1. Introduction
The health-related quality of life (H-QOL) is a patient-centered clinical outcome that is used internationally for patients with various diseases, including diabetes mellitus, and cardiovascular diseases, renal diseases and malignancies [
1,
2,
3,
4]. Chronic liver diseases (CLDs) can also affect H-QOL [
5,
6,
7,
8,
9]. Due to the adverse clinical and patient-reported outcomes, and the economic burden of CLDs, improving H-QOL in patients with CLDs should be a major treatment goal [
5,
6,
7,
8,
9]. A previous study reported that higher H-QOL was associated with favorable clinical outcome in patients with CLDs and increasing the number of pivotal clinical trials have adopted H-QOL as additional study endpoints [
10,
11]. The most extensively used assessment methods for H-QOL is the 36-Item Short Form Health Survey (SF-36) [
12,
13,
14,
15,
16].
Skeletal muscle mass (SMM) increases till 20 years, peaks between 20 and 50 years, and decreases by approximately 1% after the age of 50 years, due to changes in muscle fiber type and size [
17]. Sarcopenia is a clinical disease entity that is defined by diminished muscle function and SMM [
18,
19,
20,
21,
22,
23,
24,
25,
26,
27,
28]. It can be associated with worse clinical outcomes and higher health care costs in various diseases, and there is therefore urgent need for the establishment of methods for improving sarcopenia [
18,
19,
20,
21,
22,
23,
24,
25,
26,
27,
28]. This also applies to CLD patients [
19,
21,
23]. Sarcopenia is the main component of malnutrition, and it is primarily responsible for the unfavorable clinical consequences that are observed in CLD patients [
19,
21,
23]. Liver cirrhosis (LC) can easily complicate sarcopenia, due to impaired protein synthesis [
19]. Currently, the Japanese Society of Hepatology (JSH) reported that the original criteria for sarcopenia in liver diseases, with reference to the Asian criteria for sarcopenia [
18,
22]. The JSH criteria use hand grip strength (HGS) for muscle strength assessment, and bioimpedance analysis (BIA) and/or computed tomography for muscle mass assessment, while unlike the Asian criteria for sarcopenia, there is no age restriction for the assessment of sarcopenia in the JSH criteria, because younger patients with severe advanced CLDs such as liver failure are likely to be involved in sarcopenia [
18].
However, as far as we are aware, scarce data regarding the relevance between H-QOL and HGS and SMM in CLD patients are currently available, although there are several reports where it is not diminished SMM, but diminished muscle strength, that is related to the weakness of physical function in patients with diabetes-related dementia, and that HGS is an important correlate of health in breast cancer survivors [
29,
30]. We hypothesized that HGS rather than SMM may affect H-QOL in CLD patients. To clarify these clinical research questions, we primarily sought to examine the influence of HGS and SMM on H-QOL, as evaluated by the SF-36 questionnaire, as compared with other clinical data (liver functional data, nutritional data, etc.) in patients with CLDs.
3. Results
3.1. Patient Baseline Data
Baseline data in this study (
n = 389, 198 men and 191 women, average age = 62.0 years) are indicated in
Table 1. LC was found in 148 patients (38.0%). The average ± SD HGS and SMI in male patients were 33.6 ± 8.7 kg and 7.5 ± 1.1 kg/m
2, respectively, and those in female patients were 20.9 ± 5.2 kg and 6.0 ± 0.7 kg/m
2, respectively. Sarcopenia, as defined by the JSH criteria, was observed in 27 male patients (13.6%) and 34 female patients (17.8%) [
18]. In LC patients, sarcopenia was identified in 39 patients (26.4%), while in non-LC patients, it was identified in 22 patients (9.1%).
Between-group differences (the d-HGS group (
n = 93) vs. the non-decreased HGS (nd-HGS) group (
n = 296)) were noted with statistical significance in age, gender, presence of LC, serum albumin, platelet count, lymphocyte count, total cholesterol, CONUT score, FIB-4 index, and SMI (both male and female). While in the d-SMM group (
n = 159) vs. the non-decreased SMI (nd-SMM) group (
n = 230), between-group differences in age, gender, body mass index (BMI), FIB-4 index, serum creatinine, and HGS (both male and female) reached significance. The corresponding average ± SD values and
p values are listed in
Table 1.
Between-group differences (LC patients (
n = 148) vs. non-LC patients (
n = 151)) were noted with statistical significance in the items of PF, RP, GH, VT, SF, RE, and PCS, suggesting that LC patients had poorer H-QOL compared with non-LC patients. Corresponding average ± SD values, 95% confidence intervals (CIs) and
P values were summarized in
Table 2.
3.2. Impact of HGS and SMM on the SF-36 Scores for all Cases
The average ± SD SF-36 scores (95% CIs) in the d-HGS and nd-HGS groups (
n = 93 and 296), and the d-SMM and nd-SMM groups (
n = 159 and 230) for all cases are presented in
Table 3. Between-group differences (the d-HGS group vs. the nd-HGS group) in the items of PF (
p < 0.0001), RP (
p < 0.0001), BP (
p = 0.0043), VT (
p = 0.0011), SF (
p < 0.0001), RE (
p < 0.0001), and PCS (
p < 0.0001) reached significance, while SF-36 scores in the d-SMI group were significantly higher than those in the nd-SMI group in the items of PF (
p = 0.0032), SF (
p = 0.0031) and RE (
p = 0.0030). (
Figure 1a,b).
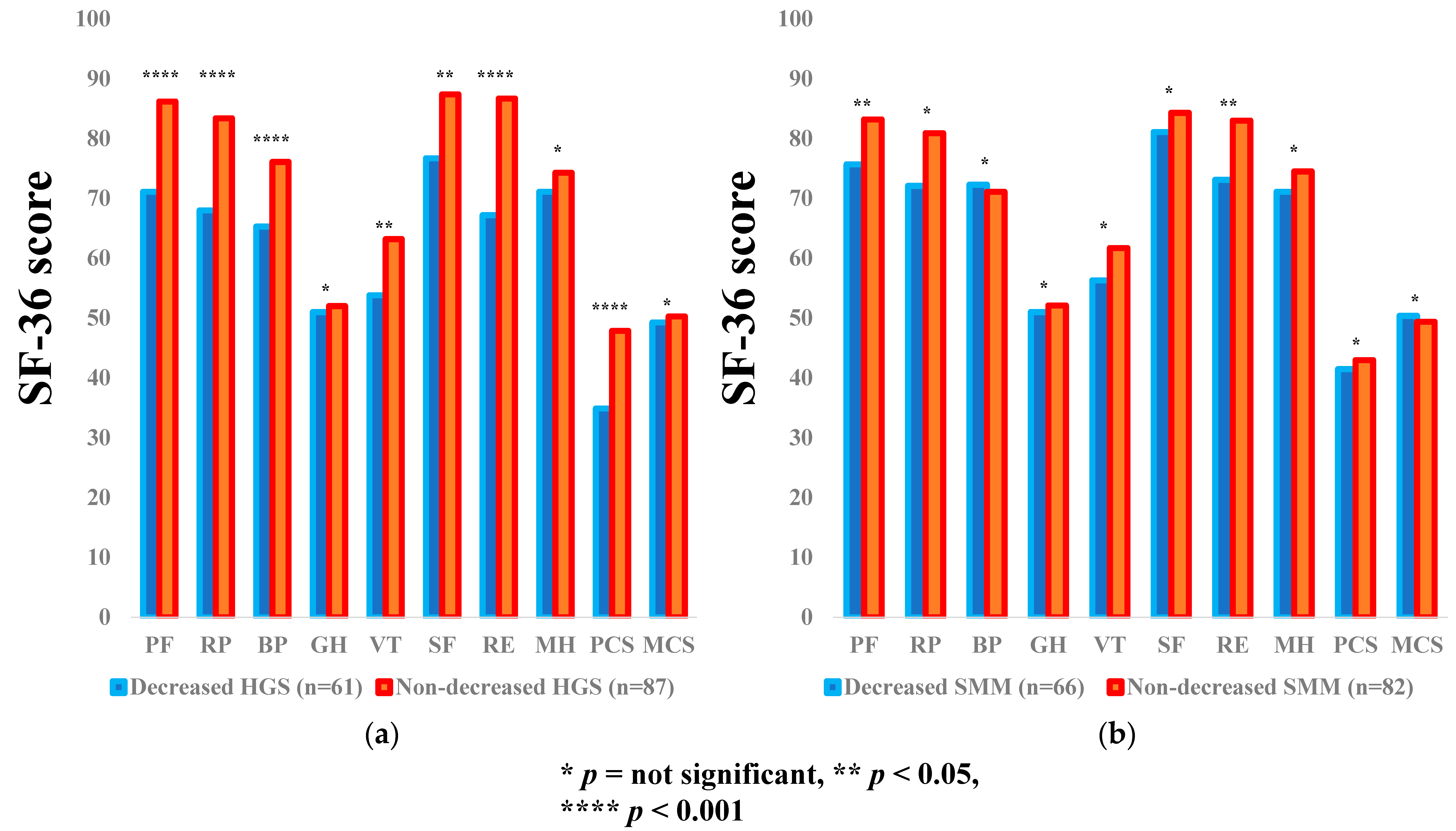
3.3. Subgroup Analysis 1: Impact of HGS and SMM on the SF-36 Scores for LC Patients
The average ± SD SF-36 scores [95% CIs] in the d-HGS and nd-HGS groups (
n = 61 and 87), and the d-SMM and nd-SMM groups (
n = 66 and 82) for LC patients are shown in
Table 3. Between-group differences (the d-HGS group vs. the nd-HGS group) in the items of PF (
p = 0.0002), RP (
p = 0.0006), BP (
p = 0.0002), VT (
p = 0.0132), SF (
p = 0.0112), RE (
p < 0.0001), and PCS (
p < 0.0001) reached significance, while in the d-SMM group vs. the nd-SMI group, the differences were noted with significance in the items of PF (
p = 0.0252) and RE (
p = 0.0131) (
Figure 2a,b).
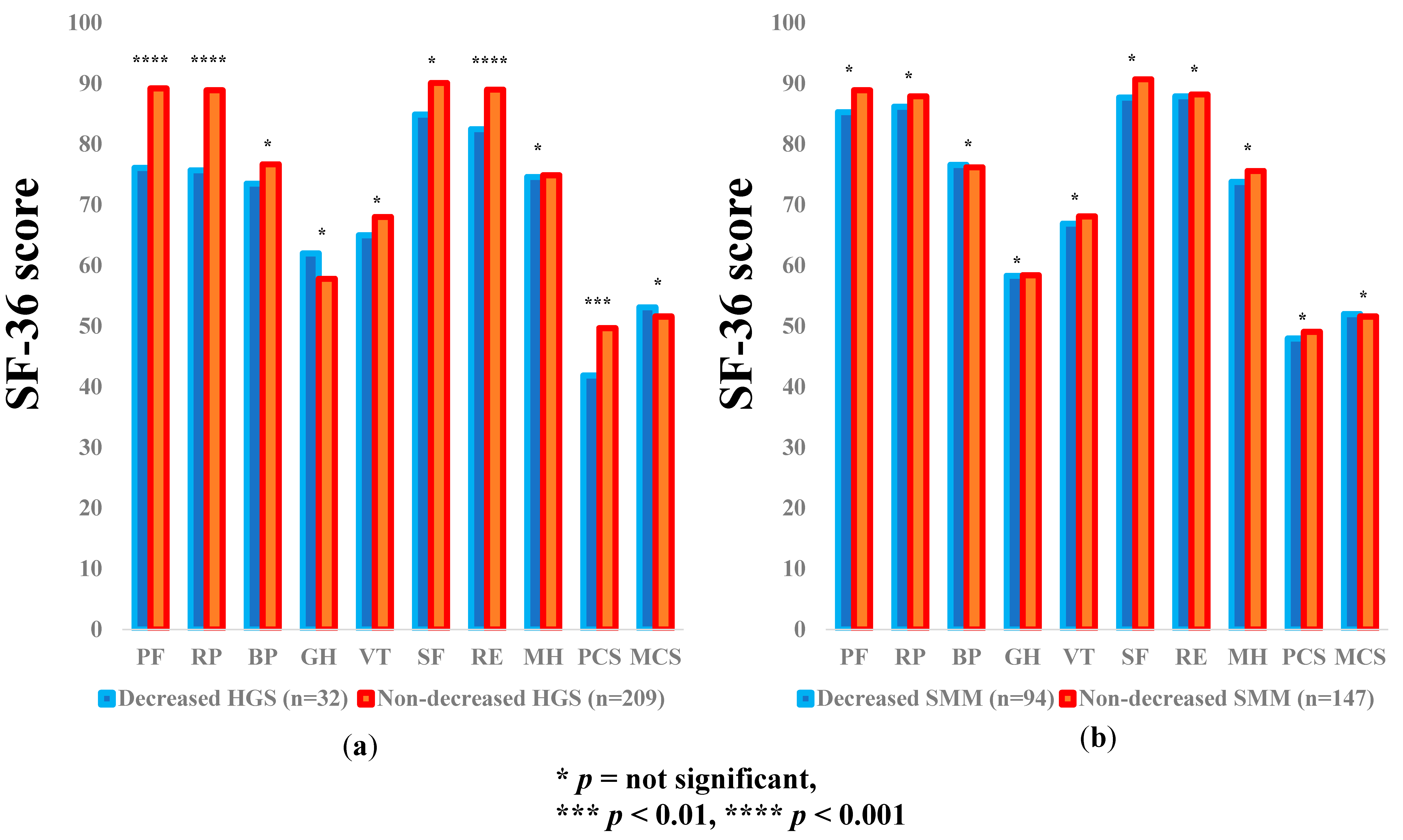
3.4. Subgroup Analysis 2: Impact of HGS and SMM on the SF-36 Scores for Non-LC Patients
The average ± SD SF-36 scores (95% CIs) in the d-HGS and nd-HGS groups (
n = 32 and 209) and the d-SMM and nd-SMM groups (
n = 94 and 147) for non-LC patients are demonstrated in
Table 3. Between-group differences (the d-HGS group vs. the nd-HGS group) in the items of PF (
p = 0.0002), RP (
p = 0.0006), RE (
p = 0.0002), and PCS (
p = 0.0018) reached significance, while in the d-SMM group vs. the nd-SMM group, no significant difference was noted in all items (
Figure 3a,b).
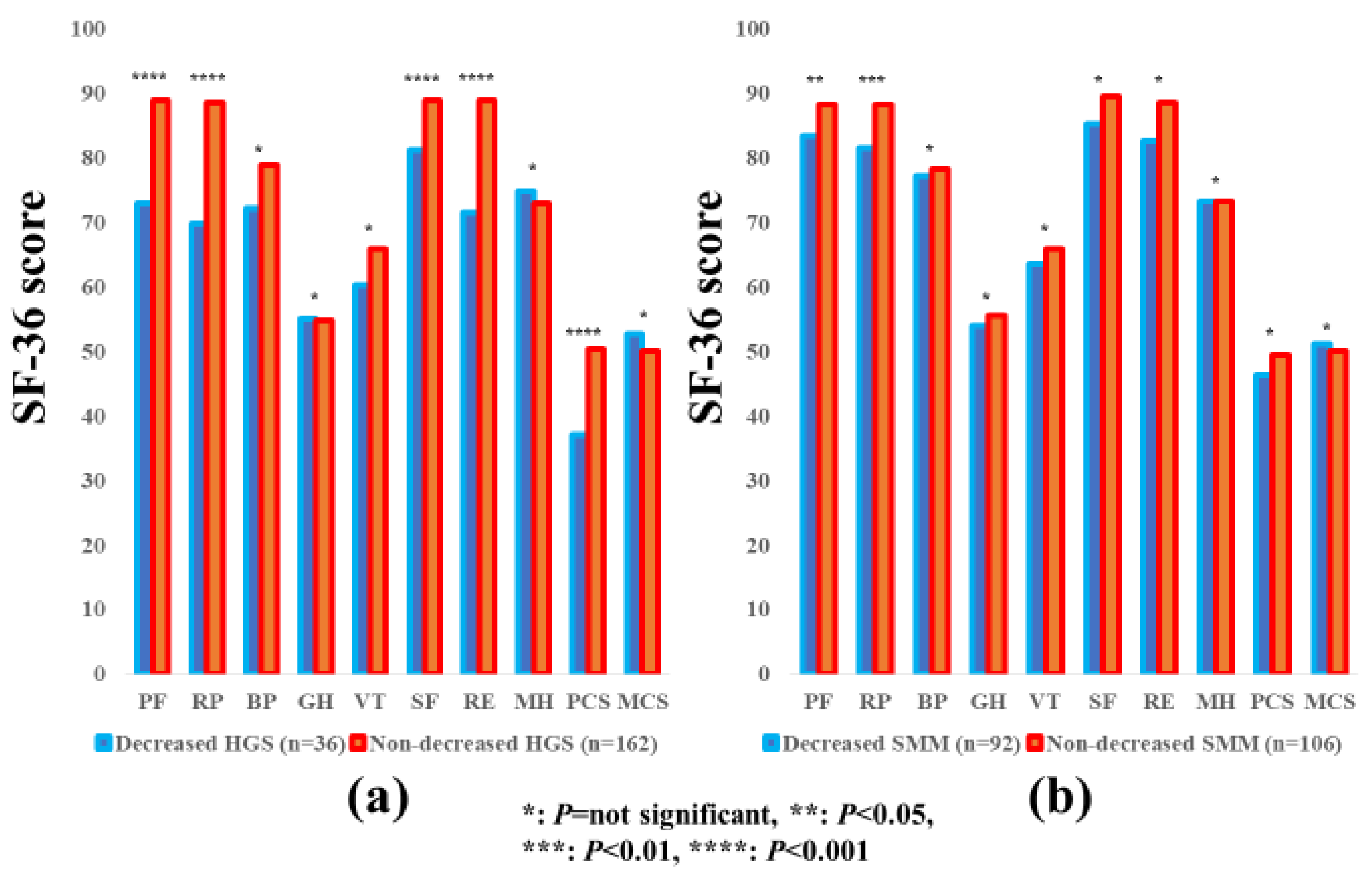
3.5. Subgroup Analysis 3: Impact of HGS and SMM on the SF-36 Scores for Male Patients
The average ± SD SF-36 scores (95% CIs) in the d-HGS and nd-HGS groups (
n = 36 and 162) and the d-SMM and nd-SMM groups (
n = 92 and 106) for male patients are indicated in
Table 3. Between-group differences (the d-HGS group vs. the nd-HGS group) in the items of PF (
p < 0.0001), RP (
p < 0.0001), SF (
p < 0.0001), RE (
p < 0.0001) and PCS (
p < 0.0001) reached significance, while the SF-36 scores in the d-SMM group were significantly higher than those in the nd-SMM group in the items of PF (
p = 0.0451) and RP (
p = 0.0035) (
Figure 4a,b).
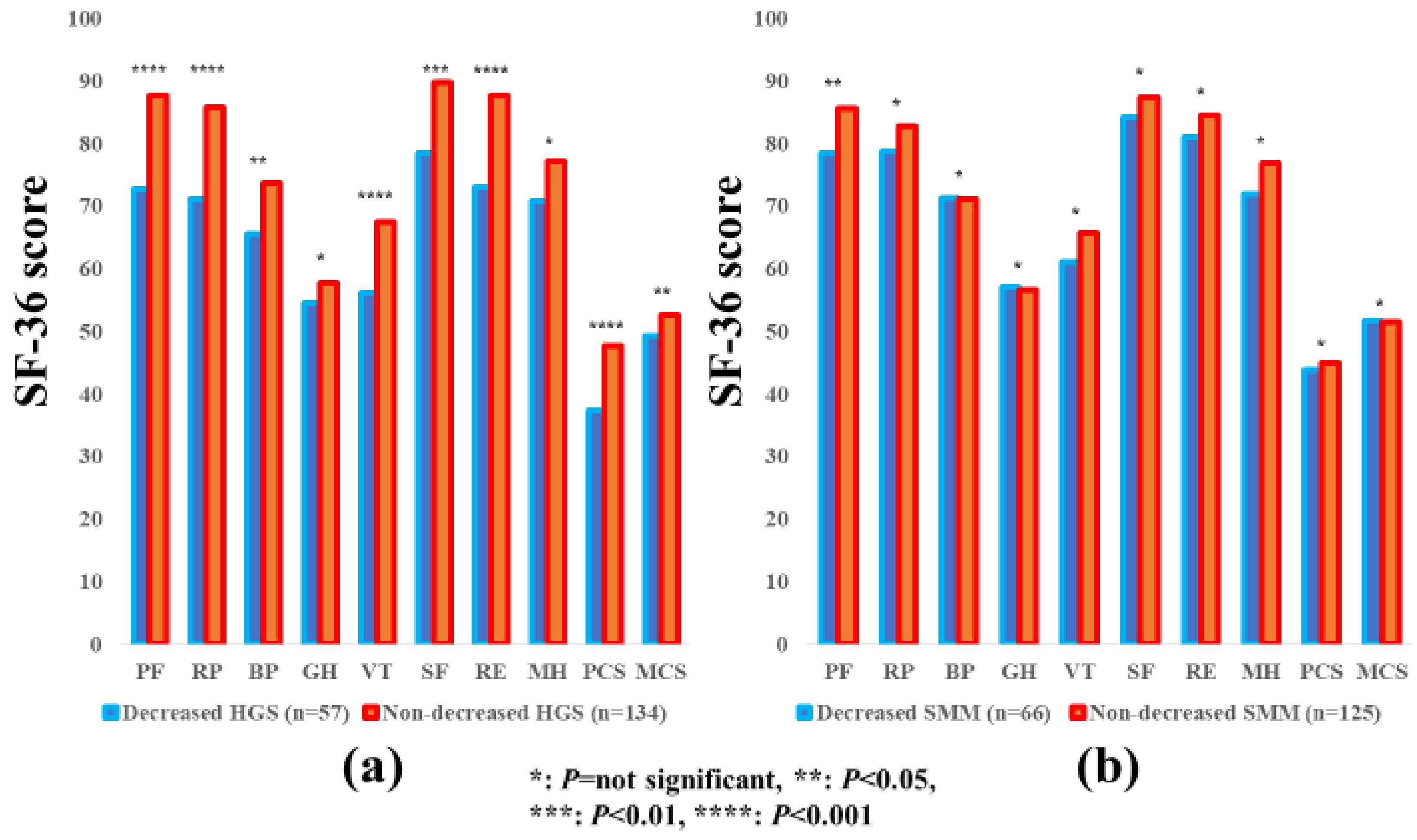
3.6. Subgroup Analysis 4: Impact of HGS and SMM on the SF-36 Scores for Female Patients
The average ± SD SF-36 scores [95% CIs] in the d-HGS and nd-HGS groups (
n = 57 and 134) and the d-SMM and nd-SMM groups (
n = 66 and 125) for female patients are indicated in
Table 3. Between-group differences (the d-HGS group vs. the nd-HGS group) in the items of PF (
p < 0.0001), RP (
p < 0.0001), BP (
p = 0.0432), VT (
p = 0.0006), SF (
p = 0.0012), RE (
p < 0.0001), PCS (
p < 0.0001) and MCS (
p = 0.0326) reached significance, while in the d-SMM group vs. the nd-SMI group, the difference was observed with significance only in the item of PF (
p = 0.0124). (
Figure 5a,b).
3.7. Subgroup Analysis 5: Impact of HGS and SMM on the SF-36 Scores for Patients Aged ≥65 Years
The average ± SD SF-36 scores (95% CIs) in the d-HGS and nd-HGS groups (
n = 74 and 121) and the d-SMM and nd-SMM groups (
n = 110 and 85) for patients aged ≥65 years are indicated in
Table 3. Between-group differences (the d-HGS group vs. the nd-HGS group) in the items of PF (
p = 0.0001), RP (
p < 0.0001), BP (
p = 0.0111), VT (
p = 0.0021), SF (
p < 0.0001), RE (
p < 0.0001), and PCS (
p < 0.0001) reached significance, while in the d-SMM group vs. the nd-SMM group, no significant differences were observed in all items (
Figure 6a,b).
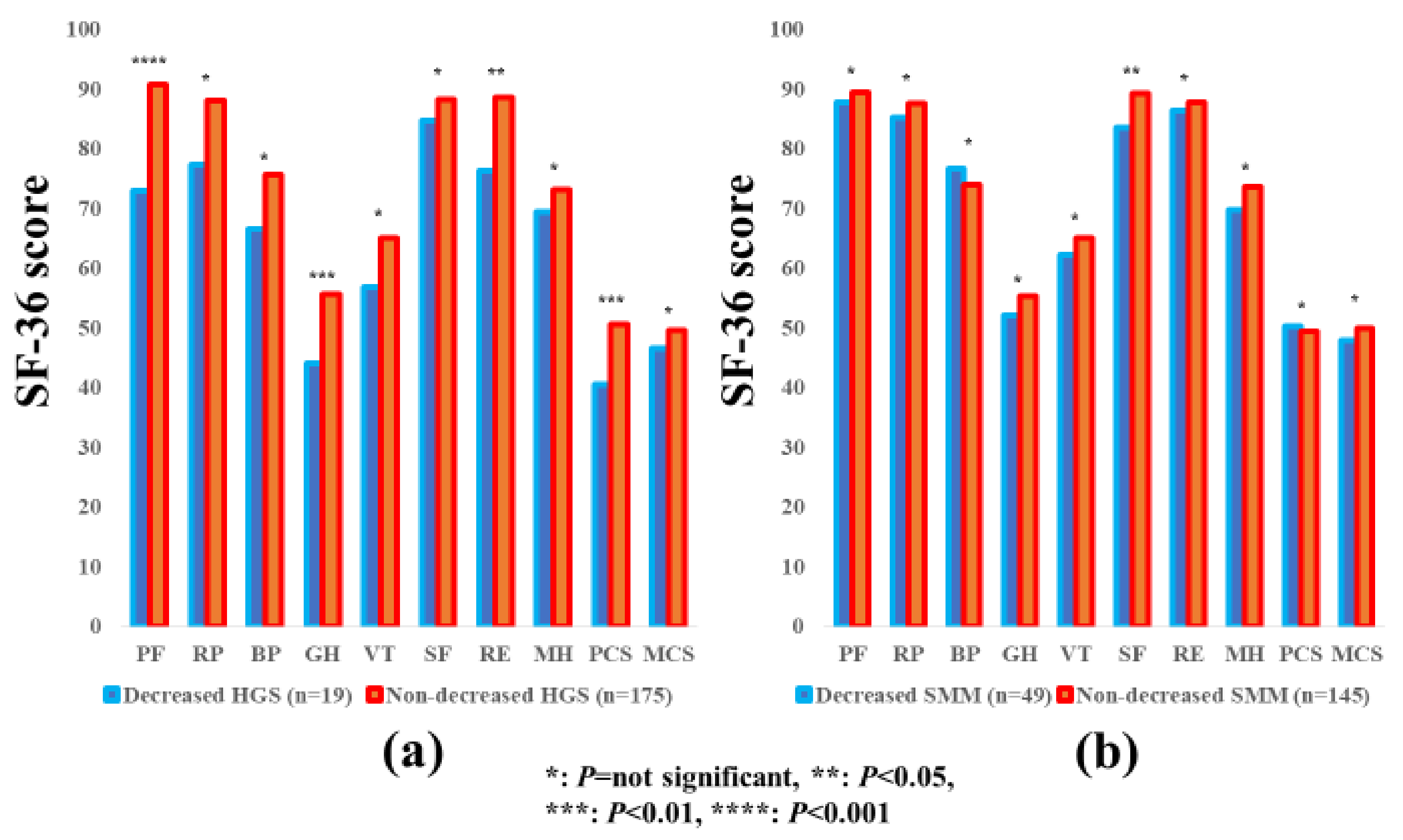
3.8. Subgroup Analysis 6: Impact of HGS and SMM on the SF-36 Scores for Patients Aged <65 Years
The average ± SD SF-36 scores (95% CIs) in the d-HGS and nd-HGS groups (
n = 19 and 175) and the d-SMM and nd-SMM groups (
n = 49 and 145) in patients aged <65 years are indicated in
Table 3. Between-group differences (the d-HGS group vs. the nd-HGS group) in the items of PF (
p < 0.0001), GH (
p = 0.0088), RE (
p = 0.0281), and PCS (
p = 0.0081) reached significance, while in the d-SMM group vs. the nd-SMM group, between-group difference was significant only in the item of SF (
p = 0.0286) (
Figure 7a,b).
3.9. Relationship between the SF-36 Scores and Baseline Parameters in Male Patients and Female Patients
Correlation coefficients and
p values between the SF-36 scores across 10 items, and baseline parameters in male patients and female patients are summarized in
Table 4.
In male patients, HGS significantly correlated with PF (r = 0.32, p < 0.0001), RP (r = 0.25, p = 0.0007), RE (r = 0.16, p = 0.0324), and PCS (r = 0.29, p < 0.0001), while SMI did not significantly correlate with any item. Serum albumin level significantly correlated with all items other than MH and HCS.
In female patients, HGS significantly correlated with PF (r = 0.35, p < 0.0001), RP (r = 0.18, p = 0.0195), VT (r = 0.23, p = 0.0022), SF (r = 0.18, p = 0.0179), RE (r = 0.19, p = 0.0112), MH (r = 0.17, p = 0.0222), PCS (r = 0.28, p = 0.0003), and MCS (r = 0.15, p = 0.0446), whereas SMI significantly correlated with PF only (r = 0.20, p = 0.0053). Serum albumin levels significantly correlated with all items other than MH.
3.10. Multivariate Analyses of Factors Linked to the SF-36 Scores in Male Patients and Female Patients
In male patients, multivariate analyses of factors for the SF-36 scores revealed that HGS was significantly linked to PF (
p = 0.0031), RP (
p = 0.0185) and PCS (
p = 0.0421), while serum albumin was a significant factor for PF (
p = 0.0048), RP (
p = 0.0004), VT (
p = 0.0327), SF (
p = 0.0085), RE (
p = 0.0002) and PCS (
p < 0.0001) (
Table 5).
In female patients, multivariate analyses of factors for the SF-36 scores revealed that HGS was significantly linked to PF (
p = 0.0034), VT (
p = 0.0150), RE (
p = 0.0422), and PCS (
p = 0.0191), whereas serum albumin did not significantly correlate with any item (
Table 5).
4. Discussion
The loss of SMM in CLDs is caused by the progressive withdrawal of anabolism, and an increase in catabolism [
34]. The liver is an essential organ that is involved in protein, fat, and carbohydrate metabolism, and energy generation [
35,
36]. H-QOL in CLDs has been demonstrated to be significantly compromised, and the decrease in H-QOL in CLDs is frequently overlooked or unrecognized [
37]. To our knowledge, this is the first study demonstrating the relevance between HGS and SMM and H-QOL in CLD patients. To elucidate these issues is clinically of importance, because sarcopenia in liver diseases has been gaining much attention these days, due to its high prognostic predictability, and its definition includes HGS and SMM [
18,
19,
20,
21,
22,
23,
24,
25,
26,
27,
28]. We therefore conducted the current analysis.
In our results, mean values in the d-HGS and nd-HGS groups were largely different, with statistical significance in the items of PF and PCS for all cases and all subgroup analyses, while in comparison, between the d-SMM and nd-SMM groups, such tendencies were not observed. Additionally, our multivariate analyses revealed that HGS was an independent predictor associated with PF and PCS irrespective of gender; however, in terms of mentality-related domains such as MH or MCS, both HGS and SMI appeared not to have an impact on the SF-36 scores. These results demonstrated that not SMM, but HGS has a strong influence on the physiological domains in the SF-36, which may be linked to clinical outcomes in CLD patients [
11]. Numerous previous studies have reported that SMM is an independent outcome predictor in CLD patients [
18,
19,
21,
23,
25,
26]. However, reviewing our current results, decreased SMM itself is not possibly a prognostic factor, but the presence of a large number of patients with diminished muscle strength in diminished SMM patients leads to poor prognosis. Our data showing that SMI was significantly correlated with HGS, both in males (
r = 0.37,
p < 0.0001) and females (
r = 0.46,
p < 0.0001), support this hypothesis. In this respect, the current results seem to shed some insights on the better understanding of muscle mass and muscle weakness in CLD patients.
Notably, as presented in
Table 1, age affected both HGS and SMI, while the presence of LC, serum albumin, and the CONUT score affected only HGS, and BMI affected only SMM. As described above, SMM decreases by approximately 1% after the age of 50 years, owing to changes in muscle fiber type and size [
17]. These morphological and functional changes of skeletal muscle due to aging appear to account for the impact of aging on HGS and SMM. On the other hand, our current results denoted that d-SMM does not occur by poor nutritional state alone, and d-HGS does not occur by lower BMI alone, although the mechanisms for these remains unclear. In our comparison of the SF-36 scores across 10 items in patients with and without LC, significant differences were noted in numerous items, which are in agreement with previous reports [
19,
21,
38,
39]. LC patients tend to have worse H-QOL and exercise training can be a pivotal recommendation for LC patients [
38]. While there have been few reports regarding H-QOL in non-LC patients. In that sense, our data are worthy of report.
In our multivariate analyses, serum albumin was an independent factor in several items of the SF-36 in male patients, while in female patients, serum albumin was not significant in any item of the SF-36. The average ± SD serum albumin levels in male and female in this study were 4.1 ± 0.53 g/dL and 4.2 ± 0.47 g/dL (
p = 0.4726). Gender differences of hormones, including estrogen and progesterone or physiological and psychological attributes of men and women, may be attributed to our current results, however, it is likely that the ability of protein synthesis is associated with H-QOL in male CLD patients [
40,
41]. In our previous investigation, we have reported that serum levels of myostatin, which is a negative regulator of muscle protein synthesis, significantly differed in male and female LC patients [
23].
The proportions of sarcopenia in LC and non-LC patients were 26.4% and 9.1%, respectively, in this study. Sarcopenia includes primary and secondary sarcopenia [
18]. LC patients may have secondary sarcopenia due to impaired protein synthesis, and non-LC patients may have aging-related primary sarcopenia [
18]. Clinicians should fully consider the etiology for sarcopenia in each patient.
Several limitations related to the study warrant mention. Firstly, the study was a single-center observational study with a retrospective nature. Secondly, the study data was derived from a Japanese liver disease population data, and additional investigations on other races are required to further verify and extend the application to other races. Thirdly, HGS can vary depending on patients’ daily life activities. Fourthly, patients with massive ascites or hepatic encephalopathy, who are potentially involved in sarcopenia were excluded, due to the lack of reliability in the BIA or the self-reported questionnaire, creating bias. Finally, the interpretation of our results should be done cautiously, since the direction of the association between the SF-36 scores and HGS or SMM remains unclear, due to the cross-sectional nature of our data. Nevertheless, our study results denoted that patients with d-HGS scored lower in the SF-36 vs. those with nd-HGS, especially in the physical health domains. In conclusion, HGS appears to have a strong impact on H-QOL in patients with CLDs, and exercise may be beneficial for improving H-QOL. In CLD patients with d-HGS, clinicians should be aware of the presence of CLD patients with decreased H-QOL.









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}