1. Introduction
Imperforate hymen (IH) is an uncommon congenital anomaly of the female genital tract, in which the hymen completely obstructs the vaginal opening, with an approximate incidence of 0.05–0.1% [
1,
2]. IH obstructs uterine and vaginal secretions (also called hematocolpos), causing amenorrhea and cyclic pelvic pain [
2]. IH may be associated with other developmental anomalies [
3], but some reports propose that it is not generally related to Müllerian anomalies, and evaluating urogenital anomalies is unnecessary [
4]. There have been rare cases of familial IH occurrence; most cases are thought to occur sporadically and no genetic mutations have been identified [
5].
IH is often diagnosed in adolescent girls after menarche, mainly presenting with amenorrhea and lower abdominal pain or urinary retention [
6]. Most young girls with IH are asymptomatic and diagnosed incidentally until menarche. Rarely, however, especially in newborns, the fetus’ secretion by maternal estrogen may cause hydrocolpos and hydrometrocolpos, presenting as abdominal mass in 0.006% of female neonates [
7].
IH can be diagnosed by inspecting the external genitalia, which presents a bulging, bluish hymenal membrane [
1], but an abdominal ultrasound may accurately show a pelvic cystic mass [
1]. Although IH is a benign congenital disorder, late detection and diagnosis may result in severe morbidity and requirement of additional interventions [
2]. Without proper management, IH can cause infections, subfertility, endometriosis, or hydronephrosis and renal failure in rare cases [
8]. The treatment of choice is based on cruciate incision or excision of the hymen [
1]. In contrast to hymenectomy with X, T, cross, or crucial incision, and resection of excess tissues, hymen-preserving surgeries, such as a simple vertical incision and annular hymenotomy, can be an option for patients desiring virginity [
9,
10]. Alternative treatments include a carbon dioxide laser or insertion of a Foley catheter [
11,
12].
Despite the simple diagnosis and treatment of IH, missed/delayed diagnosis is a critical issue owing to low incidence, nonspecific symptoms, or insufficient physical examination. Therefore, when adolescent girls present with abdominal pain or acute urinary retention, clinicians must suspect IH and conduct thorough abdominal and gynecological examinations.
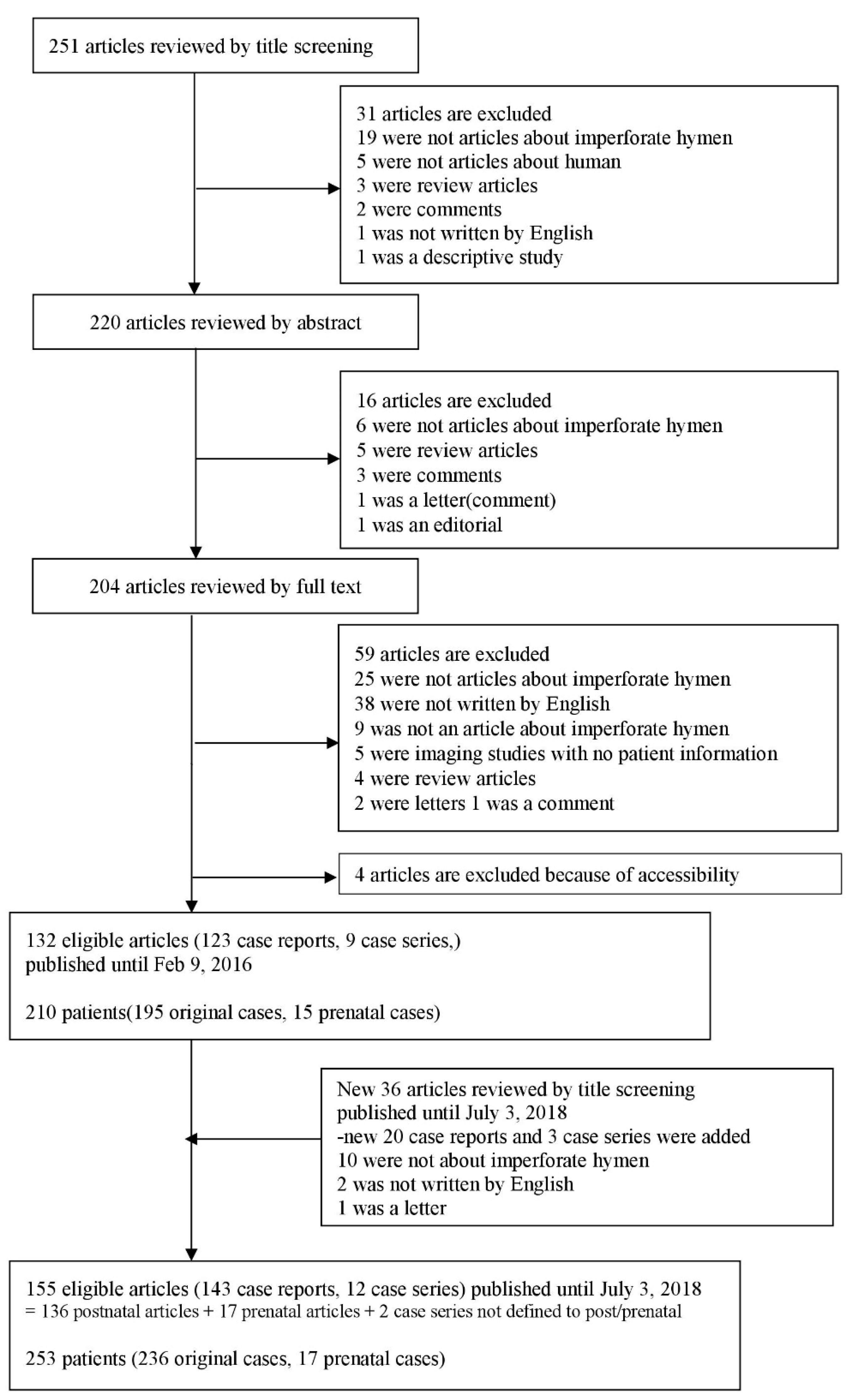
Although there have been many case reviews and reports, no systematic review on IH has been reported. Therefore, we searched 253 cases of IH and reviewed the epidemiology, symptoms, treatment options, and clinical outcomes. We also aimed to raise awareness among clinicians by discussing several cases of IH with severe complications.
4. Discussion
The hymen is the junction of the urogenital sinus and the sinovaginal bulbs. In embryonic stages, the hymen is perforated to make a connection between the vestibule and the vaginal canal. If this stage fails, individuals are born with IH [
15,
16]. IH is a rare disease, with an estimated incidence rate of 0.05%–0.1% [
17]. Generally, this rare congenital anomaly is diagnosed during adolescence after menarche, presenting with abdominal pain and amenorrhea. IH does not present itself as an abdominal mass during the perinatal period [
15], and most patients with IH are asymptomatic and not diagnosed until menarche. Our study also showed that among 253 patients included in the reviewed articles, 236 patients were diagnosed after birth and only 17 (6.7%) were diagnosed during their prenatal period. Early diagnosis was missed in the remaining patients. Most patients presented with abdominal pain (54.2%) and many patients had urinary retention (20.3%), abnormal menstruation (
n = 33, 14%), dysuria (9.7%), and urinary frequency (
n = 12, 5.1%).
Delayed diagnosis is mainly associated with the asymptomatic period for a long time as it is painless during the accumulation of menstrual blood. IH is a rare disease that may not be detected until the onset of menses, when the accumulation of menstrual blood in the uterus and vagina (called hematocolpos) develops symptoms resulting from its mechanical effect on the bladder and urethra [
18,
19,
20]. If left untreated, this condition can also cause obstructive urinary symptoms, constipation, or dysuria [
9]. However, IH can be detected for diagnosis in adolescent girls with abdominal pain, even before menarche.
In our study, 26 (11.0%) patients were newborns and 72 (30.5%) were under 12 years of age. This indicates that IH can be readily diagnosed by inspecting the external genitalia. If uncertainties remain, ultrasonography or magnetic resonance imaging can help ease the diagnosis [
1]. However, clinicians rarely conduct appropriate physical examinations and take a detailed gynecological history because of the low incidence and nonspecific symptoms of IH. Therefore, diagnosis of IH is missed or delayed in most cases [
6].
Choice of treatment is based on hymenectomy (cruciate incision or excision of hymen) [
8]. Hymen-preserving surgeries, such as simple vertical incision and annular hymenotomy, can be an option for patients desiring virginity [
9,
10]. Alternative treatments include carbon dioxide laser or insertion of a Foley catheter [
10,
12]. In our study, most patients received surgical therapy (83.5%), most of whom were treated with a hymenotomy (35.2%) or hymenectomy (36.4%). Surgery was the main single treatment option (68.2%); however, 8.1% patients received two kinds of therapies, e.g., a combination of hymenectomy and vaginal septum repair (1.3%). Three patients received three kinds of therapies (1.3%). In cases with a conservative approach, no improvement was observed. There was no difference of improved outcome between hymenotomy and hymenectomy, and use of prophylactic antibiotics were only identified in six patients. Besides, complications such as reclosure, vaginal adenosis, or vaginal adhesion were only noted in 6.6% patients. According to our data (
Table 5) and previous several papers, hymenotomy can be enough for reducing these complications [
9,
18,
21]. Thus, we propose that early diagnosis, detection of IH, and minimal preserving hymen surgery are of importance. Although IH is a benign congenital disorder, it can cause endometriosis, subfertility, infection, or hydronephrosis and renal failure without proper management.
Among patients described in case reports, there were five patients with transverse vaginal septum combined with imperforate hymen [
22,
23,
24,
25,
26] and one patient with uterocervicovaginal septum [
27]. Also, there was one patient who was a neonate at the time of diagnosis with sacral agenesis [
3] not fully separated with an imperforate hymen. However, no case reports described misdiagnosis other diseases as an imperforate hymen. Other gynecological diseases, especially vaginal septum and agenesis, require much more complex care and should not be confused with IH, which is fairly easy to correct and not associated with as many or severe complications such as stricture and ascending infection. Clinicians should always keep in mind both of the possibilities that the IH may have been combined with these diseases and that other diseases have been misidentified as IH.
There are several potential limitations in this review. It can be possible that several studies were not detected although we comprehensively selected researches across multiple databases. In addition, we could only include data on information provided in case reports and series. Due to the characteristics of a systematic review, this article represents a synthesis of the opinions of the authors who wrote the case reports or case series, rather than new concepts or information about this disease.
In conclusion, IH is a rare disease for which early diagnosis is easy to miss. IH can cause acute urinary retention. However, the diagnosis is easy and postsurgical prognosis is good. Therefore, clinicians, especially urologists, gynecologists, or pediatricians, should carefully examine every female patient at birth. Even when the detection is delayed until adolescence, IH should be considered a possibility in patients who complain of abdominal pain, lower back pain, or urinary retention, and assessed by conducting prompt and appropriate physical examinations of the genital introitus. Moreover, it is important to diagnose IH accurately by not misdiagnosing it as vaginal septum or agenesis to prevent severe complications of wrong treatment. Further prospective and bigger studies would be necessary addressing the issue of the specificity of the outcome according to the each treatment in the future.

 ,
, 

{kind=link}