
Long-Term Visual Outcomes for a Treat and Extend Anti-Vascular Endothelial Growth Factor Regimen in Eyes with Neovascular Age-Related Macular Degeneration

Abstract
:1. Introduction
2. Methods
2.1. Data Collection
2.2. Injection Technique
2.3. Image Grading
2.4. Statistical Analysis
3. Results
3.1. Baseline Demographic Characteristics and Correlation with Visual Outcome
3.2. Neovascular Lesions and Number of Injections

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics N = 128 Eyes | VA at 3 Years (logMAR) | VA Change at 3 Years (logMAR) | ≥3 Line Gainat 3 Years | ≥1 Line Lossat 3 Years | ||||
|---|---|---|---|---|---|---|---|---|
| Adjusted Mean (SE) | p Value | Adjusted Mean (SE) | p Value | Number (%) | p Value | Number (%) | p Value | |
| Baseline VA | - | <0.001 | - | <0.001 | - | <0.001 | - | 0.11 |
| 6-month VA | - | <0.001 | - | 0.068 | - | 0.979 | - | 0.083 |
| Total | 0.544 (0.037) | −0.106 (0.033) | 38 (28%) | 28 (22%) | ||||
| Anatomic classification | 0.006 | 0.001 | 0.041 | 0.478 | ||||
| 1 | 0.390 (0.050) | −0.113 (0.048) | 18 (47%) | 9 (32%) | ||||
| 2 | 0.695 (0.129) | −0.215 (0.123) | 6 (16%) | 3 (11%) | ||||
| 3 | 0.534 (0.055) | −0.060 (0.051) | 9 (24%) | 9 (32%) | ||||
| 4 | 0.761 (0.096) | −0.109 (0.087) | 5 (13%) | 7 (25%) | ||||
| Fluorescein classification | 0.544 (0.037) | 0.214 | −0.106 (0.033) | 0.194 | 0.521 | 0.613 | ||
| 1 | 0.463 (0.051) | −0.076 (0.043) | 18 (47%) | 13 (46%) | ||||
| 2 | 0.651 (0.109) | −0.269 (0.100) | 8 (21%) | 3 (11%) | ||||
| 3 | 0.606 (0.066) | −0.068 (0.064) | 9 (24%) | 8 (29%) | ||||
| 4 | 0.593 (0.122) | −0.094 (0.098) | 3 (8%) | 4 (14%) | ||||
| Lesion location | 0.841 | 0.023 | 0.09 | 0.01 | ||||
| foveal | 0.552 (0.045) | −0.166 (0.041) | 31 (82%) | 14 (50%) | ||||
| juxta | 0.559 (0.082) | 0.001 (0.065) | 3 (8%) | 6 (21%) | ||||
| extra | 0.490 (0.104) | 0.048 (0.066) | 4 (11%) | 8 (29%) | ||||
| Lesion area | - | 0.301 | - | 0.039 | - | 0.138 | - | 0.298 |
| Number of injections | - | <0.001 | - | 0.022 | - | 0.259 | - | 0.104 |
| Neovascular Lesion Type (FA + OCT) | Mean Number of Injections per Year | |||||
|---|---|---|---|---|---|---|
| 1st Year | 2nd Year | 3rd Year | 4th Year | 5th Year | 6th Year | |
| Type 1 | 9.4 | 8.2 | 8.6 | 8.6 | 8.5 | 9.1 |
| Type 2 | 8.3 | 6 | 7.8 | 7.8 | 8.1 | 8.2 |
| Type 3 | 8.7 | 8 | 7.5 | 8.1 | 7.8 | 8.4 |
| Type 4 (mixed) | 8.8 | 7.3 | 7.4 | 6.8 | 7.9 | 7 |
3.3. Retention Rate
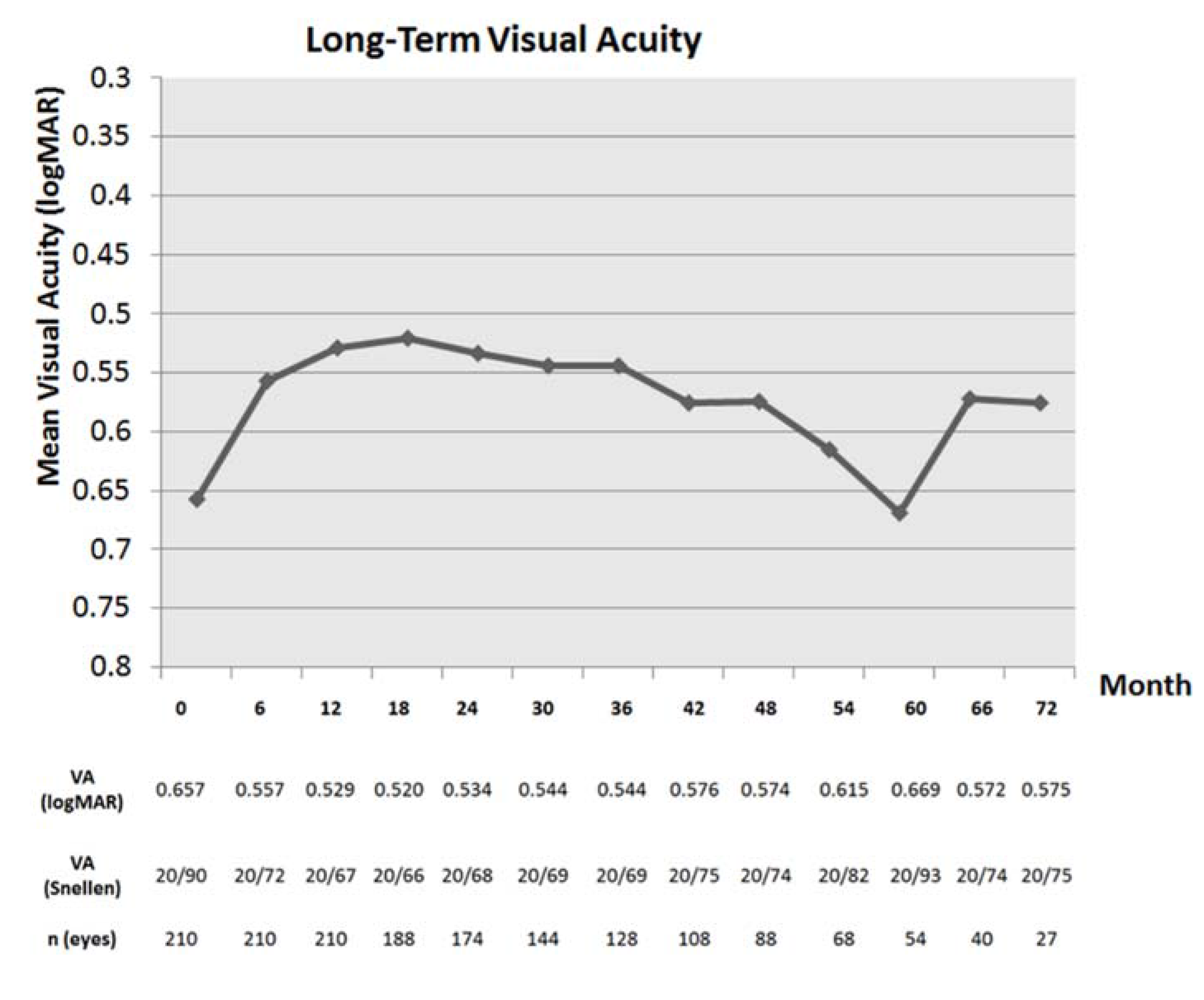
3.4. Visual Results for the Entire Cohort


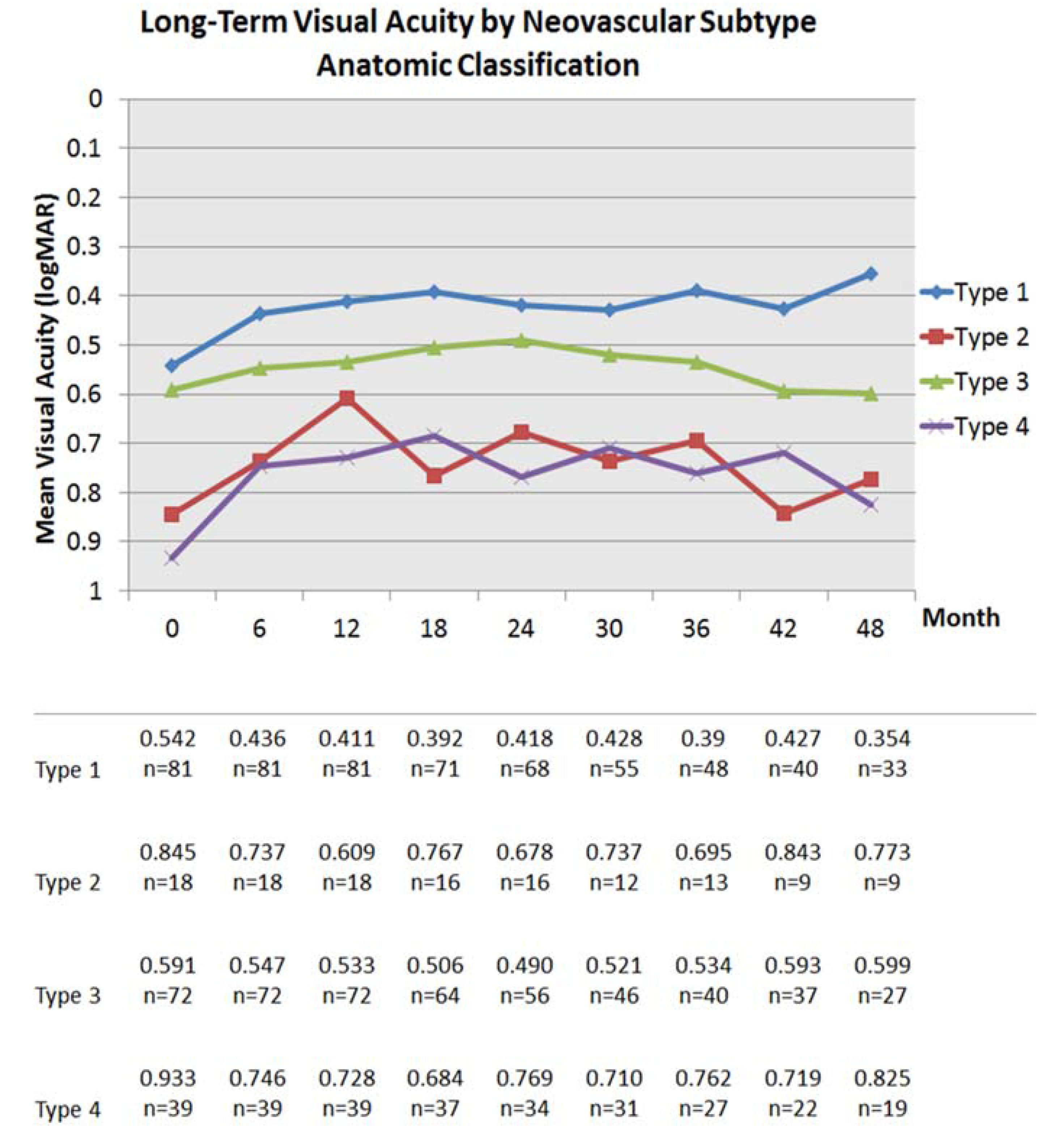
3.5. Visual Results by Neovascular Phenotype
| Baseline Characteristics N = 88 Eyes | VA at 4 Years (logMAR) | VA Change at 4 Years (logMAR) | ≥3 Line Gain at 4 Years | ≥1 Line Loss at 4 Years | ||||
|---|---|---|---|---|---|---|---|---|
| Adjusted Mean (SE) | p Value | Adjusted Mean (SE) | p Value | Number (%) | p Value | Number (%) | p Value | |
| Baseline VA | - | <0.001 | - | 0.002 | - | 0.001 | - | 0.384 |
| 6 month VA | - | <0.001 | - | 0.092 | - | 0.661 | - | 0.169 |
| Total | 0.574 (0.051) | −0.090 (0.044) | 26 (30%) | 20 (23%) | ||||
| Anatomic classification | 0.006 | 0.652 | 0.498 | 0.314 | ||||
| 1 | 0.354 (0.054) | −0.140 (0.054) | 11 (42%) | 5 (25%) | ||||
| 2 | 0.773 (0.185) | −0.105 (0.138) | 3 (12%) | 2 (10%) | ||||
| 3 | 0.599 (0.074) | −0.006 (0.073) | 7 (27%) | 9 (45%) | ||||
| 4 | 0.826 (0.148) | −0.114 (0.137) | 5 (19%) | 4 (20%) | ||||
| Fluorescein classification | 0.573 (0.051) | 0.135 | −0.090 (0.044) | 0.839 | 0.002 | 0.831 | ||
| 1 | 0.442 (0.061) | −0.094 (0.048) | 10 (39%) | 9 (45%) | ||||
| 2 | 0.713 (0.176) | −0.194 (0.166) | 6 (23%) | 3 (15%) | ||||
| 3 | 0.680 (0.089) | −0.022 (0.096) | 9 (35%) | 7 (35%) | ||||
| 4 | 0.650 (0.178) | −0.085 (0.107) | 1 (4%) | 1 (5%) | ||||
| Lesion location | 0.616 | 0.25 | 0.073 | 0.511 | ||||
| foveal | 0.581 (0.061) | −0.136 (0.056) | 23 (89%) | 13 (65%) | ||||
| juxta | 0.636 (0.133) | 0.022 (0.072) | 1 (4%) | 4 (20%) | ||||
| extra | 0.449 (0.139) | 0.036 (0.081) | 2 (8%) | 3 (15%) | ||||
| Lesion area | - | 0.592 | - | 0.043 | - | 0.049 | - | 0.085 |
| Number of injections | - | 0.007 | - | 0.175 | - | 0.57 | - | 0.242 |


3.6. Multivariate Analysis
| Time Point | Visual Parameter | Anatomic Classification | Number of Injections | CNV Localization | Overall Lesion Area | Age at First Injection | |
|---|---|---|---|---|---|---|---|
| 6 months | VA | B | 0.06 | −0.05 | −0.04 | 0.01 | 0.01 |
| SE | 0.03 | 0.02 | 0.04 | 0.01 | 0.00 | ||
| p | 0.02 | 0.00 | 0.26 | 0.09 | 0.05 | ||
| VA Change | B | −0.01 | −0.03 | 0.05 | −0.01 | 0.00 | |
| SE | 0.02 | 0.01 | 0.03 | 0.00 | 0.00 | ||
| p | 0.55 | 0.05 | 0.12 | 0.15 | 0.55 | ||
| 12 months | VA | B | 0.07 | −0.06 | −0.03 | 0.01 | 0.01 |
| SE | 0.03 | 0.02 | 0.04 | 0.01 | 0.00 | ||
| p | 0.01 | 0.00 | 0.50 | 0.02 | 0.06 | ||
| VA Change | B | −0.01 | −0.03 | 0.06 | 0.00 | 0.00 | |
| SE | 0.02 | 0.02 | 0.03 | 0.00 | 0.00 | ||
| p | 0.79 | 0.03 | 0.04 | 0.67 | 0.58 | ||
| 24 months | VA | B | 0.06 | −0.07 | −0.02 | 0.02 | 0.01 |
| SE | 0.03 | 0.02 | 0.05 | 0.01 | 0.00 | ||
| p | 0.04 | 0.00 | 0.71 | 0.00 | 0.07 | ||
| VA Change | B | −0.01 | −0.03 | 0.08 | 0.01 | 0.00 | |
| SE | 0.02 | 0.02 | 0.04 | 0.01 | 0.00 | ||
| p | 0.82 | 0.06 | 0.05 | 0.34 | 0.26 | ||
| 36 months | VA | B | 0.09 | −0.09 | 0.02 | 0.01 | - |
| SE | 0.03 | 0.02 | 0.05 | 0.01 | - | ||
| p | 0.00 | <0.001 | 0.65 | 0.05 | - | ||
| VA Change | B | 0.02 | −0.03 | 0.13 | 0.00 | - | |
| SE | 0.03 | 0.02 | 0.05 | 0.01 | - | ||
| p | 0.47 | 0.11 | 0.01 | 0.90 | - | ||
| 48 months | VA | B | 0.11 | −0.11 | 0.01 | 0.00 | - |
| SE | 0.04 | 0.03 | 0.07 | 0.01 | - | ||
| p | 0.01 | 0.00 | 0.87 | 0.89 | - | ||
| VA Change | B | 0.02 | −0.05 | 0.10 | −0.01 | - | |
| SE | 0.04 | 0.03 | 0.07 | 0.01 | - | ||
| p | 0.66 | 0.09 | 0.15 | 0.13 | - |
| p Values | ||||||
|---|---|---|---|---|---|---|
| Time Point | Visual Parameter | Anatomic Classification | Number of Injections | CNV Localization | Overall Lesion Area | Age at First Injection |
| 6 months | VA | 0.043 | 0.016 | 0.812 | 0.564 | 0.496 |
| VA Change | 0.674 | 0.445 | 0.056 | 0.291 | 0.492 | |
| 12 months | VA | 0.048 | 0.050 | 0.859 | 0.627 | 0.294 |
| VA Change | 0.591 | 0.856 | 0.086 | 0.277 | 0.286 | |
| 24 months | VA | 0.024 | 0.026 | 0.976 | 0.609 | 0.193 |
| VA Change | 0.367 | 0.455 | 0.110 | 0.294 | 0.202 | |
| 36 months | VA | 0.021 | 0.010 | 0.504 | 0.769 | - |
| VA Change | 0.874 | 0.271 | 0.020 | 0.211 | - | |
| 48 months | VA | 0.011 | 0.002 | 0.871 | 0.887 | - |
| VA Change | 0.661 | 0.090 | 0.151 | 0.127 | - | |
3.7. Intraocular Pressure and Safety
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Friedman, D.S.; O’Colmain, B.J.; Munoz, B.; Tomany, S.C.; McCarty, C.; de Jong, P.T.; Nemesure, B.; Mitchell, P.; Kempen, J. Eye Diseases Prevalence Research Group. Prevalence of age-related macular degeneration in the United States. Arch. Ophthalmol. 2004, 122, 564–572. [Google Scholar] [PubMed]
- Ferris, F.L., 3rd; Fine, S.L.; Hyman, L. Age-related macular degeneration and blindness due to neovascular maculopathy. Arch. Ophthalmol. 1984, 102, 1640–1642. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeld, P.J.; Brown, D.M.; Heier, J.S.; Boyer, D.S.; Kaiser, P.K.; Chung, C.Y.; Kim, R.Y.; Group, M.S. Ranibizumab for neovascular age-related macular degeneration. N. Engl. J. Med. 2006, 355, 1419–1431. [Google Scholar] [CrossRef] [PubMed]
- Brown, D.M.; Michels, M.; Kaiser, P.K.; Heier, J.S.; Sy, J.P.; Ianchulev, T.; Group, A.S. Ranibizumab versus verteporfin photodynamic therapy for neovascular age-related macular degeneration: Two-year results of the ANCHOR study. Ophthalmology 2009, 116, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Brown, D.M.; Regillo, C.D. Anti-VEGF agents in the treatment of neovascular age-related macular degeneration: Applying clinical trial results to the treatment of everyday patients. Am. J. Ophthalmol. 2007, 144, 627–637. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.Y.; Dubois, L.; Tadayoni, R.; Fajnkuchen, F.; Nghiem-Buffet, S.; Delahaye-Mazza, C.; Guiberteau, B.; Quentel, G. Results of one-year’s treatment with ranibizumab for exudative age-related macular degeneration in a clinical setting. Am. J. Ophthalmol. 2009, 148, 409–413. [Google Scholar] [CrossRef] [PubMed]
- Engelbert, M.; Zweifel, S.A.; Freund, K.B. “Treat and extend” dosing of intravitreal antivascular endothelial growth factor therapy for type 3 neovascularization/retinal angiomatous proliferation. Retina 2009, 29, 1424–1431. [Google Scholar] [CrossRef] [PubMed]
- Freund, K.B.; Korobelnik, J.F.; Devenyi, R.; Framme, C.; Galic, J.; Herbert, E.; Hoerauf, H.; Lanzetta, P.; Michels, S.; Mitchell, P.; et al. Treat-and-extend regimens with anti-VEGF inhibitors in retinal diseases: A consensus. Retina 2014. Submitted. [Google Scholar]
- Comparison of Age-related Macular Degeneration Treatments Trials Research Group; Martin, D.F.; Maguire, M.G.; Fine, S.L.; Ying, G.S.; Jaffe, G.J.; Grunwald, J.E.; Toth, C.; Redford, M.; Ferris, F.L., 3rd. Ranibizumab and bevacizumab for treatment of neovascular age-related macular degeneration: Two-year results. Ophthalmology 2012, 119, 1388–1398. [Google Scholar]
- Lalwani, G.A.; Rosenfeld, P.J.; Fung, A.E.; Dubovy, S.R.; Michels, S.; Feuer, W.; Davis, J.L.; Flynn, H.W., Jr.; Esquiabro, M. A variable-dosing regimen with intravitreal ranibizumab for neovascular age-related macular degeneration: Year 2 of the PrONTO Study. Am. J. Ophthalmol. 2009, 148, 43–58. [Google Scholar] [CrossRef] [PubMed]
- Fung, A.T.; Kumar, N.; Vance, S.K.; Slakter, J.S.; Klancnik, J.M.; Spaide, R.S.; Freund, K.B. Pilot study to evaluate the role of high-dose ranibizumab 2.0 mg in the management of neovascular age-related macular degeneration in patients with persistent/recurrent macular fluid <30 days following treatment with intravitreal anti-VEGF therapy (the LAST Study). Eye (Lond) 2012, 26, 1181–1187. [Google Scholar]
- Toalster, N.; Russell, M.; Ng, P. A 12-month prospective trial of inject and extend regimen for ranibizumab treatment of age-related macular degeneration. Retina 2013, 33, 1351–1358. [Google Scholar] [CrossRef] [PubMed]
- Abedi, F.; Wickremasinghe, S.; Islam, A.F.; Inglis, K.M.; Guymer, R.H. Anti-VEGF treatment in neovascular age-related macular degeneration: A Treat-and-Extend Protocol Over 2 Years. Retina 2014, 34, 1531–1538. [Google Scholar] [CrossRef] [PubMed]
- Gupta, O.P.; Shienbaum, G.; Patel, A.H.; Fecarotta, C.; Kaiser, R.S.; Regillo, C.D. A treat and extend regimen using ranibizumab for neovascular age-related macular degeneration clinical and economic impact. Ophthalmology 2010, 117, 2134–2140. [Google Scholar] [CrossRef] [PubMed]
- Shienbaum, G.; Gupta, O.P.; Fecarotta, C.; Patel, A.H.; Kaiser, R.S.; Regillo, C.D. Bevacizumab for neovascular age-related macular degeneration using a treat-and-extend regimen: Clinical and economic impact. Am. J. Ophthalmol. 2012, 153, 468–473. [Google Scholar] [CrossRef] [PubMed]
- Engelbert, M.; Zweifel, S.A.; Freund, K.B. Long-term follow-up for type 1 (subretinal pigment epithelium) neovascularization using a modified “treat and extend” dosing regimen of intravitreal antivascular endothelial growth factor therapy. Retina 2010, 30, 1368–1375. [Google Scholar] [CrossRef] [PubMed]
- Rayess, N.; Houston, S.K., 3rd; Gupta, O.P.; Ho, A.C.; Regillo, C.D. Treatment outcomes after 3 years in neovascular age-related macular degeneration using a treat-and-extend regimen. Am. J. Ophthalmol. 2015, 159, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Calvo, P.; Wang, Y.; Ferreras, A.; Lam, W.C.; Denevyl, R.; Brent, M.H. Treat and extend versus treat and observe in wet age-related macular degeneration patients treated with ranibizumab: 3-year surveillance period. J. Clin. Exp. Ophthalmol. 2014, 5, 1–5. [Google Scholar]
- Oubraham, H.; Cohen, S.Y.; Samimi, S.; Marotte, D.; Bouzaher, I.; Bonicel, P.; Fajnkuchen, F.; Tadayoni, R. Inject and extend dosing versus dosing as needed: A comparative retrospective study of ranibizumab in exudative age-related macular degeneration. Retina 2011, 31, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Laser photocoagulation of subfoveal neovascular lesions in age-related macular degeneration. Results of a randomized clinical trial. Macular Photocoagulation Study Group. Arch. Ophthalmol. 1991, 109, 1220–1231.
- Grossniklaus, H.E.; Gass, J.D. Clinicopathologic correlations of surgically excised type 1 and type 2 submacular choroidal neovascular membranes. Am. J. Ophthalmol. 1998, 126, 59–69. [Google Scholar] [CrossRef]
- Freund, K.B.; Zweifel, S.A.; Engelbert, M. Do we need a new classification for choroidal neovascularization in age-related macular degeneration? Retina 2010, 30, 1333–1349. [Google Scholar] [CrossRef] [PubMed]
- Jung, J.J.; Chen, C.Y.; Mrejen, S.; Gallego-Pinazo, R.; Xu, L.; Marsiglia, M.; Boddu, S.; Freund, K.B. The Incidence of Neovascular Subtypes in Newly Diagnosed Neovascular Age-Related Macular Degeneration. Am. J. Ophthalmol. 2014, 158, 769–779. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Mrejen, S.; Jung, J.J.; Gallego-Pinazo, R.; Thompson, D.; Marsiglia, M.; Freund, K.B. Geographic Atrophy in Patients Receiving Anti-Vascular Endothelial Growth Factor for Neovascular Age-Related Macular Degeneration. Retina 2014, 35, 176–186. [Google Scholar] [CrossRef] [PubMed]
- Yannuzzi, L.A.; Negrao, S.; Iida, T.; Carvalho, C.; Rodriguez-Coleman, H.; Slakter, J.; Freund, K.B.; Sorenson, J.; Orlock, D.; Borodoker, N. Retinal angiomatous proliferation in age-related macular degeneration. Retina 2001, 21, 416–434. [Google Scholar] [CrossRef] [PubMed]
- Rofagha, S.; Bhisitkul, R.B.; Boyer, D.S.; Sadda, S.R.; Zhang, K.; SEVEN-UP Study Group. Seven-year outcomes in ranibizumab-treated patients in ANCHOR, MARINA, and HORIZON: A multicenter cohort study (SEVEN-UP). Ophthalmology 2013, 120, 2292–2299. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.A.; Awh, C.C.; Sadda, S.; Freeman, W.R.; Antoszyk, A.N.; Wong, P.; Tuomi, L. HORIZON: An open-label extension trial of ranibizumab for choroidal neovascularization secondary to age-related macular degeneration. Ophthalmology 2012, 119, 1175–1183. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, A.; Bloch, S.B.; Fuchs, J.; Hansen, L.H.; Larsen, M.; Lacour, M.; Lund-Andersen, H.; Sander, B. A 4-year longitudinal study of 555 patients treated with ranibizumab for neovascular age-related macular degeneration. Ophthalmology 2013, 120, 2630–2636. [Google Scholar] [CrossRef] [PubMed]
- Silva, R.; Axer-Siegel, R.; Eldem, B.; Guymer, R.; Kirchhof, B.; Papp, A.; Seres, A.; Gekkieva, M.; Nieweg, A.; Pilz, S.; et al. The SECURE study: Long-term safety of ranibizumab 0.5 mg in neovascular age-related macular degeneration. Ophthalmology 2013, 120, 130–139. [Google Scholar] [CrossRef] [PubMed]
- Marcus, D.M. Long-Term Follow-up of Intravitreal Injection for Neovascular Age-Related Macular Degeneration in an Open-Label Extension of the VIEW 1 Study. Abstract presented at: the Association for Research in Vision and Ophthalmology (ARVO) Annual Meeting. Orlando, FL, USA, 4–8 May, 2014.
- Shah, V.P.; Freund, K.B. Growth of type 1 neovascularization following cessation of anti-vascular endothelial growth factor therapy as a possible explanation for treatment resistance. JAMA Ophthalmol. 2013, 131, 967–969. [Google Scholar] [CrossRef] [PubMed]
- Grunwald, J.E.; Daniel, E.; Huang, J.; Ying, G.S.; Maguire, M.G.; Toth, C.A.; Jaffe, G.J.; Fine, S.L.; Blodi, B.; Klein, M.L.; et al. Risk of geographic atrophy in the comparison of age-related macular degeneration treatments trials. Ophthalmology 2014, 121, 150–161. [Google Scholar] [CrossRef] [PubMed]
- McBain, V.A.; Kumari, R.; Townend, J.; Lois, N. Geographic atrophy in retinal angiomatous proliferation. Retina 2011, 31, 1043–1052. [Google Scholar] [CrossRef] [PubMed]
- Marsiglia, M.; Boddu, S.; Chen, C.Y.; Jung, J.J.; Mrejen, S.; Gallego-Pinazo, R.; Freund, K.B. Correlation between neovascular lesion type and the clinical characteristics of non-neovascular fellow eyes in patients with unilateral neovascular age-related macular degeneration. Retina 2015, 35, 966–974. [Google Scholar] [PubMed]
- Daniel, E.; Toth, C.A.; Grunwald, J.E.; Jaffe, G.J.; Martin, D.F.; Fine, S.L.; Huang, J.; Ying, G.S.; Hagstrom, S.A.; Winter, K.; et al. Risk of scar in the comparison of age-related macular degeneration treatments trials. Ophthalmology 2014, 121, 656–666. [Google Scholar] [CrossRef] [PubMed]
- Green, W.R. Histopathology of age-related macular degeneration. Mol. Vis. 1999, 5, 27. [Google Scholar] [PubMed]
- Grossniklaus, H.E.; Green, W.R. Choroidal neovascularization. Am. J. Ophthalmol. 2004, 137, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Bhavsar, K.V.; Freund, K.B. Retention of good visual acuity in eyes with neovascular age-related macular degeneration and chronic refractory subfoveal subretinal fluid. Saudi J. Ophthalmol. 2014, 28, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.Y.; Creuzot-Garcher, C.; Darmon, J.; Desmettre, T.; Korobelnik, J.F.; Levrat, F.; Quentel, G.; Palies, S.; Sanchez, A.; de Gendre, A.S.; et al. Types of choroidal neovascularisation in newly diagnosed exudative age-related macular degeneration. Br. J. Ophthalmol. 2007, 91, 1173–1176. [Google Scholar] [CrossRef] [PubMed]
- Hoang, Q.V.; Tsuang, A.J.; Gelman, R.; Mendonca, L.S.; Della Torre, K.E.; Jung, J.J.; Freund, K.B. Clinical predictors of sustained intraocular pressure elevation due to intravitreal anti-vascular endothelial growth factor therapy. Retina 2013, 33, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Hoang, Q.V.; Mendonca, L.S.; Della Torre, K.E.; Jung, J.J.; Tsuang, A.J.; Freund, K.B. Effect on intraocular pressure in patients receiving unilateral intravitreal anti-vascular endothelial growth factor injections. Ophthalmology 2012, 119, 321–326. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mrejen, S.; Jung, J.J.; Chen, C.; Patel, S.N.; Gallego-Pinazo, R.; Yannuzzi, N.; Xu, L.; Marsiglia, M.; Boddu, S.; Freund, K.B. Long-Term Visual Outcomes for a Treat and Extend Anti-Vascular Endothelial Growth Factor Regimen in Eyes with Neovascular Age-Related Macular Degeneration. J. Clin. Med. 2015, 4, 1380-1402. https://doi.org/10.3390/jcm4071380
Mrejen S, Jung JJ, Chen C, Patel SN, Gallego-Pinazo R, Yannuzzi N, Xu L, Marsiglia M, Boddu S, Freund KB. Long-Term Visual Outcomes for a Treat and Extend Anti-Vascular Endothelial Growth Factor Regimen in Eyes with Neovascular Age-Related Macular Degeneration. Journal of Clinical Medicine. 2015; 4(7):1380-1402. https://doi.org/10.3390/jcm4071380
Chicago/Turabian StyleMrejen, Sarah, Jesse J. Jung, Christine Chen, Samir N. Patel, Roberto Gallego-Pinazo, Nicolas Yannuzzi, Luna Xu, Marcela Marsiglia, Sucharita Boddu, and K. Bailey Freund. 2015. "Long-Term Visual Outcomes for a Treat and Extend Anti-Vascular Endothelial Growth Factor Regimen in Eyes with Neovascular Age-Related Macular Degeneration" Journal of Clinical Medicine 4, no. 7: 1380-1402. https://doi.org/10.3390/jcm4071380
APA StyleMrejen, S., Jung, J. J., Chen, C., Patel, S. N., Gallego-Pinazo, R., Yannuzzi, N., Xu, L., Marsiglia, M., Boddu, S., & Freund, K. B. (2015). Long-Term Visual Outcomes for a Treat and Extend Anti-Vascular Endothelial Growth Factor Regimen in Eyes with Neovascular Age-Related Macular Degeneration. Journal of Clinical Medicine, 4(7), 1380-1402. https://doi.org/10.3390/jcm4071380