Home-Based Exergaming on Preschoolers’ Energy Expenditure, Cardiovascular Fitness, Body Mass Index and Cognitive Flexibility: A Randomized Controlled Trial




Abstract
:1. Introduction
2. Methods
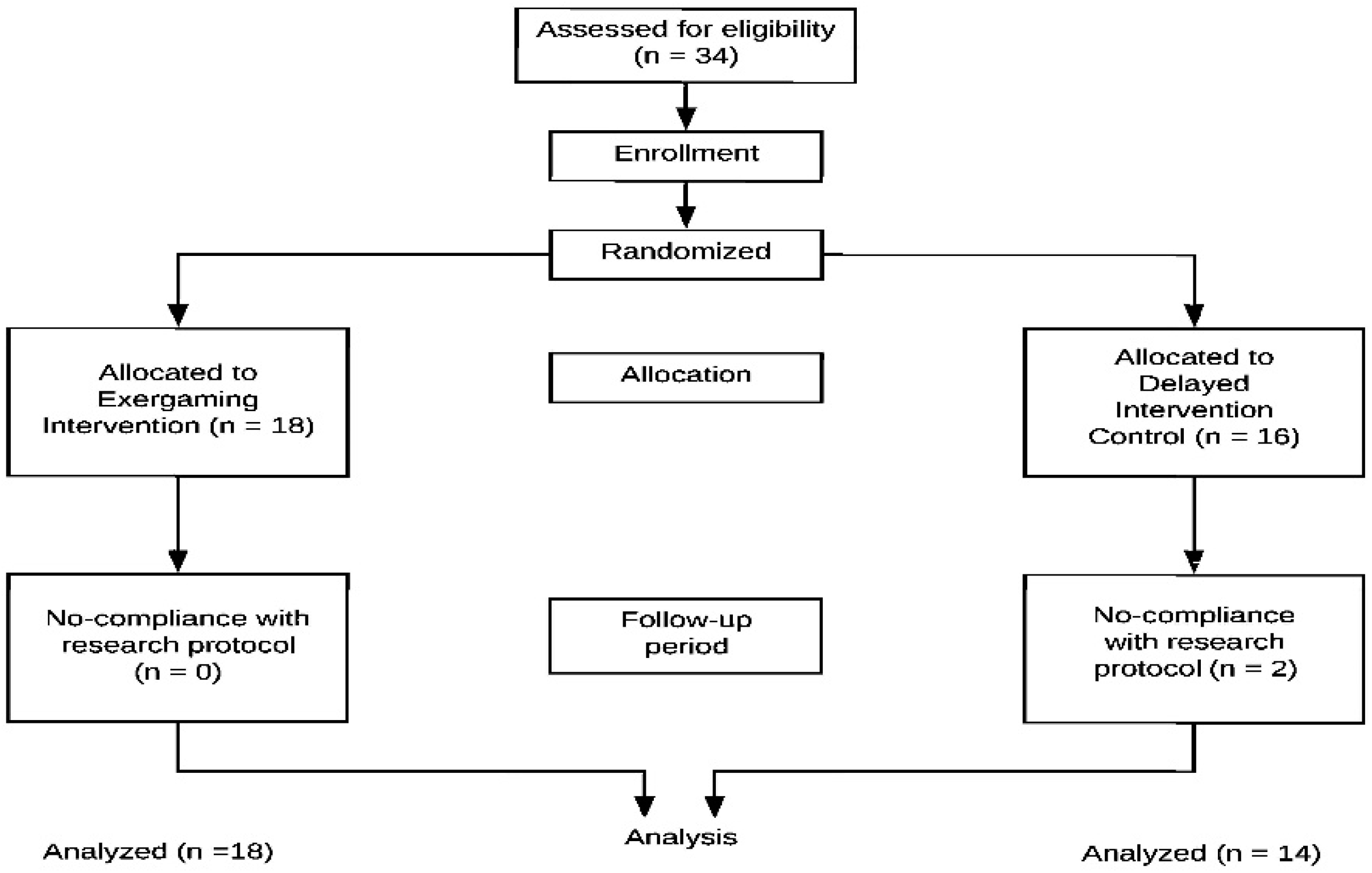
2.1. Research Design
2.2. Participants
2.3. Outcome Measures
2.4. Intervention
2.5. Procedures
2.6. Data Analysis
3. Results
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Vierola, A.; Suominen, A.L.; Lindi, V.; Viitasalo, A.; Ikävalko, T.; Lintu, N.; Väistö, J.; Kellokoski, J.; Närhi, M.; Lakka, T.A. Associations of sedentary behavior, physical activity, cardiorespiratory fitness, and body fat content with pain conditions in children: The physical activity and nutrition in children study. J. Pain 2016, 17, 845–853. [Google Scholar] [CrossRef]
- Geiss, L.S.; Kirtland, K.; Lin, J.; Shrestha, S.; Thompson, T.; Albright, A.; Gregg, E.W. Changes in diagnosed diabetes, obesity, and physical inactivity prevalence in US counties, 2004–2012. PLoS ONE 2017, 3, e0173428. [Google Scholar] [CrossRef]
- Blanca, M.C.; Gonz, R.E.; Schmidt-riovalle, J. Associations between body composition, nutrition, and physical activity in young adults. Am. J. Hum. Biol. 2017, 29, e22903. [Google Scholar] [CrossRef]
- Taylor, R.W.; Murdoch, L.; Carter, P.; Gerrard, D.F.; Williams, S.M.; Taylor, B.J. Longitudinal study of physical activity and inactivity in preschoolers: The FLAME study. Med. Sci. Sports Exerc. 2009, 41, 96–102. [Google Scholar] [CrossRef]
- Berry, D. Early Childhood Health Disparities, Biological Embedding, and Life-Course Health. In The Wiley Handbook of Early Childhood Development Programs, Practices, and Policies; Votruba-Drzal, E., Dearing, E., Eds.; Wiley: Hoboken, NJ, USA, 2017; pp. 35–65. [Google Scholar]
- Gordon-Larsen, P.; Laska, M.; Page, P.; Popkin, B.M. Inequality in the Built Environment Underlies Key Health Disparities in Physical Activity and Obesity. Pediatrics 2006, 117, 417–424. [Google Scholar] [CrossRef] [Green Version]
- Moore, L.V.; Roux, A.V.D.; Evenson, K.R.; McGinn, A.P.; Brines, S.J. Availability of recreational resources in minority and low socioeconomic status areas. Am. J. Prev. Med. 2008, 34, 16–22. [Google Scholar] [CrossRef]
- Xiong, S.; Li, X.; Tao, K. Effects of Structured Physical Activity Program on Chinese Young Children’s Executive Functions and Perceived Physical Competence in a Day Care Center. BioMed Res. Int. 2017, 2017, 1–6. [Google Scholar] [CrossRef]
- Nyström, C.D.; Sandin, S.; Henriksson, P.; Henriksson, H.; Maddison, R.; Löf, M. A 12-month follow-up of a mobile-based (mHealth) obesity prevention intervention in pre-school children: The MINISTOP randomized controlled trial. BMC Public Health 2018, 18, 658. [Google Scholar]
- Luybli, M.; Schmillen, H.; Sotos-Prieto, M. School-Based Interventions in Low Socioeconomic Settings to Reduce Obesity Outcomes among Preschoolers: A Scoping Review. Nutrients 2019, 11, 1518. [Google Scholar] [CrossRef]
- Handel, M.N.; Larsen, S.C.; Rohde, J.F.; Stougaard, M.; Olsen, N.J.; Heitmann, B.L. Effects of the Healthy Start randomized intervention trial on physical activity among normal weight preschool children predisposed to overweight and obesity. PLoS ONE 2017, 12, e0185266. [Google Scholar] [CrossRef]
- Hacke, C.; Ketelhut, S.; Wendt, U.; Müller, G.; Schlesner, C.; Ketelhut, K. Effectiveness of a physical activity intervention in preschoolers: A cluster-randomized controlled trial. Scand. J. Med. Sci. Sports 2019, 29, 742–752. [Google Scholar] [CrossRef]
- Henriksson, P.; Nystro, C.D.; Leppa, M.H.; Lo, M. Longitudinal physical activity, body composition, and physical fitness in preschoolers. Med. Sci. Sports Exerc. 2017, 49, 2078–2085. [Google Scholar] [CrossRef]
- Puder, J.J.; Schindler, C.; Zahner, L.; Kriemler, S. Body mass index, fitness and metabolic risk in children: A cross-sectional and longitudinal study. Int. J. Pediatr. Obes. 2011, 6, 297–306. [Google Scholar] [CrossRef]
- Davy, B.M.; Harrell, K.; Stewart, J.; King, D.S. Body weight status, dietary habits, and physical activity levels of middle school-aged children in rural Mississippi. South. Med. J. 2004, 97, 571–577. [Google Scholar] [CrossRef]
- Grundy, S.M.; Blackburn, G.; Higgins, M.; Lauer, R.; Perri, M.G.; Ryan, D. Physical activity in the prevention and treatment of obesity and its comorbidities: Evidence report of independent panel to assess the role of physical activity in the treatment of obesity and its comorbidities. Med. Sci. Sports Exerc. 1999, 31, 1493–1500. [Google Scholar] [CrossRef]
- Fan, X.; Cao, Z.-B.; Chen, P. Physical activity among Chinese school-aged children: National prevalence estimates from the 2016 Physical Activity and Fitness in China—The Youth Study. J. Sport Health Sci. 2017, 6, 388–394. [Google Scholar] [CrossRef]
- Malina, R.M. Physical Activity: Relationship to Growth, Maturation, and Physical Fitness. In Physical Activity, Fitness, & Health; Bouchard, C., Shephard, R., Stephens, T., Eds.; Human Kinetics: Champaign, IL, USA, 1994; pp. 918–930. [Google Scholar]
- Sharpe, P.A.; Granner, M.L.; Hutto, B.; Ainsworth, B.E.; Cook, A. Association of body mass index to meeting physical activity recommendations. Am. J. Health Behav. 2004, 28, 522–530. [Google Scholar] [CrossRef]
- Sallis, J.F.; McKenzie, T.L.; Alcaraz, J.E. Habitual Physical Activity and Health-Related Physical Fitness in Fourth-Grade Children. Arch. Pediatr. Adolesc. Med. 1993, 147, 890–896. [Google Scholar] [CrossRef]
- Fairclough, S.J.; Dumuid, D.; Taylor, S.; Curry, W.; McGrane, B.; Stratton, G.; Maher, C.; Olds, T. Fitness, fatness and the reallocation of time between children’s daily movement behaviours: An analysis of compositional data. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 64. [Google Scholar] [CrossRef]
- Davis, C.L.; Tomporowski, P.D.; McDowell, J.E.; Austin, B.P.; Miller, P.H.; Yanasak, N.E.; Allison, J.D.; Naglieri, J.A. Exercise improves executive function and achievement and alters brain activation in overweight children: A randomized, controlled trial. Health Psychol. 2011, 30, 91–98. [Google Scholar] [CrossRef]
- Kamijo, K.; Pontifex, M.B.; O’Leary, K.C.; Scudder, M.R.; Wu, C.T.; Castelli, D.M.; Hillman, C.H. The effects of an afterschool physical activity program on working memory in preadolescent children. Dev. Sci. 2011, 14, 1046–1058. [Google Scholar] [CrossRef] [Green Version]
- Niederer, I.; Kriemler, S.; Gut, J.; Hartmann, T.; Schindler, C.; Barral, J.; Puder, J.J. Relationship of aerobic fitness and motor skills with memory and attention in preschoolers (Ballabeina): A cross-sectional and longitudinal study. BMC Pediatr. 2011, 11, 34. [Google Scholar] [CrossRef]
- Pesce, C.; Garrido-miguel, M. Academic achievement and physical activity: A meta-analysis. Pediatrics 2019, 140, e20171498. [Google Scholar]
- Gao, Z.; Zeng, N.; Pope, Z. Active Video Games and Physical Activity Promotion. In Technology in Physical Activity and Health Promotion; Routledge: Abingdon, UK, 2017; pp. 165–203. [Google Scholar]
- Biddiss, E.; Irwin, J. Active video games to promote physical activity in children and youth: A systematic review. Arch. Pediatr. Adolesc. Med. 2010, 164, 664–672. [Google Scholar] [CrossRef]
- Graf, D.L.; Pratt, L.V.; Hester, C.N.; Short, K.R. Playing Active Video Games Increases Energy Expenditure in Children. Pediatrics 2009, 124, 534–540. [Google Scholar] [CrossRef]
- Gao, Z.; Chen, S. Are field-based exergames useful in preventing childhood obesity? A systematic review. Obes. Rev. 2014, 15, 676–691. [Google Scholar] [CrossRef]
- Gao, Z.; Chen, S.; Pasco, D.; Pope, Z. Effects of active video games on physiological and psychological outcomes among children and adolescents: A meta-analysis. Obes. Rev. 2015, 16, 783–794. [Google Scholar] [CrossRef]
- Baranowski, T.; Baranowski, J.; Thompson, D.; Buday, R.; Jago, R.; Griffith, M.J.; Islam, N.; Nguyen, N.; Watson, K.B. Video game play, child diet, and physical activity behavior change a randomized clinical trial. Am. J. Prev. Med. 2011, 40, 33–38. [Google Scholar] [CrossRef]
- Gao, Z.; Hannon, J.C.; Newton, M.; Huang, C. The effects of curricular activity on students’ situational motivation and physical activity levels. Res. Q. Exerc. Sport 2011, 82, 536–544. [Google Scholar] [CrossRef]
- Gao, Z.; Hannan, P.F.; Xiang, P.; Stodden, D.; Valdez, V. Effect of active video game based exercise on urban Latino children’s physical health and academic performance. Am. J. Prev. Med. 2013, 44, s240–s246. [Google Scholar] [CrossRef]
- Gao, Z.; Pope, Z.; Lee, J.E.; Stodden, D.; Roncesvalles, N.; Pasco, D.; Huang, C.C.; Feng, D. Impact of exergaming on young children’s school day energy expenditure and moderate-to-vigorous physical activity levels. J. Sport Health Sci. 2017, 6, 11–16. [Google Scholar] [CrossRef]
- Staiano, A.E.; Beyl, R.A.; Hsia, D.S.; Katzmarzyk, P.T.; Newton, R.L., Jr. Twelve weeks of dance exergaming in overweight and obese adolescent girls: Transfer effects on physical activity, screen time, and self-efficacy. J. Sport Health Sci. 2017, 6, 4–10. [Google Scholar] [CrossRef]
- Edwards, J.; Jeffrey, S.; May, T.; Rinehart, N.J.; Barnett, L.M. Does playing a sports active video game improve object control skills of children with autism spectrum disorder? J. Sport Health Sci. 2017, 6, 17–24. [Google Scholar] [CrossRef]
- Pasco, D.; Roure, C.; Kermarrec, G.; Pope, Z.; Gao, Z. The effects of a bike active video game on players’ physical activity and motivation. J. Sport Health Sci. 2017, 6, 25–32. [Google Scholar] [CrossRef]
- Gao, Z.; Podlog, L.; Huang, C. Associations among children’s situational motivation, physical activity participation, and enjoyment in an interactive dance game. J. Sport Health Sci. 2012, 2, 122–128. [Google Scholar] [CrossRef]
- Gao, Z.; Zhang, T.; Stodden, D.F. Children’s physical activity levels and their psychological correlated in interactive dance versus aerobic dance. J. Sport Health Sci. 2013, 2, 146–151. [Google Scholar] [CrossRef]
- Gao, Z. Motivated but Not Active: The Dilemmas of Incorporating Interactive Dance into Gym Class. J. Phys. Act. Health 2012, 9, 794–800. [Google Scholar] [CrossRef]
- LeapTV Education Gaming System. Available online: https://www.leapfrog.com/en-us/products/leaptv (accessed on 1 May 2019).
- Foley, L.; Maddison, R. Use of Active Video Games to Increase Physical Activity in Children: A (Virtual) Reality? Pediatr. Exerc. Sci. 2010, 22, 7–20. [Google Scholar] [CrossRef] [Green Version]
- Ni Mhurchu, C.; Maddison, R.; Jiang, Y.; Jull, A.; Prapavessis, H.; Rodgers, A. Couch potatoes to jumping beans: A pilot study of the effect of active video games on physical activity in children. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 8–12. [Google Scholar] [CrossRef]
- Gao, Z.; Huang, C.; Liu, T.; Xiong, W. Impact of interactive dance games on urban children’s physical activity correlates and behavior. J. Exerc. Sci. Fitness 2012, 10, 107–112. [Google Scholar] [CrossRef]
- Peng, W.; Crouse, J.C.; Lin, J.H. Using active video games for physical activity promotion: A systematic review of the current state of research. Health Educ. Behav. 2013, 40, 171–192. [Google Scholar] [CrossRef] [PubMed]
- Gao, Z.; Zeng, N.; Pope, Z.C.; Wang, R.; Yu, F. Effects of Exergaming on Motor Skill Competence, Perceived Competence, and Physical Activity in Preschool Children. Med. Sci. Sports Exerc. 2019, 8, 106–113. [Google Scholar]
- Guy, S.; Ratzki-Leewing, A.; Gwadry-Sridhar, F. Moving Beyond the Stigma: Systematic Review of Video Games and Their Potential to Combat Obesity. Int. J. Hypertens. 2011, 2011, 179124. [Google Scholar] [CrossRef] [PubMed]
- Staiano, A.E.; Beyl, R.A.; Guan, W.; Hendrick, C.A.; Hsia, D.S.; Newton, R.L. Home-based exergaming among children with overweight and obesity: A randomized clinical trial. Pediatr. Obes. 2018, 13, 724–733. [Google Scholar] [CrossRef] [PubMed]
- Baranowski, T.; Abdelsamad, D.; Baranowski, J.; O’Connor, T.M.; Thompson, D.; Barnett, A.; Cerin, E.; Chen, T.-A. Impact of an Active Video Game on Healthy Children’s Physical Activity. Pediatrics 2012, 129, e636–e642. [Google Scholar] [CrossRef] [PubMed]
- Xiong, S.; Zhang, P.; Gao, Z. Effects of Exergaming on Preschoolers’ Executive Functions and Perceived Competence: A Pilot Randomized Trial. J. Clin. Med. 2019, 8, 469. [Google Scholar] [CrossRef]
- Van Zutphen, M.; Bell, A.C.; Kremer, P.J.; A Swinburn, B. Association between the family environment and television viewing in Australian children. J. Paediatr. Child. Health 2007, 43, 458–463. [Google Scholar] [CrossRef]
- Reilly, J.J.; Jackson, D.M.; Montgomery, C.; A Kelly, L.; Slater, C.; Grant, S.; Paton, J.Y. Total energy expenditure and physical activity in young Scottish children: Mixed longitudinal study. Lancet 2004, 363, 211–212. [Google Scholar] [CrossRef]
- G*Power 3.1. Available online: http://www.gpower.hhu.de/en.html (accessed on 29 September 2019).
- Rothney, M.P.; Brychta, R.J.; Meade, N.N.; Chen, K.Y.; Buchowski, M.S. Validation of the ActiGraph two-regression model for predicting energy expenditure. Med. Sci. Sports Exerc. 2010, 42, 1785–1792. [Google Scholar] [CrossRef]
- Trost, S.G.; McIver, K.L.; Pate, R.R. Conducting accelerometer-based activity assessments in field-based research. Med. Sci. Sports Exerc. 2005, 37, S531–S543. [Google Scholar] [CrossRef]
- Puyau, M.R.; Adolph, A.L.; Vohra, F.A.; Butte, N.F. Validation and Calibration of Physical Activity Monitors in Children. Obes. Res. 2002, 10, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Pate, R.R.; Pfeiffer, K.A.; Trost, S.G.; Ziegler, P.; Dowda, M. Physical Activity among Children Attending Preschools. Pediatrics 2004, 114, 1258–1263. [Google Scholar] [CrossRef] [PubMed]
- Zelazo, P.D. The Dimensional Change Card Sort (DCCS): A method of assessing executive function in children. Nat. Protocols 2006, 1, 297–301. [Google Scholar] [CrossRef] [PubMed]
- Łuczyńska, G.; Pena-Pereira, F.; Tobiszewski, M.; Namieśnik, J. Expectation-Maximization Model for Substitution of Missing Values Characterizing Greenness of Organic Solvents. Molecules 2018, 23, 1292. [Google Scholar] [CrossRef]
- Richardson, J.T. Eta squared and partial eta squared as measures of effect size in educational research. Educ. Res. Rev. 2011, 6, 135–147. [Google Scholar] [CrossRef]
- Ye, S.; Lee, J.E.; Stodden, D.F.; Gao, Z. Impact of Exergaming on Children’s Motor Skill Competence and Health-Related Fitness: A Quasi-Experimental Study. J. Clin. Med. 2018, 7, 261. [Google Scholar] [CrossRef]
- McDonough, D.J.; Pope, Z.C.; Zeng, N.; Lee, J.E.; Gao, Z. Comparison of College Students’ Energy Expenditure, Physical Activity, and Enjoyment during Exergaming and Traditional Exercise. J. Clin. Med. 2018, 7, 433. [Google Scholar] [CrossRef]
- Quan, M.; Pope, Z.; Gao, Z. Examining Young Children’s Physical Activity and Sedentary Behaviors in an Exergaming Program Using Accelerometry. J. Clin. Med. 2018, 7, 302. [Google Scholar] [CrossRef]
- Staiano, A.E.; Abraham, A.A.; Calvert, S.L. Adolescent Exergame Play for Weight Loss and Psychosocial Improvement: A Controlled Physical Activity Intervention. Obesity 2012, 21, 598–601. [Google Scholar] [CrossRef]
- Maddison, R.; Mhurchu, C.N.; Jull, A.; Jiang, Y.; Prapavessis, H.; Rodgers, A. Energy expended playing video console games: An opportunity to increase children’s physical activity? Pediatr. Exerc. Sci. 2007, 19, 334–343. [Google Scholar] [CrossRef]
- Graves, L.E.; Ridgers, N.D.; Williams, K.; Stratton, G.; Atkinson, G.; Cable, N.T. The physiological cost and enjoyment of Wii Fit in adolescents, young adults, and older adults. J. Phys. Act. Health 2010, 7, 393–401. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, J.E.; Hillman, C.H.; Castelli, D.; Etnier, J.L.; Lee, S.; Tomporowski, P.; Lambourne, K.; Szabo-Reed, A.N. Physical Activity, Fitness, Cognitive Function, and Academic Achievement in Children. Med. Sci. Sports Exerc. 2016, 48, 1223–1224. [Google Scholar] [CrossRef] [PubMed]
- Hillman, C.H.; Pontifex, M.B.; Castelli, D.M.; Khan, N.A.; Raine, L.B.; Scudder, M.R.; Drollette, E.S.; Moore, R.D.; Wu, C.-T.; Kamijo, K. Effects of the FITKids Randomized Controlled Trial on Executive Control and Brain Function. Pediatrics 2014, 134, e1063–e1071. [Google Scholar] [CrossRef] [Green Version]
- Jäger, K.; Schmidt, M.; Conzelmann, A.; Roebers, C.M. Cognitive and physiological effects of an acute physical activity intervention in elementary school children. Front. Psychol. 2014, 5. [Google Scholar] [CrossRef]
- Sibley, B.A.; Etnier, J.L. The Relationship between Physical Activity and Cognition in Children: A Meta-Analysis. Pediatr. Exerc. Sci. 2003, 15, 243–256. [Google Scholar] [CrossRef] [Green Version]
- Field, T.; Diego, M.; Sanders, C.E. Exercise is positively related to adolescents’ relationships and academics. Adolescence 2001, 36, 105–110. [Google Scholar]
- Jarrett, O.S.; Maxwell, D.M.; Dickerson, C.; Hoge, P.; Davies, G.; Yetley, A. Impact of Recess on Classroom Behavior: Group Effects and Individual Differences. J. Educ. Res. 1998, 92, 121–126. [Google Scholar] [CrossRef]
- Mahar, M.T.; Murphy, S.K.; Rowe, D.A.; Golden, J.; Shields, A.T.; Raedeke, T.D. Effects of a Classroom-Based Program on Physical Activity and On-Task Behavior. Med. Sci. Sports Exerc. 2006, 38, 2086–2094. [Google Scholar] [CrossRef] [Green Version]
- Blumberg, F.C.; Altschuler, E.A.; Almonte, D.E.; Mileaf, M.I. The Impact of Recreational Video Game Play on Children’s and Adolescents’ Cognition. New Dir. Child. Adolesc. Dev. 2013, 2013, 41–50. [Google Scholar] [CrossRef]
- Wouters, P.; Van Nimwegen, C.; Van Oostendorp, H.; Van Der Spek, E.D. A meta-analysis of the cognitive and motivational effects of serious games. J. Educ. Psychol. 2013, 105, 249–265. [Google Scholar] [CrossRef]
- Girard, C.; Ecalle, J.; Magnan, A. Serious games as new educational tools: How effective are they? A meta-analysis of recent studies. J. Comput. Assist. Learn. 2013, 29, 207–219. [Google Scholar] [CrossRef]
- Granic, I.; Lobel, A.; Engels, R.C.M.E. The benefits of playing video games. Am. Psychol. 2014, 69, 66–78. [Google Scholar] [CrossRef] [PubMed]
- Green, C.; Bavelier, D. Learning, attentional control, and action video games. Curr. Biol. 2012, 22, R197–R206. [Google Scholar] [CrossRef] [PubMed]
- Best, J.R. Exergaming immediately enhances children’s executive function. Dev. Psychol. 2012, 48, 1501–1510. [Google Scholar] [CrossRef]
- Gao, Z. Fight fire with fire: Promoting physical activity and health through active video games. J. Sport Health Sci. 2017, 6, 1–3. [Google Scholar] [CrossRef]
- Baranowski, T. Exergaming: Hope for future physical activity? or blight on mankind? J. Sport Health Sci. 2017, 6, 44–46. [Google Scholar] [CrossRef]
- Gao, Z.; Pope, Z.C.; Lee, J.E.; Quan, M. Effects of Active Video Games on Children’s Psychosocial Beliefs and School Day Energy Expenditure. J. Clin. Med. 2019, 8, 1268. [Google Scholar] [CrossRef]
- Benzing, V.; Schmidt, M. Exergaming for Children and Adolescents: Strengths, Weaknesses, Opportunities and Threats. J. Clin. Med. 2018, 7, 422. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Control (n = 14) | Intervention (n = 18) | p Value * |
|---|---|---|---|
| Age, years | 4.93/0.83 | 4.56/0.62 | 0.15 |
| Gender | 0.15 | ||
| Boys, n = 16 | 5 | 11 | |
| Girls, n = 16 | 9 | 7 | |
| Race/ethnicity | 0.16 | ||
| White American, n =11 | 7 | 4 | |
| Asian American, n =19 | 7 | 12 | |
| African American, n =2 | 0 | 2 | |
| Height, cm (M/SD) | 111.46/8.21 | 108.83/6.91 | 0.33 |
| Weight, kg (M/SD) | 18.86/2.90 | 18.21/2.58 | 0.50 |
| BMI, kg/m2 (M/SD) | 15.14/1.24 | 15.32/1.12 | 0.67 |
| Intervention Group | Control Group | Overall Sample | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | 13th Week | Mean Diff | Baseline | 13th Week | Mean Diff | Baseline | 13th Week | Mean Diff | |
| EE | 357.42 /106.36 | 363.42 /112.33 | 6.07 /108.95 | 338.67 /74.25 | 384.59 /105.5 | 45.92 /64.27 | 349.29 /92.80 | 372.59 /68.08 | 23.30 /93.07 |
| Fitness | 10.22 /6.75 | 7.56 /4.18 | −3.06 /8.33 | 10.64 /5.58 | 10.57 /3.72 | −0.46 /7.22 | 10.41 /6.17 | 8.88 /4.20 | −1.53 /7.75 |
| BMI | 15.32 /1.12 | 15.42 /1.35 | 0.15 /0.65 | 15.14 /1.24 | 15.34 /1.38 | 0.14 /0.64 | 15.24 /1.15 | 15.39 /1.34 | 0.15 /0.65 |
| Cognition | 50.89 /7.70 | 59.39 /7.59 | 8.76 /5.99 | 59 /7.65 | 62.36 /9.19 | 3.54 /5.62 | 54.44 /8.59 | 60.36 /9.19 | 6.25 /6.20 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gao, Z.; Lee, J.E.; Zeng, N.; Pope, Z.C.; Zhang, Y.; Li, X. Home-Based Exergaming on Preschoolers’ Energy Expenditure, Cardiovascular Fitness, Body Mass Index and Cognitive Flexibility: A Randomized Controlled Trial. J. Clin. Med. 2019, 8, 1745. https://doi.org/10.3390/jcm8101745
Gao Z, Lee JE, Zeng N, Pope ZC, Zhang Y, Li X. Home-Based Exergaming on Preschoolers’ Energy Expenditure, Cardiovascular Fitness, Body Mass Index and Cognitive Flexibility: A Randomized Controlled Trial. Journal of Clinical Medicine. 2019; 8(10):1745. https://doi.org/10.3390/jcm8101745
Chicago/Turabian StyleGao, Zan, Jung Eun Lee, Nan Zeng, Zachary C. Pope, Ying Zhang, and Xianxiong Li. 2019. "Home-Based Exergaming on Preschoolers’ Energy Expenditure, Cardiovascular Fitness, Body Mass Index and Cognitive Flexibility: A Randomized Controlled Trial" Journal of Clinical Medicine 8, no. 10: 1745. https://doi.org/10.3390/jcm8101745
APA StyleGao, Z., Lee, J. E., Zeng, N., Pope, Z. C., Zhang, Y., & Li, X. (2019). Home-Based Exergaming on Preschoolers’ Energy Expenditure, Cardiovascular Fitness, Body Mass Index and Cognitive Flexibility: A Randomized Controlled Trial. Journal of Clinical Medicine, 8(10), 1745. https://doi.org/10.3390/jcm8101745