
Small Drusen and Age-Related Macular Degeneration: The Beaver Dam Eye Study

Abstract
:1. Introduction
2. Experimental Section
2.1. Study Population
2.2. Procedures
2.3. Genetic Measurements
2.4. Definitions
- Level 1 (No drusen): No signs of any drusen or of early or late AMD.
- Level 2 (Minimal area of small hard distinct drusen): Presence of small hard distinct drusen <63 µm in diameter as the largest size drusen involving a circular area of the macula of up to 2596 µm² and no other signs of AMD.
- Level 3 (Small area of small hard distinct drusen): Presence of small hard distinct drusen <63 µm in diameter as the largest size drusen involving a circular area of the macula between 2597 µm² and 5192 µm² and no other signs of AMD.
- Level 4 (Moderate area of small hard distinct drusen): Presence of small hard distinct drusen <63 µm in diameter as the largest size drusen involving a circular area of the macula between 5193 µm² and 9086 µm² and no other signs of AMD.
- Level 5 (Large area of small hard distinct drusen): Presence of small hard distinct drusen <63 µm in diameter as the largest size drusen involving a circular area of the macula greater than 9086 µm² and no other signs of AMD.
- Level 6 (Intermediate drusen): Presence of one or more drusen 63 to 124 µm in diameter as the largest size drusen and no other signs of AMD.
2.5. Statistical Analysis
3. Results
3.1. Participant Characteristics
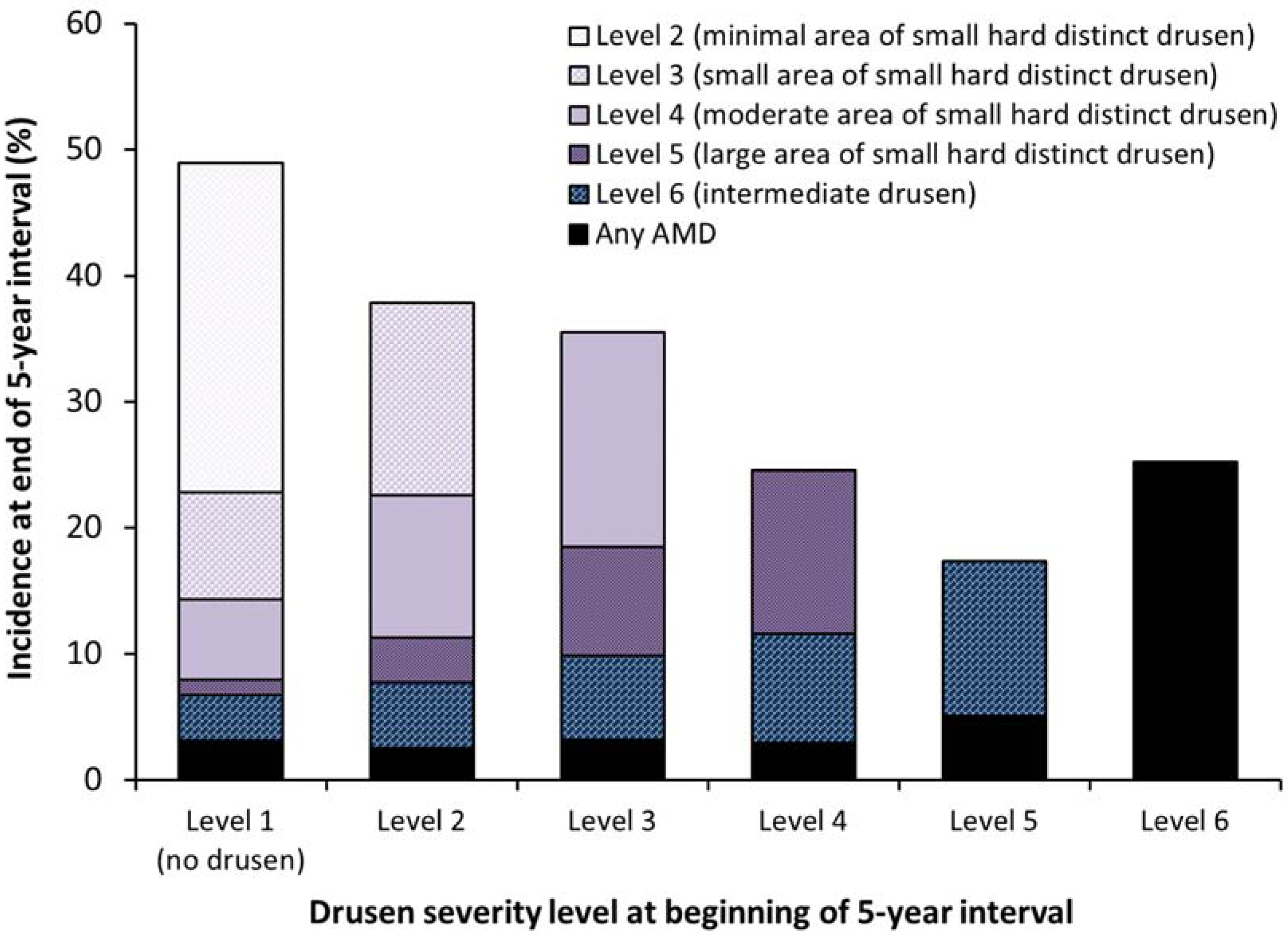
3.2. Incidence of Varying Areas of Small Hard Drusen, Intermediate Drusen, and Any AMD

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Person-Eye-Visits (N) | Mean (SD) or % | |
|---|---|---|---|
| Age, years | 15821 | 62.3 (9.5) | |
| Sex | Female | 9016 | 57.0 |
| Male | 6805 | 43.0 | |
| Beginning drusen severity level | Level 1 | 2206 | 13.9 |
| Level 2 | 4055 | 25.6 | |
| Level 3 | 2515 | 15.9 | |
| Level 4 | 2370 | 15.0 | |
| Level 5 | 2210 | 14.0 | |
| Level 6 | 2465 | 15.6 | |
| CFH genotype | T/T | 5942 | 40.6 |
| T/C | 6771 | 46.3 | |
| C/C | 1919 | 13.1 | |
| ARMS2 genotype | G/G | 9172 | 60.9 |
| G/T | 5323 | 35.3 | |
| T/T | 574 | 3.8 | |
| Hypertension present | No | 7911 | 50.4 |
| Yes | 7776 | 49.6 | |
| Body mass index, kg/m² | 15625 | 29.6 (5.6) | |
| Smoking history | Never | 7312 | 46.2 |
| Past | 6189 | 39.1 | |
| Current | 2312 | 14.6 | |
| Heavy drinking history | Never | 13377 | 84.6 |
| Past | 2154 | 13.6 | |
| Current | 276 | 1.7 | |
| Physical activity level | Active | 4843 | 30.6 |
| Sedentary | 10969 | 69.4 | |
| Using multivitamins | No | 7720 | 48.8 |
| Yes | 8101 | 51.2 | |
| Currently using aspirin | No | 10946 | 69.3 |
| Yes | 4854 | 30.7 |

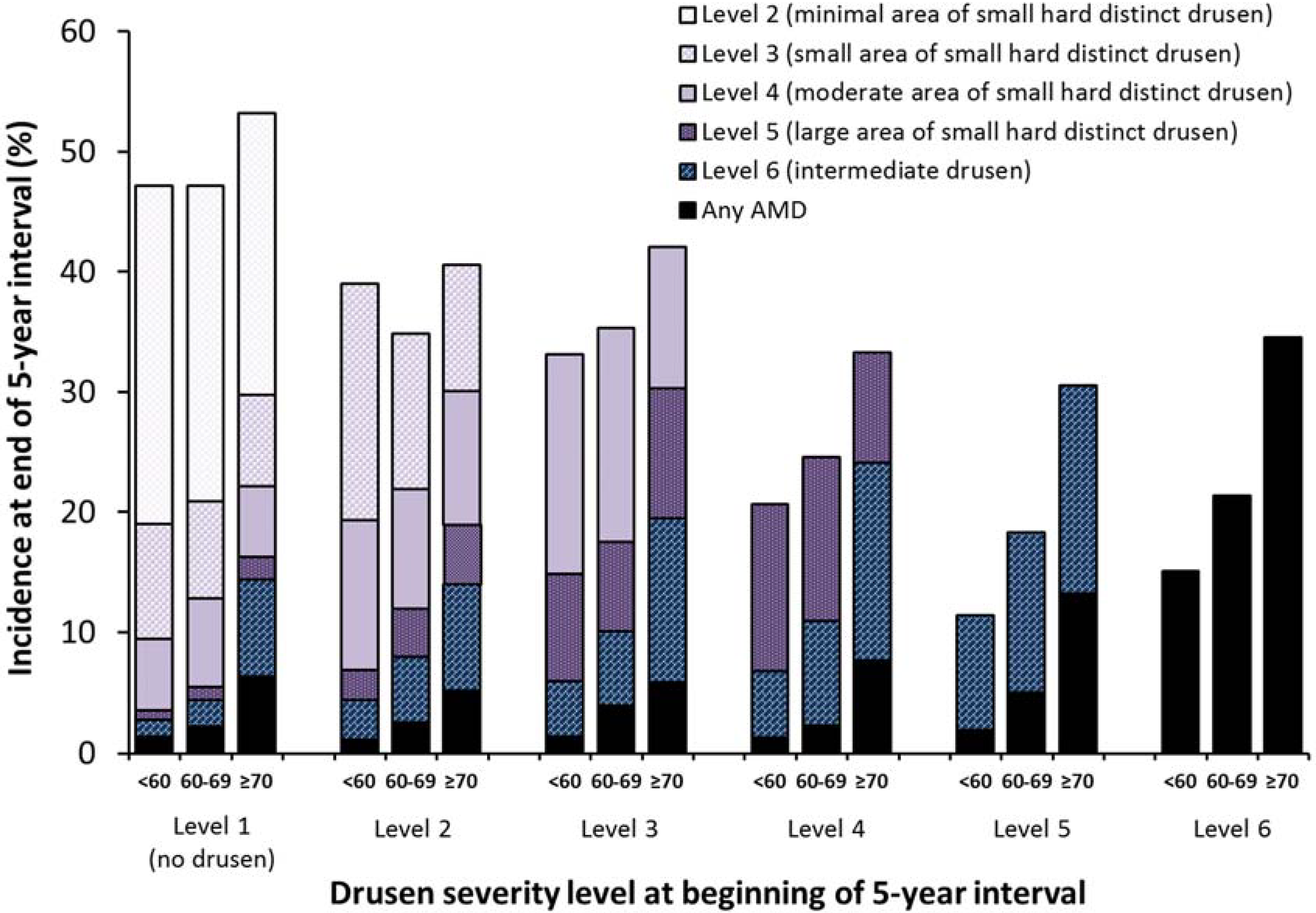
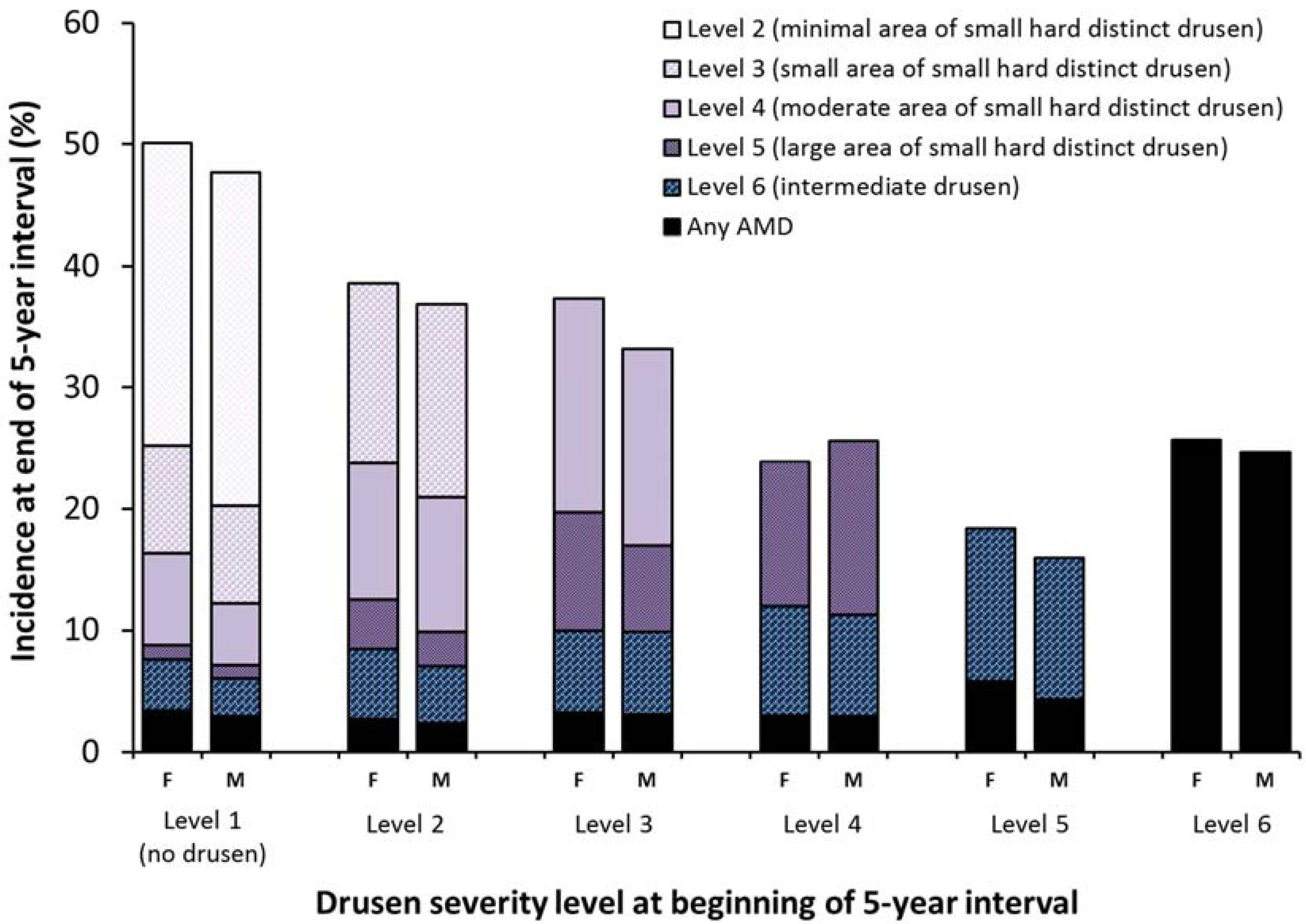
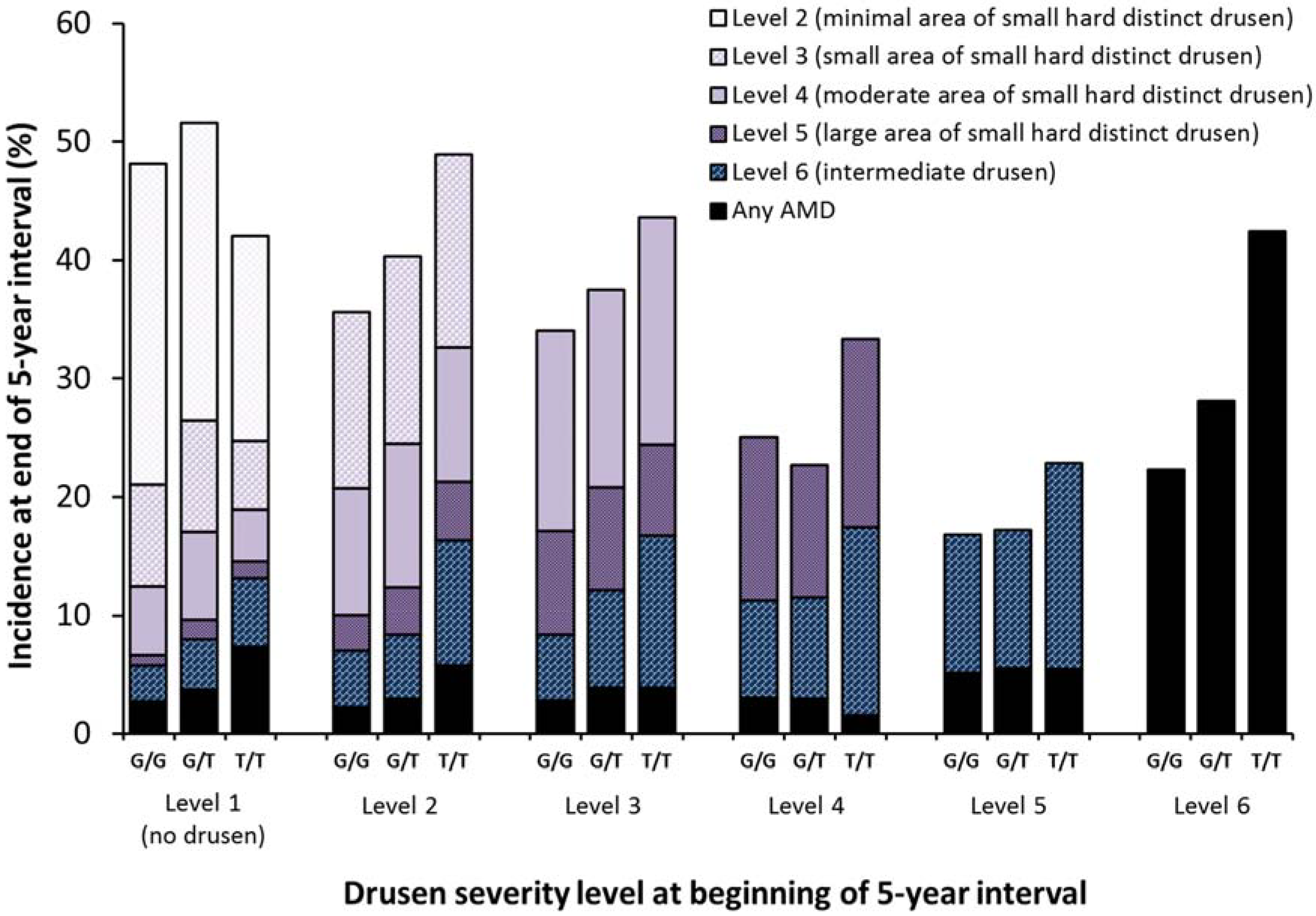
3.3. Relationships of Age, Sex and Two AMD Candidate Genes to the Five-Year Incidences of Small Hard Drusen, Intermediate Drusen and AMD
| Incidence of | Beginning Level | N at Risk | % Incident | Comparison Level | OR (95% CI) | p Value |
|---|---|---|---|---|---|---|
| Level 2 or worse | Level 1 | 2206 | 48.9 | |||
| Level 3 or worse | Level 1 | 2206 | 22.8 | <0.001 | ||
| Level 2 | 4055 | 37.8 | Level 1 | 2.0 (1.8, 2.3) | ||
| Level 4 or worse | Level 1 | 2206 | 14.3 | <0.001 | ||
| Level 2 | 4055 | 22.5 | Level 1 | 1.7 (1.5, 1.9) | ||
| Level 3 | 2515 | 35.5 | Level 2 | 1.9 (1.7, 2.1) | ||
| Per level | 1.8 (1.7, 1.9) | <0.001 | ||||
| Level 5 or worse | Level 1 | 2206 | 7.9 | <0.001 | ||
| Level 2 | 4055 | 11.3 | Level 1 | 1.4 (1.2, 1.7) | ||
| Level 3 | 2515 | 18.5 | Level 2 | 1.7 (1.5, 2.0) | ||
| Level 4 | 2370 | 24.5 | Level 3 | 1.4 (1.2, 1.6) | ||
| Per level | 1.5 (1.5, 1.6) | <0.001 | ||||
| Level 6 or worse | Level 1 | 2206 | 6.8 | <0.001 | ||
| Level 2 | 4055 | 7.7 | Level 1 | 1.2 (1.0, 1.4) | ||
| Level 3 | 2515 | 9.8 | Level 2 | 1.3 (1.1, 1.5) | ||
| Level 4 | 2370 | 11.6 | Level 3 | 1.2 (1.0, 1.4) | ||
| Level 5 | 2210 | 17.3 | Level 4 | 1.5 (1.3, 1.8) | ||
| Per level | 1.3 (1.2, 1.4) | <0.001 | ||||
| Any AMD | Level 1 | 2206 | 3.1 | <0.001 | ||
| Level 2 | 4055 | 2.5 | Level 1 | 0.8 (0.6, 1.1) | ||
| Level 3 | 2515 | 3.1 | Level 2 | 1.2 (0.9, 1.6) | ||
| Level 4 | 2370 | 2.9 | Level 3 | 0.9 (0.7, 1.3) | ||
| Level 5 | 2210 | 5.1 | Level 4 | 1.8 (1.3, 2.4) | ||
| Level 6 | 2465 | 25.2 | Level 5 | 5.5 (4.5, 6.8) | ||
| Per level | 1.8 (1.7, 1.9) | <0.001 |




4. Discussion
5. Conclusions
Supplementary Files
Supplementary File 1Acknowledgments
Author Contributions
Conflicts of Interest
References
- Van der Schaft, T.L.; Mooy, C.M.; de Bruijn, W.C.; Oron, F.G.; Mulder, P.G.; de Jong, P.T. Histologic features of the early stages of age-related macular degeneration. A statistical analysis. Ophthalmology 1992, 99, 278–286. [Google Scholar]
- Ferris, F.L.; Davis, M.D.; Clemons, T.E.; Lee, L.Y.; Chew, E.Y.; Lindblad, A.S.; Milton, R.C.; Bressler, S.B.; Klein, R. A simplified severity scale for age-related macular degeneration: AREDS Report No. 18. Arch. Ophthalmol. 2005, 123, 1570–1574. [Google Scholar] [CrossRef] [PubMed]
- Klein, R.; Klein, B.E.; Jensen, S.C.; Meuer, S.M. The five-year incidence and progression of age-related maculopathy: The Beaver Dam Eye Study. Ophthalmology 1997, 104, 7–21. [Google Scholar] [CrossRef] [PubMed]
- Seddon, J.M. Genetic and environmental underpinnings to age-related ocular diseases. Investig. Ophthalmol. Vis. Sci. 2013, 54, ORSF28–ORSF30. [Google Scholar] [CrossRef]
- Buitendijk, G.H.; Rochtchina, E.; Myers, C.; van Duijn, C.M.; Lee, K.E.; Klein, B.E.; Meuer, S.M.; de Jong, P.T.; Holliday, E.G.; Tan, A.G.; et al. Prediction of age-related macular degeneration in the general population: The Three Continent AMD Consortium. Ophthalmology 2013, 120, 2644–2655. [Google Scholar] [CrossRef] [PubMed]
- Klein, M.L.; Ferris, F.L., III; Francis, P.J.; Lindblad, A.S.; Chew, E.Y.; Hamon, S.C.; Ott, J. Progression of geographic atrophy and genotype in age-related macular degeneration. Ophthalmology 2010, 117, 1554–1559. [Google Scholar] [CrossRef] [PubMed]
- Klein, R.; Klein, B.E.; Knudtson, M.D.; Meuer, S.M.; Swift, M.; Gangnon, R.E. Fifteen-year cumulative incidence of age-related macular degeneration: The Beaver Dam Eye Study. Ophthalmology 2007, 114, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, P.; Wang, J.J.; Foran, S.; Smith, W. Five-year incidence of age-related maculopathy lesions: The Blue Mountains Eye Study. Ophthalmology 2002, 109, 1092–1097. [Google Scholar] [CrossRef] [PubMed]
- Klein, R.; Meuer, S.M.; Myers, C.E.; Buitendijk, G.H.; Rochtchina, E.; Choudhury, F.; de Jong, P.T.; McKean-Cowdin, R.; Iyengar, S.K.; Gao, X.; et al. Harmonizing the classification of age-related macular degeneration in the Three Continent AMD consortium. Ophthalmic Epidemiol. 2014, 21, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Klaver, C.C.; Assink, J.J.; van, L.R.; Wolfs, R.C.; Vingerling, J.R.; Stijnen, T.; Hofman, A.; de Jong, P.T. Incidence and progression rates of age-related maculopathy: The Rotterdam Study. Investig. Ophthalmol. Vis. Sci. 2001, 42, 2237–2241. [Google Scholar]
- Davis, M.D.; Gangnon, R.E.; Lee, L.Y.; Hubbard, L.D.; Klein, B.E.; Klein, R.; Ferris, F.L.; Bressler, S.B.; Milton, R.C. The Age-Related Eye Disease Study severity scale for age-related macular degeneration: AREDS Report No. 17. Arch. Ophthalmol. 2005, 123, 1484–1498. [Google Scholar] [CrossRef] [PubMed]
- Seddon, J.M.; Sharma, S.; Adelman, R.A. Evaluation of the clinical age-related maculopathy staging system. Ophthalmology 2006, 113, 260–266. [Google Scholar] [CrossRef] [PubMed]
- Klein, R.; Klein, B.E.; Linton, K.L. Prevalence of age-related maculopathy. The Beaver Dam Eye Study. Ophthalmology 1992, 99, 933–943. [Google Scholar] [CrossRef] [PubMed]
- Gass, J.D. Drusen and disciform macular detachment and degeneration. Arch. Ophthalmol. 1973, 90, 206–217. [Google Scholar] [CrossRef] [PubMed]
- Klein, R.; Klein, B.E.; Lee, K.E.; Cruickshanks, K.J.; Chappell, R.J. Changes in visual acuity in a population over a 10-year period: The Beaver Dam Eye Study. Ophthalmology 2001, 108, 1757–1766. [Google Scholar] [CrossRef] [PubMed]
- Klein, R.; Klein, B.E.; Lee, K.E.; Cruickshanks, K.J.; Gangnon, R.E. Changes in visual acuity in a population over a 15-year period: The Beaver Dam Eye Study. Am. J. Ophthalmol. 2006, 142, 539–549. [Google Scholar] [CrossRef] [PubMed]
- Klein, R.; Klein, B.E.; Lee, K.E. Changes in visual acuity in a population. The Beaver Dam Eye Study. Ophthalmology 1996, 103, 1169–1178. [Google Scholar] [CrossRef] [PubMed]
- Klein, R.; Lee, K.E.; Gangnon, R.E.; Klein, B.E. Incidence of visual impairment over a 20-year period: The Beaver Dam Eye Study. Ophthalmology 2013, 120, 1210–1219. [Google Scholar] [CrossRef] [PubMed]
- Klein, R.; Klein, B.E.; Linton, K.L.; de Mets, D.L. The Beaver Dam Eye Study: Visual acuity. Ophthalmology 1991, 98, 1310–1315. [Google Scholar] [CrossRef] [PubMed]
- Linton, K.L.; Klein, B.E.; Klein, R. The validity of self-reported and surrogate-reported cataract and age-related macular degeneration in the Beaver Dam Eye Study. Am. J. Epidemiol. 1991, 134, 1438–1446. [Google Scholar] [PubMed]
- Klein, R.; Klein, B.E.; Tomany, S.C.; Meuer, S.M.; Huang, G.H. Ten-year incidence and progression of age-related maculopathy: The Beaver Dam Eye Study. Ophthalmology 2002, 109, 1767–1779. [Google Scholar] [CrossRef] [PubMed]
- Klein, R.; Klein, B.E. The Beaver Dam Eye Study II. Manual of Operations; National Technical Information Sevice: Springfield, Virginia, USA, 1995; Accession No. PB95-273827. [Google Scholar]
- Klein, R.; Klein, B.E. The Beaver Dam Eye Study III. Manual of Operations; National Technical Information Service: Springfield, Virginia, USA, 1999; Accession No. PB99-137861. [Google Scholar]
- Klein, B.E.; Klein, R. The Beaver Dam Eye Study V. Manual of Operations; National Technical Information Sevice: Springfield, Virginia, USA, 2010; Accession No. PB2010-114194. [Google Scholar]
- Klein, R.; Klein, B.E. The Beaver Dam Eye Study. Manual of Operations, Revised; National Technical Information Sevice: Springfield, Virginia, USA, 1991; Accession No. PB91-149823. [Google Scholar]
- Klein, R.; Davis, M.D.; Magli, Y.L.; Segal, P.; Klein, B.E.; Hubbard, L. The Wisconsin Age-Related Maculopathy Grading System. Ophthalmology 1991, 98, 1128–1134. [Google Scholar] [CrossRef] [PubMed]
- Klein, R.; Davis, M.D.; Magli, Y.L.; Segal, P.; Klein, B.E.; Hubbard, L. The Wisconsin Age-Related Maculopathy Grading System. National Technical Information Sevice: Springfield, Virginia, USA, 1991; Accession No. PB91-184267. [Google Scholar]
- Klein, R.; Myers, C.E.; Meuer, S.M.; Gangnon, R.E.; Sivakumaran, T.A.; Iyengar, S.K.; Lee, K.E.; Klein, B.E. Risk alleles in CFH and ARMS2 and the long-term natural history of age-related macular degeneration: The Beaver Dam Eye Study. JAMA Ophthalmol. 2013, 131, 383–392. [Google Scholar] [CrossRef] [PubMed]
- Ardeljan, D.; Chan, C.C. Aging is not a disease: Distinguishing age-related macular degeneration from aging. Prog. Retin. Eye Res. 2013, 37, 68–89. [Google Scholar] [CrossRef] [PubMed]
- Ferris, F.L., III; Wilkinson, C.P.; Bird, A.; Chakravarthy, U.; Chew, E.; Csaky, K.; Sadda, S.R. Clinical classification of age-related macular degeneration. Ophthalmology 2013, 120, 844–851. [Google Scholar] [CrossRef] [PubMed]
- Rudolf, M.; Seckerdieck, K.; Grisanti, S.; Curcio, C.A. Internal structure consistent with remodelling in very small drusen, revealed by filipin histochemistry for esterified cholesterol. Br. J. Ophthalmol. 2014, 98, 698–702. [Google Scholar] [CrossRef] [PubMed]
- Rudolf, M.; Clark, M.E.; Chimento, M.F.; Li, C.M.; Medeiros, N.E.; Curcio, C.A. Prevalence and morphology of druse types in the macula and periphery of eyes with age-related maculopathy. Investig. Ophthalmol. Vis. Sci. 2008, 49, 1200–1209. [Google Scholar] [CrossRef]
- Yehoshua, Z.; Wang, F.; Rosenfeld, P.J.; Penha, F.M.; Feuer, W.J.; Gregori, G. Natural history of drusen morphology in age-related macular degeneration using spectral domain optical coherence tomography. Ophthalmology 2011, 118, 2434–2441. [Google Scholar] [CrossRef] [PubMed]
- Gragoudas, E.S.; Chandra, S.R.; Friedman, E.; Klein, M.L.; Van, B.M. Disciform degeneration of the macula. II. Pathogenesis. Arch. Ophthalmol. 1976, 94, 755–757. [Google Scholar] [CrossRef] [PubMed]
- Sarks, S.H.; Van, D.D.; Maxwell, L.; Killingsworth, M. Softening of drusen and subretinal neovascularization. Trans. Ophthalmol. Soc. UK 1980, 100, 414–422. [Google Scholar] [PubMed]
- Munch, I.C.; Ek, J.; Kessel, L.; Sander, B.; Almind, G.J.; Brondum-Nielsen, K.; Linneberg, A.; Larsen, M. Small, hard macular drusen and peripheral drusen: Associations with AMD genotypes in the Inter99 Eye Study. Investig. Ophthalmol. Vis. Sci. 2010, 51, 2317–2321. [Google Scholar] [CrossRef]
- Dietzel, M.; Pauleikhoff, D.; Arning, A.; Heimes, B.; Lommatzsch, A.; Stoll, M.; Hense, H.W. The contribution of genetic factors to phenotype and progression of drusen in early age-related macular degeneration. Graefes Arch. Clin. Exp. Ophthalmol. 2014, 252, 1273–1281. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klein, R.; Myers, C.E.; Lee, K.E.; Gangnon, R.E.; Sivakumaran, T.A.; Iyengar, S.K.; Klein, B.E.K. Small Drusen and Age-Related Macular Degeneration: The Beaver Dam Eye Study. J. Clin. Med. 2015, 4, 425-440. https://doi.org/10.3390/jcm4030425
Klein R, Myers CE, Lee KE, Gangnon RE, Sivakumaran TA, Iyengar SK, Klein BEK. Small Drusen and Age-Related Macular Degeneration: The Beaver Dam Eye Study. Journal of Clinical Medicine. 2015; 4(3):425-440. https://doi.org/10.3390/jcm4030425
Chicago/Turabian StyleKlein, Ronald, Chelsea E. Myers, Kristine E. Lee, Ronald E. Gangnon, Theru A. Sivakumaran, Sudha K. Iyengar, and Barbara E. K. Klein. 2015. "Small Drusen and Age-Related Macular Degeneration: The Beaver Dam Eye Study" Journal of Clinical Medicine 4, no. 3: 425-440. https://doi.org/10.3390/jcm4030425