Evolution of ST-Elevation Acute Myocardial Infarction Prevalence by Gender Assessed Age Pyramid Analysis—The Piramyd Study

 , ,
, ,
Abstract
:1. Introduction
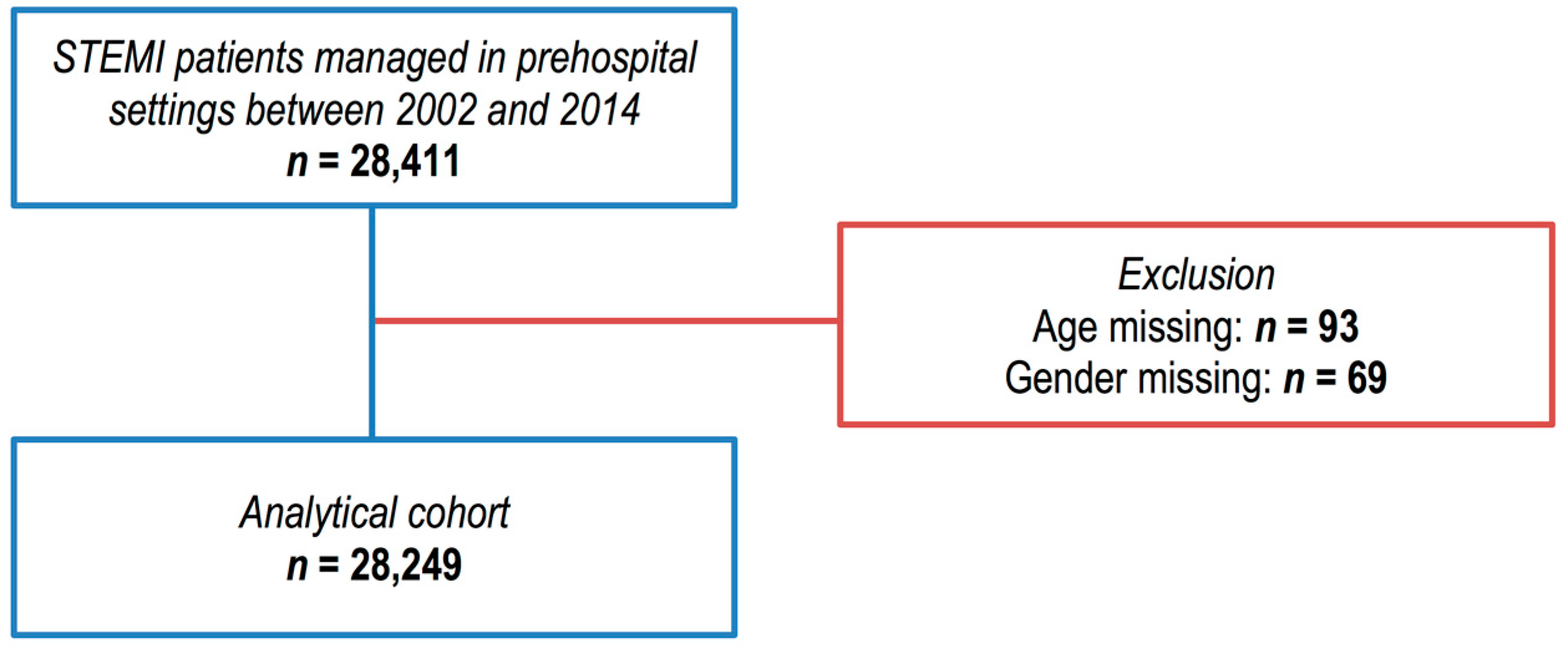
2. Methods
2.1. Settings
2.2. E-MUST Registry
2.3. Study Design, Data Extraction and Statistical Analysis
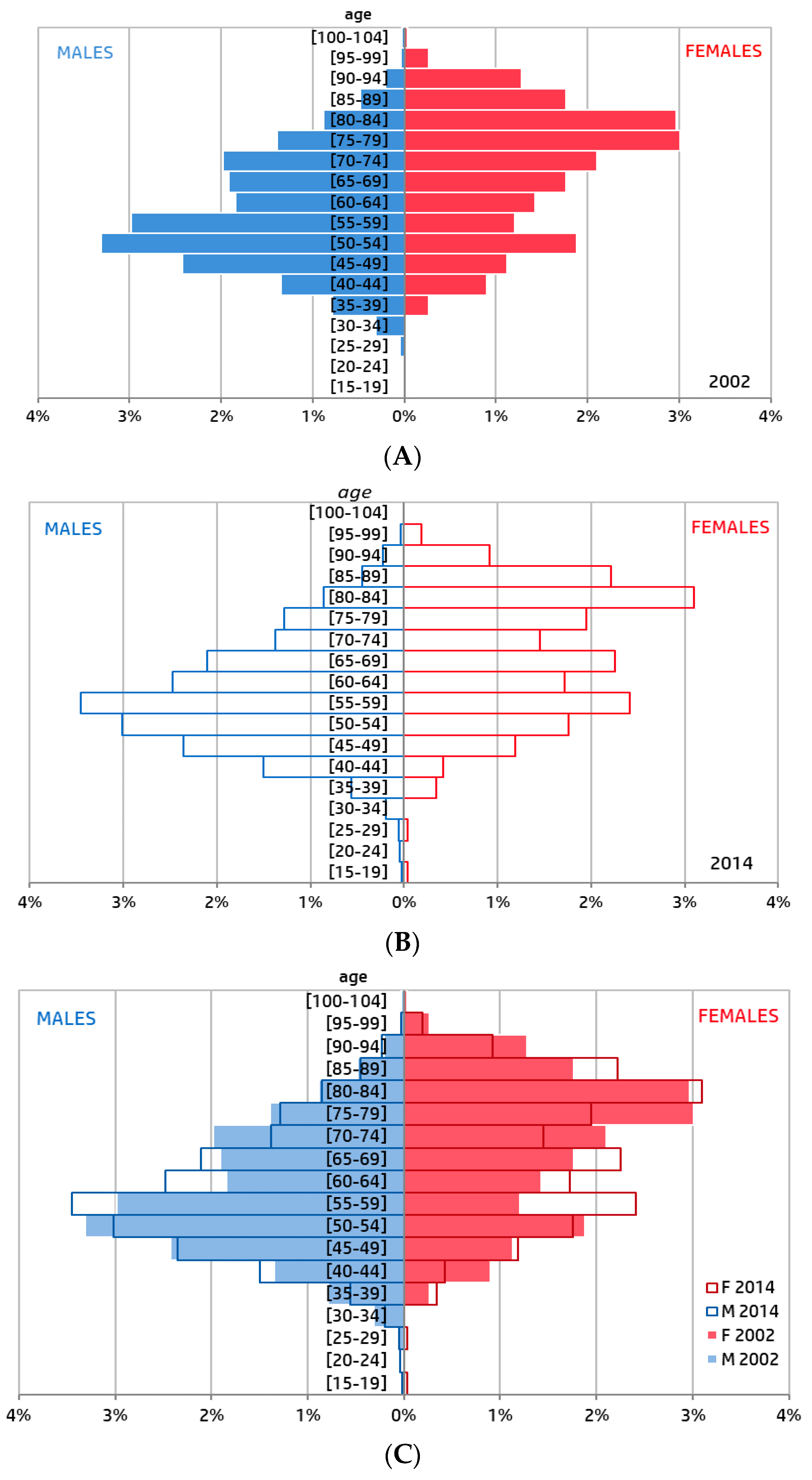
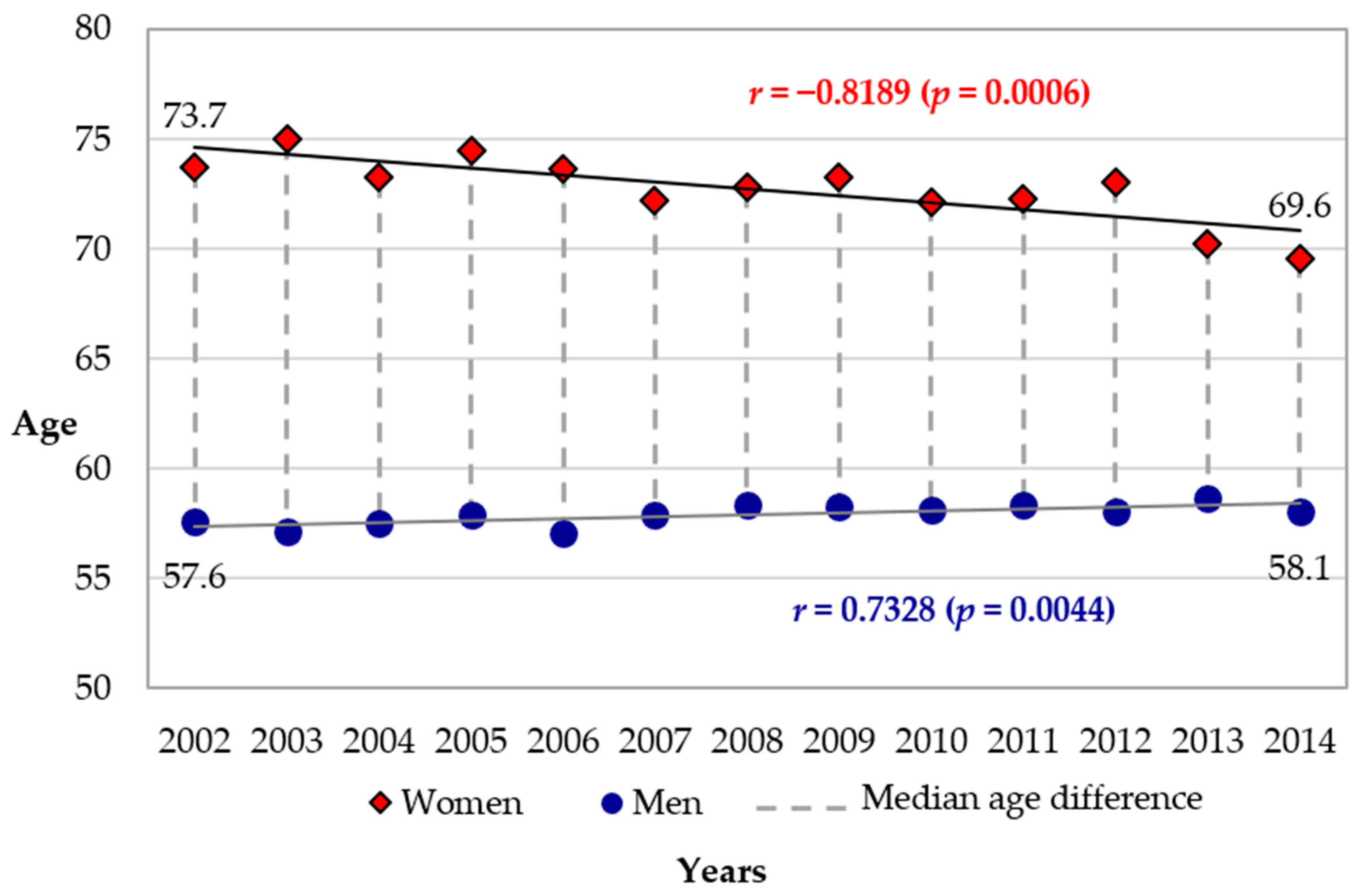
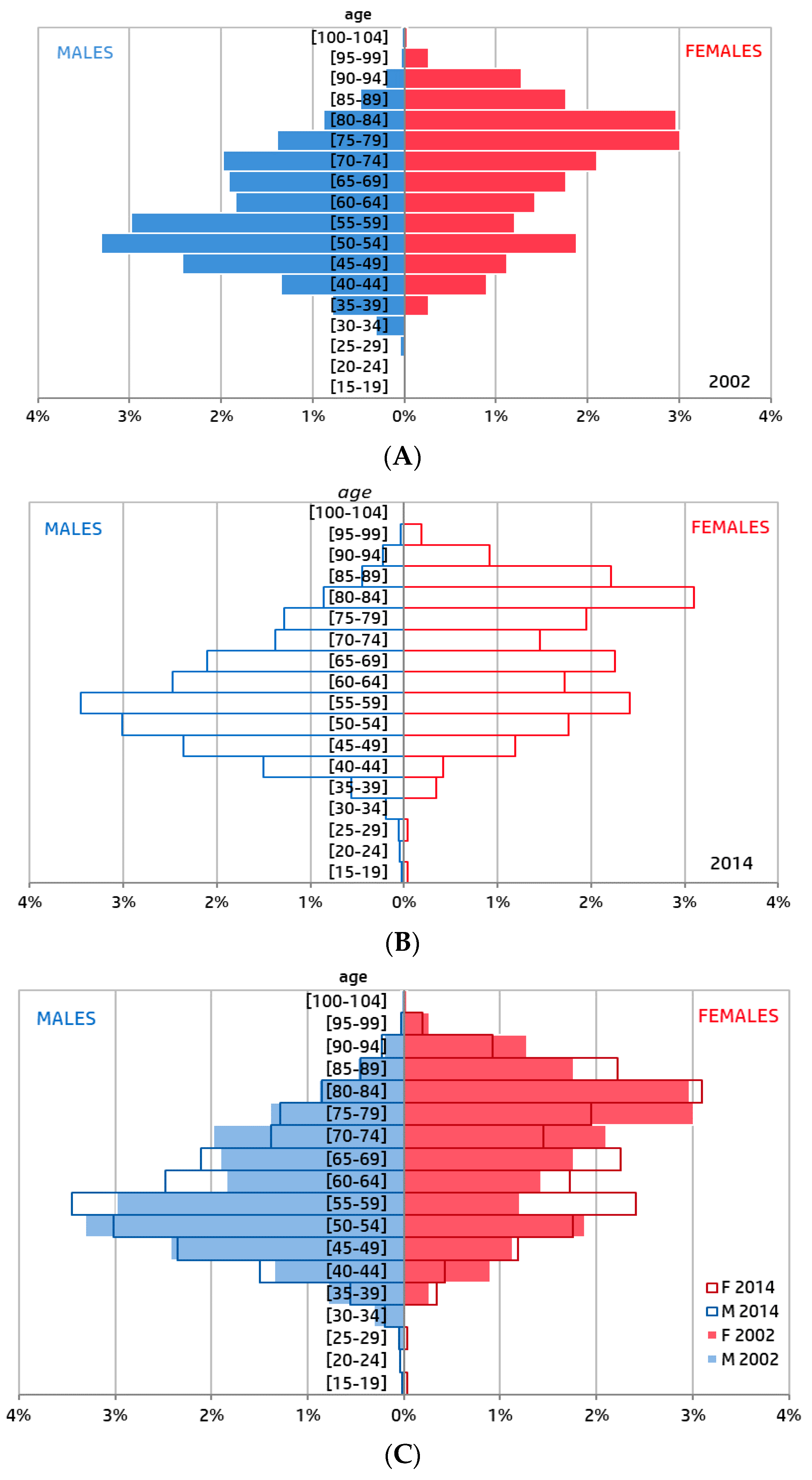
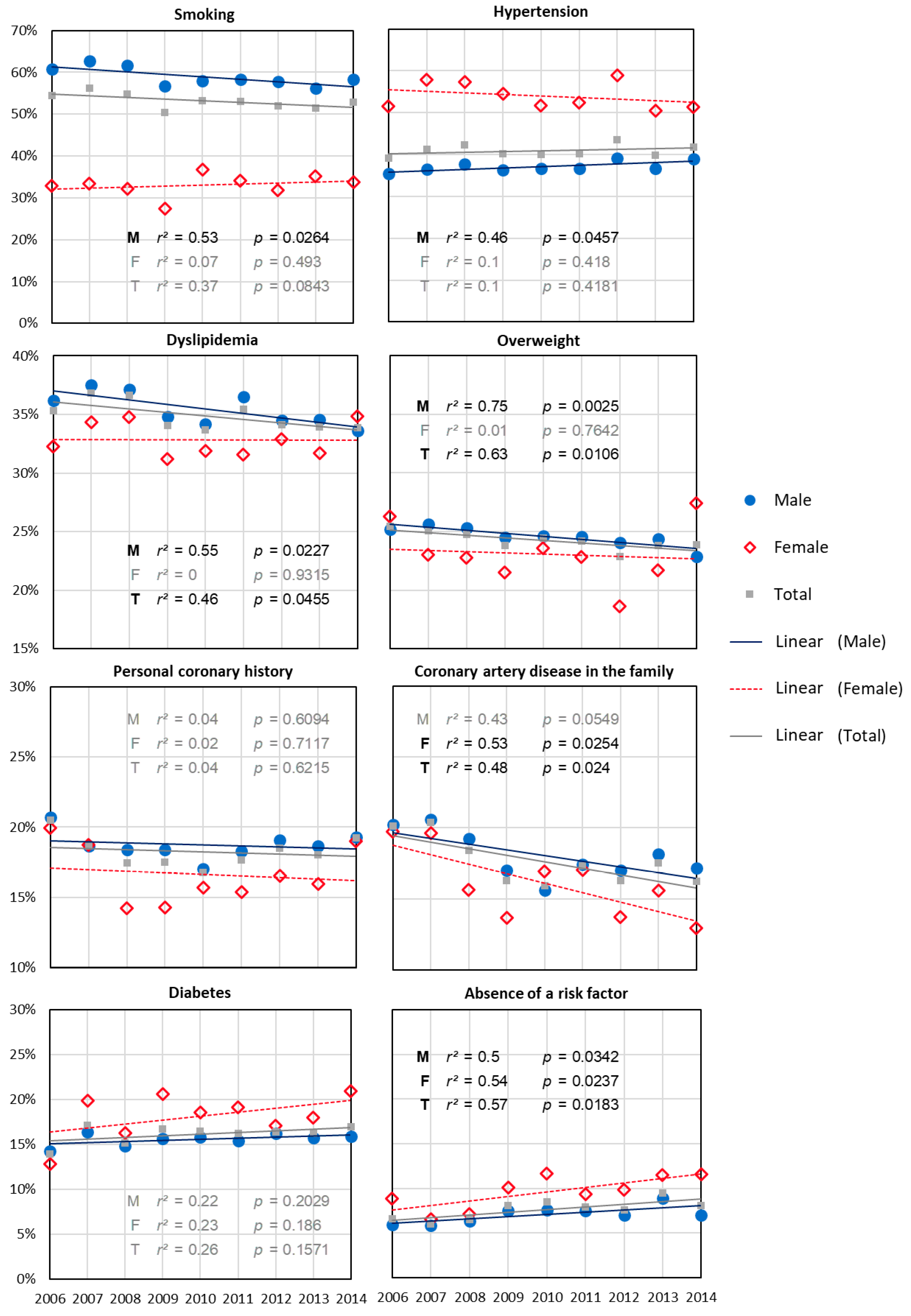
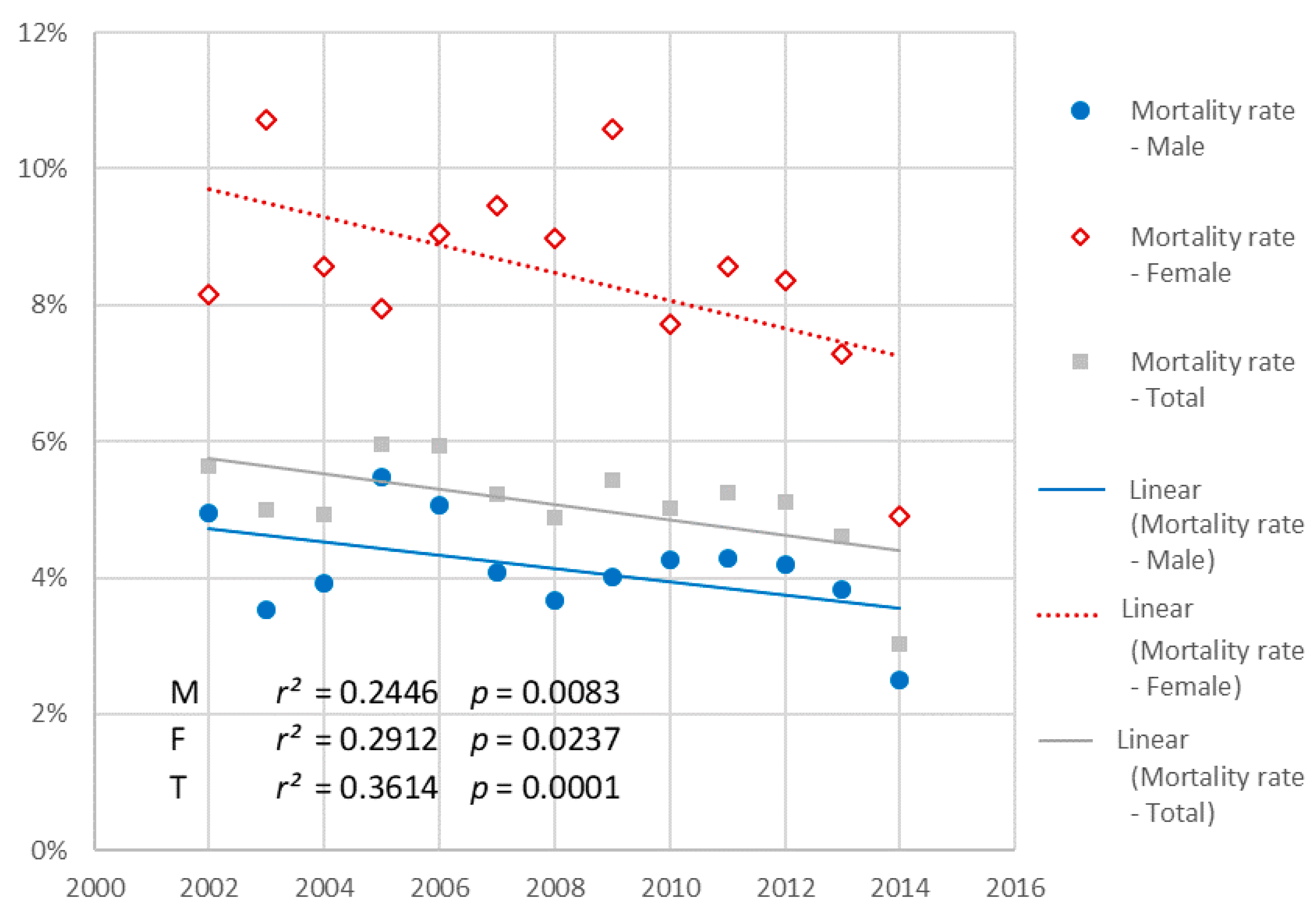
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gerber, Y.; Weston, S.A.; Jiang, R.; Roger, V.L. The changing epidemiology of myocardial infarction in Olmsted County, Minnesota, 1995–2012. Am. J. Med. 2015, 128, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Dégano, I.R.; Salomaa, V.; Veronesi, G.; Ferriéres, J.; Kirchberger, I.; Laks, T.; Havulinna, A.S.; Ruidavets, J.B.; Ferrario, M.M.; Meisinger, C.; et al. Twenty-five-year trends in myocardial infarction attack and mortality rates, and case-fatality, in six European populations. Heart 2015, 101, 1413–1421. [Google Scholar] [CrossRef] [PubMed]
- Puymirat, E.; Simon, T.; Steg, P.G.; Schiele, F.; Guéret, P.; Blanchard, D.; Khalife, K.; Goldstein, P.; Cattan, S.; Vaur, L.; et al. Association of changes in clinical characteristics and management with improvement in survival among patients with ST-elevation myocardial infarction. JAMA 2012, 308, 998–1006. [Google Scholar] [CrossRef] [PubMed]
- Chockalingam, A.; Campbell, N.R.; Fodor, J.G. Worldwide Epidemic of Hypertension. Available online: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2560860/ (accessed on 28 June 2017).
- Galka, M. How the World Got Fat: A Visualisation of Global Obesity over 40 Years. Available online: http://www.theguardian.com/global-development-professionals-network/2017/jan/03/using-data-visualisations-to-help-explain-the-global-obesity-explosion (accessed on 28 June 2017).
- Global Report on Diabetes. Available online: http://www.who.int/diabetes/global-report/en/ (accessed on 28 June 2017).
- Gupta, A.; Wang, Y.; Spertus, J.A.; Geda, M.; Lorenze, N.; Nkonde-Price, C.; D’Onofrio, G.; Lichtman, J.H.; Krumholz, H.M. Trends in acute myocardial infarction in young patients and differences by sex and race, 2001 to 2010. J. Am. Coll. Cardiol. 2014, 64, 337–345. [Google Scholar] [CrossRef] [PubMed]
- Guignard, R.; Beck, F.; Wilquin, J.-L.; Andler, R.; Nguyen-Thanh, V.; Richard, J.-B.; Arwidson, P. La consommation de tabac en France et son évolution: Résultats du Baromètre santé 2014. BEH. 2015, 17–18, 281–288. (In French) [Google Scholar]
- Marques-Vidal, P.; Cambou, J.P.; Ferrières, J.; Thomas, D.; Grenier, O.; Cantet, C.; Danchin, N.; Prevenir, E. Distribution and treatment of cardiovascular risk factors in coronary patients: The prevenir Study. Arch. Mal. Coeur. Vaiss. 2001, 94, 673–680. [Google Scholar] [PubMed]
- Available online: http://www.bmj.com/about-bmj/resources-readers/publications/statistics-square-one/11-correlation-and-regression (accessed on 14 January 2018).
- Yusuf, S.; Hawken, S.; Ounpuu, S.; Dans, T.; Avezum, A.; Lanas, F.; McQueen, M.; Budaj, A.; Pais, P.; Varigos, J.; et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): Case-control study. Lancet Lond. Engl. 2004, 364, 937–952. [Google Scholar] [CrossRef]
- Vaccarino, V.; Parsons, L.; Every, N.R.; Barron, H.V.; Krumholz, H.M. Sex-based differences in early mortality after myocardial infarction. N. Engl. J. Med. 1999, 341, 217–225. [Google Scholar] [CrossRef]
- Benamer, H.; Tafflet, M.; Bataille, S.; Escolano, S.; Livarek, B.; Fourchard, V.; Caussin, C.; Teiger, E.; Garot, P.; Lambert, Y.; et al. Female gender is an independent predictor of in-hospital mortality after STEMI in the era of primary PCI: Insights from the greater Paris area PCI Registry. EuroIntervention 2011, 6, 1073–1079. [Google Scholar] [CrossRef]
- Sederholm Lawesson, S.; Isaksson, R.-M.; Thylén, I.; Ericsson, M.; Ängerud, K.; Swahn, E.; SymTime Study Group. Gender differences in symptom presentation of ST-elevation myocardial infarction—An observational multicenter survey study. Int. J. Cardiol. 2018, 264, 7–11. [Google Scholar] [CrossRef]
- Alabas, O.A.; Gale, C.P.; Hall, M.; Rutherford, M.J.; Szummer, K.; Lawesson, S.S.; Alfredsson, J.; Lindahl, B.; Jernberg, T. Sex differences in treatments, relative survival, and excess mortality following acute myocardial infarction: National cohort study using the SWEDEHEART registry. J. Am. Heart Assoc. 2017, 6. [Google Scholar] [CrossRef] [PubMed]
- Potts, J.; Sirker, A.; Martinez, S.C.; Gulati, M.; Alasnag, M.; Rashid, M.; Kwok, C.S.; Ensor, J.; Burke, D.L.; Riley, R.D.; et al. Persistent sex disparities in clinical outcomes with percutaneous coronary intervention: Insights from 6.6 million PCI procedures in the United States. PLoS ONE 2018. [Google Scholar] [CrossRef] [PubMed]
- Cenko, E.; Yoon, J.; Kedev, S.; Stankovic, G.; Vasiljevic, Z.; Krljanac, G.; Kalpak, O.; Ricci, B.; Milicic, D.; Manfrini, O.; et al. Sex differences in outcomes after STEMI: Effect modification by treatment strategy and age. JAMA Intern. Med. 2018, 178, 632–639. [Google Scholar] [CrossRef] [PubMed]
- Mendelsohn, M.E.; Karas, R.H. The protective effects of estrogen on the cardiovascular system. N. Engl. J. Med. 1999, 340, 1801–1811. [Google Scholar] [CrossRef] [PubMed]
- Johansson, S.; Bergstrand, R.; Ulvenstam, G.; Vedin, A.; Wilhelmsson, C.; Wedel, H.; Wilhelmsen, L.; Aberg, A. Sex differences in preinfarction characteristics and longterm survival among patients with myocardial infarction. Am. J. Epidemiol. 1984, 119, 610–623. [Google Scholar] [CrossRef] [PubMed]
- Albrektsen, G.; Heuch, I.; Løchen, M.-L.; Thelle, D.S.; Wilsgaard, T.; Njølstad, I.; Bønaa, K.H. Lifelong gender gap in risk of incident myocardial infarction: The Tromsø study. JAMA Intern. Med. 2016, 176, 1673–1679. [Google Scholar] [CrossRef] [PubMed]
- Johannes, J.; Bairey Merz, C.N. Is cardiovascular disease in women inevitable?: Preparing for menopause and beyond. Cardiol. Rev. 2011, 19, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Arbustini, E.; Dal Bello, B.; Morbini, P.; Burke, A.P.; Bocciarelli, M.; Specchia, G.; Virmanic, R. Plaque erosion is a major substrate for coronary thrombosis in acute myocardial infarction. Heart Br. Card. Soc. 1999, 82, 269–272. [Google Scholar] [CrossRef] [Green Version]
- Vanzetto, G.; Berger-Coz, E.; Barone-Rochette, G.; Chavanon, O.; Bouvaist, H.; Hacini, R.; Blin, D.; Machecourt, J. Prevalence, therapeutic management and medium-term prognosis of spontaneous coronary artery dissection: Results from a database of 11,605 patients. Eur. J. Cardiothorac. Surg. 2009, 35, 250–254. [Google Scholar] [CrossRef]
- Gleerup, H.B.; Dahm, C.C.; Thim, T.; Jensen, S.E.; Jensen, L.O.; Kristensen, S.D.; Bøtker, H.E.; Maeng, M. Smoking is the dominating modifiable risk factor in younger patients with STEMI. Eur. Heart J. Acute Cardiovasc. Care 2018. [Google Scholar] [CrossRef]
- Coutinho, T. Arterial stiffness and its clinical implications in women. Can. J. Cardiol. 2014, 30, 756–764. [Google Scholar] [CrossRef] [PubMed]
- Gebhard, C.; Gebhard, C.E.; Stähli, B.E.; Maafi, F.; Bertrand, M.-J.; Wildi, K.; Fortier, A.; Galvan Onandia, Z.; Toma, A.; Zhang, Z.W.; et al. Weather and risk of ST-elevation myocardial infarction revisited: Impact on young women. PLoS ONE 2018, 13. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, L.R.; Frestad, D.; Michelsen, M.M.; Mygind, N.D.; Rasmusen, H.; Suhrs, H.E.; Eva, P. Risk factors for myocardial infarction in women and men: A review of the current literature. Curr. Pharm. Des. 2016, 22, 3835–3852. [Google Scholar] [CrossRef] [PubMed]
- Reimold, S.C.; Hill, J.A. inaugural go red for women issue. Circulation 2017, 135, 493–494. [Google Scholar] [CrossRef] [PubMed]
- Mehta, L.S.; Beckie, T.M.; DeVon, H.A.; Grines, C.L.; Krumholz, H.M.; Johnson, M.N.; Lindley, K.J.; Vaccarino, V.; Wang, T.Y.; Watson, K.E.; et al. Acute myocardial infarction in women: A scientific statement from the american heart association. Circulation 2016, 133, 916–947. [Google Scholar] [CrossRef] [PubMed]
- Huded, C.P.; Johnson, M.; Kravitz, K.; Menon, V.; Abdallah, M.; Gullett, T.C.; Hantz, S.; Ellis, S.G.; Podolsky, S.R.; Meldon, S.W.; et al. 4-Step protocol for disparities in STEMI care and outcomes in women. J. Am. Coll. Cardiol. 2018, 71, 2122–2132. [Google Scholar] [CrossRef] [PubMed]
- Abbott, J.D.; Curtis, J.P. More than one way to close the gender gap. J. Am. Coll. Cardiol. 2018, 71, 2133–2135. [Google Scholar] [CrossRef] [PubMed]
- Langabeer, J.R.; Champagne-Langabeer, T.; Fowler, R.; Henry, T. Gender-based outcome differences for emergency department presentation ofnon-STEMI acute coronary syndrome. Am. J. Emerg. Med. 2018. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n | Men | Women | p-Value (khi2 Test) | |
|---|---|---|---|---|
| Personal coronary history | 19,077 | 2772 (19%) | 709 (17%) | 0.0015 |
| Family coronary artery disease | 19,076 | 2664 (18%) | 681 (16%) | 0.0019 |
| Smoking | 19,018 | 8686 (59%) | 1406 (33%) | <0.0001 |
| Diabetes | 19,076 | 2309 (16%) | 777 (18%) | <0.0001 |
| Hypertension | 19,078 | 5507 (37%) | 2306 (54%) | <0.0001 |
| Dyslipidemia | 19,079 | 5242 (35%) | 1404 (33%) | 0.0021 |
| Excess weight | 19,082 | 3633 (25%) | 982 (23%) | 0.0388 |
| Absence of risk factor | 19,076 | 1054 (7%) | 413 (10%) | <0.0001 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Loyeau, A.; Benamer, H.; Bataille, S.; Tepper, S.; Boche, T.; Lamhaut, L.; Pirès, V.; Simon, B.; Dupas, F.; Weisslinger, L.; et al. Evolution of ST-Elevation Acute Myocardial Infarction Prevalence by Gender Assessed Age Pyramid Analysis—The Piramyd Study. J. Clin. Med. 2018, 7, 509. https://doi.org/10.3390/jcm7120509
Loyeau A, Benamer H, Bataille S, Tepper S, Boche T, Lamhaut L, Pirès V, Simon B, Dupas F, Weisslinger L, et al. Evolution of ST-Elevation Acute Myocardial Infarction Prevalence by Gender Assessed Age Pyramid Analysis—The Piramyd Study. Journal of Clinical Medicine. 2018; 7(12):509. https://doi.org/10.3390/jcm7120509
Chicago/Turabian StyleLoyeau, Aurélie, Hakim Benamer, Sophie Bataille, Sarah Tepper, Thévy Boche, Lionel Lamhaut, Virginie Pirès, Benoit Simon, François Dupas, Lisa Weisslinger, and et al. 2018. "Evolution of ST-Elevation Acute Myocardial Infarction Prevalence by Gender Assessed Age Pyramid Analysis—The Piramyd Study" Journal of Clinical Medicine 7, no. 12: 509. https://doi.org/10.3390/jcm7120509