Stress Exposure and the Course of ADHD from Childhood to Young Adulthood: Comorbid Severe Emotion Dysregulation or Mood and Anxiety Problems

Abstract
:1. Introduction
2. Methods
2.1. Sample
2.2. Measurements
2.2.1. ADHD
2.2.2. Internalizing problems
2.2.3. Emotion Dysregulation
2.2.4. Effortful Control
2.2.5. Stress Exposure
2.2.6. IQ
2.2.7. Analysis
3. Results
3.1. Model Selection
3.2. Demographics
3.3. Overall Developmental Trends
3.4. Course Differences in Stress Exposure and Symptoms
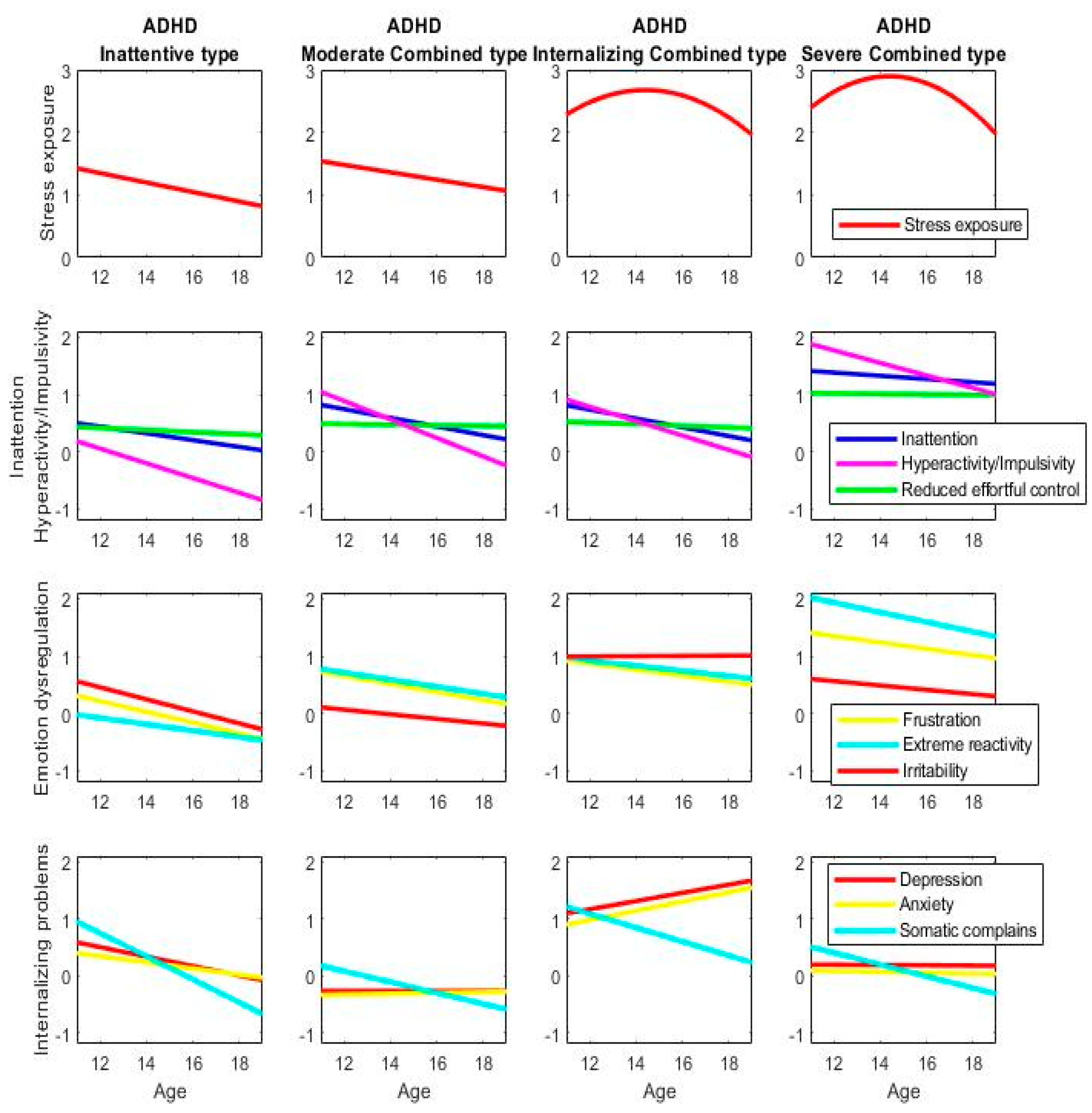
3.4.1. Developmental Trajectories
3.4.2. Stress Exposure and the Course of ADHD
4. Discussion
5. Conclusions
- -
- Cross-sectional studies have indicated that individuals with ADHD are on average exposed to more stressful conditions than typically developing individuals.
- -
- Current findings show that stress exposure is strongly intertwined with a persistent course of ADHD between childhood and young adulthood.
- -
- High exposure to stress that peaks in mid-adolescence go jointly with two different persistent courses: combined type ADHD with strong irritability, extreme reactivity, and high frustration and combined type ADHD with elevated and increasing irritability, anxiety, and depression.
- -
- Consideration of stressful conditions should be part of the diagnosis and treatment of ADHD for prognosis as well as potential prevention or interruption of adverse trajectories.
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Hartman, C.A.; Geurts, H.M.; Franke, B.; Buitelaar, J.K.; Rommelse, N.N. Changing ASD-ADHD symptom co-occurrence across the lifespan with adolescence as crucial time window: Illustrating the need to go beyond childhood. Neurosci. Biobehav. Rev. 2016, 71, 529–541. [Google Scholar] [CrossRef]
- Franke, B.; Michelini, G.; Asherson, P.; Banaschewski, T.; Bilbow, A.; Buitelaar, J.K.; Cormand, B.; Faraone, S.V.; Ginsberg, Y.; Haavik, J.; et al. Live fast, die young? A review on the developmental trajectories of ADHD across the lifespan. Eur. Neuropsychopharmacol. 2018, 28, 1059–1088. [Google Scholar] [CrossRef]
- Grant, K.E.; Compas, B.E.; Thurm, A.E.; McMahon, S.D.; Gipson, P.Y. Stressors and child and adolescent psychopathology: Measurement issues and prospective effects. J. Clin. Child Adolesc. Psychol. 2004, 33, 412–425. [Google Scholar] [CrossRef]
- Biederman, J.; Milberger, S.; Faraone, S.V.; Kiely, K.; Guite, J.; Mick, E.; Warburton, R.; Reed, E.; Davis, S.G. Impact of adversity on functioning and comorbidity in children with attention-deficit hyperactivity disorder. J. Am. Acad. Child Adolesc. Psychiatry 1995, 34, 1495–1503. [Google Scholar] [CrossRef] [PubMed]
- Björkenstam, E.; Björkenstam, C.; Jablonska, B.; Kosidou, K. Cumulative exposure to childhood adversity, and treated attention deficit/hyperactivity disorder: A cohort study of 543 650 adolescents and young adults in Sweden. Psychol. Med. 2018, 48, 498–507. [Google Scholar] [CrossRef] [PubMed]
- Blazer, D.; Hughes, D.; George, L.K. Stressful life events and the onset of a generalized anxiety syndrome. Am. J. Psychiatry 1987, 144, 1178–1183. [Google Scholar] [PubMed]
- Campo, J.V. Annual Research Review: Functional somatic symptoms and associated anxiety and depression–developmental psychopathology in pediatric practice. J. Child Psychol. Psychiatry 2012, 53, 575–592. [Google Scholar] [CrossRef]
- Kendler, K.S.; Karkowski, L.M.; Prescott, C.A. Stressful life events and major depression: Risk period, long-term contextual threat, and diagnostic specificity. J. Nerv. Ment. Dis. 1998, 186, 661–669. [Google Scholar] [CrossRef]
- Larsson, H.; Dilshad, R.; Lichtenstein, P.; Barker, E.D. Developmental trajectories of DSM-IV symptoms of attention-deficit/hyperactivity disorder: Genetic effects, family risk and associated psychopathology. J. Child Psychol. Psychiatry 2011, 52, 954–963. [Google Scholar] [CrossRef]
- Barkley, R.A. Emotional dysregulation is a core component of ADHD. In Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis and Treatment; The Guilford Press: New York, NY, USA, 2015; pp. 81–115. [Google Scholar]
- Bunford, N.; Evans, S.W.; Wymbs, F. ADHD and emotion dysregulation among children and adolescents. Clin. Child Fam. Psychol. Rev. 2015, 18, 185–217. [Google Scholar] [CrossRef]
- Wheeler Maedgen, J.; Carlson, C.L. Social functioning and emotional regulation in the attention deficit hyperactivity disorder subtypes. J. Clin. Child Psychol. 2000, 29, 30–42. [Google Scholar] [CrossRef] [PubMed]
- Melnick, S.M.; Hinshaw, S.P. Emotion regulation and parenting in AD/HD and comparison boys: Linkages with social behaviors and peer preference. J. Abnorm. Child Psychol. 2000, 28, 73–86. [Google Scholar] [CrossRef] [PubMed]
- Oldehinkel, A.J.; Rosmalen, J.G.; Buitelaar, J.K.; Hoek, H.W.; Ormel, J.; Raven, D.; Reijneveld, S.A.; Veenstra, R.; Verhulst, F.C.; Vollebergh, W.A.; et al. Cohort Profile Update: The TRacking Adolescents’ Individual Lives Survey (TRAILS). Int. J. Epidemiol. 2015, 44, 76–76n. [Google Scholar] [CrossRef] [PubMed]
- Muthén, B. Latent variable analysis: Growth mixture modeling and related techniques for longitudinal data. In Handbook of Quantitative Methodology for the Social Sciences; Kaplan, D., Ed.; Sage: Newbury Park, CA, USA, 2004; pp. 345–368. [Google Scholar]
- Costello, A.; Edelbrock, C.; Kalas, R.; Kessler, M.; Klaric, S.A. Diagnostic Interview Schedule for Children (DISC); National Institute of Mental Health: Bethesda, MD, USA, 1982.
- Steenhuis, M.P.; Serra, M.; Minderaa, R.B.; Hartman, C.A. An internet version of the Diagnostic Interview Schedule for Children (DISC-IV): Correspondence with paper and pencil version using the ADHD section. Psychol. Assess. 2009, 21, 231–234. [Google Scholar] [CrossRef]
- Achenbach, T.M.; Ruffle, T.M. The Child Behavior Checklist and related forms for assessing behavioral/emotional problems and competencies. Pediatr. Rev. 2000, 21, 265–271. [Google Scholar] [CrossRef]
- Hartman, C.A.; Luteijn, E.; Serra, M.; Minderaa, R. Refinement of the Children’s Social Behavior Questionnaire (CSBQ): An instrument that describes the diverse problems seen in milder forms of PDD. J. Autism Dev. Disord. 2006, 36, 325–342. [Google Scholar] [CrossRef]
- Putnam, S.P.; Ellis, L.K.; Rothbart, M.K. The structure of temperament from infancy through adolescence. In Advances/Proceedings in Research on Temperament; Eliasz, A., Angleitner, A., Eds.; Pabst Scientist Publisher: Berlin, Germany, 2001; pp. 165–182. [Google Scholar]
- Sattler, J.M. Assessment of Children; (revised and updated 3rd edn); Jerome M. Sattler: San Diego, CA, USA, 1992. [Google Scholar]
- Nagin, D.S.; Tremblay, R.E. Analyzing developmental trajectories of distinct but related behaviors: A group-based method. Psychol. Methods 2001, 6, 18–34. [Google Scholar] [CrossRef]
- Lanza, S.T.; Collins, L.M.; Lemmon, D.; Schafer, J.L. PROC LCA: A SAS procedure for latent class analysis. Struct. Equ. Model. 2007, 14, 671–694. [Google Scholar] [CrossRef]
- Yang, C. Evaluating latent class analysis models in qualitative phenotype identification. Comput. Stat. Data Anal. 2006, 50, 1090–1104. [Google Scholar] [CrossRef]
- Vermunt, J.K. Latent class modeling with covariates: Two improved three-step approaches. Political Anal. 2010, 18, 450–469. [Google Scholar] [CrossRef]
- Vermunt, J.K.; Magidson, J. Technical Guide for Latent GOLD 5.1: Basic, Advanced and Syntax; Statistical Innovations Inc.: Belmont, MA, USA, 2016. [Google Scholar]
- Cubillo, A.; Halari, R.; Smith, A.; Taylor, E.; Rubia, K. A review of fronto-striatal and fronto-cortical brain abnormalities in children and adults with Attention Deficit Hyperactivity Disorder (ADHD) and new evidence for dysfunction in adults with ADHD during motivation and attention. Cortex 2012, 48, 194–215. [Google Scholar] [CrossRef] [PubMed]
- Burnett Heyes, S.; Jih, Y.R.; Block, P.; Hiu, C.F.; Holmes, E.A.; Lau, J.Y. Relationship reciprocation modulates resource allocation in adolescent social networks: Developmental effects. Child Dev. 2015, 86, 1489–1506. [Google Scholar] [CrossRef] [PubMed]
- Koolschijn, P.C.M.; Crone, E.A. Sex differences and structural brain maturation from childhood to early adulthood. Dev. Cogn. Neurosci. 2013, 5, 106–118. [Google Scholar] [CrossRef] [PubMed]
- Ladouceur, C.D. Neural systems supporting cognitive-affective interactions in adolescence: The role of puberty and implications for affective disorders. Front. Integr. Neurosci. 2012, 6, 65. [Google Scholar] [CrossRef]
- Lupien, S.J.; McEwen, B.S.; Gunnar, M.R.; Heim, C. Effects of stress throughout the lifespan on the brain, behaviour and cognition. Nat. Rev. Neurosci. 2009, 10, 434–445. [Google Scholar] [CrossRef]
- Caspi, A.; Houts, R.M.; Belsky, D.W.; Goldman-Mellor, S.J.; Harrington, H.; Israel, S.; Moffitt, T.E. The p factor: One general psychopathology factor in the structure of psychiatric disorders? Clin. Psychol. Sci. 2014, 2, 119–137. [Google Scholar] [CrossRef]
- Bloemen, A.J.P.; Oldehinkel, A.J.; Laceulle, O.M.; Ormel, J.; Rommelse, N.J.; Hartman, C.A. The association between executive functioning and psychopathology: General or specific? Psychol. Med. 2018, 48, 1787–1794. [Google Scholar] [CrossRef]
- Beauchaine, T.P.; Zisner, A.R.; Sauder, C.L. Trait impulsivity and the externalizing spectrum. Ann. Rev. Clin. Psychol. 2017, 13, 343–368. [Google Scholar] [CrossRef]
- Addicoat, A.; Thapar, A.K.; Riglin, L.; Thapar, A.; Collishaw, S. Adult mood problems in children with neurodevelopmental problems: Evidence from a prospective birth cohort followed to age 50. Soc. Psychiatry Psychiatr. Epidemiol. 2019, 1–8. [Google Scholar] [CrossRef]
- Eyre, O.; Hughes, R.A.; Thapar, A.K.; Leibenluft, E.; Stringaris, A.; Davey Smith, G.; Stergiakouli ECollishaw, S.; Thapar, A. Childhood neurodevelopmental difficulties and risk of adolescent depression: The role of irritability. J. Child Psychol. Psychiatry 2019. [Google Scholar] [CrossRef]
- McGough, J.J.; Barkley, R.A. Diagnostic controversies in adult attention deficit hyperactivity disorder. Am. J. Psychiatry 2004, 161, 1948–1956. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Non-ADHD Subgroups | ADHD Subgroups | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Characteristic | Overall | No Problems | Mild Inattention | Mild Internalizing | Moderate Combined | Inattentive | Internalizing Combined | Severe Combined | Wald (df), p-value |
| N (%) | N (%) | N (%) | N (%) | N (%) | N (%) | N (%) | |||
| Overall | 1831 | 389 | 367 | 235 | 267 | 227 | 153 | 193 | 587 (6), p < 0.0001 |
| Cohort | 174053 (6), p < 0.0001 | ||||||||
| Population | 1587 | 389 (100%) | 358 (98%) | 235 (100%) | 204 (76%) | 207 (91%) | 115 (75%) | 80 (41%) | |
| Clinical | 244 | 0 (0%) | 9 (2%) | 0 (0%) | 63 (24%) | 20 (9%) | 38 (25%) | 113 (59%) | |
| Gender | 480 (6), p < 0.0001 | ||||||||
| Female | 583 | 108 (28%) | 68 (19%) | 135 (57%) | 67 (25%) | 65 (29%) | 80 (52%) | 60 (31%) | |
| Male | 1248 | 281 (72%) | 299 (81%) | 100 (43%) | 200 (75%) | 162 (71%) | 73 (48%) | 133 (69%) | |
| SES | 220 (6), p < 0.0001 | ||||||||
| <25% | 474 | 76 (20%) | 88 (24%) | 56 (24%) | 80 (30%) | 55 (24%) | 56 (38%) | 63 (33%) | |
| 25-75% | 890 | 167 (44%) | 186 (51%) | 110 (48%) | 134 (51%) | 117 (52%) | 72 (48%) | 104 (55%) | |
| >75% | 437 | 138 (36%) | 89 (25%) | 64 (28%) | 50 (19%) | 53 (24%) | 21 (14%) | 22 (12%) | |
| Ethnicity | 31 (6), p < 0.0001 | ||||||||
| Western | 1659 | 351 (90%) | 333 (91%) | 207 (88%) | 247 (93%) | 207 (91%) | 132 (87%) | 182 (95%) | |
| Non-western2 | 170 | 38 (10%) | 34 (9%) | 29 (12%) | 20 (7%) | 20 (9%) | 20 (13%) | 9 (5%) | |
| IQ | 206 (6), p < 0.0001 | ||||||||
| Low | 576 | 92 (24%) | 108 (30%) | 53 (23%) | 116 (44%) | 69 (30%) | 62 (41%) | 76 (40%) | |
| Middle | 675 | 145 (37%) | 135 (37%) | 94 (40%) | 97 (36%) | 87 (38%) | 48 (31%) | 69 (36%) | |
| High | 574 | 152 (39%) | 121 (33%) | 88 (37%) | 53 (20%) | 71 (31%) | 43 (28%) | 46 (24%) | |
| ADHD | 1096 (6), p < 0.0001 | ||||||||
| Negative screen | 1222 | 382 (98%) | 315 (86%) | 224 (95%) | 86 (32%) | 147 (65%) | 57 (37%) | 11 (6%) | |
| Positive screen | 365 | 7 (2%) | 43 (12%) | 10 (4%) | 118 (44%) | 60 (26%) | 58 (38%) | 69 (36%) | |
| Clinical3 | 244 | 0 (0%) | 9 (2%) | 1 (1%) | 63 (24%) | 20 (9%) | 38 (25%) | 113 (59%) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hartman, C.A.; Rommelse, N.; van der Klugt, C.L.; Wanders, R.B.K.; Timmerman, M.E. Stress Exposure and the Course of ADHD from Childhood to Young Adulthood: Comorbid Severe Emotion Dysregulation or Mood and Anxiety Problems. J. Clin. Med. 2019, 8, 1824. https://doi.org/10.3390/jcm8111824
Hartman CA, Rommelse N, van der Klugt CL, Wanders RBK, Timmerman ME. Stress Exposure and the Course of ADHD from Childhood to Young Adulthood: Comorbid Severe Emotion Dysregulation or Mood and Anxiety Problems. Journal of Clinical Medicine. 2019; 8(11):1824. https://doi.org/10.3390/jcm8111824
Chicago/Turabian StyleHartman, Catharina A., Nanda Rommelse, Cees L. van der Klugt, Rob B.K. Wanders, and Marieke E. Timmerman. 2019. "Stress Exposure and the Course of ADHD from Childhood to Young Adulthood: Comorbid Severe Emotion Dysregulation or Mood and Anxiety Problems" Journal of Clinical Medicine 8, no. 11: 1824. https://doi.org/10.3390/jcm8111824
APA StyleHartman, C. A., Rommelse, N., van der Klugt, C. L., Wanders, R. B. K., & Timmerman, M. E. (2019). Stress Exposure and the Course of ADHD from Childhood to Young Adulthood: Comorbid Severe Emotion Dysregulation or Mood and Anxiety Problems. Journal of Clinical Medicine, 8(11), 1824. https://doi.org/10.3390/jcm8111824