Examining the Association and Directionality between Mental Health Disorders and Substance Use among Adolescents and Young Adults in the U.S. and Canada—A Systematic Review and Meta-Analysis


Abstract
:1. Background
2. Methods
2.1. Data Sources
2.2. Eligibility Criteria, Data Extraction and Analysis
2.3. Definitions of Mental Health Disorders and Substance Use
2.4. Quality Assessment
2.5. Meta-Analysis
3. Results
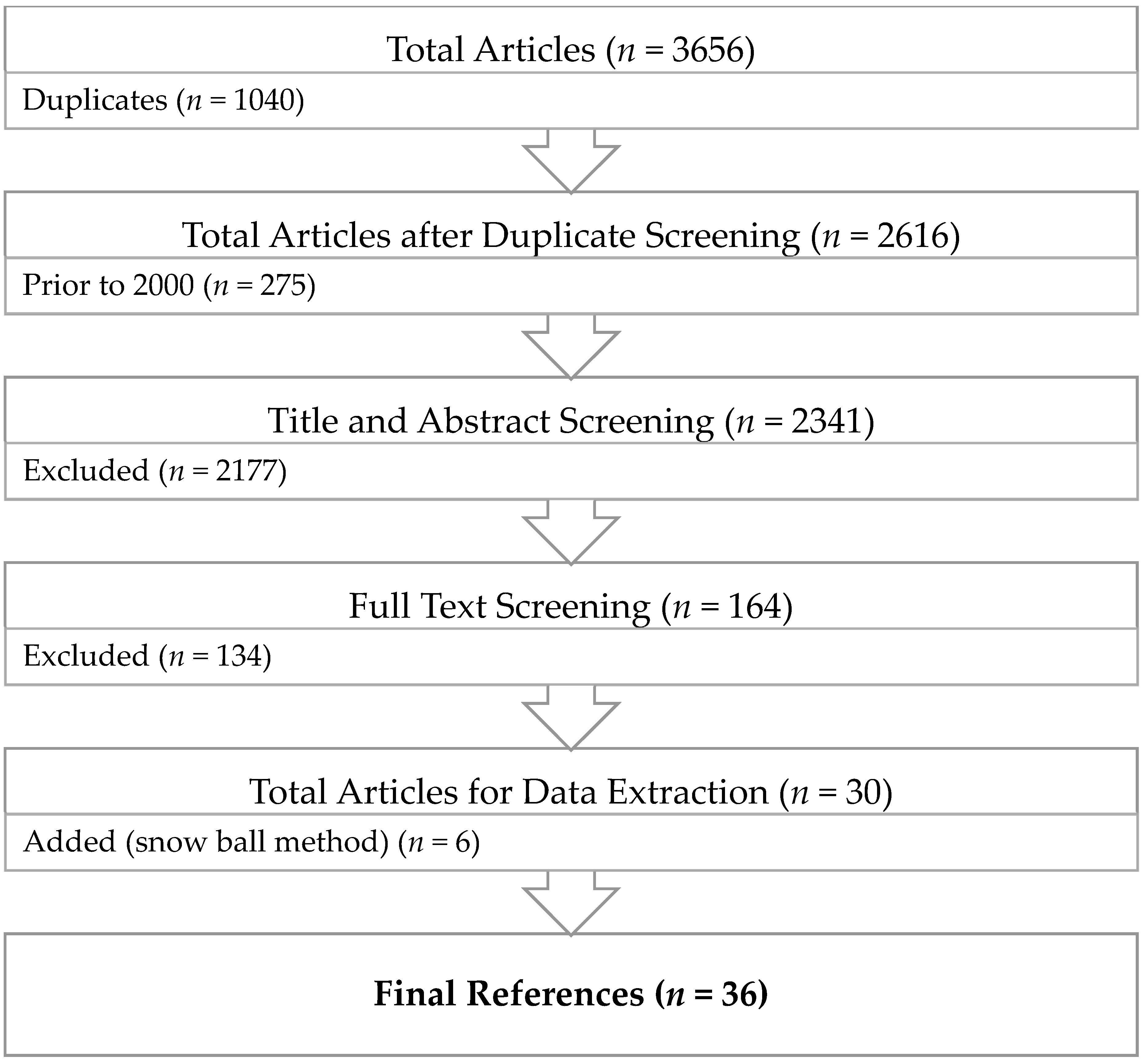
3.1. Study Selection and Characteristics
3.2. Synthesis of Results
3.3. Analysis of the Directionality
3.4. Subgroup Analysis
3.5. Publication Bias
4. Discussion
4.1. Strengths and Limitations
4.2. Implications for Practice, Research and Policy
- (1)
- Practice: our study helps highlight the importance of addressing adolescents and young adults’ mental health (depression/anxiety) and substance use behaviors (drinking, smoking, cannabis use) early, concurrently and with an integrated clinical approach through the use of timely screening, team-based diagnosis, patient-oriented treatment and effective interventions. These observations underscore the need for a shift in our collective perspective, when implementing integrated services for patients with co-occurring disorders.
- (2)
- Research: our findings corroborate and expand those reported in previous studies and provide invaluable insight and guidance to future rigorous, longitudinal research that aims to widen our knowledge of psychopathology by elucidating the associated links and delineating best practices in the prevention, diagnosis, and treatment of co-occurring mental health disorders and substance use. Additionally, it will be of keen scientific interest to investigate and determine whether substance use cessation treatments lead to reduction and/or remission of depression/anxiety or whether the treatment of depression/anxiety leads to reduction and/or cessation of substance use among adolescents and young adults.
- (3)
- Policy: our results demonstrate that integrated treatment approaches and health education campaigns are needed to improve quality of care and increase awareness among the public and healthcare practitioners of the associations between depression/anxiety and substance use among adolescents and young adults. School-based intervention programs, in particular, hold much promise as they could encourage adolescents and young adults to seek professional help safely and in a supportive environment.
4.3. Recommendations
- (1)
- Bilateral cooperation between the U.S. and Canada: along with sharing the longest international boarder, the two countries share many common socio-cultural factors, demonstrate similar patterns in the prevalence of mental health disorders and substance use, and report common health priorities (i.e., advancement of mental health and substance use services) [76,77]. Therefore, it would be beneficial for key stakeholders at educational settings in both the U.S. and Canada to collaborate and exchange information and ideas on how to further improve their health education and promotion programs.
- (2)
- Implementation of the quadrants of care model (the New York Model): in our systematic review, it became apparent that as the severity of mental health disorders and intensity of substance use varied, different approaches to their healthcare management were needed. Thus, the potential usefulness of the quadrants of care model to most appropriately direct the efforts of healthcare professionals [78]. Individuals treated simultaneously by two or more healthcare providers at one point of entry may receive an integrated treatment plan for both conditions. By following this model, individuals will receive an appropriate level of care based on their needs, and this will ensure the efficient use of available resources.
- (3)
- Reforming the healthcare system: healthcare reforms are needed to make the necessary changes from the current parallel and independent practice sectors towards coordinated systems of care. Coordinated practice sectors will require sharing funds, developing mandates in concert, and treating affected individuals collaboratively. Reforms should be broad and encompass all levels of service delivery including health promotion and prevention, diagnosis, treatment, and research.
- (4)
- Efficient use of limited resources: preventive interventions, early detection, diagnosis, and treatment of the co-occurrence of mental health disorders and substance use, can improve the quality of life of adolescents and young adults. Addressing this issue upstream will reduce the associated healthcare costs and permit the efficient use of limited resources, including the need for frequent psychiatric hospitalizations, over-use of emergency departments, and ambulatory care.
- (5)
- Training of healthcare providers: it is essential to cross-train healthcare providers from different sectors to increase their awareness of the existing association between mental health disorders and substance use. There is a need for the characterization of patient risk profiles, the use of valid assessment tools, and updated diagnostic and treatment guidelines to help improve outcomes for these two conditions among adolescents and young adults.
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. Definitions of Mental Health Disorders and Substance Use
| Depression |
| The center for epidemiologic studies depression scale (CES-D) [27,33,37,38,39,40,41,42,43,44,45] |
| Beck depression inventory-II (BDI-II) [32] |
| One item question: Whether respondents felt so sad or hopeless almost daily for two consecutive weeks that usual activities were interrupted [25] |
| Youth self-report checklist (8 self-reported symptoms of depression within the past 6 months): I feel guilty, I cry a lot, I deliberately try to hurt myself, I think of killing myself, I feel lonely, I am unhappy, I feel that no one loves me, and I feel worthless (YSR) [46] |
| A five-item question: within the past 12 months how often have you felt too tired to do things? Felt unhappy, sad, or depressed? Felt hopeless about the future? Felt nervous or tense? And worried too much about things? [47] |
| Modified version of the children depression inventory (CDI) [48] |
| Depression medication prescribed by a doctor or a nurse in the last 12 months [28] |
| National institute of mental health diagnostic interview schedule for children version IV (NIMH-DISC, version IV): A structured diagnostic interview administered by lay interviewers to assess diagnostic criteria for mental disorders in children and adolescents, in accordance with the diagnostic and statistical manual of mental disorders, fourth edition (DSM-IV) [49] |
| CIDI-SF: 12-month prevalence of major depressive disorder (MDD), based on the Composite International Diagnostic Interview–Short Form [50,51] |
| The university of Michigan composite international diagnostic interview (CIDI): A highly structured research diagnostic instrument developed for use by trained lay interviewers to assess the most common diagnoses among children, adolescents, and young adults as described in the DSM-III-R [52,53] |
| A 6-item question: During the past 3-month how often you have felt too tired to do things; had trouble going to sleep or staying asleep; felt unhappy, sad or depressed; felt hopeless about the future; felt nervous or tense; worried too much about things [54] |
| Major depressive episode diagnosis: self-reported depression diagnosed by a medical professional with the past year [26] |
| The short-form (36) health survey (SF-36) [55] |
| Mental health component of national health and nutrition examination survey (NHANES), assess diagnostic criteria for mental disorders in children and adolescents, in accordance with the diagnostic and statistical manual of mental disorders, third edition (DSM-III) [31,56] |
| Anxiety |
| Social interaction anxiety scale (SIAS) [29,30,57,58] |
| Diagnostic interview schedule for children, version IV (DISC-IV) [26,35,59] |
| Primary care evaluation of mental disorders (PRIME-MD) [36] |
| Schedule for affective disorders and schizophrenia for school-age children (K-SADS) [34,60] |
| Anxiety medication prescribed by a doctor or a nurse in the last 12 months [28] |
| National Institute of Mental Health Diagnostic Interview for children (NIMHD) [49] |
| Alcohol |
| Ever drinkers: Drinking at least once within a lifetime [52] |
| Light drinkers: Consuming less than three drinks per week [31] |
| Moderate drinkers: Drinking without engaging in heavy episodic or binge drinking in the past two weeks [55] |
| Moderate drinkers: Drinking no more than 1 to 2 drinks per occasion in the past year, and no intoxication or heavy drinking in the past year [26,44] |
| Moderate to heavy drinkers: Consuming more than 3 drinks per week [31] |
| Regular drinkers: Drink at least once a month or more frequently and consume at least three to four drinks when drinking [48] |
| Current drinkers: Drinking at least one time during the past 30 days [33] |
| Daily drinking questionnaire (DDQ): The total number of standard alcoholic drinks consumed during the past week by summing the number of drinks reported for each day [29] |
| Frequent/heavy drinkers: Those who over the past 6 months had a drink at least once a week or had been drunk at least once [59] |
| Binge drinkers: Men/women as drinking five/four or more drinks per drinking occasion at least once in the past two weeks [26,32,33,44,51,55,57] |
| Alcohol use disorders identification test (AUDIT) [29,58] |
| Diagnostic interview schedule for children, version IV, alcohol use disorder (DISC-IV, AUD) [35] |
| Primary care evaluation for mental disorders, alcohol use disorder (PRIME-MD, AUD) [36] |
| Longitudinal interval follow-up evaluation and structured clinical interview for DSM-IV, non-patient version, alcohol use disorder (LIFE and SCID-I/NP, AUD) [60] |
| Cannabis |
| Ever cannabis users: Using cannabis at least once within a lifetime [45,52] |
| Any use of cannabis or hashish in the past six months [50] |
| Infrequent cannabis users: Using cannabis at least once per year but not more than once per month [56] |
| Infrequent cannabis users: Less than weekly cannabis use [30] |
| Frequent cannabis users: Weekly or more cannabis use [30] |
| Current cannabis users: Cannabis use at least one time during the past 30 days [27,32,33,40] |
| The substance abuse module of the composite international diagnostic interview, cannabis use disorder (CIDI-SAM, CUD) [35,36,53,56,60] |
| Tobacco |
| Ever smokers: Smoking at least once within a lifetime [34,37,38,39,52] |
| Current smokers: Smoking at least one time during the past 30 days [25,31,32,33,40,41,42,43,46,47] |
| Regular smokers: Smoking several cigarettes or more per week [48] |
| Regular smokers: Self-report measure: I’m a regular smoker/I’m a heavy smoker [28] |
| Daily smokers: Daily consumption of cigarettes or cigars for a continuous 30-day period or longer [28,34,50,51,59] |
References
- Pearson, C.; Janz, T.; Ali, J. Health at a Glance: Mental and Substance Use Disorders in Canada; Statistics Canada: Ottawa, Canada, 2013.
- Whiteford, H.A.; Ferrari, A.J.; Degenhardt, L.; Feigin, V.; Vos, T. The global burden of mental, neurological and substance use disorders: An analysis from the Global Burden of Disease Study 2010. PLoS ONE 2015, 10, e0116820. [Google Scholar] [CrossRef] [PubMed]
- Canadian Centre on Substance Abuse. Substance Abuse in Canada: Youth in Focus. Available online: http://www.ccsa.ca/Resource%20Library/ccsa-011521-2007-e.pdf (accessed on 9 September 2018).
- Kessler, R.C.; Amminger, G.P.; Aguilar-Gaxiola, S.; Alonso, J.; Lee, S.; Ustün, T.B. Age of onset of mental disorders: A review of recent literature. Curr. Opin. Psychiatry 2007, 20, 359–364. [Google Scholar] [CrossRef] [PubMed]
- Mueser, K.T.; Drake, R.E.; Wallach, M.A. Dual diagnosis: A review of etiological theories. Addict. Behav. 1998, 23, 717–734. [Google Scholar] [CrossRef]
- Canadian Centre on Substance Abuse. Substance Abuse in Canada: Concurrent Disorders. Available online: http://www.ccsa.ca/Resource%20Library/ccsa-011811-2010.pdf (accessed on 9 September 2018).
- World Health Organization. Caring for Children and Adolescents with Mental Disorders: Setting WHO Directions. Available online: http://www.who.int/mental_health/media/en/785.pdf (accessed on 9 September 2018).
- Bitsko, R.H.; Holbrook, J.R.; Ghandour, R.M.; Blumberg, S.J.; Visser, S.N.; Perou, R.; Walkup, J.T. Epidemiology and impact of health care provider-diagnosed anxiety and depression among US children. J. Dev. Behav. Pediatr. 2018, 39, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Public Health Agency of Canada. Chapter 3: The Chief Public Health Officer’s Report on the State of Public Health in Canada 2011—The Health and Well-Being of Canadian Youth and Young Adults. Available online: https://www.canada.ca/en/public-health/corporate/publications/chief-public-health-officer-reports-state-public-health-canada/chief-public-health-officer-report-on-state-public-health-canada-2011/chapter-3.html (accessed on 10 September 2018).
- Demyttenaere, K.; Bruffaerts, R.; Posada-Villa, J.; Gasquet, I.; Kovess, V.; Lepine, J.; Angermeyer, M.C.; Bernert, S.; Morosini, P.; Polidori, G.; et al. Prevalence, severity, and unmet need for treatment of mental disorders in the World Health Organization World Mental Health Surveys. JAMA 2004, 291, 2581–2590. [Google Scholar] [PubMed]
- Holmes, A.; Silvestri, R. Rates of mental illness and associated academic impacts in Ontario’s College students. Can. J. Sch. Psychol. 2016, 31, 27–46. [Google Scholar] [CrossRef]
- Gallagher, M.; Prinstein, M.J.; Simon, V.; Spirito, A. Social anxiety symptoms and suicidal ideation in a clinical sample of early adolescents: Examining loneliness and social support as longitudinal mediators. J. Abnorm. Child Psychol. 2014, 42, 871–883. [Google Scholar] [CrossRef] [PubMed]
- Shrier, L.A.; Harris, S.; Sternberg, M.; Beardslee, W.R. Associations of depression, self-esteem, and substance use with sexual risk among adolescents. Prev. Med. 2001, 33, 179–189. [Google Scholar] [CrossRef] [PubMed]
- Serafini, G.; Muzio, C.; Piccinini, G.; Flouri, E.; Ferrigno, G.; Pompili, M.; Girardi, P.; Amore, M. Life adversities and suicidal behavior in young individuals: A systematic review. Eur. Child Adolesc. Psychiatry 2015, 24, 1423–1446. [Google Scholar] [CrossRef] [PubMed]
- Patel, V.; Flisher, A.J.; Hetrick, S.; McGorry, P. Mental health of young people: A global public-health challenge. Lancet 2007, 369, 1302–1313. [Google Scholar] [CrossRef]
- Health Canada. Canadian Tobacco Alcohol and Drugs (CTADS): 2015 Summary. Available online: https://www.canada.ca/en/health-canada/services/canadian-tobacco-alcohol-drugs-survey/2015-summary.html (accessed on 9 September 2018).
- Banken, J.A. Drug abuse trends among youth in the United States. Ann. N.Y. Acad. Sci. 2004, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Nock, M.K.; Green, J.G.; Hwang, I.; McLaughlin, K.A.; Sampson, N.A.; Zaslavsky, A.M.; Kessler, R.C. Prevalence, correlates, and treatment of lifetime suicidal behavior among adolescents: Results from the National Comorbidity Survey Replication Adolescent Supplement. JAMA Psychiatry 2013, 70, 300–310. [Google Scholar] [CrossRef] [PubMed]
- Townsend, L.; Flisher, A.J.; King, G. A systematic review of the relationship between high school dropout and substance use. Clin. Child Fam. Psychol. Rev. 2007, 10, 295–317. [Google Scholar] [CrossRef] [PubMed]
- Henkel, D. Unemployment and substance use: A review of the literature (1990–2010). Curr. Drug Abuse Rev. 2011, 4, 4–27. [Google Scholar] [CrossRef] [PubMed]
- Ritchwood, T.D.; Ford, H.; DeCoster, J.; Sutton, M.; Lochman, J.E. Risky sexual behavior and substance use among adolescents: A meta-analysis. Child Youth Serv. Rev. 2015, 52, 74–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jordan, C.J.; Andersen, S.L. Sensitive periods of substance abuse: Early risk for the transition to dependence. Dev. Cogn. Neurosci. 2017, 25, 29–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sadock, B.J.; Sadock, V.A.; Ruiz, P. Kaplan and Sadock’s Concise Textbook of Clinical Psychiatry, 4th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2016. [Google Scholar]
- Khantzian, E.J. The self-medication hypothesis of substance use disorders: A reconsideration and recent applications. Harv. Rev. Psychiatry 1997, 4, 231–244. [Google Scholar] [CrossRef]
- Chung, S.S.; Joung, K.H. Risk factors for current smoking among American and South Korean adolescents. 2005–2011. J. Nurs. Scholarsh. 2014, 46, 408–415. [Google Scholar] [CrossRef]
- Richter, L.; Pugh, B.S.; Peters, E.A.; Vaughan, R.D.; Foster, S.E. Underage drinking: Prevalence and correlates of risky drinking measures among youth aged 12–20. Am. J. Drug Alcohol Abuse 2016, 42, 385–394. [Google Scholar] [CrossRef]
- Rasic, D.; Weerasinghe, S.; Asbridge, M.; Langille, D.B. Longitudinal associations of cannabis and illicit drug use with depression, suicidal ideation, and suicidal attempts among Nova Scotia high school students. Drug Alcohol Depend. 2013, 129, 49–53. [Google Scholar] [CrossRef]
- Grunau, G.L.; Ratner, P.A.; Hossain, S.; Johnson, J.L. Depression and anxiety as possible mediators of the association between smoking and attention deficit hyperactivity disorder. Int. J. Ment. Health Addict. 2010, 8, 595–607. [Google Scholar] [CrossRef]
- Villarosa, M.C.; Madson, M.B.; Zeigler-Hill, V.; Noble, J.J.; Mohn, R.S. Social anxiety symptoms and drinking behaviors among college students: The mediating effects of drinking motives. Psychol. Addict. Behav. 2014, 28, 710–718. [Google Scholar] [CrossRef] [PubMed]
- Buckner, J.D.; Schmidt, N.B. Marijuana effect expectancies: Relations to social anxiety and marijuana use problems. Addict. Behav. 2008, 33, 1477–1483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanna, E.Z.; Yi, H.Y.; Dufour, M.C.; Whitmore, C.C. The relationship of early-onset regular smoking to alcohol use, depression, illicit drug use, and other risky behaviors during early adolescence: Results from the youth supplement to the third national health and nutrition examination survey. J. Subst. Abuse 2001, 13, 265–282. [Google Scholar] [CrossRef]
- Roberts, S.J.; Glod, C.A.; Kim, R.; Hounchell, J. Relationships between aggression, depression, and alcohol, tobacco: Implications for healthcare providers in student health. J. Am. Acad. Nurse Pract. 2010, 22, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Kubik, M.Y.; Lytle, L.A.; Birnbaum, A.S.; Murray, D.M.; Perry, C.L. Prevalence and correlates of depressive symptoms in young adolescents. Am. J. Health Behav. 2003, 27, 546–553. [Google Scholar] [CrossRef]
- Goodwin, R.D.; Lewinsohn, P.M.; Seeley, J.R. Cigarette smoking and panic attacks among young adults in the community: The role of parental smoking and anxiety disorders. Biol. Psychiatry 2005, 58, 686–693. [Google Scholar] [CrossRef]
- Roberts, R.E.; Roberts, C.R.; Xing, Y. Comorbidity of substance use disorders and other psychiatric disorders among adolescents: Evidence from an epidemiologic survey. Drug Alcohol Depend. 2007, 88, S4–S13. [Google Scholar] [CrossRef]
- Low, N.C.; Lee, S.S.; Johnson, J.G.; Williams, J.B.; Harris, E.S. The association between anxiety and alcohol versus cannabis abuse disorders among adolescents in primary care settings. Fam. Pract. 2008, 25, 321–327. [Google Scholar] [CrossRef] [Green Version]
- Weiss, J.W.; Mouttapa, M.; Chou, C.P.; Nezami, E.; Johnson, C.A.; Palmer, P.H.; Cen, S.; Gallaher, P.; Ritt-Olson, A.; Azen, S.; et al. Hostility, depressive symptoms, and smoking in early adolescence. J. Adolesc. 2005, 28, 49–62. [Google Scholar] [CrossRef]
- Mendel, J.R.; Berg, C.J.; Windle, R.C.; Windle, M. Predicting young adulthood smoking among adolescent smokers and non-smokers. Am. J. Health Behav. 2012, 36, 542–554. [Google Scholar] [CrossRef] [PubMed]
- Munafò, M.R.; Hitsman, B.; Rende, R.; Metcalfe, C.; Niaura, R. Effects of progression to cigarette smoking on depressed mood in adolescents: Evidence from the National Longitudinal Study of Adolescent Health. Addiction 2008, 103, 162–171. [Google Scholar] [CrossRef]
- Ridner, S.L.; Staten, R.R.; Danner, F.W. Smoking and depressive symptoms in a college population. J. Sch. Nurs. 2005, 21, 229–235. [Google Scholar] [CrossRef] [PubMed]
- Duncan, B.; Rees, D.I. Effect of smoking on depressive symptomatology: A re-examination of data from the National Longitudinal Study of Adolescent Health. Am. J. Epidemiol. 2005, 162, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Goodman, E.; Capitman, J. Depressive symptoms and cigarette smoking among teens. Pediatrics 2000, 106, 748–755. [Google Scholar] [CrossRef] [PubMed]
- Lechner, W.V.; Janssen, T.; Kahler, C.W.; Audrain-McGovern, J.; Leventhal, A.M. Bi-directional associations of electronic and combustible cigarette use onset patterns with depressive symptoms in adolescents. Prev. Med. 2017, 96, 73–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paschall, M.J.; Freisthler, B.; Lipton, R.I. Moderate alcohol use and depression in young adults: Findings from a national longitudinal study. Am. J. Public Health 2005, 95, 453–457. [Google Scholar] [CrossRef] [PubMed]
- Suerken, C.K.; Reboussin, B.A.; Sutfin, E.L.; Wagoner, K.G.; Spangler, J.; Wolfson, M. Prevalence of marijuana use at college entry and risk factors for initiation during freshman year. Addict. Behav. 2014, 39, 302–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martini, S.; Wagner, F.A.; Anthony, J.C. The association of tobacco smoking and depression in adolescence: Evidence from the United States. Subst. Use Misuse 2002, 37, 1853–1867. [Google Scholar] [CrossRef] [PubMed]
- Berg, C.; Choi, W.S.; Kaur, H.; Nollen, N.; Ahluwalia, J.S. The roles of parenting, church attendance, and depression in adolescent smoking. J. Community Health 2009, 34, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Simantov, E.; Schoen, C.; Klein, J.D. Health-compromising behaviors: Why do adolescents smoke or drink? Identifying underlying risk and protective factors. Arch. Pediatr. Adolesc. Med. 2000, 154, 1025–1033. [Google Scholar] [CrossRef] [PubMed]
- Richardson, A.; He, J.P.; Curry, L.; Merikangas, K. Cigarette smoking and mood disorders in U.S. adolescents: Sex-specific associations with symptoms, diagnoses, impairment and health services use. J. Psychosom. Res. 2012, 72, 269–275. [Google Scholar] [CrossRef] [Green Version]
- Georgiades, K.; Boyle, M.H. Adolescent tobacco and cannabis use: Young adult outcomes from the Ontario Child Health Study. J. Child Psychol. Psychiatry 2007, 48, 724–731. [Google Scholar] [CrossRef] [PubMed]
- Naicker, K.; Galambos, N.L.; Zeng, Y.; Senthilselvan, A.; Colman, I. Social, demographic, and health outcomes in the 10 years following adolescent depression. J Adolesc. Heal. 2013, 52, 533–538. [Google Scholar] [CrossRef] [PubMed]
- Brook, D.W.; Brook, J.S.; Zhang, C.; Cohen, P.; Whiteman, M. Drug use and the risk of major depressive disorder, alcohol dependence, and substance use disorders. Arch. Gen. Psychiatry 2002, 59, 1039–1044. [Google Scholar] [CrossRef] [PubMed]
- Harder, V.S.; Stuart, E.A.; Anthony, J.C. Adolescent cannabis problems and young adult depression: Male-female stratified propensity score analyses. Am. J. Epidemiol. 2008, 168, 592–601. [Google Scholar] [CrossRef] [PubMed]
- O’Loughlin, J.; O’Loughlin, E.K.; Wellman, R.J.; Sylvestre, M.P.; Dugas, E.N.; Chagnon, M.; Dutczak, H.; Laguë, J.; McGrath, J.J. Predictors of cigarette smoking initiation in early, middle, and late adolescence. J. Adolesc. Health 2017, 61, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Weitzman, E.R. Poor mental health, depression, and associations with alcohol consumption, harm, and abuse in a national sample of young adults in college. J. Nerv. Ment. Dis. 2004, 192, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Marmorstein, N.R. Anxiety disorders and substance use disorders: Different associations by anxiety disorder. J. Anxiety Disord. 2012, 26, 88–94. [Google Scholar] [CrossRef] [Green Version]
- Meade, E.A.; Woolaway-Bickel, K.; Schmidt, N.B. Social anxiety and alcohol use: Evaluation of the moderating and mediating effects of alcohol expectancies. J. Anxiety Disord. 2004, 18, 33–49. [Google Scholar] [CrossRef]
- Strahan, E.Y.; Panayiotou, G.; Clements, R.; Scott, J. Beer, wine, and social anxiety: Testing the “self-medication hypothesis” in the US and Cyprus. Addict. Res. Theory 2011, 19, 302–311. [Google Scholar] [CrossRef]
- Wu, P.; Goodwin, R.D.; Fuller, C.; Liu, X.; Comer, J.S.; Cohen, P.; Hoven, C.W. The relationship between anxiety disorders and substance use among adolescents in the community: Specificity and gender differences. J. Youth Adolesc. 2010, 39, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Buckner, J.D.; Schmidt, N.B.; Lang, A.R.; Small, J.W.; Schlauch, R.C.; Lewinsohn, P.M. Specificity of social anxiety disorder as a risk factor for alcohol and cannabis dependence. J. Psychiatr. Res. 2008, 42, 230–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; Ottawa Health Research Institute: Ottawa, ON, Canada, 1999. [Google Scholar]
- Hedges, L.V.; Vevea, J.L. Fixed and random effects models in meta-analysis. Psychol. Methods 1998, 3, 486–504. [Google Scholar] [CrossRef]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Chaiton, M.O.; Cohen, J.E.; O’Loughlin, J.; Rehm, J. A systematic review of longitudinal studies on the association between depression and smoking in adolescents. BMC Public Health 2009, 9, 356. [Google Scholar] [CrossRef] [PubMed]
- Moore, T.H.; Zammit, S.; Lingford-Hughes, A.; Barnes, T.R.; Jones, P.B.; Burke, M.; Lewis, G. Cannabis use and risk of psychotic or affective mental health outcomes: A systematic review. Lancet 2007, 370, 319–328. [Google Scholar] [CrossRef]
- Kedzior, K.K.; Laeber, L.T. A positive association between anxiety disorders and cannabis use or cannabis use disorders in the general population- a meta-analysis of 31 studies. BMC Psychiatry 2014, 14, 136. [Google Scholar] [CrossRef] [PubMed]
- Windle, M. Alcohol use among adolescents and young adults. Alcohol Res. Health 2003, 27, 79–85. [Google Scholar] [PubMed]
- Brière, F.N.; Rohde, P.; Seeley, J.R.; Klein, D.; Lewinsohn, P.M. Comorbidity between major depression and alcohol use disorder from adolescence to adulthood. Compr. Psychiatry 2014, 55, 526–533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rohde, P.; Lewinsohn, P.M.; Kahler, C.W.; Seeley, J.R.; Brown, R.A. Natural course of alcohol use disorders from adolescence to young adulthood. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Lev-Ran, S.; Roerecke, M.; Le Foll, B.; George, T.P.; McKenzie, K.; Rehm, J. The association between cannabis use and depression: A systematic review and meta-analysis of longitudinal studies. Psychol. Med. 2014, 44, 797–810. [Google Scholar] [CrossRef] [PubMed]
- Degenhardt, L.; Hall, W.; Lynskey, M. Exploring the association between cannabis use and depression. Addiction 2003, 98, 1493–1504. [Google Scholar] [CrossRef]
- Picciotto, M.R.; Brunzell, D.H.; Caldarone, B.J. Effect of nicotine and nicotinic receptors on anxiety and depression. Neuroreport 2002, 13, 1097–1106. [Google Scholar] [CrossRef] [PubMed]
- Tweed, J.O.; Hsia, S.H.; Lutfy, K.; Friedman, T.C. The endocrine effects of nicotine and cigarette smoke. Trends Endocrinol. Metab. 2012, 23, 334–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kassel, J.D.; Stroud, L.R.; Paronis, C.A. Smoking, stress, and negative affect: Correlation, causation, and context across stages of smoking. Psychol. Bull. 2003, 129, 270–304. [Google Scholar] [CrossRef] [PubMed]
- Moylan, S.; Jacka, F.N.; Pasco, J.A.; Berk, M. How cigarette smoking may increase the risk of anxiety symptoms and anxiety disorders: A critical review of biological pathways. Brain Behav. 2013, 3, 302–326. [Google Scholar] [CrossRef]
- American College Health Association. American College Health Association-National College Health Assessment II: Canadian Reference Group Executive Summary Spring 2016; American College Health Association: Hanover, MD, USA, 2016. [Google Scholar]
- American College Health Association. American College Health Association-National College Health Assessment II: U.S. Reference Group Executive Summary Spring 2016; American College Health Association: Hanover, MD, USA, 2016. [Google Scholar]
- National Association of State Mental Health Program Directors and National Association of State Alcohol and Drug Abuse Directors. National Dialogue on Co-Occurring Mental Health and Substance Abuse Disorders; National Association of State Alcohol and Drug Abuse Directors: Washington, DC, USA, 1999.




{kind=link}
{kind=link}
{kind=link}
| First Author’s Name, Year, Country | Sample Size | Target Population | Substance Use Measure | Mental Health Disorders Assessment | % of Depressive Participants | Controlled Variables | OR (95% CI) |
|---|---|---|---|---|---|---|---|
| Association between Depression and Alcohol Use | |||||||
| Cross-Sectional Studies | |||||||
| Elissa Weitzman, 2004, U.S. [55] | 27,687 | College students aged 18–24 | Binge/non-drinkers | Depressive symptoms: The 5-item subscale of SF36 | 4.9% | Age, sex, ethnicity | Adjusted: 1.05 (0.96–1.14) |
| Martha Kubik, 2005, U.S. [33] | 3466 | Grade 7 students | Heavy/non-drinkers | Depressive symptoms: CES-D, cut-off point of 16. | 35% | Age, ethnicity, socioeconomic status (SES), smoking, cannabis, and inhalants use | Adjusted: 2.03 (1.30–3.17) |
| Susan Roberts, 2009, U.S. [32] | 418 | College students | Binge/non-drinkers | Depressive symptoms: BDI-II, cut-off point of 20 | 22% | - | Crude: 0.99 (0.61–1.58) |
| Elisabeth Simantov, 2000, U.S. [48] | 5513 | Grade 7–12 students | Regular/non-drinkers | Depressive symptoms: Modified version of CDI, cut-off point of 9 | 18.2% | - | Crude: 2.08 (1.79–2.42) |
| Linda Richter, 2015, U.S. [26] | 24,445 | Adolescents aged 12–20 | Binge/non-drinkers | Major depressive disorder: Diagnosed depression (self-reported) | - | Sex, ethnicity, and age | Adjusted: 1.45 (1.11–1.91) |
| Eleanor Hanna, 2001, U.S. [31] | 2001 | Adolescents aged 12–16 | Moderate/non-drinkers | Major depressive disorder: Diagnostic interview schedule, DSM-III | 9% | Age, sex, ethnicity, family poverty level, school problem, smoking status | Adjusted: 3.31 (1.39–7.90) |
| Longitudinal Studies: Alcohol Use (Exposure) → Depression (Outcome) | |||||||
| Mallie Paschall, 2005, U.S. [44] | 13,892 | Grade 6–12 students | Moderate/non-drinkers | Depressive symptoms: CES-D, cut-off point of 16. | 5.3% | - | Crude: 1.17 (1.11–1.23) |
| David Brook, 2002, U.S. [52] | 736 | Adolescents aged 14, 13-year follow-up | Ever/never alcohol users | Major depressive disorder: Modified version of CIDI | 8.3% | Age, sex, parental educational level, family income, prior psychiatric disorders | Adjusted: 1.72 (1.35–2.20) |
| Longitudinal Study: Depression (Exposure) → Alcohol Use (Outcome) | |||||||
| Kiyuri Naicker, 2012, Canada [51] | 1027 | Adolescents aged 16–17, 10-year follow-up | Heavy/non-drinkers | Major Depressive Disorder: CIDI-SF, cut-off point of 5 | 6.9% | Sex and SES | Adjusted: 1.78 (1.10–2.88) |
| Association between Depression and Cannabis Use | |||||||
| Cross-Sectional Studies | |||||||
| Lee Ridner, 2005, U.S. [40] | 895 | College students aged 18–24 | Current/non- cannabis users | Depressive symptoms: CES-D, cut-off point of 16 | - | - | Crude: 1.27 (1.00–1.61) |
| Susan Roberts, 2009, U.S. [32] | 418 | College students | Current/non- cannabis users | Depressive symptoms: BDI-II, cut-off point of 20 | 22% | - | Crude: 1.99 (1.23–3.22) |
| Martha Kubik, 2005, U.S. [33] | 3466 | Grade 7 students | Current/non- cannabis users | Depressive symptoms: CES-D, cut-off point of 16 | 35% | Age, ethnicity, SES, smoking, alcohol, and inhalants use. | Adjusted: 1.02 (0.66–1.57) |
| Longitudinal Studies: Cannabis Use (Exposure) → Depression (Outcome) | |||||||
| Daniel Rasic, 2012, Canada [27] | 976 | Grade 10 students, 2-year follow-up | Current/non- cannabis users | Depressive symptoms: CES-D, cut-off point of 22 (M) and 24 (F) | 20% | Sex | Adjusted: 1.24 (1.05–1.46) |
| Katholiki Georgiades, 2007, Canada [50] | 1282 | Adolescents aged 12–16, 14-year follow-up | Past 6-month/non- cannabis users | Major depressive disorder: CIDI-SF | 11.8% | Physical health, life satisfaction, personal income, years of education | Adjusted: 1.97 (0.81–4.81) |
| David Brook, 2002, U.S. [52] | 736 | Adolescents aged 14, 10-year follow-up | Ever/never cannabis users | Major depressive disorder: Modified version of CIDI | 8.3% | Age, sex, parental educational level, family income, prior psychiatric disorders | Adjusted: 1.36 (1.14–1.62) |
| Naomi Marmorstein, 2011, U.S. [56] | 1252 | Adolescents aged 17, A 6-year follow-up | CUD/non- cannabis users | Major depressive disorder: The structured clinical interview for DSM-III-R. | 13.9% | MDD by age 17 and gender | Adjusted: 1.86 (1.11–3.11), |
| Valerie Harder, 2008, U.S. [53] | 1494 | Adolescents aged 12–16, 7-year follow-up | CUD/non- cannabis users | Major depressive disorder: CIDI, DSM IV diagnostic criteria | 6% | Ethnicity, family income, free lunch, tobacco, alcohol, and other illegal drug use, parental monitoring, concentration, behavior problems, shyness, anxiety symptoms, intervention status | Adjusted: 1.33 (0.70–2.53) |
| Longitudinal Study: Depression (Exposure) → Cannabis Use (Outcome) | |||||||
| Cynthia Suerken, 2014, U.S. [45] | 3146 | College students, A 6-month follow-up | Ever/never cannabis users | Depressive symptoms: CES-D, Iowa short form | - | Sex, ethnicity, parental education and spending money available, varsity athlete, club, intramural sports, member of a sorority/fraternity, attend religious services, live on campus, relationship status, current use of tobacco, alcohol, and lifetime use of other illicit drugs | Crude: 1.03 (1.01–1.05) |
| Association between Depression and Tobacco Use | |||||||
| Cross-Sectional Studies | |||||||
| Lee Ridner, 2005, U.S. [40] | 895 | College students aged 18–24 | Current/non-tobacco users | Depressive symptoms: CES-D, cut-off point of 16 | - | - | Crude: 1.49 (1.18–1.90) |
| Susan Roberts, 2009, U.S. [32] | 418 | College students, aged 18–21 | Current/non- tobacco users | Depressive symptoms: BDI-II, cut-off point of 20 | 22% | - | Crude: 2.08 (1.29–3.36) |
| Elisabeth Simantov, 2000, U.S. [48] | 5513 | Grade 7–12 students | Regular/non- tobacco users | Depressive symptoms: Modified version of CDI, cut-off point of 9 | 18.2% | - | Crude: 2.47 (2.06–2.97) |
| Sung Chung, 2014, U.S. [25] | 11,848 | Grade 9–11 students | Current/non- tobacco users | Depressive symptoms: 1 item question | 28.4% | - | Crude: 1.33 (1.16–1.53) |
| Shahm Martini, 2002, U.S. [46] | 11,201 | Adolescents aged 12–17 | Current/non- tobacco users | Depressive symptoms: YSR, cut-off point of 3 | - | Age, ethnicity, school attendance, site, substance use behaviors | Crude: 1.83 (1.67–2.01) |
| Carla Berg, 2008, U.S. [47] | 299 | Adolescents aged 10–19 | Current/non- tobacco users | Depressive symptoms: A 5-item question, cut-off point of 21 | 12% | Age, sex, ethnicity, church attendance, perceived parental attitude | Crude: 3.83 (1.65–8.88) |
| Martha Kubik, 2005, U.S. [33] | 3466 | Grade 7 students | Current/non- tobacco users | Depressive symptoms: CES-D, cut-off point of 16 | 35% | Age, ethnicity, SES, all other substance use behaviors | Adjusted: 1.56 (1.14–2.14) |
| Gilat Grunau, 2009, Canada [28] | 6943 | Students aged 13–18 | Current/non- tobacco users | Major depressive disorder: Prescribed depression medications | 2.2% | Age, sex, ethnicity, parent(s), sibling(s), peer(s) smokes, anxiety | Adjusted: 2.59 (1.79–3.73) |
| Amanda Richardson, 2012, U.S. [49] | 1884 | Adolescents aged 12–15 | Ever/never tobacco users | Major depressive disorder: NIMH-DISC-IV | - | Age, ethnicity, attending school, poverty index ratio, live with smokers, anxiety disorders | Adjusted: 2.80 (1.13–6.91) |
| Eleanor Hanna, 2001, U.S. [31] | 719 | Adolescents aged 12–16 | Current/non- tobacco users | Major depressive disorder: Diagnostic interview schedule, DSM-III | 9% | Age, sex, ethnicity, family poverty status, school problem, drinking status | Adjusted: 0.98 (0.33–2.90) |
| Longitudinal Studies: Tobacco Use (Exposure) → Depression (Outcome) | |||||||
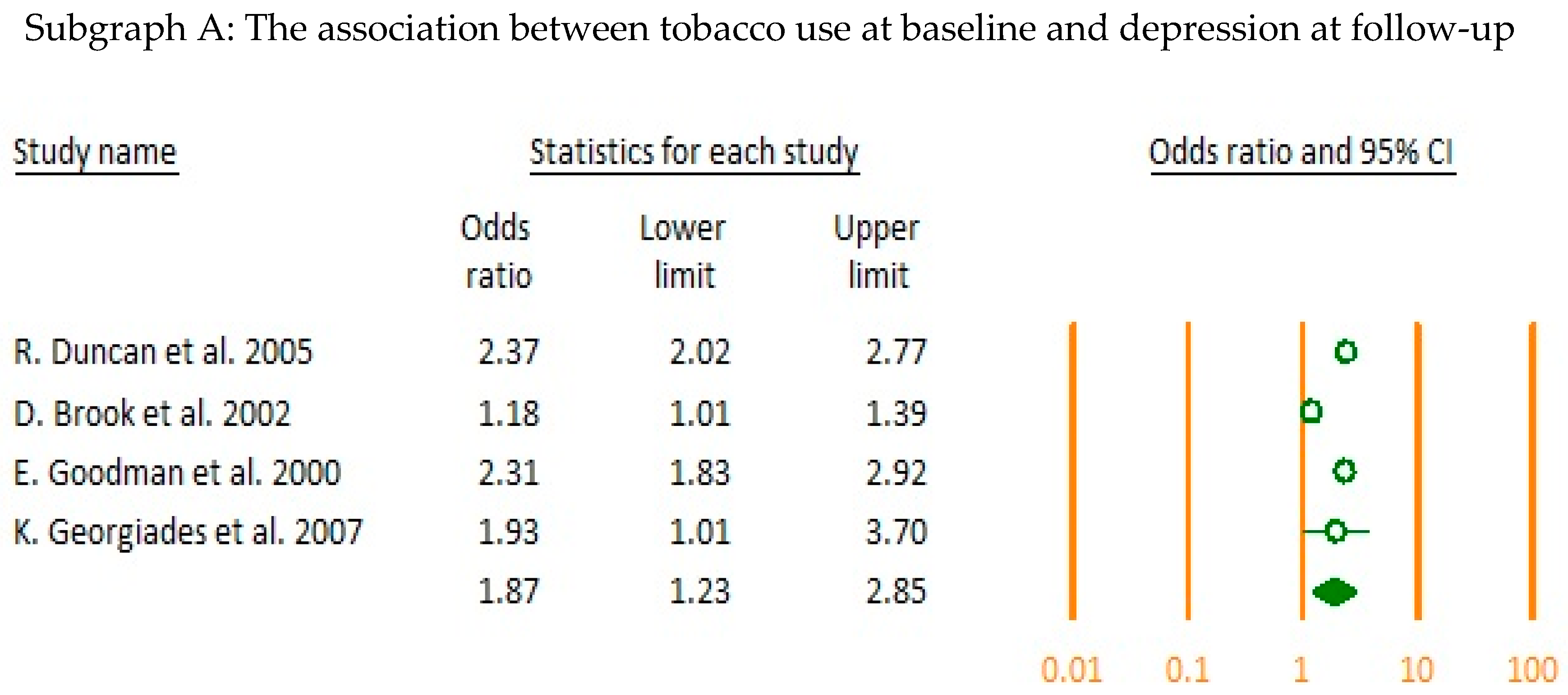
| Brian Duncan, 2005, U.S. [41] | 13,068 | Students grade 7–12, 1-year follow-up | Current/non- tobacco users | Depressive symptoms: CES-D, cut-off point of 22 (M) and 24 (F) | - | Disability, age, ethnicity, household, parental education, county-level variables | Crude: 2.37 (2.02–2.77) |
| Elizabeth Goodman, 2000, U.S. [42] | 8704 | Adolescents aged 11–22, 1-year follow-up | Current/non- tobacco users | Depressive symptoms: CES-D, cut-off point of 22 (M) and 24 (F) | 6.4% | Age, sex, ethnicity, parental education | Crude: 2.31 (1.83–2.92) |
| Katholiki Georgiades, 2007, Canada [50] | 1282 | Adolescents aged 12–16, 14-year follow-up | Daily/non- tobacco users | Major depressive disorder: CIDI-SF | 11.8% | Physical health, life satisfaction, personal income, years of education | Adjusted: 1.93 (1.01–3.70) |
| David Brook, 2002, U.S. [52] | 736 | Adolescents aged 14, A 13-year follow-up | Ever/never tobacco users | Major depressive disorder: Modified version of CIDI | 8.3% | Age, sex, parental educational level, family income, prior psychiatric disorders | Adjusted: 1.18 (1.01–1.39) |
| Longitudinal Studies: Depression (Exposure) → Tobacco Use (Outcome) | |||||||
| Elizabeth Goodman, 2000, U.S. [42] | 6947 | Adolescents aged 11–22, 1-year follow-up | Current/non- tobacco users | Depressive symptoms: CES-D, cut-off point of 22 (M) and 24 (F) | 6.4% | Age, sex, ethnicity, education | Crude: 2.81 (1.67–4.74) |
| Kiyuri Naicker, 2012, Canada [51] | 681 | Adolescents aged 16–17, 10-year follow-up | Daily/non- tobacco users | Major depressive disorder: CIDI-SF, cut-off point of 5 | 6.9% | Sex and SES | Adjusted: 2.89 (1.53–5.45) |
| Jie Wu Weiss, 2004, U.S. [37] | 1699 | Grade 6 students, A 1-year follow-up | Ever/never tobacco users | Depressive symptoms: CES-D, cut-off point of 16 | - | change in depression and hostility, sex, ethnicity, SES | Adjusted: 1.76 (1.30–2.38) |
| Jennifer Mendel, 2012, U.S. [38] | 1205 | Grade 10–11 students, A 5-year follow-up | Ever/never tobacco users | Depressive symptoms: CES-D, cut-off point of 16 | - | Sex, parental marital status, family income, education level, marital status, children, GPA, delinquency, stressful life events, family support, quality of friendship, parental smoking, adolescent alcohol, cannabis use, extent of alcohol problems, peers who drink or use drugs, change in CESD and alcohol use | Adjusted: 0.97 (0.92–1.03) |
| Jennifer O’Loughlin, 2016, Canada [54] | 690 | Grade 5 students, 7-year follow-up | Ever/never tobacco users | Depressive symptoms: 6-item question | - | Age, sex, mother’s education | Adjusted: 1.34 (1.16–1.56) |
| Marcus Munafo, 2007, U.S. [39] | 12,149 | Grade 7–12 students, 1-year follow-up | Ever/never tobacco users | Depressive symptoms: CES-D, cut-off point of 22 (M) and 24 (F) | - | Age, sex, ethnicity, depressed mood, parental/peer tobacco, alcohol use, delinquency score | Adjusted: 1.13 (1.03–1.25) |
| William Lechner, 2016, U.S. [43] | 2460 | Grade 9 students, A 1-year follow-up | Ever/never tobacco users | Depressive symptoms: CES-D, cut-off point of 22 (M) and 24 (F) | - | Age, sex, ethnicity, school, living situation, parental education, use of alcohol and other tobacco products | Adjusted: 1.02 (1.01–1.04) |
| First author’s name, year, country | Sample size | Target population | Substance use measure | Mental health disorders assessment | % of participants with anxiety | Controlled variables | OR (95% CI) |
| Association between Anxiety and Alcohol Use | |||||||
| Cross-Sectional Studies | |||||||
| Margo Villarosa, 2014, U.S. [29] | 532 | College students aged 18–22 | Alcohol Use Disorder: AUDIT | Social anxiety symptoms: SIAS | - | - | Crude: 1.61 (1.29–2.00) |
| Meade Eggleston, 2003, U.S. [57] | 284 | College students aged 17–23 | Binge/non-drinkers | Social anxiety symptoms: SIAS | - | - | Crude: 1.55 (1.15–2.10) |
| Esther Strahan, 2010, U.S. [58] | 697 | College students aged 17–27 | Alcohol Use Disorder: AUDIT | Social anxiety symptoms: SIAS | - | - | Crude: 1.04 (1.01–1.08) |
| Ping Wu, 2009, U.S. [59] | 781 | Adolescents aged 13–17 | Frequent, heavy/non-drinkers | Any anxiety disorders: DISC | 18.4% | Age, ethnicity, public assistance, not living with parents, parental drug/alcohol problems, site | Adjusted: 1.74 (1.07–2.81) |
| Linda Richter, 2015, U.S. [26] | 24,445 | Adolescents aged 12–20 | Binge/non-drinkers | Any anxiety disorders: Diagnosed anxiety (self-reported) | - | Age, sex, ethnicity | Adjusted: 1.54 (1.12–2.12) |
| Robert Roberts, 2007, U.S. [35] | 4175 | Adolescents aged 11–17 | Alcohol Use Disorder: AUD | Any anxiety disorders: DISC-IV | 6.9% | Mood, conduct oppositional, and ADHD disorders. | Crude: 1.57 (0.72–3.40) |
| Nancy Low, 2008, U.S. [36] | 632 | Adolescents aged 13–19 | Alcohol Use Disorder: AUD | Any Anxiety Disorders: PRIME-MD | 7% | Age, sex, ethnicity, sample site, mood disorders | Adjusted: 3.80 (1.21–11.91) |
| Longitudinal Study: Anxiety (Exposure) → Alcohol Use (Outcome) | |||||||
| Julia Buckner, 2008, U.S. [60] | 816 | Students aged 15–17, 14-year follow-up | Alcohol Use Disorder: AUD | Any anxiety disorders: K-SADS | - | Sex, conduct, mood, CUDs, T1 AUD excluded | Adjusted: 2.16 (0.82–5.69) |
| Association between Anxiety and Cannabis Use | |||||||
| Cross-Sectional Studies | |||||||
| Julia Buckner, 2008, U.S. [30] | 337 | College students aged 18–26 | Frequent/non-cannabis users | Social anxiety symptoms: SIAS | 18.8% | - | Crude: 1.23 (0.88–1.73) |
| Robert Roberts, 2007, U.S. [35] | 4175 | Adolescents aged 11–17 | Cannabis Use Disorder: CUD | Any anxiety disorder: DISC-IV | 6.9% | Mood, conduct oppositional, and ADHD disorders | Crude: 1.38 (0.70–2.75) |
| Nancy Low, 2008, U.S. [36] | 632 | Adolescents aged 13–19 | Cannabis Use Disorder: CUD | Any anxiety disorder: PRIME-MD | 7% | Age, sex, ethnicity, sample site, mood disorders | Crude: 1.40 (0.40–4.70) |
| Longitudinal Study: Anxiety (Exposure) → Cannabis Use (Outcome) | |||||||
| Julia Buckner, 2008, U.S. [60] | 816 | Students aged 15–17, 14-year follow-up | Cannabis Use Disorder: CUD | Social anxiety disorder: K-SADS | - | Sex, conduct, mood, AUDs, T1 CUD excluded | Adjusted: 3.28 (1.14–9.40) |
| Association between Anxiety and Cannabis Use | |||||||
| Cross-Sectional Studies | |||||||
| Gilat Grunau, 2009, Canada [28] | 6943 | Students aged 13–18 | Current/non-cannabis users | Any anxiety disorder: Prescribed anxiety medications | 0.6% | Sex, ethnicity, age, parent(s), sibling(s), peer(s) smokes, depression | Adjusted: 1.83 (1.05–3.22) |
| Ping Wu, 2009, U.S. [59] | 781 | Adolescents aged 13–17 | Daily/non- cannabis users | Any anxiety disorders: DISC | 18.4% | Age, ethnicity, public assistance, not living with parents, parental drug/alcohol problems, site. | Adjusted: 3.14 (1.69–5.81) |
| Amanda Richardson, 2012, U.S. [49] | 1884 | Adolescents aged 12–15 | Ever/never cannabis users | Any anxiety disorder: NIMH-DISC-IV | - | Age, ethnicity, attending school, poverty index ratio, live with smokers, depressive disorder | Adjusted: 4.70 (1.61–13.75) |
| Longitudinal Study: Tobacco Use (Exposure) → Anxiety (Outcome) | |||||||
| Renee Goodwin, 2005, U.S. [34] | 940 | Students aged 14–18, anxiety: young adults mean age 24.2 | Ever/never cannabis users | Any anxiety disorders: K-SADS | - | - | Crude: 1.88 (1.47–2.41) |
| Longitudinal Study: Anxiety (Exposure) → Tobacco Use (Outcome) | |||||||
| Renee Goodwin, 2005, U.S. [34] | 940 | Students aged 14–18, tobacco use: young adults mean age 24.2 | Ever/Never cannabis users | Any anxiety disorders: K-SADS | - | - | Crude: 1.38 (0.83–2.29) |
| Topics | Study Designs | n | OR (95% CI) | I2% and p-Value |
|---|---|---|---|---|
| Depression and Alcohol use | Overall | 9 | 1.50 (1.24–1.83) | 90.54, <0.001 |
| Cross-Sectional | 6 | 1.57 (1.09–2.26) | 92.89, <0.001 | |
| Longitudinal: Alcohol use at baseline | 2 | 1.39 (0.95–2.03) | 89.24, <0.001 | |
| Longitudinal: Depression at baseline | 1 | 1.78 (1.10–2.88) | n/a | |
| Depression and Cannabis use | Overall | 9 | 1.29 (1.10–1.51) | 74.79, <0.01 |
| Cross-Sectional | 3 | 1.34 (0.97–1.84) | 53.26, 0.12 | |
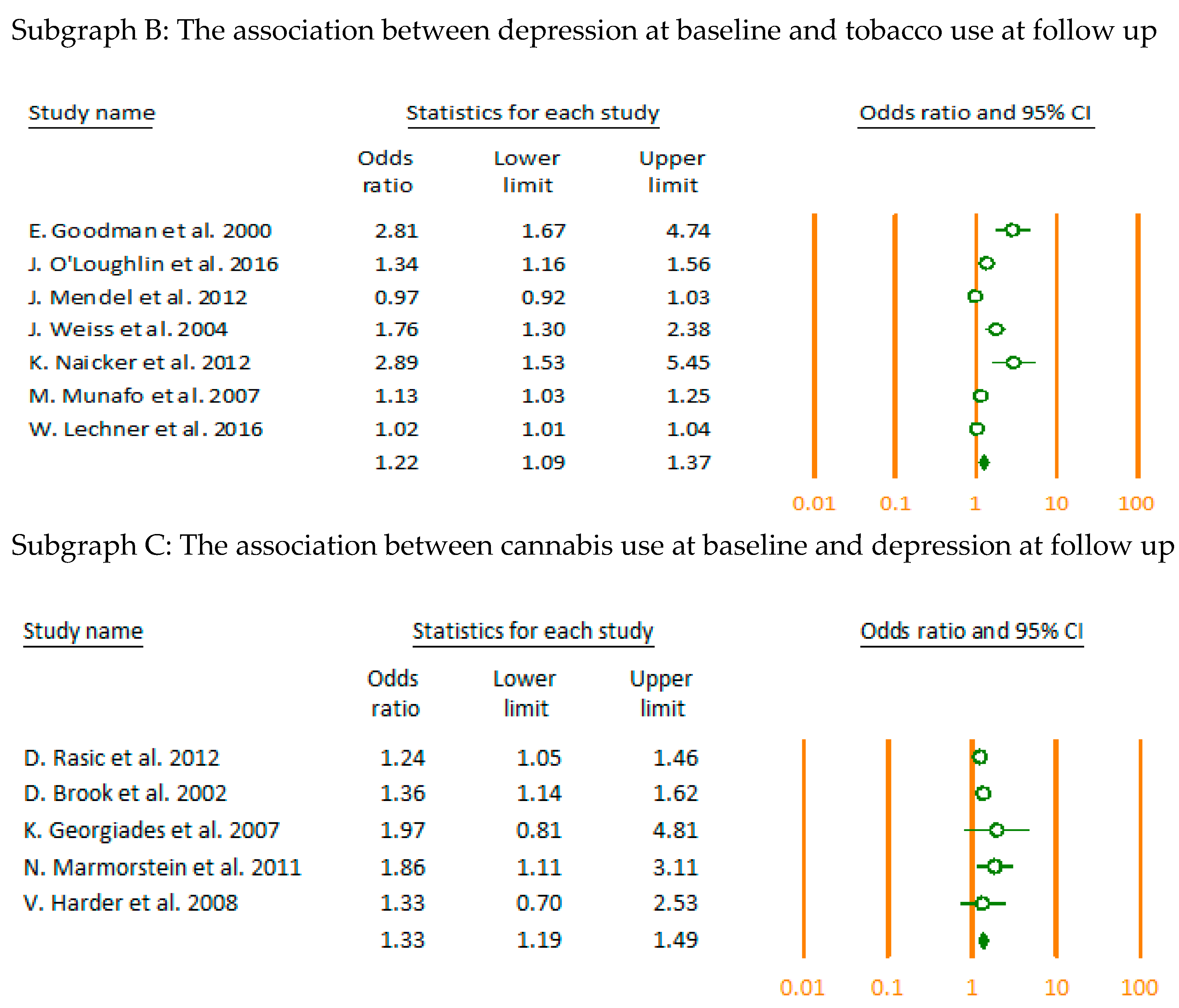
| Longitudinal: Cannabis use at baseline | 5 | 1.33 (1.19–1.49) | 0.00, 0.53 | |
| Longitudinal: Depression at baseline | 1 | 1.03 (1.01–1.05) | n/a | |
| Depression and Tobacco use | Overall | 20 | 1.65 (1.43–1.92) | 96.23, <0.01 |
| Cross-Sectional | 10 | 1.87 (1.55–2.25) | 78.60, <0.01 | |
| Longitudinal: Tobacco use at baseline | 4 | 1.87 (1.23–2.85) | 92.95, <0.01 | |
| Longitudinal: Depression at baseline | 7 | 1.22 (1.09–1.37) | 89.56, <0.001 | |
| Anxiety and Alcohol use | Overall | 8 | 1.54 (1.19–2.00) | 81.52, <0.001 |
| Cross-Sectional | 7 | 1.51 (1.16–1.97) | 83.28, <0.001 | |
| Longitudinal: Alcohol use at baseline | - | - | - | |
| Longitudinal: Anxiety at baseline | 1 | 2.16 (0.82–5.69) | n/a | |
| Anxiety and Cannabis use | Overall | 4 | 1.36 (1.02–1.81) | 0.39, 0.39 |
| Cross-Sectional | 3 | 1.27 (0.94–1.70) | 0.00, 0.94 | |
| Longitudinal: Cannabis use at baseline | - | - | - | |
| Longitudinal: Anxiety at baseline | 1 | 3.28 (1.14–9.40) | n/a | |
| Anxiety and Tobacco use | Overall | 4 | 2.21 (1.54–3.17) | 46.17, 0.13 |
| Cross-Sectional | 3 | 2.67 (1.62–4.37) | 33.12, 0.22 | |
| Longitudinal: Tobacco use at baseline | 1 | 1.88 (1.47–2.41) | n/a | |
| Longitudinal: Anxiety at baseline | 1 | 1.38 (0.83–2.29) | n/a |
| Subgroup Analysis | n | OR (95% CI) | I2% and p-Value | p-Value | ||
|---|---|---|---|---|---|---|
| Depression and Alcohol use | Point Estimate | Crude | 3 | 1.37 (0.87–2.18) | 96.08, <0.001 | 0.56 |
| Adjusted | 6 | 1.62 (1.19–2.19) | 84.60, <0.001 | |||
| Target Population | Adolescents | 7 | 1.69 (1.28–2.25) | 90.63, <0.001 | 0.28 | |
| Young adults | 3 | 1.28 (0.83–1.97) | 82.52, <0.001 | |||
| Severity of MHDs 1 | Symptoms | 5 | 1.37 (1.08–1.75) | 94.04, <0.001 | 0.21 | |
| Disorders | 4 | 1.67 (1.38–2.02) | 14.68, 0.32 | |||
| Intensity of substance use | Not binge drinkers | 6 | 1.61 (1.29–2.01) | 79.79, <0.001 | 0.06 | |
| Binge drinkers | 6 | 1.21 (0.99–1.47) | 87.67, <0.001 | |||
| Depression and Cannabis use | Point Estimate | Crude | 3 | 1.27 (0.95–1.69) | 80.29, <0.001 | 0.85 |
| Adjusted | 6 | 1.31 (1.17–1.46) | 0.00, 0.48 | |||
| Target Population | Adolescents | 6 | 1.34 (1.17–1.54) | 9.96, 0.35 | 0.46 | |
| Young adults | 4 | 1.22 (0.99–1.51) | 72,62, 0.01 | |||
| Severity of MHDs | Symptoms | 5 | 1.20 (1.01–1.42) | 73.16, <0.001 | 0.16 | |
| Disorders | 4 | 1.41 (1.21–1.65) | 0.00, 0.60 | |||
| Intensity of substance use | Cannabis use | 7 | 1.25 (1.06–1.47) | 77.10, <0.001 | 0.23 | |
| CUD 2 | 2 | 1.63 (1.09–2.44) | 0.00, 0.42 | |||
| Depression and Tobacco use | Point Estimate | Crude | 8 | 1.99 (1.65–2.40) | 86.62, <0.001 | <0.001 |
| Adjusted | 12 | 1.30 (1.16–1.45) | 87.12, <0.001 | |||
| Target Population | Adolescents | 18 | 1.67 (1.43–1.96) | 96.56, <0.001 | 0.40 | |
| Young adults | 3 | 1.37 (0.89–2.12) | 84.18, <0.001 | |||
| Severity of MHDs | Symptoms | 14 | 1.61 (1.36–1.89) | 97.18, <0.001 | 0.48 | |
| Disorders | 6 | 1.91 (1.22–2.97) | 78.86, <0.001 | |||
| Intensity of substance use | Ever smokers | 7 | 1.14 (1.04–1.25) | 84.89, <0.001 | <0.001 | |
| Current smokers | 14 | 1.90 (1.62–2.23) | 82.65, <0.001 | |||
| Anxiety and Alcohol use | Point Estimate | Crude | 4 | 1.37 (1.00–1.88) | 86.27, <0.001 | 0.3 |
| Adjusted | 4 | 1.70 (1.32–2.18) | 0.00, 0.47 | |||
| Target Population | Adolescents | 5 | 1.69 (1.33–2.14) | 0.00, 0.64 | 0.29 | |
| Young adults | 3 | 1.35 (0.96–1.90) | 90.40, <0.001 | |||
| Severity of MHDs | Symptoms | 3 | 1.35 (0.96–1.90) | 90.40, <0.001 | 0.29 | |
| Disorders | 5 | 1.69 (1.33–2.14) | 0.00, 0.64 | |||
| Intensity of substance use | Alcohol use | 6 | 1.49 (1.26–1.76) | 0.00, 0.88 | 0.59 | |
| AUD 3 | 5 | 1.71 (1.05–2.79) | 83.88, <0.001 | |||
| Anxiety and Cannabis use | Point Estimate | Crude | 2 | 1.26 (0.93–1.71) | 0.00, 0.76 | 0.19 |
| Adjusted | 2 | 2.28 (1.00–5.20) | 5.37, 0.30 | |||
| Target Population | Adolescents | 3 | 1.71 (1.02–2.89) | 0.00, 0.38 | 0.29 | |
| Young adults | 1 | 1.23 (0.88–1.73) | n/a | |||
| Severity of MHDs | n/a | |||||
| Intensity of substance use | Cannabis use | 1 | 1.23 (0.88–1.73) | n/a | 0.29 | |
| CUD | 3 | 1.71 (1.02–2.89) | 0.00, 0.38 | |||
| Anxiety and Tobacco use | Point Estimate | Crude | 1 | 1.78 (1.42–2.22) | n/a | 0.14 |
| Adjusted | 3 | 2.67 (1.62–4.37) | 33.125, 0.22 | |||
| Target Population | n/a | |||||
| Severity of MHDs | n/a | |||||
| Intensity of substance use | Ever | 3 | 1.62 (0.67–3.92) | 69.87, 0.04 | 0.58 | |
| Current | 4 | 2.10 (1.69–2.62) | 0.00, 0.52 | |||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Esmaeelzadeh, S.; Moraros, J.; Thorpe, L.; Bird, Y. Examining the Association and Directionality between Mental Health Disorders and Substance Use among Adolescents and Young Adults in the U.S. and Canada—A Systematic Review and Meta-Analysis. J. Clin. Med. 2018, 7, 543. https://doi.org/10.3390/jcm7120543
Esmaeelzadeh S, Moraros J, Thorpe L, Bird Y. Examining the Association and Directionality between Mental Health Disorders and Substance Use among Adolescents and Young Adults in the U.S. and Canada—A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2018; 7(12):543. https://doi.org/10.3390/jcm7120543
Chicago/Turabian StyleEsmaeelzadeh, Sarvenaz, John Moraros, Lilian Thorpe, and Yelena Bird. 2018. "Examining the Association and Directionality between Mental Health Disorders and Substance Use among Adolescents and Young Adults in the U.S. and Canada—A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 7, no. 12: 543. https://doi.org/10.3390/jcm7120543
APA StyleEsmaeelzadeh, S., Moraros, J., Thorpe, L., & Bird, Y. (2018). Examining the Association and Directionality between Mental Health Disorders and Substance Use among Adolescents and Young Adults in the U.S. and Canada—A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 7(12), 543. https://doi.org/10.3390/jcm7120543