Prevalence of ADHD in Accident Victims: Results of the PRADA Study

 ,
,
Abstract
:1. Introduction
2. Experimental Section
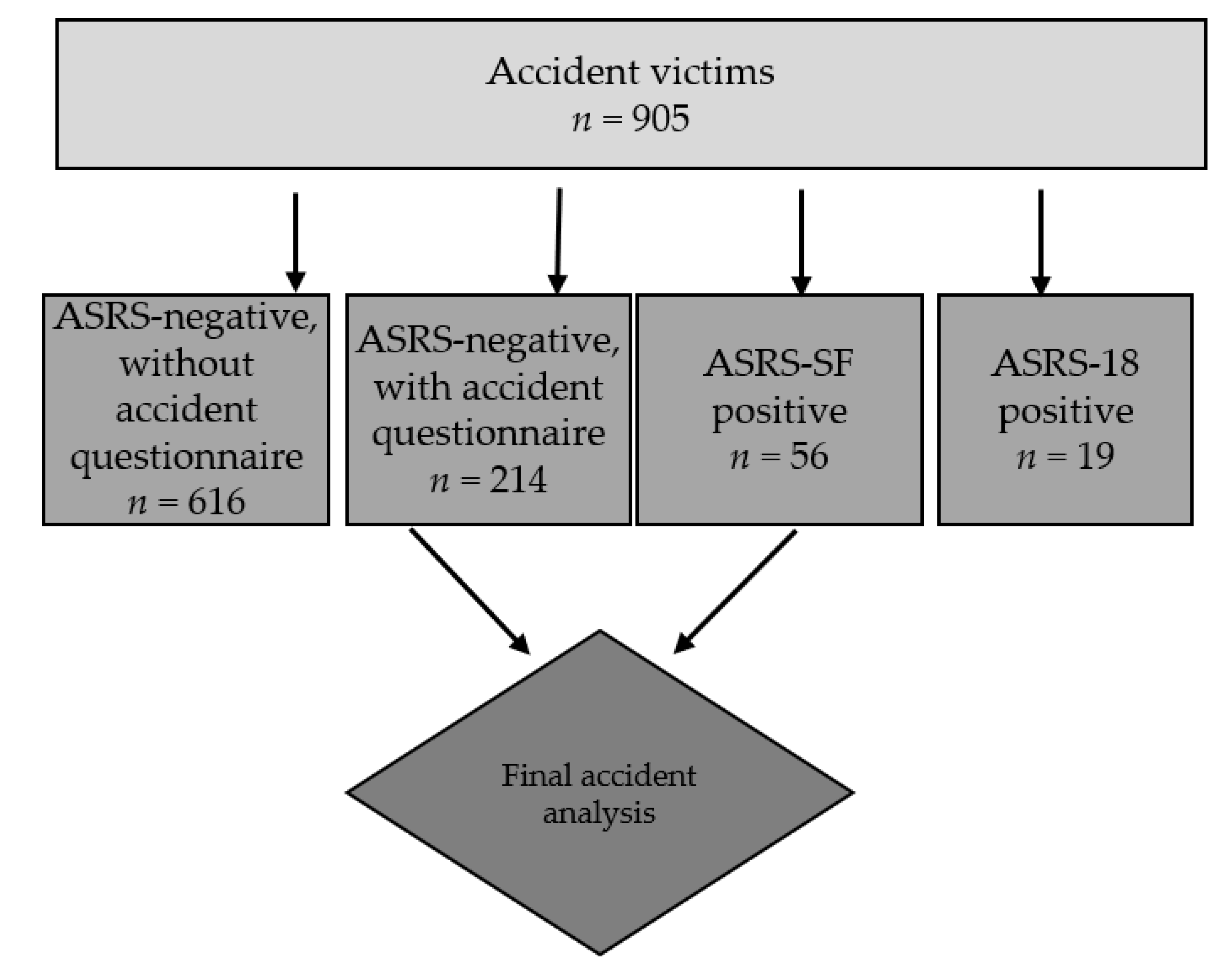
2.1. Participants
2.2. Questionnaires
2.2.1. Adult ADHD Self-Report Scale Version 1.1 (ASRSv1.1)
2.2.2. Accident Questionnaire
2.3. Statistical Analysis
3. Results
3.1. ADHD Prevalence
3.2. Differences in Demographic Data Between ADHD and Non-ADHD Accident Victims
3.3. Circumstances and Mechanisms of Accidents
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Biederman, J.; Petty, C.; Faraone, S. P.7.e.001 Adult outcome of attention deficit hyperactivity disorder: A controlled 16-year follow-up study. Eur. Neuropsychopharmacol. 2012, 22, S435. [Google Scholar] [CrossRef]
- Caci, H.M.; Morin, A.J.; Tran, A. Prevalence and Correlates of Attention Deficit Hyperactivity Disorder in Adults from a French Community Sample. J. Nerv. Ment. Dis. 2014, 202, 324–332. [Google Scholar] [CrossRef] [PubMed]
- Caye, A.; Rocha, T.B.; Anselmi, L.; Murray, J.; Menezes, A.M.; Barros, F.C.; Goncalves, H.; Wehrmeister, F.; Jensen, C.M.; Steinhausen, H.C.; et al. Attention-Deficit/Hyperactivity Disorder Trajectories from Childhood to Young Adulthood: Evidence from a Birth Cohort Supporting a Late-Onset Syndrome. JAMA Psychiatry 2016, 73, 705–712. [Google Scholar] [CrossRef] [PubMed]
- Biederman, J. Attention-Deficit/Hyperactivity Disorder: A Selective Overview. Boil. Psychiatry 2005, 57, 1215–1220. [Google Scholar] [CrossRef] [PubMed]
- Bernardi, S.; Faraones, S.V.; Cortese, S.; Kerrdge, B.T.; Pallanti, S.; Wang, S.; Blanco, C. The lifetime impact of attention deficit hyperactivity disorder: Results from the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC). Psychol. Med. 2012, 42, 875–887. [Google Scholar] [CrossRef] [PubMed]
- Jacob, C.P.; Romanos, J.; Dempfle, A.; Heine, M.; Windemuth-Kieselbach, C.; Kruse, A.; Reif, A.; Walitza, S.; Romanos, M.; Strobel, A.; et al. Co-morbidity of adult attention-deficit/hyperactivity disorder with focus on personality traits and related disorders in a tertiary referral center. Eur. Arch. Psychiatry Clin. Neurosci. 2007, 257, 309–317. [Google Scholar] [CrossRef]
- Instanes, J.T.; Klungsøyr, K.; Halmøy, A.; Famser, O.B.; Haavik, J. Adult ADHD and Comorbid Somatic Disease: A Systematic Literature Review. J. Atten. Disord. 2018, 22, 203–228. [Google Scholar] [CrossRef] [PubMed]
- Dalsgaard, S.; Østergaard, S.D.; Leckman, J.F.; Mortensen, P.B.; Pedersen, M.G. Mortality in children, adolescents, and adults with attention deficit hyperactivity disorder: A nationwide cohort study. Lancet 2015, 385, 2190–2196. [Google Scholar] [CrossRef]
- Cox, D.J.; Cox, B.S.; Cox, J. Self-Reported Incidences of Moving Vehicle Collisions and Citations Among Drivers With ADHD: A Cross-Sectional Survey Across the Lifespan. Am. J. Psychiatry 2011, 168, 329–330. [Google Scholar] [CrossRef]
- Koisaari, T.; Michelsson, K.; Holopainen, J.M.; Maksimainen, R.; Päivänsalo, J.; Rantala, K.; Tervo, T. Traffic and Criminal Behavior of Adults with Attention-Deficit/Hyperactivity with A Prospective Follow-Up from Birth to the Age of 40 Years. Traffic Inj. Prev. 2015, 16, 824–830. [Google Scholar] [CrossRef]
- Adeyemo, B.O.; Biederman, J.; Zafonte, R.; Kagan, E.; Spencer, T.J.; Uchida, M.; Kenworthy, T.; Spencer, A.E.; Faraone, S.V. Mild traumatic brain injury and ADHD: A systematic review of the literature and meta-analysis. J. Atten. Disord. 2014, 18, 576–584. [Google Scholar] [CrossRef]
- Ruiz-Goikoetxea, M.; Cortese, S.; Magallón, S.; Luis, E.O.; De Castro-Manglano, P.; Soutullo, C.; Arrondo, G.; Zallo, N.A.; Aznarez-Sanado, M. Risk of unintentional injuries in children and adolescents with ADHD and the impact of ADHD medications: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2018, 84, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Vaa, T. ADHD and relative risk of accidents in road traffic: A meta-analysis. Accid. Anal. Prev. 2014, 62, 415–425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuermaier, A.B.; Tucha, L.; Evans, B.L.; Koerts, J.; Waard, D.; Brookhuis, K.; Aschenbrenner, S.; Thome, J.; Lange, K.W.; Tucha, O. Driving and attention deficit hyperactivity disorder. J. Neural Transm. 2017, 124, 55–67. [Google Scholar] [CrossRef] [PubMed]
- Philip, P.; Micoulaud-Franchi, J.-A.; Lagarde, E.; Taillard, J.; Canel, A.; Sagaspe, P.; Bioulac, S. Attention Deficit Hyperactivity Disorder Symptoms, Sleepiness and Accidental Risk in 36140 Regularly Registered Highway Drivers. PLoS ONE 2015, 10, e0138004. [Google Scholar] [CrossRef] [PubMed]
- El Farouki, K.; Lagarde, E.; Orriols, L.; Bouvard, M.-P.; Contrand, B.; Galéra, C. The Increased Risk of Road Crashes in Attention Deficit Hyperactivity Disorder (ADHD) Adult Drivers: Driven by Distraction? Results from a Responsibility Case-Control Study. PLoS ONE 2014, 9, e115002. [Google Scholar] [CrossRef] [PubMed]
- Dalsgaard, S.; Leckman, J.F.; Mortensen, P.B.; Nielsen, H.S.; Simonsen, M. Effect of drugs on the risk of injuries in children with attention deficit hyperactivity disorder: A prospective cohort study. Lancet Psychiatry 2015, 2, 702–709. [Google Scholar] [CrossRef]
- Biederman, J.; Fried, R.; Hammerness, P.; Surman, C.; Mehler, B.; Petty, C.R.; Faraone, S.V.; Miller, C.; Bourgeois, M.; Meller, B.; et al. The effects of lisdexamfetamine dimesylate on the driving performance of young adults with ADHD: A randomized, double-blind, placebo-controlled study using a validated driving simulator paradigm. J. Psychiatr. Res. 2012, 46, 484–491. [Google Scholar] [CrossRef] [PubMed]
- Schlander, M.; Schwarz, O.; Trott, G.E.; Viapiano, M.; Bonauer, N. Who cares for patients with attention-deficit/hyperactivity disorder (ADHD)? Insights from Nordbaden (Germany) on administrative prevalence and physician involvement in health care provision. Eur. Child Adolesc. Psychiatry 2007, 16, 430–438. [Google Scholar] [CrossRef] [PubMed]
- Schlander, M.; Trott, G.-E.; Schwarz, O. The health economics of attention deficit hyperactivity disorder in Germany. Part 1: Health care utilization and cost of illness. Der Nervenarzt 2010, 81, 289–300. [Google Scholar] [CrossRef] [PubMed]
- Wolff, S.; Queiser, K.; Wessendorf, L.; Meier, A.M.; Verdenhalven, M.; Grimm, O.; Reimertz, C.; Nau, C.; Klos, M.; Reif, A.; et al. Accident patterns in trauma surgery patients with and without self-reported ADHD. J. Neural Transm. 2019, 126, 1163–1173. [Google Scholar] [CrossRef] [PubMed]
- Adler, L.A.; Spencer, T.; Faraone, S.V.; Kessler, R.C.; Howes, M.J.; Biederman, J.; Secnik, K. Validity of Pilot Adult ADHD Self- Report Scale (ASRS) to Rate Adult ADHD Symptoms. Ann. Clin. Psychiatry 2006, 18, 145–148. [Google Scholar] [CrossRef] [PubMed]
- Buchli-Kammermann, J.; Corbisiero, S.; Stieglitz, R.-D. Screening der Aufmerksamkeitsdefizit-/Hyperaktivitätsstörung (ADHS) im Erwachsenenalter: Validierung der deutschen Version der ASRS-v1.1. Klinische Diagnostik und Evaluation 2011, 4, 219–235. [Google Scholar]
- Kessler, R.C.; Adler, L.; Ames, M.; Demler, O.; Faraone, S.; Hiripi, E.; Howes, M.J.; Jin, R.; Secnik, K.; Spencer, T.; et al. The World Health Organization adult ADHD self-report scale (ASRS): A short screening scale for use in the general population. Psychol. Med. 2005, 35, 245–256. [Google Scholar] [CrossRef] [PubMed]
- Liou, Y.-J.; Wei, H.-T.; Chen, M.-H.; Hsu, J.-W.; Huang, K.-L.; Bai, Y.-M.; Su, T.-P.; Li, C.-T.; Yang, A.C.; Tsai, S.-J.; et al. Risk of Traumatic Brain Injury Among Children, Adolescents, and Young Adults with Attention-Deficit Hyperactivity Disorder in Taiwan. J. Adolesc. Heal. 2018, 63, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Bron, T.I.; Bijlenga, D.; Breuk, M.; Michielsen, M.; Beekman, A.T.; Kooij, J.S. Risk factors for adverse driving outcomes in Dutch adults with ADHD and controls. Accid. Anal. Prev. 2018, 111, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Man, K.K.C.; Ip, P.; Chan, E.W.; Law, S.-L.; Leung, M.T.Y.; Ma, E.X.Y.; Quek, W.-T.; Wong, I.C.K. Effectiveness of Pharmacological Treatment for Attention-Deficit/Hyperactivity Disorder on Physical Injuries: A Systematic Review and Meta-Analysis of Observational Studies. CNS Drugs 2017, 31, 1043–1055. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kooij, S.J.; Bejerot, S.; Blackwell, A.; Caci, H.; Casas-Brugué, M.; Carpentier, P.J.; Edvinsson, D.; Fayyad, J.; Foeken, K.; Fitzgerald, M.; et al. European consensus statement on diagnosis and treatment of adult ADHD: The European Network Adult ADHD. BMC Psychiatry 2010, 10, 67. [Google Scholar] [CrossRef]
- De Zwaan, M.; Gruss, B.; Müller, A.; Graap, H.; Martin, A.; Glaesmer, H.; Hilbert, A.; Philipsen, A. The estimated prevalence and correlates of adult ADHD in a German community sample. Eur. Arch. Psychiatry Clin. Neurosci. 2012, 262, 79–86. [Google Scholar] [CrossRef]
- Fayyad, J.; De Graaf, R.; Kessler, R.; Alonso, J.; Angermeyer, M.; Demyttenaere, K.; De Girolamo, G.; Haro, J.M.; Karam, E.G.; Lara, C.; et al. Cross-national prevalence and correlates of adult attention-deficit hyperactivity disorder. Br. J. Psychiatry 2007, 190, 402–409. [Google Scholar] [CrossRef] [Green Version]
- Yeh, C.-B.; Gau, S.S.-F.; Kessler, R.C.; Wu, Y.-Y. Psychometric properties of the Chinese version of the adult ADHD Self-report Scale. Int. J. Methods Psychiatr. Res. 2008, 17, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Hartman, C.A.; Haavik, J.; Harro, J.; Klungsøyr, K.; Hegvik, T.-A.; Wanders, R.; Ottosen, C.; Dalsgaard, S.; Faraone, S.V.; et al. Common psychiatric and metabolic comorbidity of adult attention-deficit/hyperactivity disorder: A population-based cross-sectional study. PLoS ONE 2018, 13, e0204516. [Google Scholar] [CrossRef] [PubMed]
- Hesson, J.; Fowler, K. Prevalence and Correlates of Self-Reported ADD/ADHD in a Large National Sample of Canadian Adults. J. Atten. Disord. 2015, 22, 191–200. [Google Scholar] [CrossRef] [PubMed]
- Chang, Z.; Lichtenstein, P.; D’Onofrio, B.M.; Sjölander, A.; Larsson, H. Serious transport accidents in adults with attention-deficit/hyperactivity disorder and the effect of medication: A population-based study. JAMA Psychiatry 2014, 71, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Chien, W.-C.; Chung, C.-H.; Lin, F.-H.; Yeh, C.-B.; Huang, S.-Y.; Lu, R.-B.; Chang, H.-A.; Kao, Y.-C.; Chiang, W.-S.; Chou, Y.-C.; et al. The risk of injury in adults with attention-deficit hyperactivity disorder: A nationwide, matched-cohort, population-based study in Taiwan. Res. Dev. Disabil. 2017, 65, 57–73. [Google Scholar] [CrossRef] [PubMed]
- Swensen, A.; Birnbaum, H.; Benhamadi, R.; Greenberg, P.; Cremieux, P.; Secnik, K. Incidence and costs of accidents among attention-deficit/hyperactivity disorder patients. J. Adolesc. Heal. 2004, 35, 346.e1. [Google Scholar] [CrossRef]
- Narad, M.; Garner, A.A.; Brassell, A.A.; Saxby, D.; Antonini, T.N.; O’Brien, K.M.; Tamm, L.; Matthews, G.; Epstein, J.N. The Impact of Distraction on the Driving Performance of Adolescents with and without Attention Deficit Hyperactivity Disorder. JAMA Pediatrics 2013, 167, 933–938. [Google Scholar] [CrossRef] [PubMed]
- Jerome, L.; Segal, A.; Habinski, L. What We Know About ADHD and Driving Risk: A Literature Review, Meta-Analysis and Critique. J. Can. Acad. Child Adolesc. Psychiatry 2006, 15, 105–125. [Google Scholar] [PubMed]
- Jerome, L.; Habinski, L.; Segal, A. Attention-deficit/hyperactivity disorder (ADHD) and driving risk: A review of the literature and a methodological critique. Curr. Psychiatry Rep. 2006, 8, 416–426. [Google Scholar] [CrossRef] [PubMed]
- Kittel-Schneider, S.; Spiegel, S.; Renner, T.; Romanos, M.; Reif, A.; Reichert, S.; Heupel, J.; Schnetzler, L.; Stopper, H.; Jacob, C. Cytogenetic Effects of Chronic Methylphenidate Treatment and Chronic Social Stress in Adults with Attention-Deficit/Hyperactivity Disorder. Pharmacopsychiatry 2016, 49, 146–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christiansen, H.; Oades, R.D.; Psychogiou, L.; Hauffa, B.P.; Sonuga-Barke, E.J. Does the cortisol response to stress mediate the link between expressed emotion and oppositional behavior in Attention-Deficit/Hyperactivity-Disorder (ADHD)? Behav. Brain Funct. 2010, 6, 45. [Google Scholar] [CrossRef] [PubMed]
- Hirvikoski, T.; Lindholm, T.; Nordenström, A.; Nordström, A.-L.; Lajic, S. High self-perceived stress and many stressors, but normal diurnal cortisol rhythm, in adults with ADHD (attention-deficit/hyperactivity disorder). Horm. Behav. 2009, 55, 418–424. [Google Scholar] [CrossRef] [PubMed]
- Hatzinger, M.; Brand, S.; Perren, S.; Von Wyl, A.; Von Klitzing, K.; Holsboer-Trachsler, E. Hypothalamic–pituitary–adrenocortical (HPA) activity in kindergarten children: Importance of gender and associations with behavioral/emotional difficulties. J. Psychiatr. Res. 2007, 41, 861–870. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| ADHD (ASRS-SF) | ADHD (ASRS-18) | All Controls | Selected Controls | p | |
|---|---|---|---|---|---|
| Sex (m/f) | 40/16 | 14/5 | 537/293 | 147/67 | n.s. |
| Age (years, mean ± SD) | 40.7 ± 15.2 | 39.1 ± 13.6 | 47.4 ± 15.3 | 48.6 ± 13.2 | <0.0001 |
| ADHD | Controls | p | |
|---|---|---|---|
| Sex (m/f) | 40/16 | 143/71 | n.s. |
| Age (mean ± SD) | 40.7 ± 15.2 | 48.6 ± 13.2 | 0.001 |
| Comorbidities | n | n | |
| Affective Disorder | 4/44 | 6/208 | 0.071 |
| Personality Disorders | 0/48 | 0/214 | n.s. |
| Eating Disorder | 0/48 | 0/214 | n.s. |
| Anxiety Disorder | 1/47 | 0/214 | 0.034 |
| Adjustment Disorder | 1/48 | 0/214 | 0.036 |
| Schizophrenia | 1/47 | 0/214 | 0.034 |
| Substance Abuse | 4/45 | 1/212 | <0.0001 |
| ADHD | 7/42 | 2/212 | <0.0001 |
| Skeletal Disease | 7/43 | 14/200 | 0.079 |
| Cardiovascular Disease | 9/41 | 54/160 | n.s. |
| Thyroid Disease | 3/46 | 16/198 | n.s. |
| Metabolic Disease | 6/43 | 13/201 | n.s. |
| Pulmonary Disease | 6/44 | 13/203 | n.s. |
| Neurological Disease | 5/44 | 10/203 | n.s. |
| Chronic pain | 5/45 | 3/210 | 0.001 |
| Other | 9/41 | 36/178 | n.s. |
| Regular medication (yes/no) | 26/24 | 96/118 | n.s. |
| Sedatives (yes/no) | 4/45 | 1/211 | <0.0001 |
| Other psychopharmacological medication (yes/no) | 8/41 | 5/208 | <0.0001 |
| CVD Medication (yes/no) | 8/41 | 57/156 | n.s. |
| Anticoagulants/thrombocyte-aggregation-inhibitors (yes/no) | 0/48 | 6/207 | n.s. |
| Pain medication (yes/no) | 6/42 | 10/203 | 0.042 |
| Stimulant medication (yes/no) | 2/46 | 0/213 | 0.003 |
| Other (yes/no) | 14/34 | 51/161 | n.s. |
| p | 95% Confidence Interval | ||
|---|---|---|---|
| Lower Bound | Upper Bound | ||
| In thoughts | 0.04 | 0.05 | 0.97 |
| Substance influence | 0.41 | 0.004 | 9.67 |
| Alcohol | 0.85 | 0.03 | 56.98 |
| Illegal drugs | 0.72 | 0.04 | 8.77 |
| Stressed before accident | 0.21 | 0.27 | 1.33 |
| Having had an argument | 0.09 | 0.05 | 1.25 |
| Overconfidence | 0.02 | 0.18 | 0.87 |
| ADHD (n) | Controls (n) | p | |
|---|---|---|---|
| Road traffic | 20 | 63 | n.s. |
| At home | 7 | 19 | n.s. |
| Sports | 8 | 38 | n.s. |
| Work/School/University | 10 | 63 | n.s. |
| Public place | 5 | 28 | n.s. |
| Other | 0 | 3 | n.s. |
| Missing | 6 | 0 | |
| Self-inflicted (yes/no) | 35/14 | 121/92 | 0.06 |
| Missing | 6 | 0 | |
| Substance influence (yes/no) | 11/39 | 11/202 | <0.0001 |
| Alcohol (yes/no) | 10/40 | 10/203 | <0.0001 |
| Illegal drugs (yes/no) | 5/45 | 2/211 | <0.0001 |
| Missing | 6 | 1 | |
| Medication (yes/no) | 4/46 | 2/212 | 0.003 |
| Missing | 6 | 0 | |
| Sedatives (yes/no) | 3/47 | 1/212 | 0.004 |
| Other psychopharmacological medication (yes/no) | 1/49 | 0/214 | 0.038 |
| CVD medication (yes/no) | 1/49 | 0/214 | 0.038 |
| Anticoagulants/thrombocyte-aggregation inhibitors (yes/no) | 0/50 | 0/214 | n.s. |
| Pain medication (yes/no) | 0/50 | 1/213 | n.s. |
| Stimulants (yes/no) | 0/50 | 0/214 | n.s. |
| Other (yes/no) | 1/49 | 0/214 | 0.038 |
| Distraction (yes/no) | 18/32 | 36/177 | 0.01 |
| Missing | 0 | 1 | |
| Smartphone (yes/no) | 2/48 | 2/211 | n.s. |
| Talking to someone (yes/no) | 4/46 | 4/209 | 0.023 |
| External factors (yes/no) | 3/47 | 18/195 | n.s. |
| In thoughts (yes/no) | 6/44 | 5/208 | 0.002 |
| Listening to music (yes/no) | 1/40 | 0/213 | n.s. |
| Other (yes/no) | 0/50 | 8/205 | n.s. |
| Missing | 6 | 1 | |
| Currently stressed (yes/no) | 25/24 | 62/152 | 0.003 |
| Missing | 6 | 0 | |
| Stressed before accident (yes/no) | 18/32 | 35/179 | 0.002 |
| Missing (yes/no) | 6 | 0 | |
| Argument (yes/no) | 5/45 | 3/211 | 0.001 |
| Pressure situation (yes/no) | 10/40 | 20/194 | 0.033 |
| Bereavement (yes/no) | 0/50 | 0/214 | n.s. |
| Other (yes/no) | 2/48 | 8/206 | n.s. |
| Missing | 6 | 0 | |
| Overconfidence (Yes/no) | 19/31 | 30/183 | 0.0004 |
| Lack of sleep (yes/no) | 10/40 | 19/195 | 0.058 |
| Previous accidents (yes/no) | 21/28 | 35/179 | <0.0001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kittel-Schneider, S.; Wolff, S.; Queiser, K.; Wessendorf, L.; Meier, A.M.; Verdenhalven, M.; Brunkhorst-Kanaan, N.; Grimm, O.; McNeill, R.; Grabow, S.; et al. Prevalence of ADHD in Accident Victims: Results of the PRADA Study. J. Clin. Med. 2019, 8, 1643. https://doi.org/10.3390/jcm8101643
Kittel-Schneider S, Wolff S, Queiser K, Wessendorf L, Meier AM, Verdenhalven M, Brunkhorst-Kanaan N, Grimm O, McNeill R, Grabow S, et al. Prevalence of ADHD in Accident Victims: Results of the PRADA Study. Journal of Clinical Medicine. 2019; 8(10):1643. https://doi.org/10.3390/jcm8101643
Chicago/Turabian StyleKittel-Schneider, Sarah, Sarah Wolff, Kristin Queiser, Leonie Wessendorf, Anna Maria Meier, Moritz Verdenhalven, Nathalie Brunkhorst-Kanaan, Oliver Grimm, Rhiannon McNeill, Sascha Grabow, and et al. 2019. "Prevalence of ADHD in Accident Victims: Results of the PRADA Study" Journal of Clinical Medicine 8, no. 10: 1643. https://doi.org/10.3390/jcm8101643
APA StyleKittel-Schneider, S., Wolff, S., Queiser, K., Wessendorf, L., Meier, A. M., Verdenhalven, M., Brunkhorst-Kanaan, N., Grimm, O., McNeill, R., Grabow, S., Reimertz, C., Nau, C., Klos, M., & Reif, A. (2019). Prevalence of ADHD in Accident Victims: Results of the PRADA Study. Journal of Clinical Medicine, 8(10), 1643. https://doi.org/10.3390/jcm8101643