A TUG Value Longer Than 11 s Predicts Fall Risk at 6-Month in Individuals with COPD

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Methods
2.3. Patient Characteristics
- Pulmonary volumes, bronchial airflows, and carbon monoxide lung diffusing capacity (DLCO) were measured in a body plethysmograph (Sentrysuite, Viasys, Conshohocken, PA, USA), according to European Respiratory Society recommendations [15]. All the measurements were compared with the European Community for Coal and Steel (ECCS) predicted values [16]
- Six-minute walking distance (6MWD) was measured according to international recommendations [17]. In patients treated with LTOT, the test was performed with O2 flow prescribed for walking.
- Body composition was determined using biphotonic absorptiometry (Hologic QDR-2000, software version V5.67A, Hologic Inc., Bedford, MA), with a single scan mode [18,19]. We determined fat mass (FM) and fat-free mass (FFM). We calculated the FFM index (FFMI, the ratio of FFM over height2, kg m−2) and skeletal mass index (SMI, the ratio of appendicular FFM over height2, kg m−2).
- Maximal isokinetic concentric strength of quadriceps was measured at 60°/s (Cybex Norm, USA). Evaluation was performed in a sitting position according to the manufacturer’s instructions. Range of motion was set from 90° to 0° of knee flexion. Before each test, a gravity compensation procedure was performed. The test consisted of two repetitions for habituation followed after a resting period by four repetitions at 60°/s in a concentric mode. The best result was retained as the peak torque (PT) value and was normalized to patients’ weight.
- Anxiety and depression were evaluated by the Hospital Anxiety and Depression Scale (HADS).
2.4. Balance Assessment and Fall Records
- Timed Up and Go Test (TUG) [10]. Subjects were instructed to stand up from a standard armchair at the word “go”, walk at a regular pace for 3 m (indicated by a line on the floor), turn around, walk back, and sit down. This assesses lower limb muscle force, gait speed, and coordination—three components of postural control. TUG shows excellent intra- and inter-observer reliability, with an intraclass correlation coefficient of 0.99 [20]. A practice test was followed by the actual test, with an opportunity to recover between the trials. Gait aids were permitted when appropriate and, for patients treated with LTOT, the test was performed with O2 flow prescribed for walking that was carried in a shoulder bag or backpack. A time longer than 12 s is considered as an indicator of fall risk in the elderly and in COPD patients [14,21].
- The Berg Balance Scale [22] was performed by the same investigator (VR). It comprised 14 questions and tasks completed by patients and scored by the observer, from worst (0) to best (4). The maximum total score is 56 points, and the risk of fall is considered low above 45.
- The number of falls in the previous year was collected with the Elderly Fall Screening Test questionnaire [23]. A fall was defined as a positive response to the question “Have you ever found yourself on the ground without wanting to get there, while sitting, standing or lying down?” We considered patients as fallers with the occurrence of at least one fall.
- Fall recurrence at 6 months after evaluation was prospectively obtained via a phone survey using a standardized questionnaire with the same definition as previously used. During this phone survey, we also assessed whether a rehabilitation program was undertaken during the observational period.
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
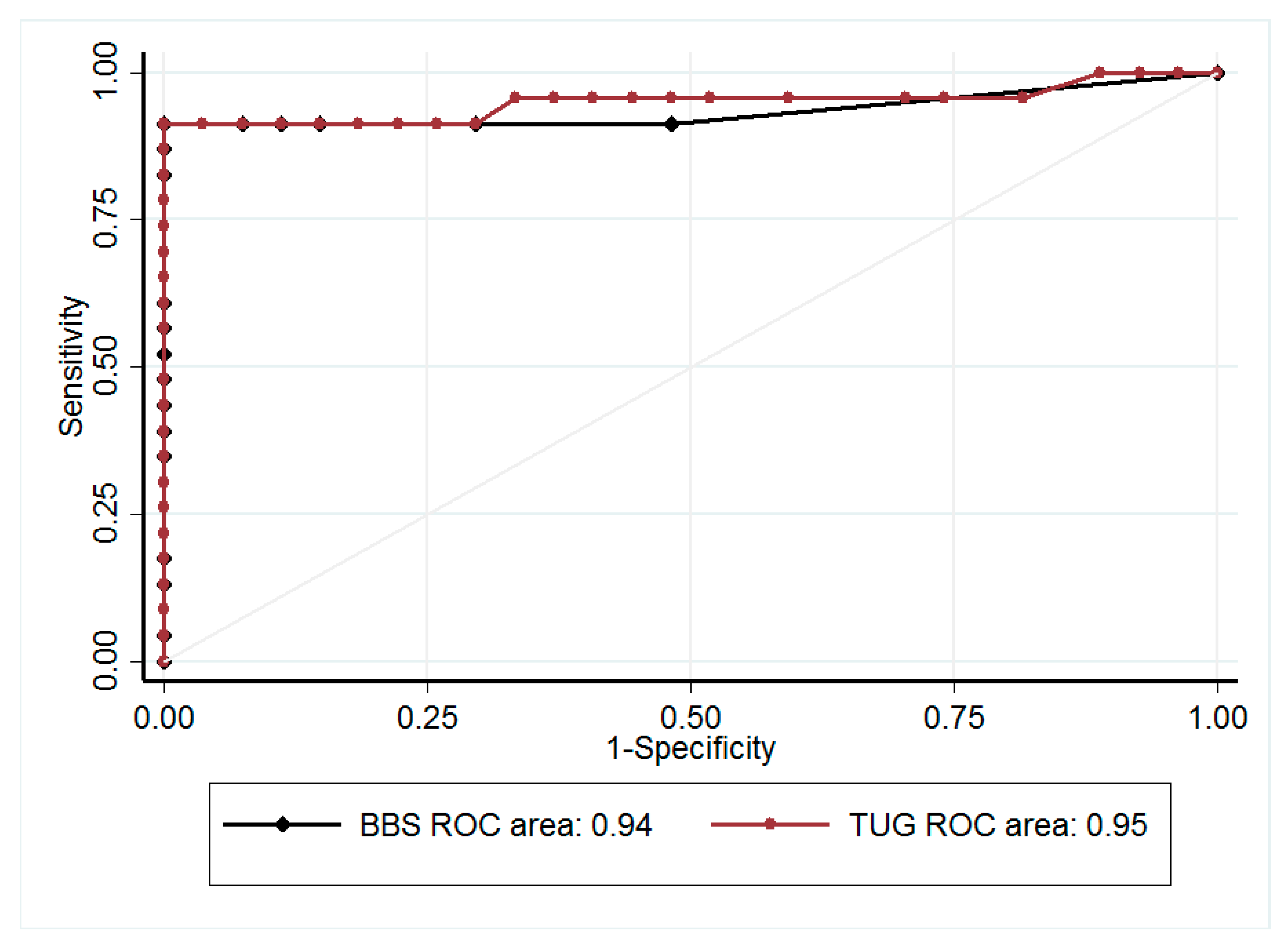
3.2. BBS, TUG, and Fall
3.3. Predictive Factors Associated with Fall
4. Discussion
4.1. TUG as a Screening Test for Fall Risk
4.2. Fall Incidence in COPD Patients
4.3. Predictive Factors Associated with Falling
4.4. Limitations of the Study
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Vanfleteren, L.E.; Spruit, M.A.; Groenen, M.; Gaffron, S.; van Empel, V.P.; Bruijnzeel, P.L.; Rutten, E.P.; Op’t Roodt, J.; Wouters, E.F.; Franssen, F.M. Clusters of comorbidities based on validated objective measurements and systemic inflammation in patients with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2013, 187, 728–735. [Google Scholar] [CrossRef]
- Roig, M.; Eng, J.J.; MacIntyre, D.L.; Road, J.D.; FitzGerald, J.M.; Burns, J.; Reid, W.D. Falls in people with chronic obstructive pulmonary disease: An observational cohort study. Respir. Med. 2011, 105, 461–469. [Google Scholar] [CrossRef] [Green Version]
- Hakamy, A.; Bolton, C.E.; Gibson, J.E.; McKeever, T.M. Risk of fall in patients with COPD. Thorax 2018, 73, 1079–1080. [Google Scholar] [CrossRef]
- Beauchamp, M.K.; Hill, K.; Goldstein, R.S.; Janaudis-Ferreira, T.; Brooks, D. Impairments in balance discriminate fallers from non-fallers in COPD. Respir. Med. 2009, 103, 1885–1891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yohannes, A.M.; Raue, P.J.; Kanellopoulos, D.; McGovern, A.; Sirey, J.A.; Kiosses, D.N.; Banerjee, S.; Seirup, J.K.; Novitch, R.S.; Alexopoulos, G.S. Predictors of All-Cause Mortality in Patients with Severe COPD and Major Depression Admitted to a Rehabilitation Hospital. Chest 2016, 149, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Beauchamp, M.K.; Sibley, K.M.; Lakhani, B.; Romano, J.; Mathur, S.; Goldstein, R.S.; Brooks, D. Impairments in systems underlying control of balance in COPD. Chest 2012, 141, 1496–1503. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, C.C.; Lee, A.; Granger, C.L.; Miller, K.J.; Irving, L.B.; Denehy, L. Postural control and fear of falling assessment in people with chronic obstructive pulmonary disease: A systematic review of instruments, international classification of functioning, disability and health linkage, and measurement properties. Arch. Phys. Med. Rehabil. 2013, 94, 1784–1799. [Google Scholar] [CrossRef]
- Crişan, A.F.; Oancea, C.; Timar, B.; Fira-Mladinescu, O.; Tudorache, V. Balance impairment in patients with COPD. PLoS ONE 2015, 10, e0120573. [Google Scholar] [CrossRef]
- Beauchamp, M.K.; O’Hoski, S.; Goldstein, R.S.; Brooks, D. Effect of pulmonary rehabilitation on balance in persons with chronic obstructive pulmonary disease. Arch. Phys. Med. Rehabil. 2010, 91, 1460–1465. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar]
- Mesquita, R.; Wilke, S.; Smid, D.E.; Janssen, D.J.; Franssen, F.M.; Probst, V.S.; Wouters, E.F.; Muris, J.W.; Pitta, F.; Spruit, M.A. Measurement properties of the Timed Up & Go test in patients with COPD. Chron. Respir. Dis. 2016, 13, 344–352. [Google Scholar] [PubMed] [Green Version]
- Gunter, K.B.; White, K.N.; Hayes, W.C.; Snow, C.M. Functional mobility discriminates nonfallers from one-time and frequent fallers. J. Gerontol. A Biol. Sci. Med. Sci. 2000, 55, 672–676. [Google Scholar] [CrossRef] [PubMed]
- Herman, T.; Giladi, N.; Hausdorff, J.M. Properties of the “timed up and go” test: More than meets the eye. Gerontology 2011, 57, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Al Haddad, M.A.; John, M.; Hussain, S.; Bolton, C.E. Role of the Timed Up and Go Test in Patients with Chronic Obstructive Pulmonary Disease. J. Cardiopulm. Rehabil. Prev. 2016, 36, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; van der Grinten, C.P.M.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quanjer, P.H. Standardized lung function testing, ECSC 1993 update. Bull. Eur. Physiopathol. Respir. 1993, 19, 5–40. [Google Scholar] [CrossRef] [PubMed]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [CrossRef]
- Forbes, G.B. Body composition: Overview. J. Nutr. 1999, 129, 270–272. [Google Scholar] [CrossRef]
- Paradisi, G.; Smith, L.; Burtner, C.; Leaming, R.; Garvey, W.T.; Hook, G.; Johnson, A.; Cronin, J.; Steinberg, H.O.; Baron, A.D. Dual energy X-ray absorptiometry assessment of fat mass distribution and its association with the insulin resistance syndrome. Diabetes Care 1999, 22, 1310–1317. [Google Scholar] [CrossRef]
- Marques, A.; Cruz, J.; Quina, S.; Regêncio, M.; Jácome, C. Reliability, Agreement and Minimal Detectable Change of the Timed Up & Go and the 10-Meter Walk Tests in Older Patients with COPD. COPD 2016, 13, 279–287. [Google Scholar]
- Bischoff, H.A.; Stähelin, H.B.; Monsch, A.U.; Iversen, M.D.; Weyh, A.; von Dechend, M.; Akos, R.; Conzelmann, M.; Dick, W.; Theiler, R. Identifying a cut-off point for normal mobility: A comparison of the timed “up and go” test in community-dwelling and institutionalised elderly women. Age Ageing 2003, 32, 315–320. [Google Scholar] [CrossRef] [PubMed]
- Berg, K.O.; Maki, B.E.; Williams, J.I.; Holliday, P.J.; Wood-Dauphinee, S.L. Clinical and laboratory measures of postural balance in an elderly population. Arch. Phys. Med. Rehabil. 1992, 73, 1073–1080. [Google Scholar] [PubMed]
- Cwikel, J.G.; Fried, A.V.; Biderman, A.; Galinsky, D. Validation of a fall-risk screening test, the Elderly Fall Screening Test (EFST), for community-dwelling elderly. Disabil. Rehabil. 1998, 20, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Beauchamp, M.K.; Janaudis-Ferreira, T.; Parreira, V.; Romano, J.M.; Woon, L.; Goldstein, R.S.; Brooks, D. A randomized controlled trial of balance training during pulmonary rehabilitation for individuals with COPD. Chest 2013, 144, 1803–1810. [Google Scholar] [CrossRef]
- Mkacher, W.; Tabka, Z.; Trabelsi, Y. Minimal Detectable Change for Balance Measurements in Patients with COPD. J. Cardiopulm. Rehabil. Prev. 2017, 37, 223–228. [Google Scholar] [CrossRef]
- Butcher, S.J.; Pikaluk, B.J.; Chura, R.L.; Walkner, M.J.; Farthing, J.P.; Marciniuk, D.D. Associations between isokinetic muscle strength, high-level functional performance, and physiological parameters in patients with chronic obstructive pulmonary disease. Int. J. Chron. Obstruct. Pulm. Dis. 2012, 7, 537–542. [Google Scholar] [CrossRef]
- Mesquita, R.; Janssen, D.J.A.; Wouters, E.F.M.; Schols, J.M.G.A.; Pitta, F.; Spruit, M.A. Within-day test-retest reliability of the Timed Up & Go test in patients with advanced chronic organ failure. Arch. Phys. Med. Rehabil. 2013, 94, 2131–2138. [Google Scholar]



{kind=link}
{kind=link}
| All | LTOT− | LTOT+ | Effect of LTOT p Value | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Fallers | Non-Fallers | p | Fallers | Non-Fallers | p | In Fallers | In Non-Fallers | ||
| N | 50 | 6 | 19 | 17 | 8 | ||||
| Age (years) | 66.2 ± 8.2 | 65.0 ± 4.1 | 64.2 ± 7.3 | 68.6 ± 9.8 | 66.4 ± 8.8 | ||||
| BMI (kg m−2) | 28.0 ± 6.5 | 24.2 ± 3.8 | 26.0 ± 5.5 | 32.0 ± 7.4 | 27.0 ± 3.7 | 0.004 | |||
| FEV1 % pred | 51.8 ± 15.9 | 63.3 ± 20.4 | 51.4 ± 15.4 | 50.0 ± 15.4 | 47.6 ± 13.2 | ||||
| FVC % pred | 87.1 ± 20.7 | 88.3 ± 21.1 | 83.1 ± 19.8 | 82.6 ± 15.4 | 105.4 ± 25.2 | 0.04 | 0.04 | ||
| TLC % pred | 123.0 ± 21.7 | 113.7 ± 31.7 | 122.2 ± 18.8 | 118.4 ± 18.0 | 141.8 ± 19.8 | 0.01 | 0.03 | ||
| RV/TLC % | 55.3 ± 11.6 | 54.1 ± 8.7 | 54.1 ± 13.1 | 57.2 ± 12.0 | 55.2 ± 9.6 | ||||
| DLCO % pred | 45.5 ± 18.3 | 38.6 ± 7.5 | 57.5 ± 19.7 | 0.01 | 37.6 ± 13.0 | 33.7 ± 15.9 | |||
| 6MWD % pred | 79.0 ± 24.2 | 71.1 ± 15.8 | 93.8 ± 12.1 | 0.02 | 59.6 ± 26.4 | 91.0 ± 14.8 | 0.001 | 0.03 | |
| qPT (Nm/kg) | 116.5 ± 37.9 | 98.1 ± 23.5 | 134.4 ± 42.3 | 0.02 | 95.0 ± 26.3 | 133.4± 29.6 | 0.008 | ||
| Use of assistive device (cane) | 2 (4%) | 0 | 0 | 2 (11.7%) | 0 | ||||
| All | LTOT− | LTOT+ | Effect of LTOT p Value | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Fallers | Non-Fallers | p | Fallers | Non-Fallers | p | In Fallers | In Non-Fallers | ||
| FM (%) | 27.8 ± 7.9 | 28.9 ± 6.2 | 23.7 ± 8.0 | 32.5 ± 6.8 | 26.9 ± 6.5 | ||||
| FFM (kg) | 53.1 ± 11.7 | 44.8 ± 9.8 | 52.8 ± 12.7 | 56.6 ± 9.9 | 52.5 ± 12.6 | 0.03 | |||
| FFM (%) | 68.8 ± 8.4 | 68.4 ± 5.8 | 71.6 ± 10.3 | 65.0 ± 6.5 | 70.2 ± 6.2 | ||||
| FFMI (kg·m−2) | 20.0 ± 3.4 | 17.3 ± 3.2 | 19.8 ± 3.1 | 0.04 | 21.3 ± 19.7 | 19.7 ± 3.6 | 0.007 | ||
| SMI (kg·m−2) | 7.7 ± 1.5 | 6.7 ± 0.9 | 7.7 ± 1.3 | 8.1 ± 1.5 | 7.8 ± 1.7 | 0.04 | 0.02 | ||
| All | LTOT− | LTOT+ | |
|---|---|---|---|
| With a cut-off value of 12 s for TUG | |||
| κ coefficient | 0.92 | 0.87 | 0.92 |
| Sensitivity (%) | 95.0 (75.1–99.9) | 80.0 (28.4–99.5) | 100 (78.2–100) |
| Specificity (%) | 96.7 (82.8–99.9) | 100 (83.0–100) | 90.0 (55.5–99.7) |
| PPV (%) | 95.0 (75.1–99.9) | 100 (39.8–100) | 93.8 (69.8–99.8) |
| NPV (%) | 96.7 (82.8–99.9) | 95.2 (76.2–99.9) | 100 (66.4–100) |
| With a cut–off value of 11 s for TUG | |||
| κ coefficient | 0.96 | 1.00 | 0.92 |
| Sensitivity (%) | 100 (83.2; 100) | 100 (47.8; 100) | 90.0 (55.5–99.7) |
| Specificity (%) | 96.7 (82.8; 99.9) | 100 (83.2; 100) | 93.8 (69.8–99.8) |
| PPV (%) | 95.2 (76.2; 99.9) | 100 (47.8; 100) | 100 (66.4–100) |
| NPV (%) | 100 (88.1; 100) | 100 (83.2; 100) | 90.0 (55.5–99.7) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reynaud, V.; Muti, D.; Pereira, B.; Greil, A.; Caillaud, D.; Richard, R.; Coudeyre, E.; Costes, F. A TUG Value Longer Than 11 s Predicts Fall Risk at 6-Month in Individuals with COPD. J. Clin. Med. 2019, 8, 1752. https://doi.org/10.3390/jcm8101752
Reynaud V, Muti D, Pereira B, Greil A, Caillaud D, Richard R, Coudeyre E, Costes F. A TUG Value Longer Than 11 s Predicts Fall Risk at 6-Month in Individuals with COPD. Journal of Clinical Medicine. 2019; 8(10):1752. https://doi.org/10.3390/jcm8101752
Chicago/Turabian StyleReynaud, Vivien, Daniela Muti, Bruno Pereira, Annick Greil, Denis Caillaud, Ruddy Richard, Emmanuel Coudeyre, and Frédéric Costes. 2019. "A TUG Value Longer Than 11 s Predicts Fall Risk at 6-Month in Individuals with COPD" Journal of Clinical Medicine 8, no. 10: 1752. https://doi.org/10.3390/jcm8101752
APA StyleReynaud, V., Muti, D., Pereira, B., Greil, A., Caillaud, D., Richard, R., Coudeyre, E., & Costes, F. (2019). A TUG Value Longer Than 11 s Predicts Fall Risk at 6-Month in Individuals with COPD. Journal of Clinical Medicine, 8(10), 1752. https://doi.org/10.3390/jcm8101752