Cerebral Palsy: Early Markers of Clinical Phenotype and Functional Outcome

 , ,
, ,  , ,
, ,  , , , , ,
, , , , ,  ,
,  and add
Show full author list
and add
Show full author list
Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Setting
2.3. Participants
2.4. Variables
2.5. General Movements Assessment, GMA
2.6. Functional Assessment of the Neurological Findings
2.7. Ethics
2.8. Statistical Analysis
2.9. Data Availability
3. Results
3.1. The Motor Optimality Score and Its Association with GMFCS Outcomes
3.2. Fidgety Movements and Outcome
3.3. Quality of Movement Patterns and Age-Adequate Repertoire
3.4. Postural Patterns
3.5. The Movement Character
3.6. Early Markers of Unilateral CP
3.7. Are Early Signs for Dyskinesia Different From Those for Spasticity?
3.8. Does the Early Motor Repertoire Reveal Markers for Ataxia or Hypotonia?
4. Discussion
4.1. Lower Optimality Scores Justify Referral to Treatment Programs
4.2. Absent Fidgety Movements, a Reliable Predictor for Cerebral Palsy
4.3. Movement and Postural Patterns: Quantity Counts but Quality is More Relevant
4.4. An Asymmetry of Segmental Movements Indicate a High Risk for Unilateral Cerebral Palsy
4.5. Circular Arm Movements and an Atypical Body Posture are Associated with Dyskinesia
4.6. Limitations
5. Conclusions and Future Aspects
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Novak, I.; Morgan, C.; Adde, L.; Blackman, J.; Boyd, R.N.; Brunstrom-Hernandez, J.; Cioni, G.; Damiano, D.; Darrah, J.; Eliasson, A.C.; et al. Early, accurate diagnosis and early intervention in cerebral palsy. Advances in diagnosis and treatment. JAMA Pediatr. 2017, 171, 897–907. [Google Scholar] [CrossRef] [PubMed]
- Herskind, A.; Greisen, G.; Nielsen, J.B. Early identification and intervention in cerebral palsy. Dev. Med. Child Neurol. 2015, 57, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Morgan, C.; Fahey, M.; Roy, B.; Novak, I. Diagnosing cerebral palsy in full-term infants. J. Paediatr. Child Health 2018, 54, 1159–1164. [Google Scholar] [CrossRef] [PubMed]
- Hutchon, B.; Gibbs, D.; Harniess, P.; Jary, S.; Crossley, S.L.; Moffat, J.V.; Basu, N.; Basu, A. Early intervention programmes for infants at high risk of atypical neurodevelopmental outcome. Dev. Med. Child Neurol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Einspieler, C.; Prechtl, H.F.R.; Bos, A.F.; Ferrari, F.; Cioni, G. Prechtl’s Method on the Qualitative Assessment of General Movements in Preterm, Term and Young Infants; MacKeith Press: London, UK, 2004; pp. 1–104. [Google Scholar]
- Einspieler, C.; Utsch, F.; Brasil, P.; Panvequio Aizawa, C.Y.; Peyton, C.; Hydee Hasue, R.; Françoso Genovesi, F.F.; Damasceno, L.; Moreira, M.E.; Adachi, K.; et al. Association of infants exposed to prenatal Zika virus infection with their clinical, neurological, and developmental status evaluated via the general movement assessment tool. JAMA Netw. Open 2019, 2, e187235. [Google Scholar] [CrossRef] [PubMed]
- Prechtl, H.F.R.; Einspieler, C.; Cioni, G.; Bos, A.F.; Ferrari, F.; Sontheimer, D. An early marker for neurological deficits after perinatal brain lesion. Lancet 1997, 349, 1361–1363. [Google Scholar] [CrossRef]
- Romeo, D.M.; Guzzetta, A.; Scoto, M.; Cioni, M.; Patusi, P.; Mazzone, D.; Romeo, M.G. Early neurological assessment in preterm infants: Integration of traditional neurologic examination and observation of general movements. Eur. J. Paediatr. Neurol. 2008, 12, 183–189. [Google Scholar] [CrossRef]
- Bosanquet, M.; Copeland, L.; Ware, R.; Boyd, R. A systematic review of tests to predict cerebral palsy in young children. Dev. Med. Child Neurol. 2013, 55, 418–426. [Google Scholar] [CrossRef]
- Kwong, A.K.L.; Fitzgerald, T.L.; Doyle, L.W.; Cheong, J.L.Y.; Spittle, A.J. Predictive validity of spontaneous early infant movement for later cerebral palsy: A systematic review. Dev. Med. Child Neurol. 2018, 60, 480–489. [Google Scholar] [CrossRef]
- Einspieler, C.; Peharz, R.; Marschik, P.B. Fidgety movements—Tiny in appearance, but huge in impact. J. Pediatr. 2016, 92, S64–S70. [Google Scholar] [CrossRef]
- Ferrari, F.; Frassoldati, R.; Berardi, A.; Di Palma, F.; Ori, L.; Lucaccioni, L.; Bertoncelli, N.; Einspieler, C. The ontogeny of fidgety movements from 4 to 20 weeks post-term age in healthy full-term infants. Early Hum. Dev. 2016, 103, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Einspieler, C.; Marschik, P.B.; Prechtl, H.F.R. Human motor behavior. Prenatal origin and early postnatal development. J. Psychol. 2008, 216, 148–154. [Google Scholar]
- Fjørtoft, T.; Evensen, K.A.I.; Øberg, G.K.; Songstad, N.T.; Labori, C.; Silberg, I.E.; Loennecken, M.; Møinichen, U.I.; Vågen, R.; Støen, R.; et al. High prevalence of abnormal motor repertoire at 3 months corrected age in extremely preterm infants. Eur. J. Paediatr. Neurol. 2016, 20, 236–242. [Google Scholar]
- Zang, F.F.; Yang, H.; Han, Q.; Cao, J.Y.; Tomantschger, I.; Krieber, M.; Shi, W.; Luo, D.D.; Zhu, M.; Einspieler, C. Very low birth weight infants in China: The predictive value of the motor repertoire at 3 to 5 months for the motor performance at 12 months. Early Hum. Dev. 2016, 100, 27–32. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Yuge, M.; Marschik, P.B.; Nakajima, Y.; Yamori, Y.; Kanda, T.; Hirota, H.; Yoshida, N.; Einspieler, C. Movements and postures of infants aged 3 to 5 months: To what extend is their optimality related to perinatal events and to the neurological outcome? Early Hum. Dev. 2011, 87, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Salavati, S.; Einspieler, C.; Vagelli, G.; Zhang, D.; Pansy, J.; Burgerhof, J.G.M.; Marschik, P.B.; Bos, A.F. The association between the early motor repertoire and language development in term children born after normal pregnancy. Early Hum. Dev. 2017, 111, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Hitzert, M.M.; Roze, E.; van Braekel, K.N.J.A.; Bos, A.F. Motor development in 3-month-old healthy term-born infants is associated with cognitive and behavioural outcomes at early school age. Dev. Med. Child Neurol. 2014, 56, 869–876. [Google Scholar] [CrossRef]
- Prechtl, H.F.R. The optimality concept. Early Hum. Dev. 1980, 4, 201–205. [Google Scholar] [PubMed]
- Bruggink, J.L.; Einspieler, C.; Butcher, P.R.; Stremmelar, E.F.; Prechtl, H.F.R.; Bos, A.F. Quantitative aspects of the early motor repertoire in preterm infants: Do they predict minor neurological dysfunction at school age? Early Hum. Dev. 2009, 85, 25–36. [Google Scholar] [CrossRef]
- Butcher, P.R.; van Braeckel, K.; Bouma, A.; Einspieler, C.; Stremmelaar, E.F.; Bos, A.F. The quality of preterm infants' spontaneous movements: An early indicator of intelligence and behaviour at school age. J. Child Psychol. Psychiatry 2009, 50, 920–930. [Google Scholar] [CrossRef]
- Bruggink, J.L.M.; Cioni, G.; Einspieler, C.; Maathuis, C.G.B.; Pascale, R.; Bos, A.F. Early motor repertoire is related to level of self-mobility in children with cerebral palsy at school age. Dev. Med. Child Neurol. 2009, 51, 878–885. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Einspieler, C.; Shi, W.; Marschik, P.B.; Wang, Y.; Cao, Y.; Li, H.; Liao, Y.G.; Shao, X.M. Cerebral palsy in children: Movements and posture during early infancy, dependent of preterm vs. full term birth. Early Hum. Dev. 2012, 88, 837–843. [Google Scholar] [CrossRef] [PubMed]
- Einspieler, C.; Cioni, G.; Paolicelli, P.B.; Bos, A.F.; Dressler, A.; Ferrari, F.; Roversi, M.F.; Prechtl, H.F.R. The early markers for later dyskinetic cerebral palsy are different from those for spastic cerebral palsy. Neuropediatrics 2002, 33, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Cioni, G.; Bos, A.F.; Einspieler, C.; Ferrari, F.; Martijn, A.; Paolicelli, P.B.; Rapisardi, G.; Roversi, M.F.; Prechtl, H.F.R. Early neurological signs in preterm infants with unilateral intraparenchymal echodensity. Neuropediatrics 2000, 31, 240–251. [Google Scholar] [CrossRef] [PubMed]
- Guzzetta, A.; Mercuri, E.; Rapisardi, G.; Ferrari, F.; Roversi, M.F.; Cowan, F.; Rutherford, M.; Paolicelli, P.B.; Einspieler, C.; Boldrini, A.; et al. General movements detect early signs of hemiplegia in term infants with neonatal cerebral infarction. Neuropediatrics 2003, 34, 61–66. [Google Scholar] [PubMed]
- Guzzetta, A.; Pizzardi, A.; Belmonti, V.; Boldrini, A.; Carotenuto, M.; D’Acunto, G.; Ferrari, F.; Fiori, S.; Gallo, C.; Ghirri, P.; et al. Hand movements at 3 months predict later hemiplegia in term infants with neonatal cerebral infarction. Dev. Med. Child Neurol. 2010, 52, 767–772. [Google Scholar] [CrossRef] [PubMed]
- Darsaklis, V.; Snider, L.; Majnemer, A.; Mazer, B. Predictive validity of Prechtl’s method on the qualitative assessment of general movements: A systematic review of evidence. Dev. Med. Child Neurol. 2011, 53, 896–906. [Google Scholar] [CrossRef] [PubMed]
- Bernhardt, I.; Marbacher, M.; Hilfiker, R.; Radlinger, L. Inter-and intra-observer agreement of Prechtl’s method on the qualitative assessment of general movements in preterm, term and young infants. Early Hum. Dev. 2011, 87, 633–639. [Google Scholar] [CrossRef]
- Brown, A.K.; Greisen, G.; Haugsted, U.; Jonsbo, F. Formal training in general movement assessment is required to effectively evaluate infants with perinatal asphyxia in outpatient settings. Acta Paediatr. 2016, 105, 1056–1060. [Google Scholar] [CrossRef]
- Palisano, R.J.; Rosenbaum, P.; Walter, S.; Russell, D.J.; Wood, E.P.; Galuppi, B.E. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev. Med. Child Neurol. 1997, 39, 214–223. [Google Scholar] [CrossRef]
- Palisano, R.J.; Rosenbaum, P.; Bartlett, D.; Livingston, M.H. Content validity of the expanded and revised Gross Motor Function Classification System. Dev. Med. Child Neurol. 2008, 50, 744–750. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, F.; Todeschini, A.; Guidotti, I.; Martinez-Biarge, A.; Roversi, M.F.; Berardi, A.; Ranzi, A.; Cowan, F.M.; Rutherford, M.A. General movements in full-term infants with perinatal asphyxia are related to basal ganglia and thalamic lesions. J. Pediatr. 2011, 158, 904–911. [Google Scholar] [CrossRef] [PubMed]
- Marschik, P.B.; Pokorny, F.B.; Peharz, R.; Zhang, D.; O’Muircheartaigh, J.; Roeyers, H.; Bölte, S.; Spittle, A.J.; Urlesberger, B.; Schuller, B.; et al. A novel way to measure and predict development: A heuristic approach to facilitate the early detection of neurodevelopmental disorders. Curr. Neurol. Neurosci. Rep. 2017, 17, 43. [Google Scholar] [CrossRef] [PubMed]
- Spittle, A.J.; Olsen, J.; Kwong, A.; Doyle, L.W.; Marschik, P.B.; Einspieler, C.; Cheong, J.L.Y. The Baby Moves prospective cohort study protocol: Using a smartphone application with the general movements assessment to predict neurodevelopmental outcomes at age 2 years for extremely preterm or extremely low birthweight infants. BMJ Open 2016, 6, e013446. [Google Scholar] [CrossRef] [PubMed]
- Herrero, D.; Einspieler, C.; Panvequio Aizawa, C.Y.; Mutlu, A.; Yang, H.; Nogolová, A.; Pansy, J.; Nielsen-Saines, K.; Marschik, P.B.; GenGM Study Group. The motor repertoire in 3- to 5-month old infants with Down syndrome. Res. Dev. Disabil. 2017, 67, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Fjørtoft, T.; Einspieler, C.; Adde, L.; Strand, L.I. Inter-observer reliability of the “Assessment of motor repertoire—3 to 5 months” based on video recordings of infants. Early Hum. Dev. 2009, 85, 297–302. [Google Scholar] [CrossRef]
- Piek, J.P. A quantitative analysis of spontaneous kicking in two-month-old infants. Early Hum. Dev. 1996, 15, 707–726. [Google Scholar] [CrossRef]
- Konishi, Y.; Prechtl, H.F.R. Finger movements and finger postures in pre-term infants are not a good indicator of brain damage. Early Hum. Dev. 1994, 36, 89–100. [Google Scholar] [CrossRef]
- McIntyre, S.; Morgan, C.; Walker, K.; Novak, I. Cerebral palsy—Don’t delay. Dev. Disabil. Res. Rev. 2011, 17, 114–129. [Google Scholar] [CrossRef]
- Morgan, C.; Crowle, C.; Goyen, T.A.; Hradman, C.; Jackman, M.; Novak, I.; Badawi, N. Sensitivity and specificity of general movement assessment for diagnostic accuracy of detecting cerebral palsy early in an Australian context. J. Paediatr. Child Health 2016, 52, 54–59. [Google Scholar] [CrossRef]
- Eliasson, A.C.; Nordstrand, L.; Ek, L.; Lennartsson, F.; Sjöstrand, L.; Tedroff, K.; Krumlinde-Sundholm, L. The effectiveness of Baby-CIMT in infants younger than 12 months with clinical signs of unilateral-cerebral palsy; an explorative study with randomized design. Res. Dev. Disabil. 2018, 72, 191–201. [Google Scholar] [CrossRef]
- Chamudot, R.; Parush, S.; Rigbi, A.; Horovitz, R.; Gross-Tsur, V. Effectiveness of modified constraint-induced movement therapy compared with bimanual therapy home programs for infants with hemiplegia: A randomized controlled trial. Am. J. Occup. Ther. 2018, 72, 7206205010p1–7206205010p9. [Google Scholar] [CrossRef]
- Nordstrand, L.; Holmefur, M.; Kits, A.; Eliasson, A.C. Improvements in bimanual hand function after baby-CIMT in two-year old children with unilateral cerebral palsy: A retrospective study. Res. Dev. Disabil. 2015, 41, 86–93. [Google Scholar] [CrossRef]
- Kwong, A.K.L.; Olsen, J.E.; Eeles, A.L.; Einspieler, C.; Lee, K.J.; Doyle, L.W.; Cheong, J.L.Y.; Spittle, A.J. Occurrence and temporal trends in fidgety general movements in infants born extremely preterm/extremely low birthweight and term-born controls. Early Hum. Dev. 2019, 135, 11–15. [Google Scholar] [CrossRef]
- Burger, M.; Frieg, A.; Louw, Q.A. General Movements as a predictive tool of the neurological outcome in very low and extremely low birthweight infants—A South African perspective. Early Hum. Dev. 2011, 87, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Spittle, A.J.; Brown, N.C.; Doyle, L.W.; Boyd, R.N.; Hunt, R.W.; Bear, M.; Inder, T.E. Quality of general movements is related to white matter pathology in very preterm infants. Pediatrics 2008, 121, e1184–e1189. [Google Scholar] [CrossRef] [PubMed]
- Peyton, C.; Yang, E.; Kocherginsky, M.; Adde, L.; Fjørtoft, T.; Støen, R.; Bos, A.F.; Einspieler, C.; Schreiber, M.D.; Msall, M.E. Relationship between white matter pathology and performance on the General Movement Assessment and the Test of Infant Motor Performance in very preterm infants. Early Hum. Dev. 2016, 95, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Spittle, A.J.; Doyle, L.W.; Anderson, P.J.; Inder, T.E.; Lee, K.J.; Boyd, R.N.; Cheong, J.L. Reduced cerebellar diameter in very preterm infants with abnormal general movements. Early Hum. Dev. 2010, 86, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Adde, L.; Helbostad, J.L.; Jensenius, A.R.; Langaas, M.; Støen, R. Identification of fidgety movements and prediction of CP by the use of computer-based video analysis is more accurate when based on two video recordings. Physiother. Theory Pract. 2013, 52, 773–778. [Google Scholar] [CrossRef]
- Einspieler, C.; Yang, H.; Bartl-Pokorny, K.D.; Chi, X.; Zang, F.F.; Marschik, P.B.; Guzzetta, A.; Ferrari, F.; Bos, A.F.; Cioni, G. Are sporadic fidgety movements as clinically relevant as is their absence? Early Hum. Dev. 2015, 91, 247–252. [Google Scholar] [CrossRef]
- Ferrari, F.; Cioni, G.; Prechtl, H.F.R. Qualitative changes of general movements in preterm infants with brain lesions. Early Hum. Dev. 1990, 23, 193–231. [Google Scholar] [CrossRef]
- Jeon, H.; Jung, J.H.; Yoon, J.A.; Choi, H. Strabism is correlated with gross motor function in children with spastic cerebral palsy. Curr. Eye Res. 2019, 18, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Vaal, J.; van Soest, A.J.; Hopkins, B.; Sie, L.T.L.; van der Knaap, M.S. Development of spontaneous leg movements in infants with and without periventricular leukomalacia. Exp. Brain Res. 2000, 135, 94–105. [Google Scholar] [CrossRef] [PubMed]
- Fetters, L.; Chen, Y.; Jonsdottir, J.; Tronick, E.Z. Kicking coordination captures differences between full-term and premature infants with white matter disorder. Hum. Mov. Sci. 2004, 22, 729–748. [Google Scholar] [CrossRef] [PubMed]
- Jones, M.W.; Morgan, E.; Shelton, J.E.; Thorogood, C. Cerebral palsy: Introduction and diagnosis (part I). J. Pediatr. Health Care 2007, 21, 146–152. [Google Scholar] [CrossRef]
- Harris, S.R. Early neuromotor predictors of cerebral palsy in low birthweight infants. Dev. Med. Child Neurol. 1987, 29, 508–519. [Google Scholar] [CrossRef]
- Faridi, M.M.; Rath, S.; Aggarwal, A. Profile of fisting in term newborns. Eur. J. Paediatr. Neurol. 2005, 9, 67–70. [Google Scholar] [CrossRef]
- Ferrari, F.; Cioni, G.; Einspieler, C.; Roversi, M.F.; Bos, A.F.; Paolicelli, P.B.; Ranzi, A.; Prechtl, H.F.R. Cramped synchronized general movements in preterm infants as an early marker for cerebral palsy. Arch. Pediatr. Adolesc. Med. 2002, 145, 460–467. [Google Scholar] [CrossRef]
- Zappella, M.; Einspieler, C.; Bartl-Pokorny, K.D.; Krieber, M.; Coleman, M.; Bölte, S.; Marschik, P.B. What do home-videos tell us about early motor and socio-communicative behaviours in children with autistic features during the second year of life—An exploratory study. Early Hum. Dev. 2015, 91, 569–575. [Google Scholar] [CrossRef]
- Fjørtoft, T.; Grunewaldt, K.H.; Løhaugen, G.C.; Mørkved, S.; Skranes, J.; Evensen, K.A.I. Assessment of motor behaviour in high-risk infants at 3 months predicts motor and cognitive outcomes in 10 years old children. Early Hum. Dev. 2013, 89, 787–793. [Google Scholar] [CrossRef]
- de Vries, N.K.; van der Veere, C.N.; Reijneveld, S.A.; Bos, A.F. Early neurological outcome of young infants exposed to selective serotonin reuptake inhibitors during pregnancy: Results from the observational SMOK study. PLoS ONE 2013, 8, e64654. [Google Scholar] [CrossRef] [PubMed]
- Einspieler, C.; Hirota, H.; Yuge, M.; Dejima, S.; Marschik, P.B. Early behavioural manifestation of Smith-Magenis syndrome (del 17p11.2) in a 4-month-old boy. Dev. Neurorehabil. 2012, 15, 313–316. [Google Scholar] [CrossRef] [PubMed]
- Pansy, J.; Barones, C.; Urlesberger, B.; Pokorny, F.B.; Bartl-Pokorny, K.D.; Verheyen, S.; Marschik, P.B.; Einspieler, C. Early motor and pre-linguistic verbal development in Prader-Willi syndrome—A case report. Res. Dev. Disabil. 2019, 88, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Eyre, J.A.; Taylor, J.P.; Villagra, F.; Smith, M.; Miller, S. Evidence of activity-dependent withdrawal of corticospinal projections during human development. Neurology 2001, 57, 1543–1554. [Google Scholar] [CrossRef] [PubMed]
- Einspieler, C. Early markers for unilateral spastic cerebral palsy in premature infants. Nat. Clin. Pract. Neurol. 2008, 4, 186–187. [Google Scholar] [CrossRef] [PubMed]
- Tomantschger, I.; Herrero, D.; Einspieler, C.; Hamamura, C.; Voos, M.C.; Marschik, P.B. The general movement assessment in non-European low- and middle-income countries. Rev. Saude Publica 2018, 5, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Sundrum, R.; Logan, S.; Wallace, A.; Spencer, N. Cerebral palsy and socioeconomic status: A retrospective cohort study. Arch. Dis. Child. 2005, 90, 15–18. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Solaski, M.; Majnemer, A.; Oskoui, M. Contribution of socio-economic status on the prevalence of cerebral palsy: A systematic search and review. Dev. Med. Child Neurol. 2014, 56, 1043–1051. [Google Scholar] [CrossRef]
- Dan, B.; Paneth, N. Making sense of cerebral palsy prevalence in low-income countries. Lancet Glob. Health 2017, 5, e1174–e1175. [Google Scholar] [CrossRef][Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Movement Pattern | Definition |
|---|---|
| Swipes | Ballistic-like movements with a sudden onset but fluid course and smooth offset; can go in downward or upward direction; most noticeable in extended arms; but also in partially or fully extended legs; large amplitude and high speed. |
| Score atypical if repetitively occurring in more than one third of the observation time. | |
| Wiggling-Oscillating Movements | Oscillatory, uniplanar movements; most noticeable in partially or fully extended arms but from time to time also in partially extended legs, with a frequency of 2–3 Hz; small amplitude and moderate speed. |
| Score atypical if repetitively occurring in more than one third of the observation time. | |
| Kicking | Can occur in a single leg and/or as simultaneous bilateral kicking with a fast flexion phase followed by a slower extension phase with decoupling of hip, knee and ankle. |
| Score atypical if monotonous and/or coupling of hip, knee, and ankle is observed such that all joints tend to flex or extend in temporal synchrony. | |
| Excitement Bursts | Wiggling-oscillating movements and/or swipes co-occur with kicking and are accompanied by a pleasurable and excited facial expression. |
| Score atypical if monotonous and without pleasure mimic. | |
| Smiles | Score atypical if awkward and frozen. |
| Mouth Movements | Are variable and usually related to vocalization (cooing) and/or non-nutritive sucking. |
| Score atypical if opening and closing occur repetitively. | |
| Tongue Movements | Score atypical if tongue protrusion is repetitive and/or long-lasting. |
| Side-to-Side Movements of the Head | The head crosses the midline smoothly and fluently. Do not mark if the head moves only from midline to side and back. Score atypical if repetitive. |
| Hand-to-Mouth Contact | The arm is moved against gravity and the hand touches the mouth with or without finger inserted. Do not mark if the head is on the side and the arm is not moved against gravity. Score atypical if repetitive. |
| Hand-to-Hand Contact | Both hands are brought together in the midline and the fingers of both hands repetitively touch, stroke or grasp each other. Score atypical if asymmetrical, or if both hands are fisted. |
| Fiddling | The fingers of one or both hands repetitively touch, stroke or grasp an object, most often the own clothing. Score atypical if the infant touches an object or the own clothing, no finger movements occur, and the hand has difficulties to release. |
| Reaching | One or both arms intentionally extend to some object in the immediate environment; the fingers may or may not contact the surface of the object. (This behavior is not elicited by a tester but occurs spontaneously.) |
| Foot-to-Foot Contact | Legs are elevated and feet are brought together with plantar-to-plantar touching from time to time. Do not mark if the feet remain on the surface during contact. Score atypical if foot-to-foot contact occurs mainly on the tibial side and/or is characterized by repetitive rubbing. |
| Legs Lift | Both legs lift vertically upward; partial or full extension at the knees; hips and pelvis are slightly tilted upward; one or both hands may touch or grasp the knees; sometimes it occurs together with anteflexion of the head. Score atypical if it occurs stiff and without variation. |
| Hand-to-Toe Contact | One or both hands touch, stroke or grasp the toes. |
| Segmental Movements of Fingers and Wrists | Independent movements of fingers and/or movements of moderate speed at the level of the wrist joint including rotation, palmar flexion and extension, and ulnar or radial flexion. Score atypical if asymmetrical. |
| Arching | After the soles touch the surface, the infant extends the back and neck causing a full trunk and head curve to form. Sometimes locomotion occurs. Do not mark if arching is a sign of discomfort. Score atypical if arching is prolonged and/or too stiff. |
| Rolling to Side | As a result of the soles of the feet pushing down on the lying surface, one side of the hip is lifted and rotated. From about 18 weeks onwards, the whole body is turned from supine to prone lying in a movement started by the head. Sometimes the infant returns to supine lying. Score atypical if the infant moves head and pelvis simultaneously sideways upward, moves the top leg forward and topples over en bloc, and/or if rolling is non-intentionally. |
| Visual Exploration | The infant visually explores the environment. Score atypical, if abnormal eye movements, (transient) strabismus, nystagmus, and/or setting sun phenomenon occur. Each atypical eye movement pattern is given a separate atypical mark; for instance, if the child has both nystagmus and setting sun phenomenon, give two atypical scores. |
| Hand Regard | The infant visually attends to the movements of his/her hand(s). |
| Head Anteflexion | The head is moved against gravity, sometimes the chin touches the trunk. Score atypical if prolonged and too stiff. |
| Circular Arm Movements | Uni- or bilateral, monotonous, slow forward rotations of the semi-flexed or extended arms, starting in the shoulder. They occur with or without spread fingers. |
| Postural Pattern | Definition |
| Head Centered | The head can be kept centered for at least 10 s; chin and sternum are in one line. Score atypical if the head cannot be centered, i.e., is tilted or in lateral position. |
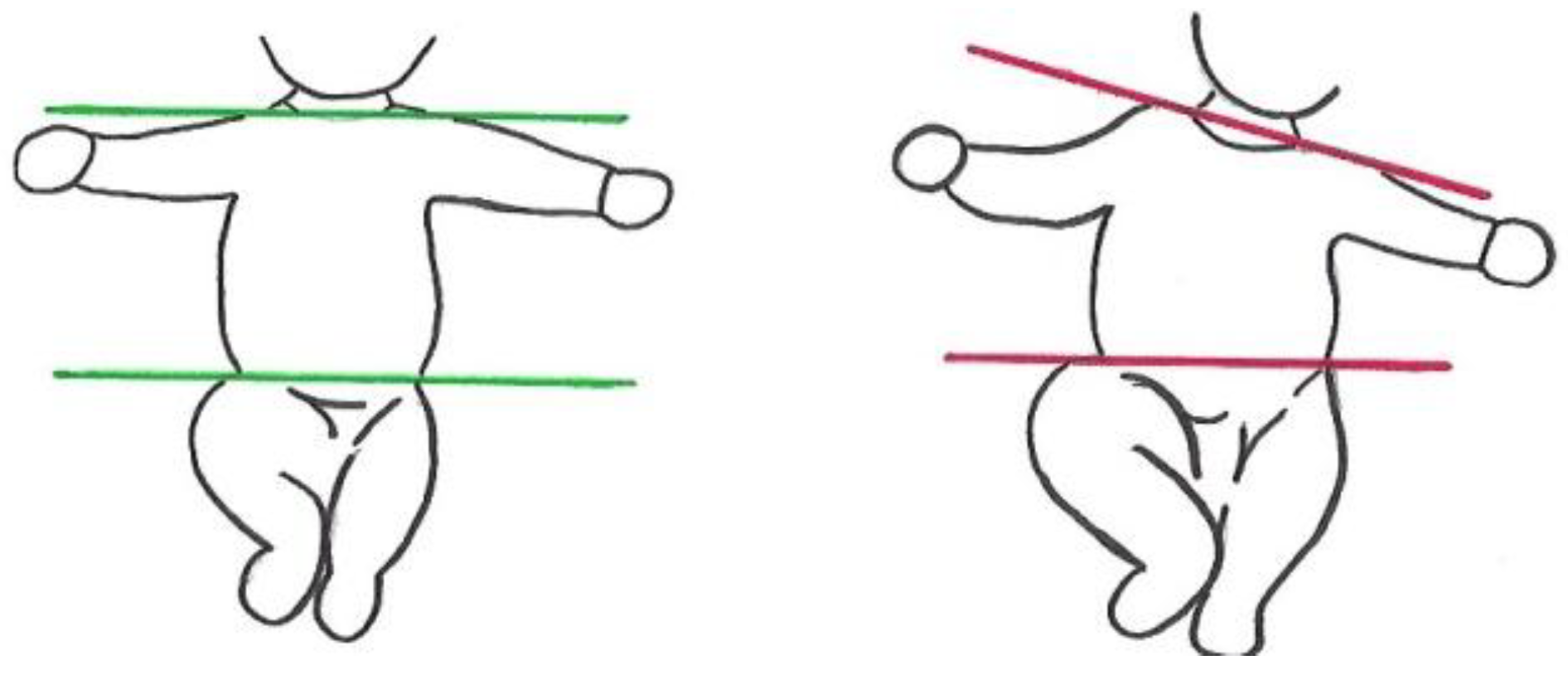
| Body Symmetry | An imaginary line through the shoulder joints and an imaginary line through the hip joints run parallel (Figure 3). Score atypical if this is not the case throughout the recording. |
| Asymmetric Tonic Neck (ATN) Posture | The ATN posture cannot be observed or the extended arm can be easily flexed without turning the head. Score atypical if each spontaneous side movement of the head elicits an ATN that cannot be overcome by flexion of the extended arm. |
| Flat Posture | Lying in supine, all four limbs are mainly on the surface; antigravity movements and flexion in hips and knees are rare; arms and legs hardly move above the level of the trunk. |
| Variability of Finger Postures | Postures of the fingers, which result from isolated movements of one finger, simultaneous movements of two or three fingers, and/or sequential movements of two or more fingers. Fisting might occur from time to time. Score atypical if finger postures are rare and/or lack variability. |
| Predominant Fisting | Score atypical if fisting occurs more than 80% of the observation time. In this case also variability of finger postures is scored “atypical”. |
| Synchronized Opening and Closing of Fingers | Bilateral simultaneous extension of all fingers away from the palm is followed by bilateral flexion of all fingers towards the palm. |
| Finger Spreading | Unilateral or bilateral abduction and extension of all fingers. |
| Asymmetry of Finger Postures | Score atypical if one hand shows different finger postures and the other hand is fisted. |
| Hyperextension of Neck and/or Trunk | Do not mark if the infant focusses his/her attention to an object or a person in the right or left upper corner. |
| Extended Arms | Bilateral predominant extension of the arms on or above the surface. |
| Extended Legs | Bilateral predominant extension of the legs on or above the surface. |
| 9 to 11 Weeks PTA | 12 to 13 Weeks PTA | 14 to 15 Weeks PTA | 16 Weeks PTA and Older a | |
|---|---|---|---|---|
| Score 4 | at least four normal movement patterns | at least four normal movement patterns including normal foot-to-foot contact | at least four normal movement patterns including normal foot-to-foot contact and normal hand-to hand contact | at least four normal movement patterns including the following three obligatory patterns: normal foot-to-foot contact and normal hand-to-hand contact and normal legs lift |
| Score 2 | three normal movement patterns | at least four normal movement patterns but not foot-to-foot contact | at least four normal movement patterns including normal foot-to-foot contact or normal hand-to hand contact | at least four normal movement patterns including only two of the above-mentioned obligatory movement patterns |
| Score 1 | less than three normal movement patterns | less than four normal movement patterns | normal foot-to-foot contact and normal hand-to-hand contact are not observable | only one of the above-mentioned obligatory movement patterns is present or all of them are absent |
| Subcategories of the MOS | Estimated Coefficient | SE | Wald Statistics | p-Value | 95% CI |
|---|---|---|---|---|---|
| (i) Fidgety Movements | −0.19 | 0.06 | 11.43 | 0.001 | −0.30 to −0.08 |
| (ii) Quality of Movement Patterns | −0.68 | 0.08 | 71.71 | <0.001 | −0.84 to −0.52 |
| (iii) Age-Adequate Movement Repertoire | −0.16 | 0.15 | 1.16 | 0.282 | −0.44 to −0.13 |
| (iv) Postural Patterns | −0.36 | 0.08 | 19.20 | <0.001 | −0.52 to −0.20 |
| (v) Movement Character | −1.26 | 0.25 | 24.75 | <0.001 | −1.76 to −0.76 |
| Movement Pattern | Normal Quality n (%) | Atypical n (%) | Not Observed n (%) | GMFCS-E&R Levels I–II (n = 162; 34.6%) vs. III–V (n = 306; 65.4%) | Unilateral (n = 92; 19.7%) vs. Bilateral (n = 376; 80.3%) CP | Spastic (n = 415; 92.6%) vs. Non-Spastic (n = 33; 7.4%) CP a |
|---|---|---|---|---|---|---|
| Swipes | 57 (12.2%) | 34 (7.3%) | 377 (80.5%) | ORGMFCS III-V = 4.11 (95% CI = 1.62−10.38; z = 2.98, p < 0.01) | ORbilateral = 4.38 (95% CI = 1.35−14.15; z = 2.46, p < 0.05) | No difference (p = 0.554) |
| Wiggling-Oscillating Movements | 53 (11.3%) | 45 (9.6%) | 370 (79.1%) | ORGMFCS III-V = 3.58 (95% CI = 1.55−8.26; z = 2.99, p < 0.01) | No difference (p = 0.059) | No difference (p = 0.821) |
| Kicking | 55 (11.8%) | 170 (36.3%) | 243 (51.8%) | ORGMFCS III-V = 2.60 (95% CI = 1.40−4.85; z = 3.01, p < 0.01) | No difference (p = 0.683) | No difference (p = 0.183) |
| Excitement Bursts | 17 (3.6%) | 19 (4.1%) | 432 (92.3%) | ORGMFCS III-V = 5.57 (95% CI = 1.30−23.93; z=2.31, p < 0.05) | ORbilateral = 5.13 (95% CI = 1.23−21.36; z = 2.25, p < 0.05) | No difference (p = 0.455) |
| Smiles | 94 (20.1%) | 21 (4.5%) | 353 (75.4) | ORGMFCS III-V = 2.84 (95% CI = 1.01−7.96; z = 1.99, p < 0.05) | ORbilateral = 5.38 (95% CI = 1.18−24.53; z=2.18, p < 0.05) | No difference (p = 0.537) |
| Mouth Movements | 83 (17.7%) | 147 (31.4%) | 238 (50.9%) | ORGMFCS III-V = 6.50 (95% CI = 3.44−12.32; z = 5.75, p < 0.001) | ORbilateral = 4.84 (95% CI = 2.37-9.88; z = 4.32, p < 0.001) | No difference (p = 0.395) |
| Tongue Movements | n.a. | 134 (28.6%) | 334 (71.4%) | ORGMFCS III-V = 1.65 (95% CI = 1.06−2.56; z = 2.22, p < 0.05) | No difference (p = 0.705) | No difference (p = 0.552) |
| Side-to-Side Movements of the Head | 114 (24.4%) | 105 (22.4%) | 245 (53.2%) | ORGMFCS III-V = 3.43 (95% CI = 1.92−6.13; z = 4.17, p < 0.001) | ORbilateral = 3.12 (95% CI = 1.60−6.10; z = 3.33, p < 0.001) | No difference (p = 0.216) |
| Hand-to-Mouth Contact | 65 (13.9%) | 20 (4.3%) | 383 (81.8%) | ORGMFCS III-V = 3.73 (95% CI = 1.27−10.98; z = 2.39, p < 0.05) | No difference (p = 0.525) | No difference (p = 0.136) |
| Hand-to-Hand Contact | 27 (5.8%) | 18 (3.8%) | 423 (90.4%) | No difference (p = 0.143) | No difference (p = 0.917) | No difference (p = 0.250) |
| Fiddling | 40 (8.5%) | 10 (2.1%) | 418 (89.4%) | No difference (p = 0.308) | No difference (p = 0.204) | No difference (p = 0.451) |
| Reaching | 0 | n.a. | 468 (100%) | n.a. | n.a. | n.a. |
| Foot-to-Foot Contact | 38 (8.1%) | 81 (17.3%) | 349 (74.6%) | ORGMFCS III-V = 9.37 (95% CI = 3.65−24.07; z = 4.65, p < 0.001) | ORbilateral = 5.32 (95% CI = 2.25−12.55; z=3.81, p < 0.001) | No difference (p = 0.558) |
| Legs Lift | 40 (8.5%) | 40 (8.5%) | 388 (83%) | ORGMFCS III-V = 3.86 (95% CI = 1.53−9.75; z = 2.85, p < 0.01) | ORbilateral = 4.67 (95% CI = 1.51−14.46; z=2.67, p < 0.01) | No difference (p = 0.127) |
| Segmental Movements of Fingers and Wrists | n.a. | 64 (13.7%) | 404 (86.3%) | ORGMFCS I-II = 16.96 (95% CI = 8.10−35.50; z = 7.51, p < 0.001) | ORunilateral = 105.20 (95% CI = 42.30−261.60; z = 10.02, p < 0.001) | No difference (p = 0.080) |
| Arching | 8 (1.7%) | 33 (7.1%) | 427 (91.2%) | ORGMFCS III-V = 26.00 (95% CI = 2.73−248.02; z = 2.83, p < 0.01) | ORbilateral = 12.08 (95% CI = 2.05−71.12; z=2.76, p < 0.01) | No difference (p = 0.704) |
| Rolling to Side | 5 (1%) | 42 (9%) | 421 (90%) | ORGMFCS III-V = 9.00 (95% CI=1.23−65.64; z = 2.17, p < 0.05) | ORbilateral = 13.33 (95% CI=1.36−130.92; z = 2.22, p < 0.05) | No difference (p = 0.663) |
| Visual Exploration | 158 (33.8%) | 97 (20.7%) | 213 (45.5%) | ORGMFCS III-V = 4.32 (95% CI = 2.39−7.79; z = 4.86, p < 0.001) | No difference (p = 0.061) | No difference (p = 0.112) |
| Hand Regard | 21 (4.5%) | n.a. | 447 (95.5%) | ORGMFCS I-II = 4.04 (95% CI = 1.60−10.22; z = 2.95, p < 0.01) | ORunilateral = 6.12 (95% CI = 2.49−15.01; z = 3.96, p < 0.001) | No difference (p = 0.679) |
| Head Anteflexion | 2 (0.4%) | 10 (2.1%) | 456 (97.5%) | No difference (p = 0.061) | No difference (p = 0.216) | No difference (p = 0.612) |
| Circular Arm Movements | n.a. | 60 (12.8%) | 408 (87.2%) | ORGMFCS III-V = 18.71 (95% CI = 4.51−77.68; z = 4.03, p < 0.001) | ORbilateral = 16.94 (95% CI =2.31−123.93; z = 2.79, p < 0.01) | ORnon-spastic = 8.77 (95% CI = 4.08−18.87; z = 5.56, p < 0.001) |
| Almost No Leg Movements | n.a. | 32 (6.8%) | 436 (93.2%) | ORGMFCS III-V = 5.55 (95% CI = 1.66−18.51; z = 2.79, p < 0.01) | No difference (p = 0.088) | No difference (p = 0.879) |
| Postural Pattern | Normal n (%) | Atypical n (%) | Not Observed n (%) | GMFCS-E&RLevels I–II (n = 162; 34.6%) vs. III–V (n = 306; 65.4%) | Unilateral (n = 92; 19.7%) vs. Bilateral (n = 376; 80.3%) CP | Spastic (n = 415; 92.6%) vs. Non-spastic (n = 33; 7.4%) CP a |
|---|---|---|---|---|---|---|
| Head Centered | 182 (38.9%) | 286 (60.1%) | n.a. | ORGMFCS III-V = 3.29 (95% CI = 2.21−4.89; z=5.87, p < 0.001) | ORbilateral = 3.09 (95% CI = 1.93−4.94; z = 4.70, p < 0.001) | No difference (p = 0.261) |
| Body Symmetry | 164 (35%) | 304 (65%) | n.a. | ORGMFCS III-V = 2.47 (95% CI = 1.66−3.68; z = 4.48, p < 0.001) | No difference (p = 0.120) | ORnon-spastic = 3.30 (95% CI = 1.25−8.74; z = 2.41, p < 0.05) |
| ATN Posture | 351 (75%) | 117 (25%) | n.a. | ORGMFCS III-V = 2.08 (95% CI =1.29−3.37; z = 2.99, p < 0.01) | ORbilateral = 1.91 (95% CI = 1.05−3.48; z = 2.12, p < 0.05) | No difference (p = 0.087) |
| Flat Posture | n.a. | 67 (14.3%) | 401 (85.7%) | No difference (p = 0.107) | No difference (p = 0.821) | No difference (p = 0.359) |
| Variability of Finger Postures | 50 (10.7%) | 418 (89.3%) | n.a. | ORGMFCS III-V = 5.96 (95% CI = 3.11−11.43; z = 5.37, p < 0.001) | No difference (p = 0.127) | No difference (p = 0.138) |
| Predominant Fisting | n.a. | 175 (37.4%) | 293 (62.6%) | No difference (p = 0.627) | No difference (p = 0.084) | No difference (p = 0.056) |
| Synchronized Opening and Closing of Fingers | n.a. | 41 (8.8%) | 427 (91.2%) | No difference (p = 0.074) | No difference (p = 0.197) | No difference (p = 0.217) |
| Finger Spreading | n.a. | 87 (18.6%) | 381 (81.4% | ORGMFCS III-V = 2.76 (95% CI = 1.54−4.93; z = 3.43, p < 0.001) | No difference (p = 0.327) | No difference (p = 0.499) |
| Hyperextension of Neck and/or Trunk | n.a. | 94 (20.7%) | 371 (79.3) | ORGMFCS III-V = 3.29 (95% CI = 1.85−5.84; z = 4.05, p < 0.001) | ORbilateral = 3.26 (95% CI = 1.52−6.98; z = 3.03, p < 0.01) | No difference (p = 0.847) |
| Extended Arms | n.a. | 76 (16.1%) | 392 (83.9%) | No difference (p = 0.158) | No difference (p = 0.966) | No difference (p = 0.103) |
| Extended Legs | n.a. | 124 (26.5%) | 344 (73.5%) | ORGMFCS III-V = 2.06 (95% CI = 1.29−3.30; z = 3.03, p < 0.01) | No difference (p = 0.054) | No difference (p = 0.130) |
| Movement Character | Yes n (%) | No n (%) | GMFCS-E&R Levels I–II (n = 162; 34.6%) vs. III–V (n = 306; 65.4%) | Unilateral (n = 92; 19.7%) vs. Bilateral (n = 376; 80.3%) CP | Spastic (n = 415; 92.6%) vs. Non-spastic (n = 33; 7.4%) CP a |
|---|---|---|---|---|---|
| Smooth and Fluent | 1 (0.3%) | 467 (99.7%) | n.a. | n.a. | n.a. |
| Cramped-Synchronized | 88 (18.8%) | 380 (81.2%) | ORGMFCS III-V = 11.69 (95% CI = 4.63−29.48; z = 5.21, p < 0.001) | ORbilateral = 27.39 (95% CI = 3.76−199.46; z = 3.27, p < 0.01) | No difference (p = 0.707) |
| Monotonous | 385 (82.3%) | 83 (17.7%) | ORGMFCS III-V = 1.67 (95% CI = 1.03−2.71; z = 2.09, p < 0.05) | ORbilateral = 1.76 (95% CI = 1.02−3.03; z = 2.02, p < 0.05) | No difference (p = 0.575) |
| Jerky | 106 (22.6%) | 362 (77.4%) | No difference (p = 0.090) | No difference (p = 0.276) | No difference (p = 0.058) |
| Stiff | 264 (56.4%) | 204 (43.6%) | ORGMFCS III-V = 2.89 (95% CI = 1.95−4.28; z = 5.29, p < 0.001) | ORbilateral = 2.26 (95% CI = 1.42−3.61; z = 3.44, p < 0.001) | No difference (p = 0.113) |
| Tremulous | 76 (16.2%) | 392 (83.8%) | ORGMFCS III-V = 2.69 (95% CI = 1.45−4.97; z = 3.15, p < 0.01) | No difference (p = 0.198) | No difference (p = 0.381) |
| Predominantly Slow | 84 (17.9%) | No difference (p = 0.113) | No difference (p = 0.283) | No difference (p = 0.547) | |
| Predominantly Fast | 26 (5.6%) | No difference (p = 0.295) | No difference (p = 0.275) | No difference (p = 0.614) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Einspieler, C.; Bos, A.F.; Krieber-Tomantschger, M.; Alvarado, E.; Barbosa, V.M.; Bertoncelli, N.; Burger, M.; Chorna, O.; Del Secco, S.; DeRegnier, R.-A.; et al. Cerebral Palsy: Early Markers of Clinical Phenotype and Functional Outcome. J. Clin. Med. 2019, 8, 1616. https://doi.org/10.3390/jcm8101616
Einspieler C, Bos AF, Krieber-Tomantschger M, Alvarado E, Barbosa VM, Bertoncelli N, Burger M, Chorna O, Del Secco S, DeRegnier R-A, et al. Cerebral Palsy: Early Markers of Clinical Phenotype and Functional Outcome. Journal of Clinical Medicine. 2019; 8(10):1616. https://doi.org/10.3390/jcm8101616
Chicago/Turabian StyleEinspieler, Christa, Arend F. Bos, Magdalena Krieber-Tomantschger, Elsa Alvarado, Vanessa M. Barbosa, Natascia Bertoncelli, Marlette Burger, Olena Chorna, Sabrina Del Secco, Raye-Ann DeRegnier, and et al. 2019. "Cerebral Palsy: Early Markers of Clinical Phenotype and Functional Outcome" Journal of Clinical Medicine 8, no. 10: 1616. https://doi.org/10.3390/jcm8101616
APA StyleEinspieler, C., Bos, A. F., Krieber-Tomantschger, M., Alvarado, E., Barbosa, V. M., Bertoncelli, N., Burger, M., Chorna, O., Del Secco, S., DeRegnier, R.-A., Hüning, B., Ko, J., Lucaccioni, L., Maeda, T., Marchi, V., Martín, E., Morgan, C., Mutlu, A., Nogolová, A., ... Marschik, P. B. (2019). Cerebral Palsy: Early Markers of Clinical Phenotype and Functional Outcome. Journal of Clinical Medicine, 8(10), 1616. https://doi.org/10.3390/jcm8101616