, p < 0.001), suggesting a moderate and statistically significant overall effect of therapeutic interventions. This supports their efficacy, particularly when embedded in comprehensive and individualized care plans.
Nevertheless, a high level of heterogeneity was noted (Qe = 32.12, df = 11, p < 0.001; τ2 = 5.19 × 10−3, τ = 0.07, I2 = high), likely attributable to variations in therapy types, intensities, patient profiles, follow-up periods, and outcome definitions.
The 95% prediction interval (0.21 to 0.54) indicates the potential range of effect sizes in different clinical contexts. While some studies showed minimal benefits, others demonstrated substantial improvements, underscoring the role of context-specific factors and methodological differences.
These findings emphasize the need for greater protocol standardization and better patient stratification in future trials to optimize treatment effectiveness and improve cross-study comparability. (See Figure 5)
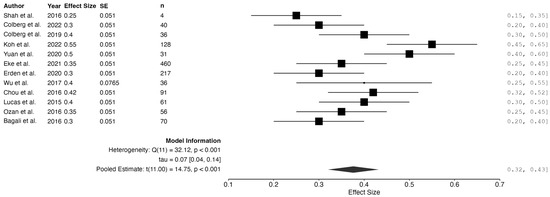
Figure 5.
Meta-analysis: use of adjuvant therapy. Studies included: Shah et al., 2016 [14]; Colberg et al., 2022 [17]; Colberg et al., 2019 [18]; Koh et al., 2022 [30]; Yuan et al., 2020 [29]; Eke et al., 2021 [22]; Erden et al., 2020 [23]; Wu et al., 2017 [28]; Chou et al., 2016 [21]; Lucas et al., 2015 [24]; Ozan et al., 2016 [26]; Bagali et al., 2016 [20].
3.6. Meta-Regression
In the meta-regression for patient satisfaction, the model demonstrated an R2 of 0.827, indicating that it accounts for approximately 82.7% of the variability in postoperative satisfaction. Among the factors evaluated, the duration of follow-up presented a coefficient of −0.00, without achieving statistical significance (p = 0.521), suggesting that a longer follow-up period is not directly associated with increased satisfaction.
Conversely, the utilization of adjuvant therapies exhibited a positive coefficient of 1.04, albeit without statistical significance (p = 0.302), implying that these complementary treatments may be associated with greater patient satisfaction, although the evidence is inconclusive. These findings underscore the necessity for further research to definitively determine whether adjuvant therapies can enhance the patient experience post-intervention.
For improvement in the VAS score, the model yielded an R2 of 0.561, explaining 56.1% of the variability in postoperative pain reduction. Regarding predictive factors, the duration of follow-up exhibited a coefficient of −0.01 (p = 0.792), with no discernible relationship between the follow-up duration and pain reduction.
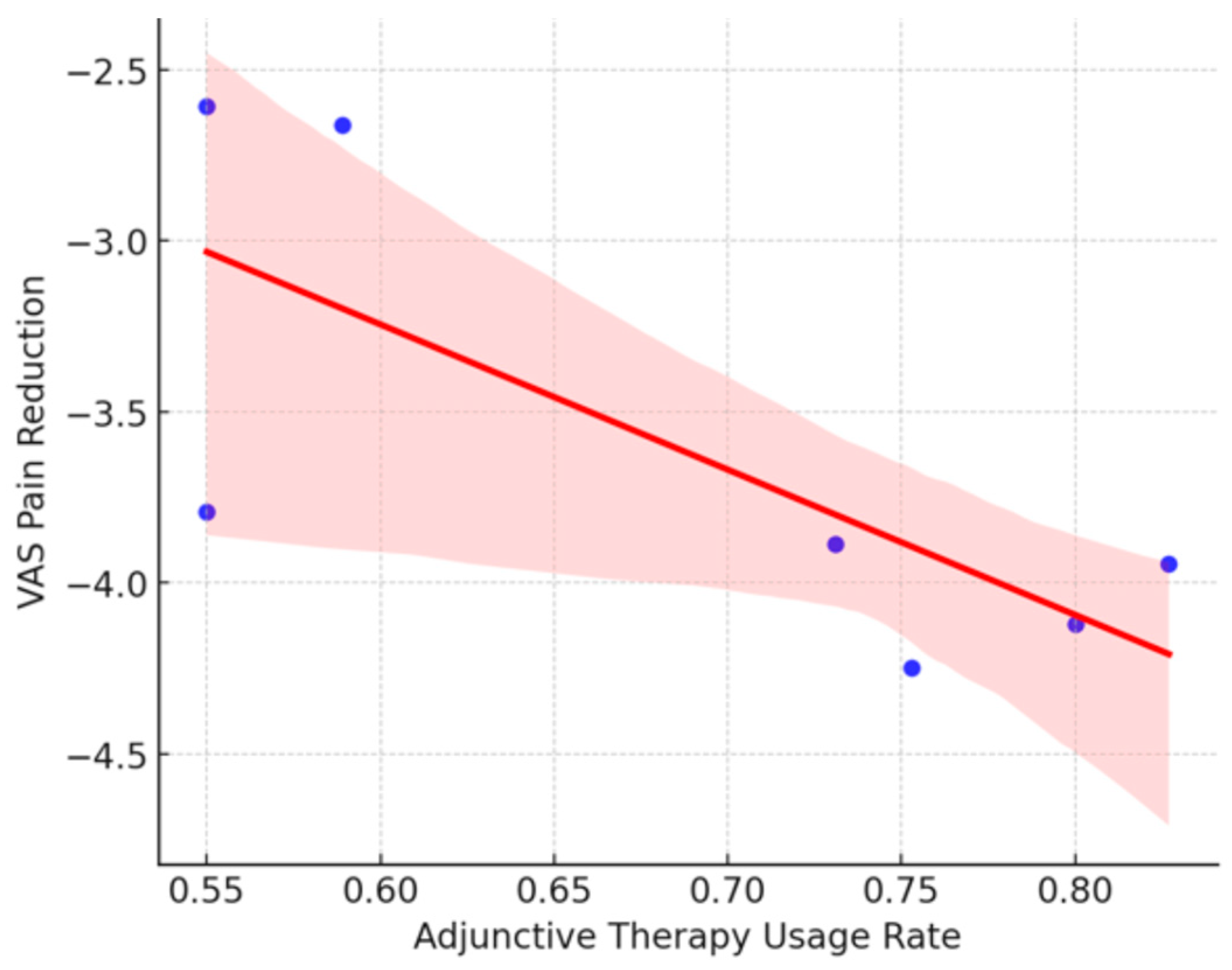
However, the utilization of adjuvant therapies presented a negative coefficient of −3.77, although not statistically significant (p = 0.211), which may indicate that the addition of complementary therapies does not consistently result in significant improvement in pain relief. Nevertheless, given the lack of statistical significance, these results should be interpreted with caution, considering that other unexamined factors may influence these outcomes.
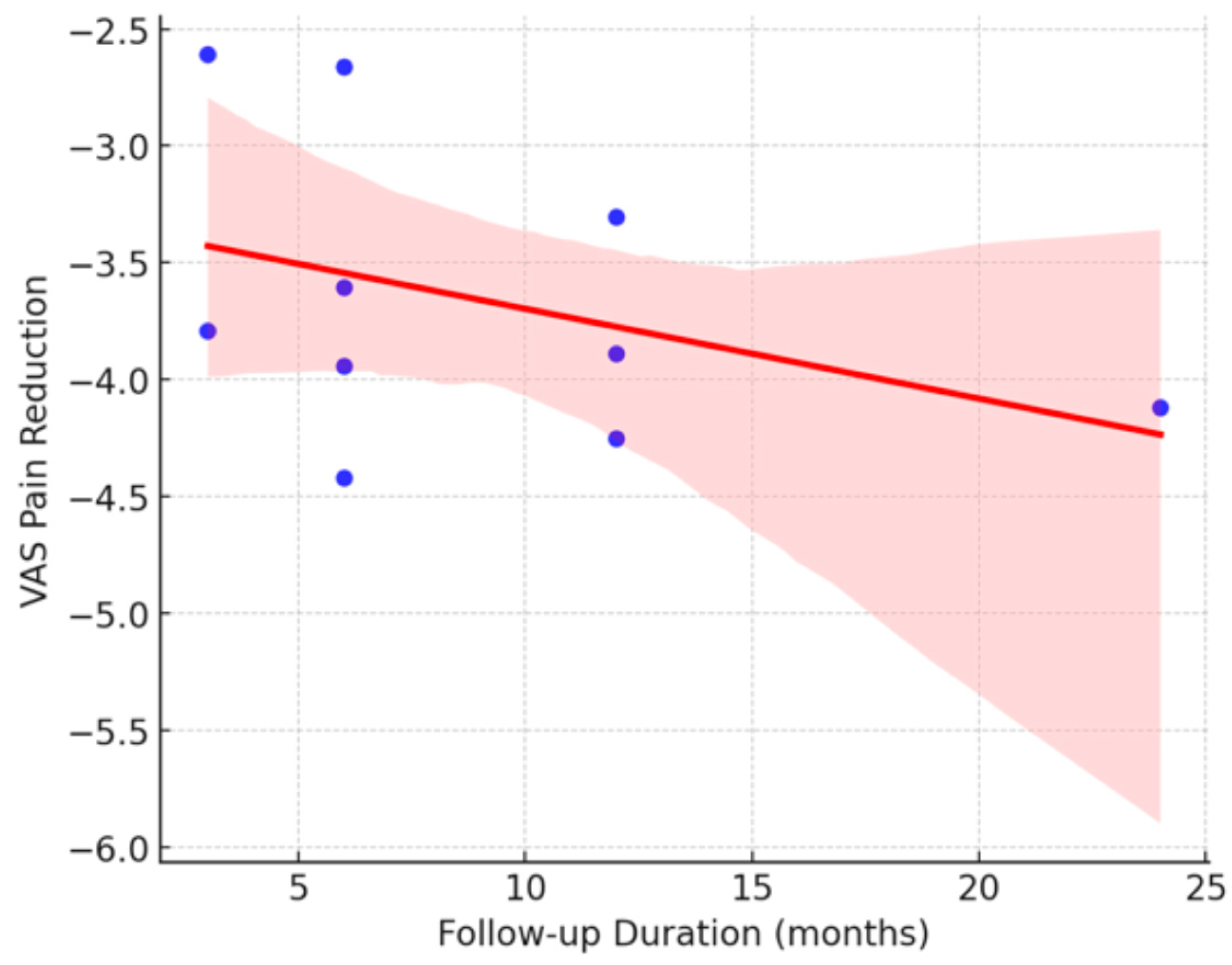
These findings suggest that patient satisfaction and improvement in VAS pain are influenced by multiple factors; however, none of the variables analyzed demonstrated a statistically significant association. This indicates that other factors, such as individual patient characteristics, variations in surgical techniques employed, or subjective evaluation criteria, may affect postoperative outcomes. (See Figure 6 and Figure 7).
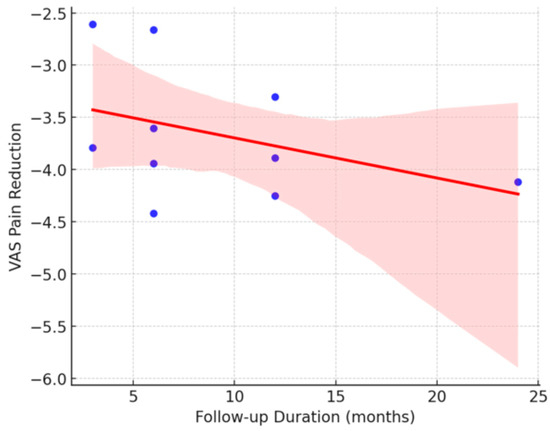
Figure 6.
Impact of follow-up duration on pain reduction (VAS) after treatment.
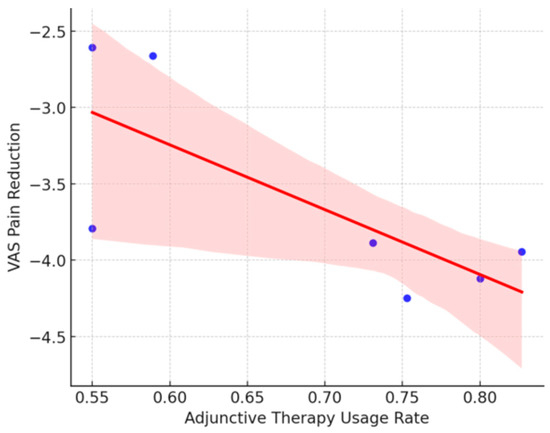
Figure 7.
Influence of adjunctive therapy usage on pain reduction (VAS).
The graphs illustrate the relationship between clinical factors and postoperative outcomes in terms of patient satisfaction and pain reduction, measured using the VAS. In Figure 6, the Duration of Follow-up vs. Pain Reduction (VAS) shows a slight negative trend, although not statistically significant, suggesting that studies with longer follow-up periods do not necessarily demonstrate greater pain reduction. In Figure 7, the Use of Adjuvant Therapies vs. Pain Reduction (VAS) shows a negative trend, indicating that the use of adjuvant therapies is not consistently associated with greater pain reduction, and in some instances, may not confer additional benefits. However, the absence of statistical significance necessitates cautious interpretation of these observations, and further evidence is required to draw definitive conclusions.
4. Discussion
The objective of this systematic review was to evaluate the efficacy of the Topaz technique in the treatment of chronic plantar fasciitis and to assess the duration and postoperative care required following its implementation. Furthermore, the most prevalent potential adverse effects associated with this technique were identified. We aimed to compare the benefits of the Topaz technique, both in isolation and in combination with other treatments, such as gastrocnemius lengthening, and to elucidate its advantages over alternative surgical techniques for the plantar fascia.
In the literature reviewed, the majority of articles focused on the evaluation of the Topaz technique for the treatment of chronic plantar fasciitis. This treatment is primarily utilized for lesions with a duration exceeding six months and previous failures of conservative treatment. Certain studies, such as that of Huang et al. [16], have combined this technique with gastrocnemius lengthening. That study compared the success rate of the technique in isolation and combined with gastrocnemius intervention, demonstrating that the combination of both techniques yielded superior results. This suggests that retraction of the posterior leg musculature may be closely linked to fascial involvement due to structural tension.
Some authors have compared RFM with other surgical techniques, such as fasciotomy, either endoscopically (Wang et al. [27]) or open (Yuan et al. [29]). These comparisons highlight the benefits of RFM over conventional techniques, including improved wound healing, earlier return to activity, and preservation of nerve branches. Although fasciotomies exhibit high success rates (88%), preliminary results indicate that the Topaz technique has higher success rates (95%) [13]. Moreover, the Topaz technique has the advantage of mitigating post-surgical complications, such as flatfoot or Achilles tendon injuries, which may be more frequent in more invasive procedures, such as fasciotomy [29] to emphasize the absence of side effects.
Additionally, to provide better clinical context and a more comprehensive understanding of the procedure’s safety profile, we included a comparative analysis of complication rates reported for other therapeutic approaches, both surgical and conservative. Open surgical techniques, such as plantar fasciotomy, are often associated with a higher incidence of complications, including infections, biomechanical alterations, and nerve injuries (REF). In contrast, conservative treatments generally offer a favorable safety profile but may not yield sustained improvements in chronic cases (REF). In contrast, the Topaz technique demonstrates a significantly lower complication rate, as shown in this review (3.00%) (REF), highlighting its safety and positioning it as an effective and minimally invasive alternative within the stepwise management of chronic plantar fasciopathy.
It is noteworthy that isolated complications such as cellulitis, tendinitis of the flexor of the first toe or peroneal tendons, and even ulcerations or deep vein thrombosis may occur, which generally resolve without apparent sequelae [18,24]. There are low failure rates in performing Topaz, as demonstrated by Wang W et al. [27] and Colberg et al. [17]. In these cases, the persistence of pain or its recurrence could be attributed to an incorrect diagnosis of the pathology, as occurs when a positive Tinel’s sign is present, suggesting neuropathic involvement leading to pain, as concluded by Chou A et al. [21] and Koh DTS et al. [30]. Therefore, it is essential to establish an accurate diagnosis and utilize the necessary diagnostic tests to confirm the etiology of pain [8].
Regarding clinical indications, several authors concur on the exclusion of specific patient groups, including pregnant women, diabetics, individuals with systemic diseases, those exhibiting a positive Tinel’s sign, patients with a BMI exceeding 35 kg/m2, and those with a history of previous foot and ankle pathologies or surgeries. This exclusion is essential to prevent confounding factors from influencing the results. In this context, Wu P et al. [31] observed that in patients with obesity, recovery was prolonged in these cases, with delayed healing and symptom resolution, compared to non-obese patients. However, studies conducted by Koh et al., 2022 [30], Eke et al., 2021 [22], and Shah et al., 2016 [14] reported no variability in the results due to this factor.
RFM can be performed using either ultrasound-guided or non-ultrasound-guided techniques, both of which are based on the same principle but employ different approaches [9,10]. The accuracy and outcomes of the ultrasound-guided technique appear to be highly favorable, although there is limited scientific evidence owing to the novelty of the technique. Nevertheless, authors such as Wu et al., 2017 [28] and Shah et al., 2016 [14] asserted that the ultrasound-guided technique yielded superior results, with reduced tissue damage and increased accuracy.
Regarding post-surgical care, the majority of studies advocate for the application of a compressive bandage covering the incisions, as indicated by Lucas et al., 2015 [24] and Moller et al., 2022 [25]. However, there is debate concerning the duration of rest and progression of weight-bearing. Authors such as Ozan et al., 2016 [26] support a more rapid recovery, while others, such as Yuan et al., 2020 [29] and Colberg et al., 2019 [18], propose a more extended rest period. Ultimately, post-surgical care, including appropriate rest and progressive rehabilitation, is crucial for ensuring optimal outcomes of the intervention.
One limitation of this review is the paucity of clinical evidence, as the technique is relatively novel, and the available literature is limited. An exhaustive search of the past decade was conducted, resulting in the selection of 15 articles. Additionally, radiofrequency is utilized as an ablative method for nerve branch disorders, such as neuropathy of Baxter’s nerve, which induces heel pain. However, this treatment modality was excluded from this review due to its distinct objectives and techniques compared to Topaz.
In addition to the limited number and methodological variability of the studies included, another relevant limitation was the lack of standardization of postoperative rehabilitation protocols. Differences in weight-bearing progression, physical therapy approaches, and follow-up durations may have influenced the reported outcomes and potentially acted as confounding variables. Furthermore, although the Topaz technique is widely used, the exact biological mechanisms underlying its effectiveness have not yet been fully elucidated. Current evidence suggests that radiofrequency microtenotomy promotes tissue regeneration through two primary mechanisms: neuromodulation, which alters local nociceptive input and reduces chronic pain signaling, and collagen remodeling, which stimulates angiogenesis and reparative cellular activity at the treatment site. However, variability in patient response may be partially explained by individual differences in tissue biology, comorbidities, and adherence to post-surgical care. Future studies should aim to clarify these mechanisms and control for these factors to enhance the reliability and reproducibility of outcomes.
The RFM technique shows potential to become the gold standard for treating chronic plantar fasciitis, due to the high success rate observed and the low incidence of complications post-surgery. Several studies have highlighted that combining radiofrequency coblation (Topaz technique) with gastrocnemius recession may yield superior clinical outcomes compared with either technique alone in patients with recalcitrant plantar fasciitis. Koh et al., 2022 [30] demonstrated that the combined treatment group showed greater pain reduction (VAS) at both 6 and 24 months postoperatively, without an increase in complications. Similarly, Huang et al., 2018 [16] observed more significant improvements in both pain and function when both interventions were applied together, supporting the hypothesis that their biomechanical and neuromodulatory effects are synergistic. These findings emphasize the importance of individualized pre-surgical assessment in selecting the appropriate intervention strategy, as generalized approaches may overlook key patient-specific factors that influence outcomes.
One important consideration when interpreting the results of this review is the potential influence of patient-specific factors, such as age and symptom duration, on treatment outcomes. Although the included studies did not consistently provide stratified data in this regard, it is plausible that patients with a shorter history of symptoms may exhibit more reversible pathological changes, thereby responding more favorably to the Topaz technique. Conversely, those with longstanding chronic plantar fasciopathy may present with more advanced tissue degeneration, potentially limiting the efficacy of interventions. Similarly, the regenerative capacity of connective tissue is known to decline with age, which could negatively impact both the speed and extent of recovery in older individuals. These aspects represent a relevant clinical dimension that should be further explored in future studies to better define the patient selection criteria and optimize treatment protocols [4].
Additionally, a specific analysis was included to address how the methodological quality of the included studies may have influenced the results of this review. Although well-established tools such as GRADE, ROBINS-I, ROB-2, and the JBI scale were applied to assess the risk of bias according to study design, several studies, particularly retrospective studies and case series, presented significant limitations. These limitations may have affected the magnitude of the observed effects on key variables, such as pain reduction and functional improvement. The presence of selection bias, confounding, or selective outcome reporting may partly explain the statistical heterogeneity found in the analyses. Therefore, although the overall findings favor the Topaz technique, the results of lower-quality studies should be interpreted with caution. In this context, future randomized controlled trials with more rigorous designs and lower risk of bias are needed to strengthen the current evidence.
5. Conclusions
The Topaz technique radiofrequency appears to be a safe and effective option for the treatment of chronic plantar fasciopathy, particularly in patients unresponsive to conservative therapies. This technique is associated with high success rates, low complication risks, and relatively fast recovery. Its ultrasound-guided application enhances procedural accuracy and minimizes tissue damage. Additionally, combining this approach with gastrocnemius lengthening may improve outcomes in selected cases. While current evidence supports its clinical utility, further high-quality studies are needed to assess its long-term efficacy and standardize treatment protocols.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/jcm14082843/s1, PRISMA 2020 Checklist [19].
Author Contributions
Conceptualization, S.D.-M., J.F.-T. and J.V.-M.; Data curation, J.V.-M. and N.F.-E.; Formal analysis, E.N.-G., J.V.-M. and J.F.-T.; Investigation, L.R.-A., E.N.-G. and J.V.-M.; Methodology, S.D.-M., J.F.-T., E.N.-G. and L.R.-A.; Supervision, N.F.-E., J.V.-M., J.F.-T., E.N.-G. and S.D.-M.; Validation, S.D.-M., J.V.-M., J.F.-T., E.N.-G. and L.R.-A.; Writing—original draft, S.D.-M., J.V.-M. and J.F.-T.; Writing—review and editing, S.D.-M., J.F-T., J.V.-M., N.F.-E. and L.R.-A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are contained within this article.
Acknowledgments
The authors thank the Catholic University of Valencia San Vicente Mártir for their contributions and help in the payment of the Open Access publication free.
Conflicts of Interest
None of the authors have any financial, personal, or professional conflicts of interest related to the results of this study.
Abbreviations
The following abbreviations are used in this manuscript:
| Abbreviation | Meaning |
| AOFAS | American Orthopaedic Foot & Ankle Society |
| BMI | Body Mass Index |
| CRD | Centre for Reviews and Dissemination |
| CSI | Corticosteroid Injection |
| DVT | Deep Vein Thrombosis |
| ESWT | Extracorporeal Shock Wave Therapy |
| FAAMA | Foot and Ankle Ability Measure—Activities of Daily Living |
| FAAMS | Foot and Ankle Ability Measure—Sports |
| FADI | Foot and Ankle Disability Index |
| FHSQ-DK | Foot Health Status Questionnaire—Danish Version |
| GPE | Global Perceived Effect |
| GRADE | Grading of Recommendations, Assessment, Development, and Evaluation |
| HSRT | Heavy Slow Resistance Training |
| IPAQ | International Physical Activity Questionnaire |
| JBI | Joanna Briggs Institute |
| NRS | Numeric Rating Scale |
| PASS | Patient Acceptable Symptom State |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| PRP | Platelet-Rich Plasma |
| RF | Radiofrequency |
| RFM | Radiofrequency Microtenotomy |
| ROB-2 | Risk Of Bias In Randomized Trials |
| ROBINS-I | Risk Of Bias In Non-randomized Studies—of Interventions |
| RTL | Radiofrequency Thermal Lesioning |
| SF-36 | Short Form Health Survey |
| VAS | Visual Analog Scale |
Appendix A
Appendix A.1. Search Strings for Electronic Databases
The original search string was created using PubMed. The search strings employed for Web of Science and MEDLINE via PubMed were translated using an automatic online tool https://www.sr-accelerator.com/#/polyglot: accessed on 10 February 2025.
Appendix A.1.1. Search Strategy for PubMed
URL: https://pubmed.ncbi.nlm.nih.gov (accessed on 5 February 2025).
(“fasciitis, plantar”[MeSH Terms] OR “Tibial Neuropathy”[MeSH Terms] OR (“plantar fasciitis”[Title/Abstract] OR “plantar fasciopathy”[Title/Abstract] OR “plantar fasciosis”[Title/Abstract])) AND (“Radiofrequency Therapy”[MeSH Terms] OR “Pulsed Radiofrequency Treatment”[MeSH Terms] OR (“radiofrecuency”[Title/Abstract] OR “microtenotomy”[Title/Abstract] OR “topaz”[Title/Abstract] OR “cobla-tion”[Title/Abstract])).
Appendix A.1.2. Search Strategy for Web of Science
URL: https://www.webofscience.com/wos/alldb/basic-search (accessed on 05 February 2025).
Filters: No filters were applied.
“plantar fasciitis” OR “heel pain” OR “plantar fasciosis” OR “plantar fasciopathy” (Topic) and “radiofrequency” “microtenotomy” OR “topaz” OR “coblation” OR “rf” (Topic).
Appendix A.1.3. Search Strategy for Scopus
(TITLE-ABS-KEY ((“plantar fasciitis” OR “plantar fasciosis” OR “plantar fasciopathy” OR “heel pain”)).
AND TITLE-ABS-KEY ((“radiofrequency” OR “microtenotomy” OR “Topaz” OR “coblation” OR “RF”))).
Appendix A.1.4. Search EBSCOH
(MH “Heel Pain”) OR (MH “Plantar Fasciitis”) OR TI ( plantar fasciitis or plantar heel pain or plantar fasciopathy or plantar fasciosis) OR AB ( plantar fasciitis or plantar heel pain or plantar fasciopathy or plantar fasciosis) AND (MH “Radiofrequency Thera-py+”) OR TI (radiofrequency therapy OR topaz OR microtenotomy OR coblation) OR AB (radiofrequency therapy OR topaz OR microtenotomy OR coblation).
References
- Latt, L.D.; Jaffe, D.E.; Tang, Y.; Taljanovic, M.S. Evaluation and Treatment of Chronic Plantar Fasciitis. Foot Ankle Orthop. 2020, 5, 2473011419896763. [Google Scholar] [CrossRef] [PubMed]
- Thompson, J.V.; Saini, S.S.; Reb, C.W.; Daniel, J.N. Diagnosis and Management of Plantar Fasciitis. J. Am. Osteopath. Assoc. 2014, 114, 900–906. [Google Scholar] [CrossRef] [PubMed]
- Lim, A.T.; How, C.H.; Tan, B. Management of Plantar Fasciitis in the Outpatient Setting. Singap. Med. J. 2016, 57, 168–171. [Google Scholar] [CrossRef] [PubMed]
- Ali, Q.; Long, Y.; Ali, M. Prevalence, Causes, and Treatment of Plantar Fasciitis in Young Females of a Medical College. Bull. Fac. Phys. Ther. 2024, 29, 31. [Google Scholar] [CrossRef]
- Buchbinder, R. Plantar Fasciitis. N. Engl. J. Med. 2004, 350, 2159–2166. [Google Scholar] [CrossRef]
- Riddle, D.L.; Pulisic, M.; Pidcoe, P.; Johnson, R.E. Risk Factors for Plantar Fasciitis: A Matched Case-Control Study. J. Bone Jt. Surg. Am. 2003, 85, 872–877. [Google Scholar] [CrossRef]
- Nahin, R.L. Prevalence and Pharmaceutical Treatment of Plantar Fasciitis in United States Adults. J. Pain 2018, 19, 885–896. [Google Scholar] [CrossRef]
- Khammas, A.S.A.; Mahmud, R.; Hassan, H.A.; Ibrahim, I.; Mohammed, S.S. An Assessment of Plantar Fascia with Ultrasound Findings in Patients with Plantar Fasciitis: A Systematic Review. J Ultrasound 2023, 26, 13–38. [Google Scholar] [CrossRef]
- Bolívar, Y.A.; Belloso, A.J.P.; Sanz, J.A.; Sánchez, E.C.; Bueno, M.R.; Podología, D.E. Influencia Del Acortamiento de La Musculatura Posterior de La Extremidad Inferior En La Etiología de La Fascitis Plantar. Rev. Esp. Podol. 2012, XXIII, 92–94. Available online: https://www.revesppod.com/Documentos/ArticulosNew/X0210123812502404.pdf (accessed on 6 February 2025).
- Ang, T.W.A. The Effectiveness of Corticosteroid Injection in the Treatment of Plantar Fasciitis. Singap. Med. J. 2015, 56, 423–432. [Google Scholar] [CrossRef]
- Schuitema, D.; Greve, C.; Postema, K.; Dekker, R.; Hijmans, J.M. Effectiveness of Mechanical Treatment for Plantar Fasciitis: A Systematic Review. J. Sport Rehabil. 2019, 29, 657–674. [Google Scholar] [CrossRef] [PubMed]
- Rhim, H.C.; Kwon, J.; Park, J.; Borg-Stein, J.; Tenforde, A.S. A Systematic Review of Systematic Reviews on the Epidemiology, Evaluation, and Treatment of Plantar Fasciitis. Life 2021, 11, 1287. [Google Scholar] [CrossRef] [PubMed]
- Campillo-Recio, D.; Ibañez, M.; Martin-Dominguez, L.A.; Comas-Aguilar, M.; Fernandez-Morales, M.; Alberti-Fito, G. Local Percutaneous Radiofrequency for Chronic Plantar Fasciitis. Arthrosc. Tech. 2021, 10, e1315–e1320. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.; Best, A.J.; Rennie, W.J. Percutaneous Ultrasound-Guided TOPAZ Radiofrequency Coblation: A Novel Coaxial Technique for the Treatment of Recalcitrant Plantar Fasciitis—Our Experience. J. Ultrasound Med. 2016, 35, 1325–1331. [Google Scholar] [CrossRef]
- Gamba, C.; Ferrer-Catasus, T.; Serrano-Chinchilla, P.; Pérez-Prieto, D.; González-Lucena, G.; Ginés-Cespedosa, A. Fascitis Plantar Recalcitrante: ¿fasciotomía Parcial o Liberación de Gemelo Medial? Resultados Preliminares a 6 Meses. Rev. Del Pie Y Tobillo 2019, 33, 17. [Google Scholar] [CrossRef]
- Huang, D.M.; Chou, A.C.; Yeo, N.E.; Singh, I.R. Radiofrequency Microtenotomy with Concurrent Gastrocnemius Recession Improves Postoperative Vitality Scores in the Treatment of Recalcitrant plantar fasciitis. Ann. Acad. Med. Singap. 2018, 47, 509–515. [Google Scholar] [CrossRef]
- Colberg, R.E.; Kenneth-Nwosa, K.O.; Jurado Vélez, J.A.; Slowik, J.S.; Fleisig, G.S. Clinical and Imaging Outcomes of Plantar Fasciotomy Using Microdebrider Coblation Wand. Foot Ankle Orthop. 2022, 7, 24730114221091797. [Google Scholar] [CrossRef]
- Colberg, R.E.; Ketchum, M.; Javer, A.; Drogosz, M.; Gomez, M.; Fleisig, G.S. Clinical Outcomes of Percutaneous Plantar Fasciotomy Using Microdebrider Coblation Wand. Foot Ankle Int. 2020, 41, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Larissa, S.; Jennifer, T.; Akl Elie, A.; Brennan Sue, E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Bagali, A.M.; Saif, A.M. The Effectiveness of Radiofrequency-Based Percutaneous Microtenotomy (TOPAZ) to Treat. Refract. Plantar Fasciitis 2016, 3, 3–7. [Google Scholar]
- Chou, A.C.C.; Ng, S.Y.C.; Su, D.H.C.; Singh, I.R.; Koo, K. Radiofrequency Microtenotomy Is as Effective as Plantar Fasciotomy in the Treatment of Recalcitrant Plantar Fasciitis. Foot Ankle Surg. 2016, 22, 270–273. [Google Scholar] [CrossRef] [PubMed]
- Eke, I.; Akcal, M.A.; Sayrac, A.V.; Iyetin, Y. Effects of Intralesional Pulsed Radiofrequency Treatment on Pain in Patients with Calcaneal Spur: Results of 460 Patients. BMC Musculoskelet. Disord. 2021, 22, 1033. [Google Scholar] [CrossRef] [PubMed]
- Erden, T.; Toker, B.; Cengiz, O.; Ince, B.; Asci, S.; Toprak, A. Outcome of Corticosteroid Injections, Extracorporeal Shock Wave Therapy, and Radiofrequency Thermal Lesioning for Chronic Plantar Fasciitis. Foot Ankle Int. 2021, 42, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Lucas, D.E.; Ekroth, S.R.; Hyer, C.F. Intermediate-Term Results of Partial Plantar Fascia Release with Microtenotomy Using Bipolar Radiofrequency Microtenotomy. J. Foot Ankle Surg. 2015, 54, 179–182. [Google Scholar] [CrossRef]
- Møller, S.; Riel, H.; Wester, J.; Simony, A.; Viberg, B.; Jensen, C. Surgical or Non-Surgical Treatment of Plantar Fasciopathy (SOFT): Study Protocol for a Randomized Controlled Trial. Trials 2022, 23, 845. [Google Scholar] [CrossRef]
- Ozan, F.; Koyuncu, Ş.; Gürbüz, K.; Öncel, E.S.; Altay, T. Radiofrequency Thermal Lesioning and Extracorporeal Shockwave Therapy: A Comparison of Two Methods in the Treatment of Plantar Fasciitis. Foot Ankle Spec. 2017, 10, 204–209. [Google Scholar] [CrossRef]
- Wang, W.; Rikhraj, I.S.; Chou, A.C.C.; Chong, H.C.; Koo, K.O.T. Endoscopic Plantar Fasciotomy vs. Open Radiofrequency Microtenotomy for Recalcitrant Plantar Fasciitis. Foot Ankle Int. 2018, 39, 11–17. [Google Scholar] [CrossRef]
- Wu, Y.T.; Chang, C.Y.; Chou, Y.C.; Yeh, C.C.; Li, T.Y.; Chu, H.Y.; Chen, L.C. Ultrasound-Guided Pulsed Radiofrequency Stimulation of Posterior Tibial Nerve: A Potential Novel Intervention for Recalcitrant Plantar Fasciitis. Arch. Phys. Med. Rehabil. 2017, 98, 964–970. [Google Scholar] [CrossRef]
- Yuan, Y.; Qian, Y.; Lu, H.; Kou, Y.; Xu, Y.; Xu, H. Comparison of the Therapeutic Outcomes between Open Plantar Fascia Release and Percutaneous Radiofrequency Ablation in the Treatment of Intractable Plantar Fasciitis. J. Orthop. Surg. Res. 2020, 15, 55. [Google Scholar] [CrossRef]
- Koh, D.T.S.; Yeo, W.; Koo, K.O.T.; Singh, I.R.; Yeo, N.E.M. Radiofrequency Plantar Fascia Coblation With and Without Gastrocnemius Recession in the Management of Recalcitrant Plantar Fasciitis. Foot Ankle Int. 2022, 43, 1167–1173. [Google Scholar] [CrossRef]
- Wu, P.T.; Lee, J.S.; Wu, K.C.; Wu, T.T.; Shao, C.J.; Liang, F.W.; Chern, T.C.; Su, F.C.; Jou, I.M. Ultrasound-Guided Percutaneous Radiofrequency Lesioning When Treating Recalcitrant Plantar Fasciitis: Clinical Results. Ultraschall Medizin 2016, 37, 56–62. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).