1. Introduction
Lung cancer is the most common cause of cancer-related mortality worldwide [
1]. About 80% of all cases are non-small cell lung cancer (NSCLC), among which the most common cell type is adenocarcinoma. More than half of these NSCLC were diagnosed in advanced stage [
2]. In the past, the only treatment for advanced NSCLC was platinum-based doublet chemotherapy, resulting in a median overall survival (OS) period of around 8 months [
3]. Clinical practice has changed since the development of epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors (TKIs), with the discovery of
EGFR driver gene mutations in NSCLC. Patients with NSCLC harboring such mutations, such as exon 21 L858R point mutation and exon 19 deletion, have better progression-free survival (PFS) when treated with
EGFR TKIs [
4,
5,
6]. It is therefore very important to determine the presence of
EGFR mutation in NSCLC.
Initially, tissue samples, biopsied from either primary tumor or metastatic lesions, had been used for the
EGFR mutation testing. The procedures of tissue biopsy, including bronchoscopic biopsy, computed tomography-guided biopsy, and surgical biopsy, are all invasive, and bring risks of some complications, such as hemoptysis, pneumothorax, and pneumonitis [
7,
8,
9]. Another limitation of tissue biopsy is the tumor heterogeneity, especially in patients with advanced stages. The results of
EGFR gene testing might be different in various parts of the cancer, especially in the metastatic sites, so tissue biopsy from one part of a solitary tumor might miss the intra-tumoral and inter-metastatic molecular heterogeneity [
10,
11]. Furthermore, malignant cells could be found in 72.9% of specimens under pathological examination [
12]. Repeated biopsies may sometimes be required to obtain sufficient cancer tissue for gene testing [
13].
Liquid biopsy, identifying the genotype of tumor cells from circulating tumor DNA (ctDNA) of the patients’ blood, is a less invasive method. Since the report by Mandel and Metais in 1948, fragmented DNA in the cell-free component of serum has been a field of active research [
11]. Investigation of cell-free DNA has been conducted in many disciplines, such as exercise, end-stage renal failure, stroke, myocardial infarction, surgery, and trauma [
14,
15,
16,
17]. In the oncological field, studies of cell-free DNA derived from tumors, also known as ctDNA, has dramatically increased recently, mainly because of the development of the genomic technologies that allow detection of rare gene mutant variants of DNA [
11]. In recent studies of NSCLC, liquid biopsy was shown to detect driver gene mutations, such as
EGFR and anaplastic lymphoma kinase (ALK) mutation, and tumor mutational burden [
18,
19]. Compared to tissue biopsy, liquid biopsy done at disease progression can reduce the necessity of invasive biopsy procedures, the risk of biopsy related complications, and the cost of the complication-related hospitalization [
20].
Most patients have concordant results in liquid/tissue biopsy, while a few patients have discordant results in the gene testing of tissue biopsy and liquid biopsy. The factors related to concordant results and the clinical significance of concordant results remain unclear. Our study aimed to evaluate the predicting factors and clinical outcomes associated with concordant results in liquid/tissue biopsy in newly diagnosed lung adenocarcinoma patients with EGFR mutations.
2. Materials and Methods
2.1. Study Population
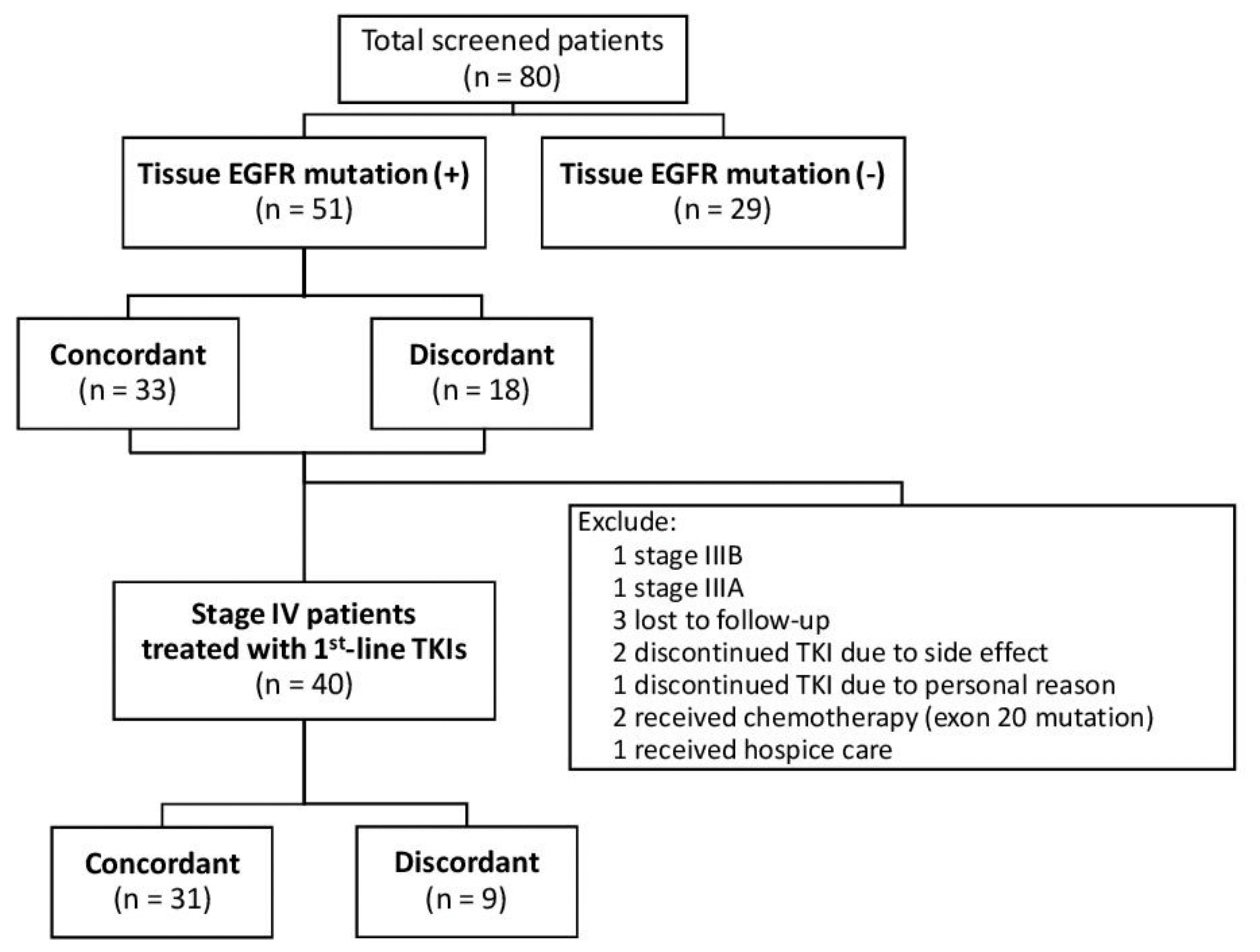
This retrospective study was conducted in Kaohsiung Medical University Hospital between June 2016 and August 2018. Treatment naïve stage III or IV lung adenocarcinoma patients with EGFR mutation tested from both their biopsied tumor tissue and liquid biopsy at their diagnosis were enrolled. All patients received imaging studies, including computed tomography of the chest, brain magnetic resonance imaging (MRI), and whole-body bone scan, to determine the extent of cancer invasion, lymph node involvement, and distant metastasis. The clinical stage was determined according to the American Joint Committee on Cancer (AJCC) Cancer Staging Manual, 7th Edition.
The Institutional Review Board (IRB) of Kaohsiung Medical University Hospital (KMUH) approved this study (KMUHIRB-G(II)-20190024) and waived the need for written informed consent from all patients.
2.2. DNA Extraction, Amplification, and Detection
The genomic DNA was extracted from formalin-fixed and paraffin-embedded (FFPE) tumor tissue samples, and
EGFR mutation was tested by using Qiagen
® EGFR RGQ PCR kit (QIAGEN, Hilden, Germany) as in our previous studies [
21,
22,
23,
24,
25,
26] or Cobas
® EGFR Mutation Test v2 (Roche Diagnostics, Rotkreuz, Switzerland) (for the latest 6 samples). The previous validation exam in the Department of Laboratory Medicine, KMUH showed excellent correlation between the results obtained from these two kits. For liquid biopsy, the plasma ctDNA was extracted and then analyzed by Cobas
® EGFR Mutation Test v2, which was a real-time PCR test for the quantitative detection and identification of mutations in exons 18, 19, 20, and 21 of the
EGFR gene.
2.3. Definitions of Variables
The EGFR mutations detected in tissue samples were taken as the reference, to which the mutations detected in plasma ctDNA were compared. The patients with the same EGFR mutation patterns detected in both biopsied tissue samples and plasma ctDNA were classified as “concordant” group, whereas those having different mutation patterns in their plasma ctDNA versus their tissue samples were classified as “discordant” group.
Patients with stage IV disease who received first-line EGFR TKIs were further extracted for outcome analyses, while those who had discontinued the EGFR TKI for personal reasons or side effects were excluded. The objective treatment response was assessed according to the Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1. A computed tomography of the chest was obtained three months after the initiation of a EGFR TKI to determine the 3-month treatment response. To determine the progression-free survival, these patients were followed till either disease progression or 16 January 2019.
2.4. Statistical Analysis
The baseline characteristics, including sex, age, performance status, tumor stage, primary tumor size, lymph node involvement, distant metastases, and EGFR mutation in tissue sample, were compared between the concordant and discordant groups. Categorical and continuous variables were analyzed using Chi-square test and Student’s t-test, respectively. The effects of factors in predicting concordant EGFR mutation test results in liquid/tissue biopsy were assessed using logistic regression analysis. The odds ratio (OR) with 95% confidence interval (CI) was reported. Following univariate analyses, all factors were included to build a maximal model of multivariable analysis. The reduced multivariable model was then developed with backward variable selection method, keeping only variables with p value less than 0.1, from the maximal model.
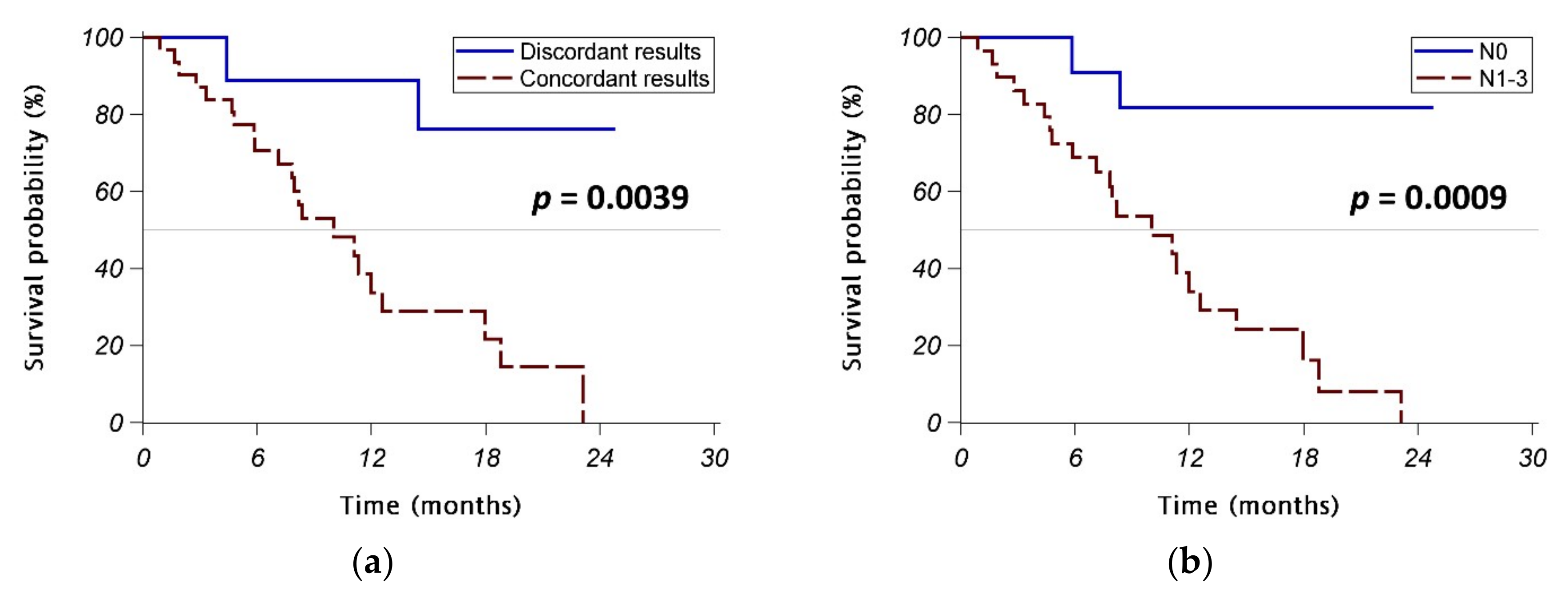
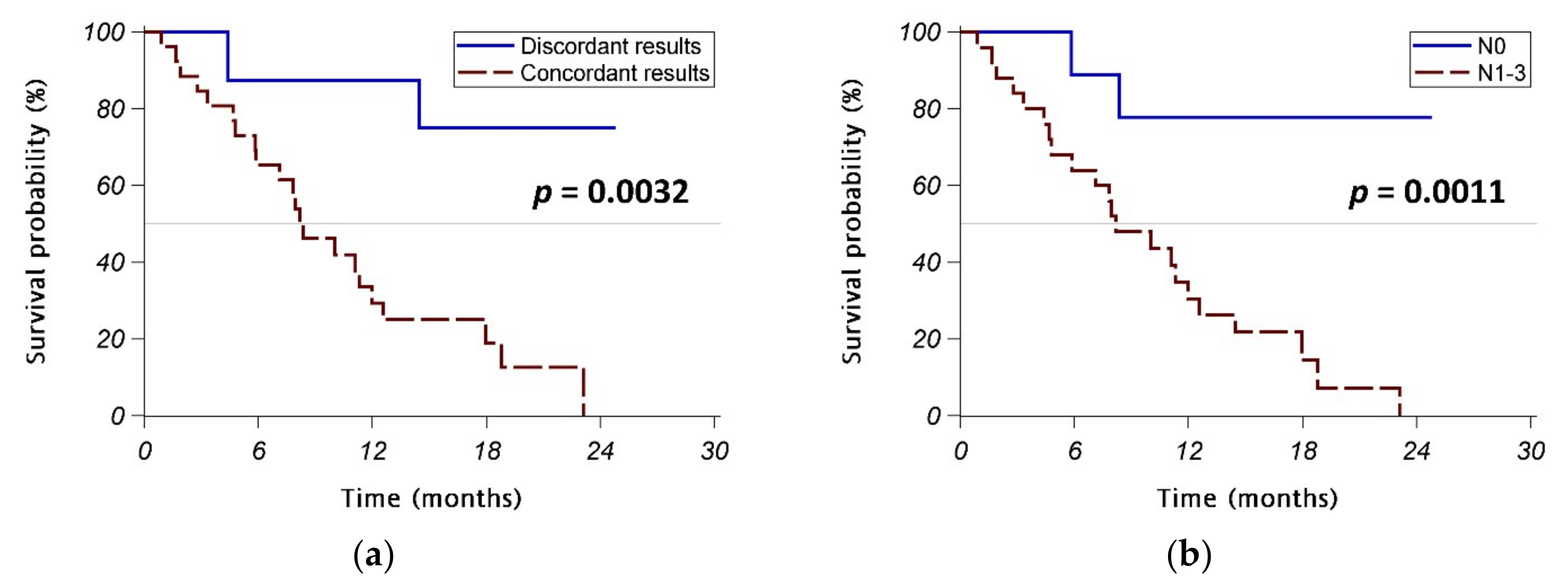
In the outcome analyses, which included only stage IV patients receiving first-line EGFR TKIs, the initial objective response rate (ORR) and disease control rate (DCR) were calculated. The PFS of patients in concordant and discordant groups were assessed with the Kaplan–Meier method and compared with log-rank test. The effects of factors in predicting PFS were assessed using Cox regression analysis. The hazard ratio (HR) with 95% CI was reported. Following univariate analyses, all factors were included to build maximal models of multivariable analyses. The reduced multivariable models were then developed with backward variable selection method, keeping only variables with p value less than 0.1, from the maximal models.
The statistical analyses were performed using SAS system (version 9.4 for Windows, SAS Institute Inc., Cary, NC, USA). A two-sided p value of <0.05 was taken as the statistical significance level.
4. Discussion
Determining EGFR mutation status is important in guiding the treatment for advanced lung adenocarcinoma. Liquid biopsy, which uses plasma ctDNA as surrogates for tissue samples, has been increasingly used in clinical practice. However, it remains unclear whether plasma ctDNA provides the same information about EGFR mutation status as do tissue samples. In the current study, we found that 65% of patients with newly diagnosed advanced lung adenocarcinoma harboring EGFR mutation in their tissue samples had concordant EGFR mutation testing results in the testing using liquid biopsy. The factors independently associated with the concordant results in liquid/tissue biopsy included lymph node involvement and bone metastasis. We further showed that the concordant results in liquid/tissue biopsy was associated with significantly poorer PFS in stage IV patients treated with EGFR TKIs. However, multivariable analysis showed that only lymph node involvement was the independent predicting factor for poorer PFS, while the concordant results in liquid/tissue biopsy was not an independently predicting factor.
There are several advantages of using liquid biopsy to determine the tumor genotypes. It is less invasive than traditional tissue biopsy, so the risk of biopsy-related complications can be eliminated. Liquid biopsy may provide similar results of
EGFR testing as tissue biopsy. In a recent study analyzing the association between plasma genotyping and treatment outcomes of osimertinib in advanced NSCLC patients who failed to the first-line
EGFR TKIs therapy, patients with T790M mutation detected by either liquid biopsy or tissue biopsy had similar outcomes [
27]. In addition, liquid biopsy provides the results of tumor genotypes more rapidly than traditional tissue biopsy. A recent study revealed that the median turnaround time for
EGFR gene analysis in newly diagnosed lung cancer patients was three business days while using liquid biopsy and was twelve business days while using tissue biopsy [
13]. Finally, investigating plasma ctDNA from cancer patients can account for molecular heterogeneity, because ctDNA fragments from all parts of cancer tissues throughout the patient’s body are collected [
28,
29,
30,
31]. In our study, two patients had different
EGFR genotypes shown in tumor tissue and ctDNA, which might be related to molecular heterogeneity.
The association between clinical features and detectable ctDNA has been investigated in some previous studies. Although a few studies found no correlation between ctDNA levels and tumor burden [
32,
33], further studies still suggested that the presence of ctDNA was significantly associated with a larger tumor burden [
34,
35,
36,
37]. A recent study of late-staged NSCLC patients even showed that patients with bone metastasis had significantly higher ctDNA quantities than those without bone metastases [
38]. A recent Korean study of 57 patients with adenocarcinoma harboring activating
EGFR mutations found that bone metastasis was the only independent factor predicting ctDNA detection [
39]. Similar to their findings, our current study found that the concordant
EGFR testing results in liquid/tissue biopsy was associated with lymph node involvement, brain metastasis, and bone metastasis. Multivariable analysis showed that lymph node involvement and bone metastasis were independent predicting factors for the concordant results in liquid/tissue biopsy, while a trend of association between larger original tumor burden (T3–4) and the concordant results was also noted. Based on our findings, liquid biopsy, rather than repeated tissue biopsies, might be considered first for patients with lung adenocarcinoma with lymph node involvement and/or bone metastasis, especially for patients with high risk of biopsy-related complications. Our findings also suggested that the concordant results in liquid/tissue biopsy might be related to a more extensive tumor burden.
The detectable ctDNA might suggest poorer clinical outcomes because circulating mutant DNA has been found quite useful in assessing tumor dynamics [
40]. In the BENEFIT study, a multicenter, single-arm, phase 2 clinical trial in 15 centers in China, patients with clearance of
EGFR mutations in ctDNA at week 8 had longer PFS than those whose
EGFR mutations persisted at week 8 [
41]. The recent Korean study found that ctDNA detection was associated with poorer PFS in patients treated with
EGFR TKIs, and also identified ctDNA detection and extrathoracic lymph node metastasis as independent factors predicting poorer PFS [
39]. Similar to their findings, our current study showed that concordant
EGFR testing results in liquid/tissue biopsy was significantly associated with a poor PFS. In contrast to their findings, the predicting effect of concordant EGFR testing results in liquid/tissue biopsy became insignificant after adjusting with other variables, especially lymph node involvement. Our finding suggested that lymph node involvement might be a confounding factor intervening between concordant results in liquid/tissue biopsy and poorer PFS. Our study was different from the Korean study in several aspects: Firstly, we included only stage IV patients actually receiving EGFR TKIs in the outcome analysis, whereas the Korean study included some patients with earlier stage (M0), which might bias the analysis. Secondly, the TKI used was included in the analysis of our study, whereas the Korean study did not include TKI used in their analysis because almost all of their patients used gefitinib (55 patients used gefitinib, one patient used erlotinib, and one patient used afatinib). Thirdly, we included lymph node involvement in the analysis and found it was independently associated with poorer PFS.
Our study still has some limitations. Firstly, the number of enrolled patients was relatively small. Nevertheless, our study was one of the largest studies discussing this topic. Currently, liquid biopsy to detect
EGFR mutation is usually performed on the failure of first-line
EGFR TKI in clinical practice, so not many patients received liquid biopsy before starting their first-line treatment. Secondly, the follow-up time was relatively short, so overall survival could not be assessed. Further follow-up study is needed to investigate the association between concordant
EGFR testing results in liquid/tissue biopsy and overall survival. Finally, our study adopted different approaches to tissue analysis (Qiagen
® EGFR RGQ PCR kit or Cobas
® EGFR Mutation Test v2) and plasma ctDNA analysis (Cobas
® EGFR Mutation Test v2). The two approaches might have different detection limits. Due to low concentrations of ctDNA in plasma, the detection rate of gene mutation by liquid biopsy might be relatively lower. This might affect the results of our study. However, the tests have been adopted in many previous studies [
21,
22,
23,
24,
25,
26,
27,
42], and previous validation examination in our hospital showed excellent correlation between the results obtained from these two kits. We also performed sensitivity analysis, i.e., another set of analysis excluding those using Cobas
® EGFR Mutation Test v2 for their tissue samples and found consistent results. Furthermore, the aim of this study is to identify the predicting factors for concordant results from both tests. All patients in the sensitivity analyses had their tumor tissue examined with the Qiagen
® kit and their plasma examined with the Cobas
® kit. We therefore believe that using different analyzing methods for different sample types might minimally affect the results of this study.


 ,
, 
{kind=link}
{kind=link}
{kind=link}


