1. Introduction
Disseminated intravascular coagulation (DIC) is a catastrophic systemic disorder of coagulation, resulting in uncontrollable bleeding, multiple organ failure (MOF) and death. It can be caused by various medical conditions including sepsis, trauma, cancers, obstetrical complications, vascular disorders, toxins, immunologic disorders, and inflammations [
1]. Excessive thrombin production triggered by overexpressed tissue factor associated with inflammation, activated monocytes, and vascular lesion ignites the explosive chain reaction in platelet activation, consumption of natural coagulation inhibitors, and inhibition of fibrinolysis, leading to a hypercoagulable state, deposition of fibrin in micro vessels, and hemorrhage [
2].
Bacterial infections are most frequently associated with the development of DIC. Clinically overt DIC may occur in up to 50% of patients with sepsis associated with gram-negative bacteria [
1]. The mortality of sepsis complicated with DIC might be significantly higher than sepsis without DIC [
3]. Therefore, it is medically relevant to manage DIC in patients with sepsis. International and Japanese guidelines for the treatment of DIC state that treatment of underlying diseases is the most effective way to reverse this catastrophic coagulation disorder [
4,
5,
6]. However, there are some discrepancies between the Japanese DIC management guidelines and other guidelines mainly regarding supportive adjunctive treatments aiming at coagulation disorders. The use of soluble human recombinant thrombomodulin is one of those discrepancies [
7]. Human thrombomodulin binds to thrombin to form a complex that inhibits thrombin activity, which converts protein C into its activated form allowing it to blind to surface receptors of vascular endothelial cells. Activated protein C plays an important role in suppressing coagulation and inflammatory systems [
8].
The effects of human soluble recombinant thrombomodulin, ART-123, in the treatment of DIC have been examined in several clinical trials. In a phase III, randomized, double-blind study, ART-123 reduced the bleeding events in patients with DIC-associated hematological malignancy or infectious diseases compared to treatment with heparin [
9]. However, the sub-analysis of this clinical trial did not show the efficacy of ART-123 in the DIC associated with infectious diseases [
10]. In a phase IIb, international, double-blind, randomized, placebo-controlled trial, the efficacy of ART-123 was tested on 371 septic patients with suspected DIC defined by impaired platelet count and prolonged prothrombin time based upon the DIC score by the International Society on Thrombosis and Hemostasis (ISTH). They concluded that ART-123 did not cause any adverse events, but there were no significant differences in 28-day mortality between ART-123 and placebo groups [
11]. The Sepsis Coagulopathy Asahi Recombinant LE Thrombomodulin (SCARLET) randomized clinical trial, an expanded phase III clinical trial of the phase IIb study, also failed to show the improvement of thrombomodulin in the 28-day all-cause mortality in the treatment of sepsis-associated DIC [
12]. On the contrary, recent retrospective observational studies in Japan claimed that ART-123 might be beneficial to treat sepsis-induced DIC in patients with severe coagulopathy [
13] or severe respiratory failure [
14].
Although ART-123 has been widely used as an adjunctive therapy in Japan, it is still unclear whether it is truly effective in improving the outcome of DIC. It is difficult to interpret the results in previous clinical trials due to different study designs: prospective or retrospective; different control groups (no optional treatments or heparin); different diagnostic criteria (ISTH or Japanese Association for Acute Medicine (JAAM)); and different parameters to evaluate outcomes (bleeding, DIC score, or mortality) [
3,
9,
11,
14,
15]. Thus, we propose that more data needs to be collected and evaluated in Japanese populations who might have originated from East Asia. In this prospective, randomized, placebo-controlled study, we investigated the effects of ART-123 in the treatment of Japanese patients with DIC associated with infectious systemic inflammatory response syndrome (SIRS) including surgical treatments at our emergency center in the past eight years.
4. Discussion
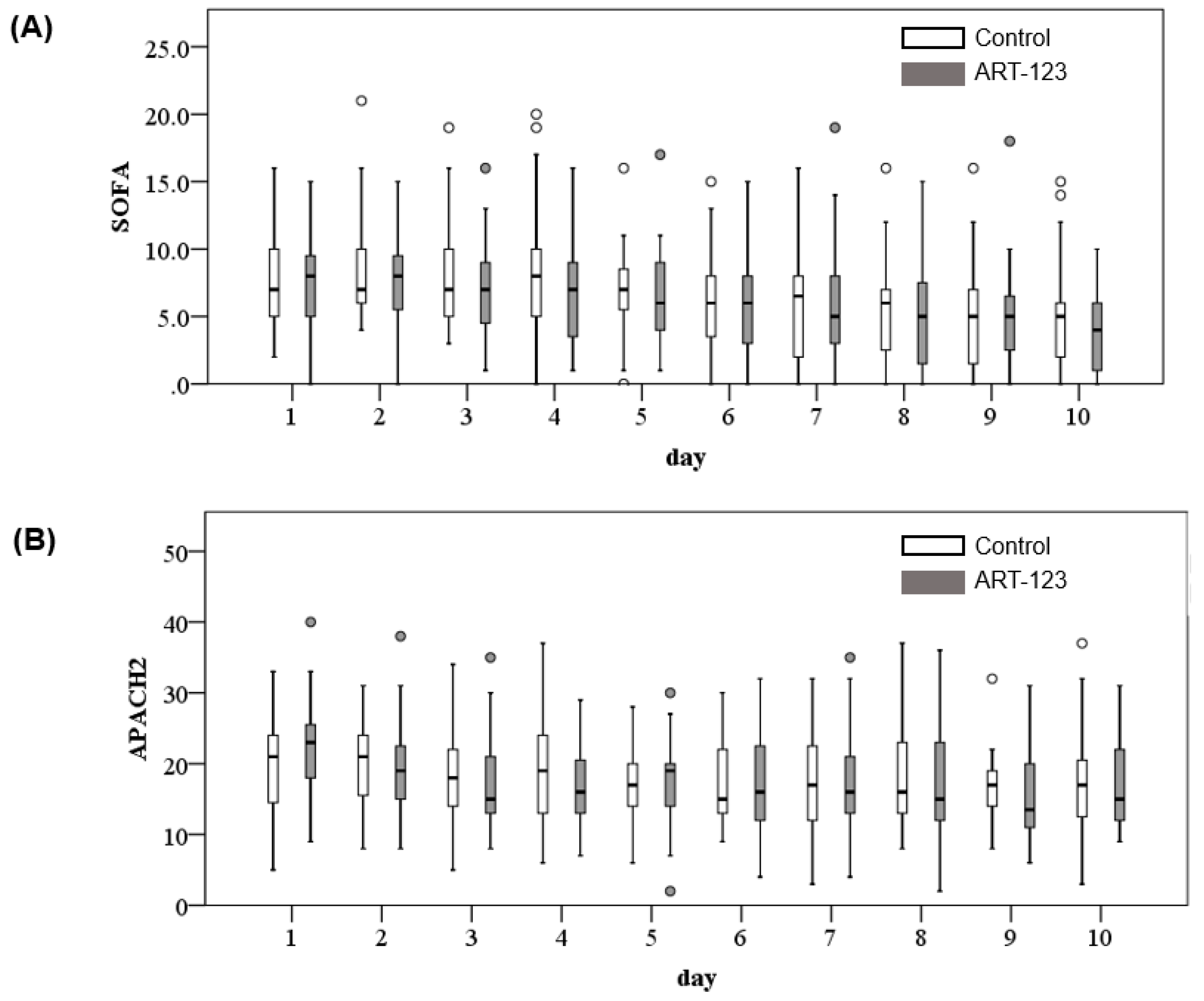
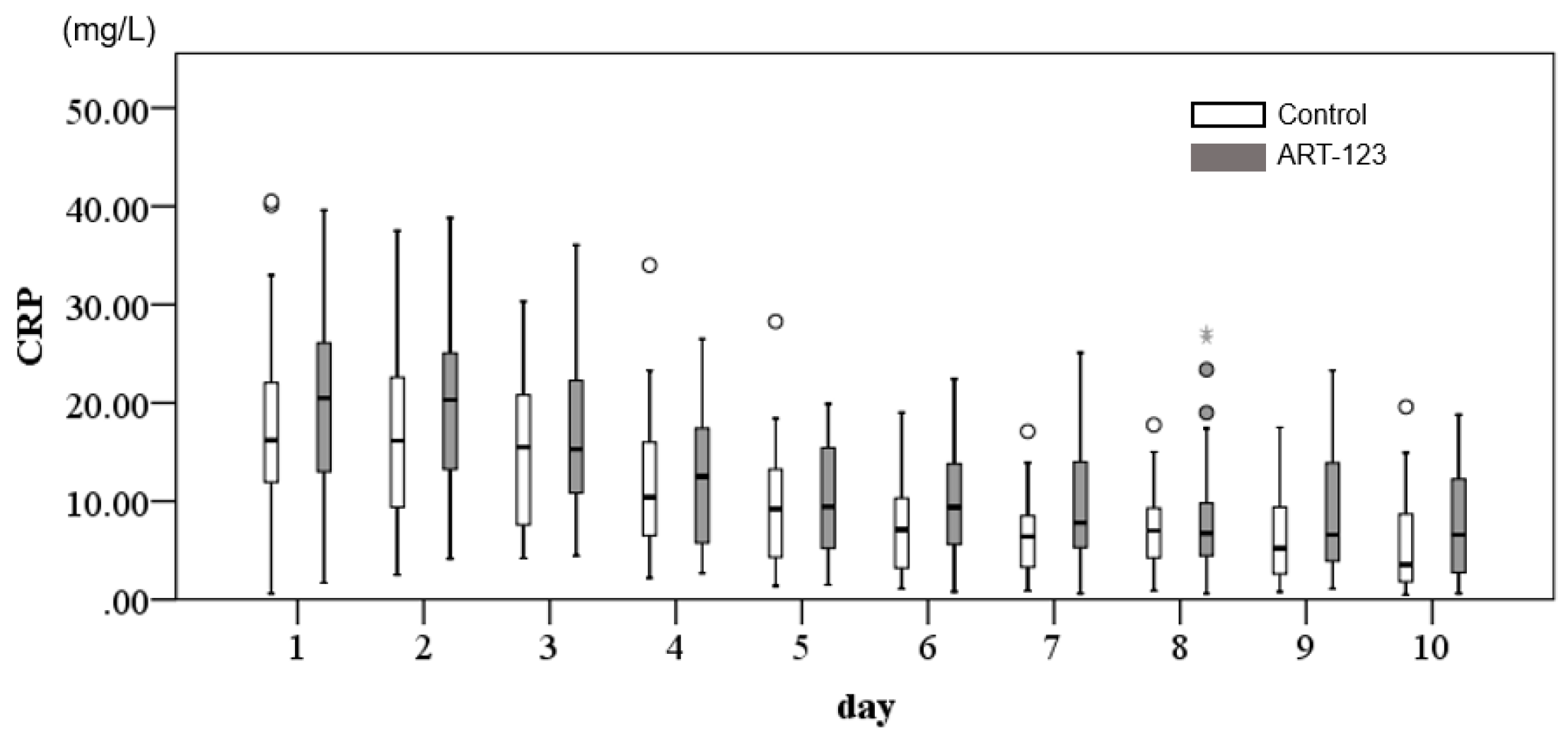
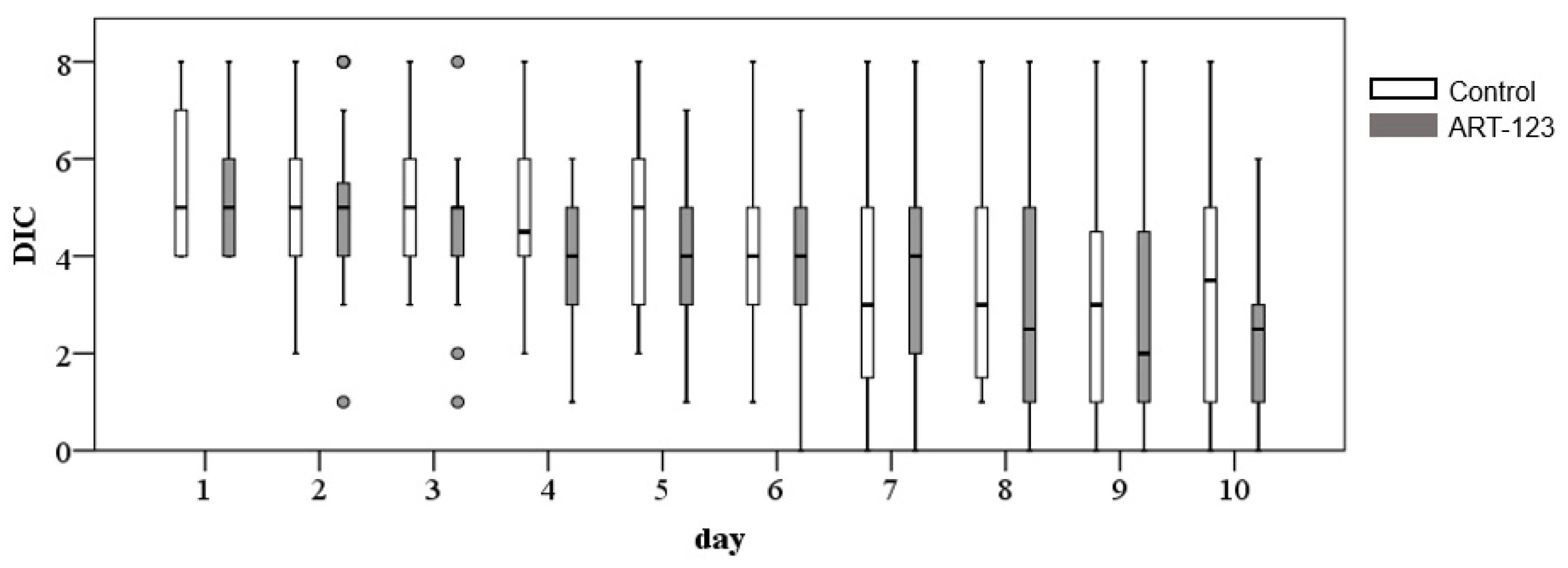
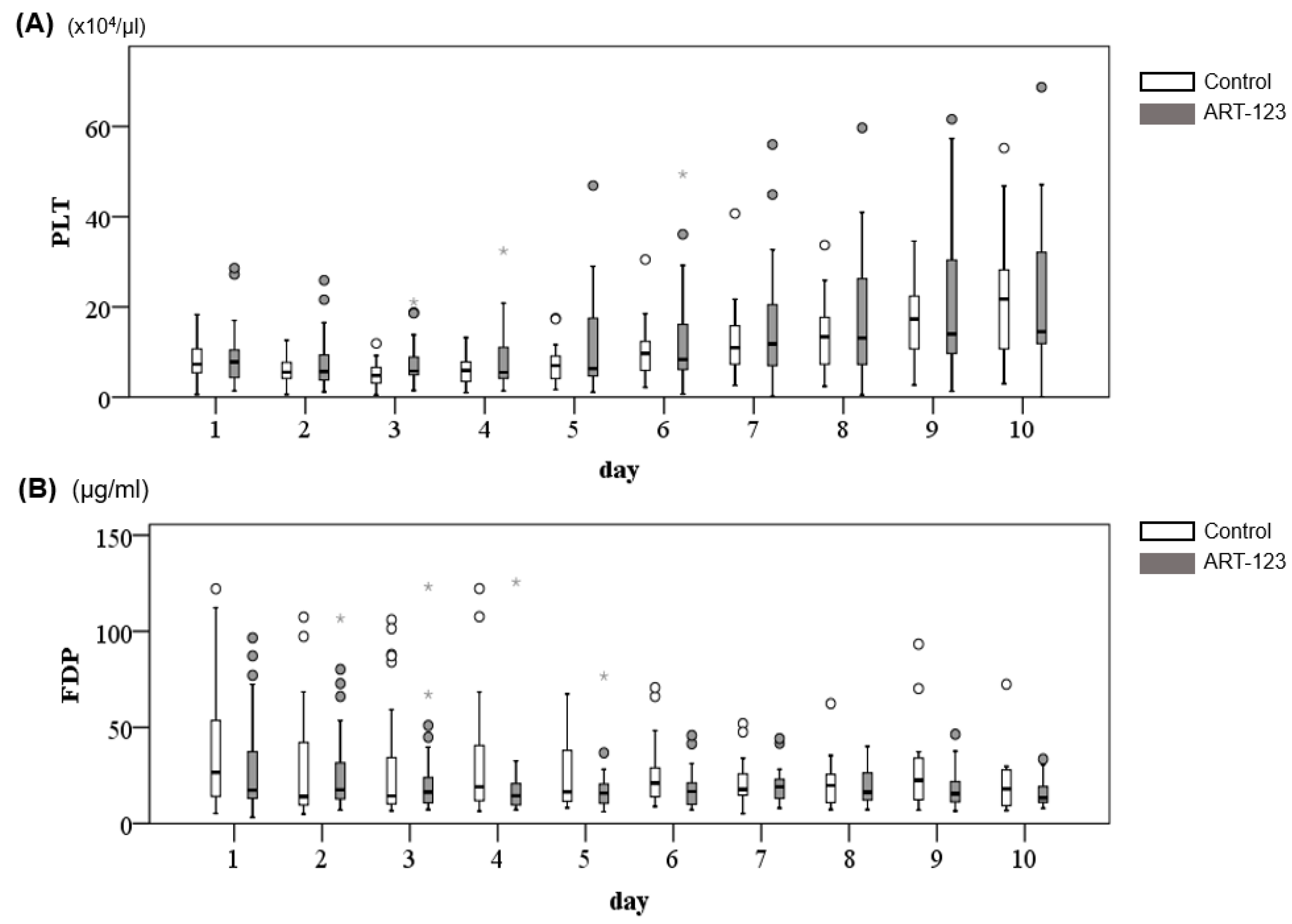
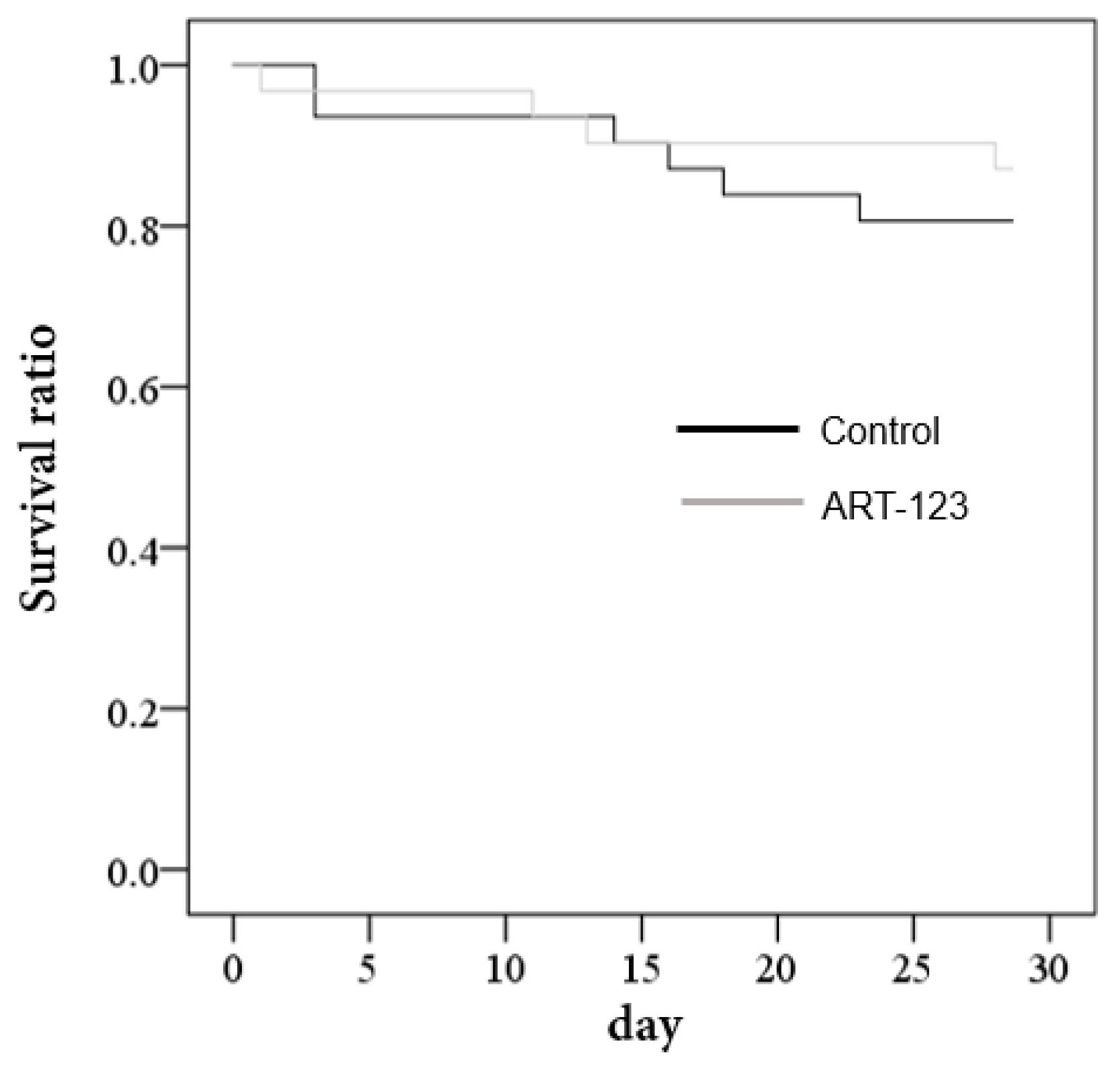
This study is one of the few prospective, randomized, placebo-controlled studies to investigate the effects of human recombinant thrombomodulin, ART-123, in the treatment of DIC associated with infectious systemic inflammatory response syndrome (SIRS). A total of 60 patients who presented SIRS-associated DIC were randomly assigned to ART-123 (n = 29) or the placebo group (n = 31), and clinical outcomes were compared between the two groups. Our data demonstrated that ART-123 did not significantly improve the mortality at 28 hospital-days although the DIC score was resolved a few days earlier in the treated group than the placebo group.
The pathology of DIC has been known since the 1990s [
1], and, to date, there is a consensus that treatment of underlying diseases is the most effective way to resolve DIC without any additional treatments [
2,
7]. However, in reality, additional available therapies such as blood transfusion, fresh frozen plasma, anticoagulants, and/or antithrombotics have been used in attempts to control life-threatening bleeding and coagulation disorders even though those treatments might not be meaningful. This dilemma is similar to that of the cardiac arrhythmia suppression trial (CAST). Arrhythmia can be life-threatening after myocardial infarction, and cardiologists thought suppressing frequent premature ventricular contractions after a heart attack using antiarrhythmics could improve mortality. Ironically, the mortality rate significantly increased with antiarrhythmics despite the reduction of premature ventricular contractions, and the trial was discontinued [
23]. Based upon recent clinical trials, including ours, ART-123 may not be harmful, but it does have a substantial impact on medical expenses.
Efficacy and safety of optional therapies for DIC aiming at correcting coagulation disorders have been examined in many clinical studies. Disappointingly, no treatments have been proven, so far, to benefit the patients. In some studies, those therapies have even worsened the mortality or caused adverse events. These include: antithrombin concentrates (KyberSept trial) [
24]; activated protein C (PROWLESS trial) [
25]; Drotecognin Alfa (ADDRESS and PROWLESS-SHOCK trials) [
26,
27]; tissue factor pathway inhibitor (OPTIMIST trial) [
28]; and anticoagulants [
29,
30]. ART-123 is a relatively new therapy aimed at restoring deleterious coagulation. Despite several clinical studies including randomized, double-blind trials, definitive conclusions have not yet been made [
3,
9,
11].
In a multicenter, randomized, double-blind clinical study, Saito et al. reported that human soluble thrombomodulin could resolve the DIC by 16% compared to the group treated with heparin, but failed to significantly improve mortality of DIC [
9]. However, more than half of the 241 enrolled patients were suffering from hematology malignancy, and the DIC resolution rate was higher in the patients with malignancy compared to patients with infectious diseases [
9]. In an international multicenter, randomized, double-blind, clinical trial, Vincent et al. studied the effects of ART-123 on the 28-day mortality rate and DIC resolution in 370 patients with sepsis and suspected DIC compared to 370 patients treated with a placebo. This study, also, failed to observe a significant difference in the 28-day mortality, the resolution of DIC, and changes in inflammatory markers between the two groups [
11]. A recent retrospective study using a large medical database in Japan (Medical Data Vision Co., Ltd.) demonstrated that ART-123 treatment for Japanese postsurgical patients with DIC was associated with significantly fewer bleeding-related adverse events compared with those receiving other DIC treatments; however, it failed to show the difference in the overall mortality [
31]. The SCARLET randomized clinical trial [
12], a phase III clinical trial following the previous phase IIb clinical trial [
11] was just published in 2019. In the trial, they reported that the incidence of life-threatening major bleeding was less in the thrombomodulin group than the placebo group (5.8% vs. 4.0%). However, the 28-day all-cause mortality was not significantly different.
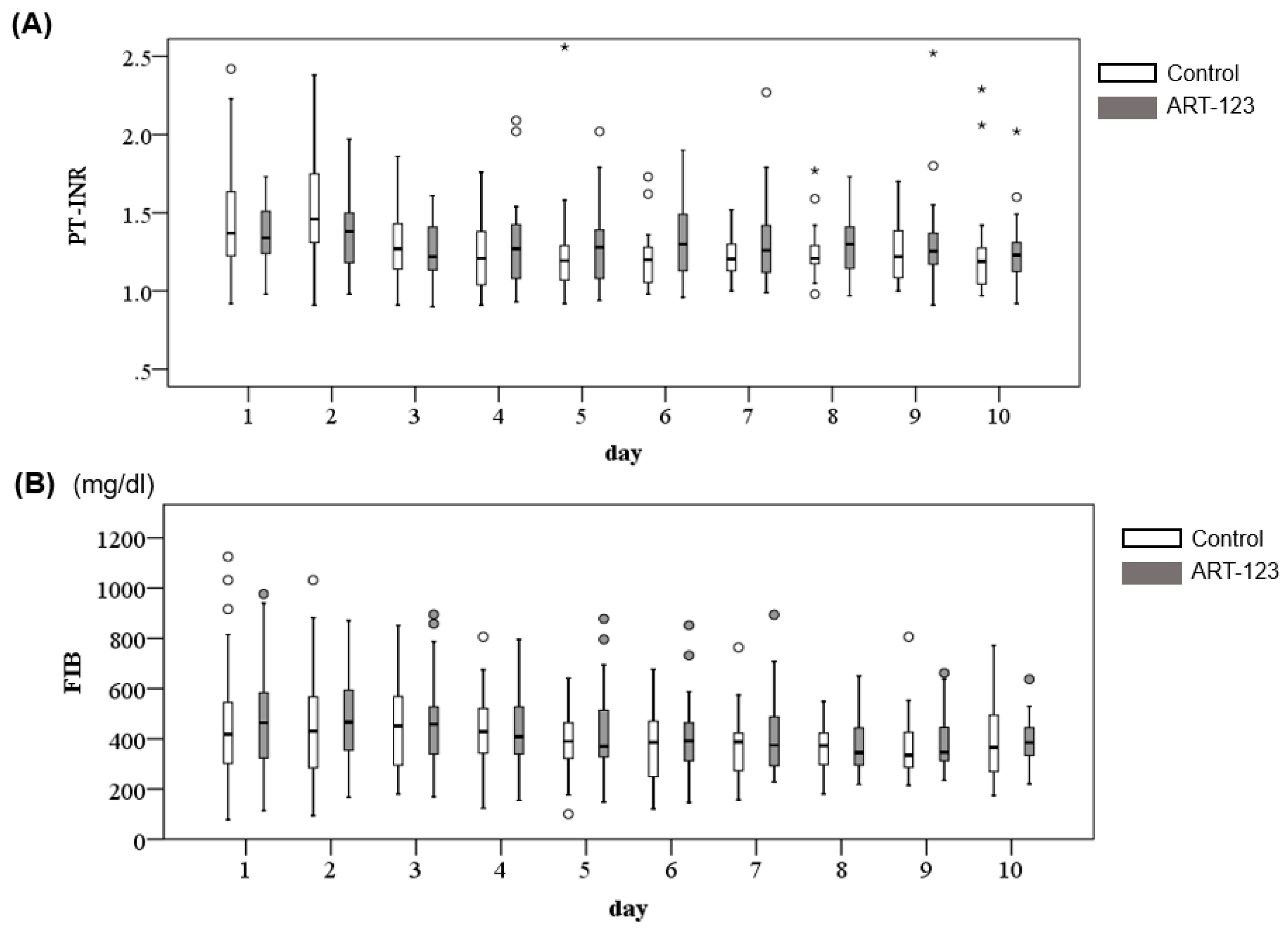
Our data, one of the few prospective randomized trials in Asians, corroborated the results of these clinical trials. However, our data demonstrated that resolution of DIC took place 2–3 days earlier in the ART-123 group than the control group although the PT-INR in our patients was relatively lower than the SCARLET trial. In addition, severe life-threatening bleeding events were not observed in either groups. Importantly, most of the death were associated with uncontrollable infection and multiple organ failures (
Table 6). Thus, our study indicates that ART-123 might play a role to resolve the DIC associated with SIRS.
Moving forward the question is: “Should we still continue to examine the effects of thrombomodulin in this entity of patients?” Despite millions of patients who have been suffering from DIC associated with sepsis, the details of pathophysiological mechanism remain unknown [
32]. Considering the number of patients, very few studies have been performed to examine the effects of reagents aiming at specific targets rather than supporting therapies. This might be due to the complex pathophysiology of the diseases. There are too many potential targets in the cascades and pathways of coagulation systems [
33] and sepsis [
34] to elucidate what is the true target(s) to prevent multi-organ failure. Furthermore, in order to compare the pharmacological effects in a stringent manner, the conditions of two groups (i.e., treated and control patients) have to be identical, including genetic backgrounds. However, achieving those conditions are highly improbable since even monozygotic twins have almost no chance of suffering from the exact same type of sepsis-induced DIC. Therefore, at a minimum, it is necessary to accumulate further data on patients with very similar conditions using consistent evaluation methods and clinical outcomes.
Our study has several significant limitations. This is a single center study with a relatively small number of patients although it is a randomized, placebo controlled, study. In the SCARLET trial, the sample size of 800 patients was supposed to provide 80% power at a 5% two-sided α level based upon a reduction level of 8% in mortality derived from the phase IIb clinical study [
11,
12]. However, the SCARLET trial did not show significant difference in the 28-day mortality between ART-123 and the placebo group [
12]. In a phase III, randomized, double-blind clinical trial to compare the effects of ART-123 and heparin in Japanese DIC patients, 110 patients were thought to be required to provide 80% power at a 5% two-sided α level. However, the underlying diseases contained hematological malignancy and infectious diseases, and non-significant trends in favor of ART-123 were observed for mortality in infectious patients compared to heparin [
9]. In a Japanese retrospective cohort study to examine the effects of recombinant human thrombomodulin in sepsis-induced DIC patients, 12 patients were assigned to the treatment group and 23 patients were assigned to the control. The study showed that the seven-day DIC score was improved in the treatment group, but the 28-day mortality was not significantly different. In this study, a sample size of 114 patients was supposed to provide 90% power at a 5% two-sided α level for the mortality, and 105 patients for the seven-day DIC resolution [
13]. In our study, according to Cohen [
35], a sample size of 79 patients or 84 patients provided 80% power at a 5% two-sided α level for the mortality or the DIC resolution. Thus, our sample size was close to but smaller than the calculated values of the required sample size. When performing a randomized controlled trial, sample size should be carefully considered. To satisfy the required sample size, which sometimes can be substantial, it is often necessary to depend on multicenter trials. The merit of single center trials is that the condition of the treatment can be consistent and access to detailed patient records is very useful to analyze the reasons why a phenomenon is observed. However, there was a significant difference in the timing for resolution of DIC scores, which, in our opinion, makes our study meaningful.
The medical conditions among the patients vary in terms of the primary infectious sites, causes, severity of sepsis, hemodynamics, immunity, type of antibiotics, and drug-metabolisms. However, these limitations are similar to the issues observed in previous clinical trials. Also, most of the patients in this study were enrolled based upon their SIRS score, although we evaluated SOFA and APACHE II scores as well. This was due to the fact that our study was performed before the recent change in the definition of sepsis [
36]. Therefore, we cannot deny that changing the inclusion criteria based upon the new definition of sepsis might have affected the results. Another limitation is that it is impossible to evaluate effects of any reagents on DIC separately from underlying conditions (sepsis in this study). Since treatments of sepsis are supposed to resolve DIC, it is impossible to dissect what actually improves DIC. Thus, we cannot investigate the pathophysiology of DIC in the absence of the underlying diseases in this study.









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}