Identifying Three-Dimensional Facial Fluctuating Asymmetry in Normal Pediatric Individuals: A Panel Assessment Outcome Study of Clinicians and Observers
_周(Chou).jpg)
 ,
,  ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
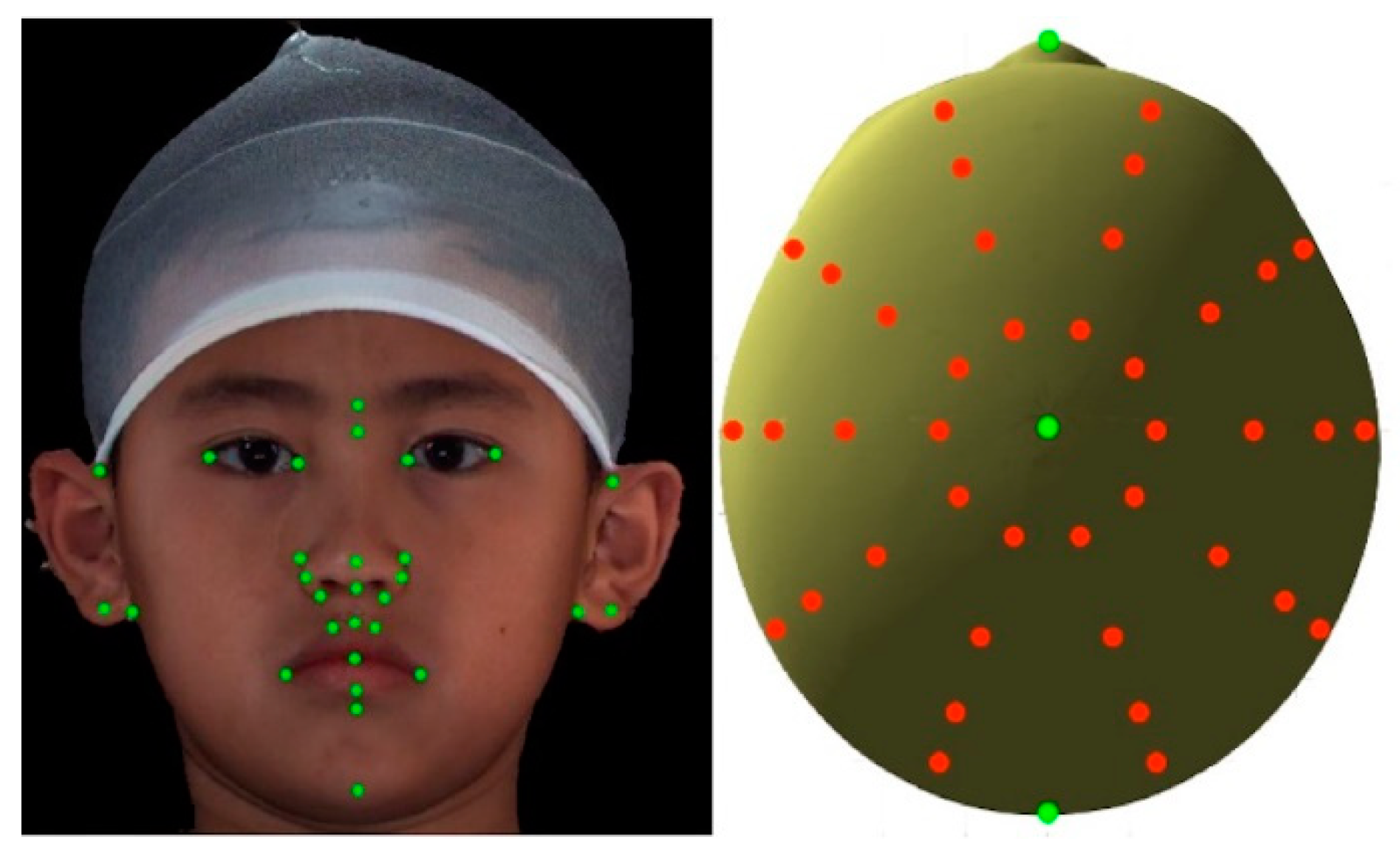
2.1. 3D Facial Image Acquisition
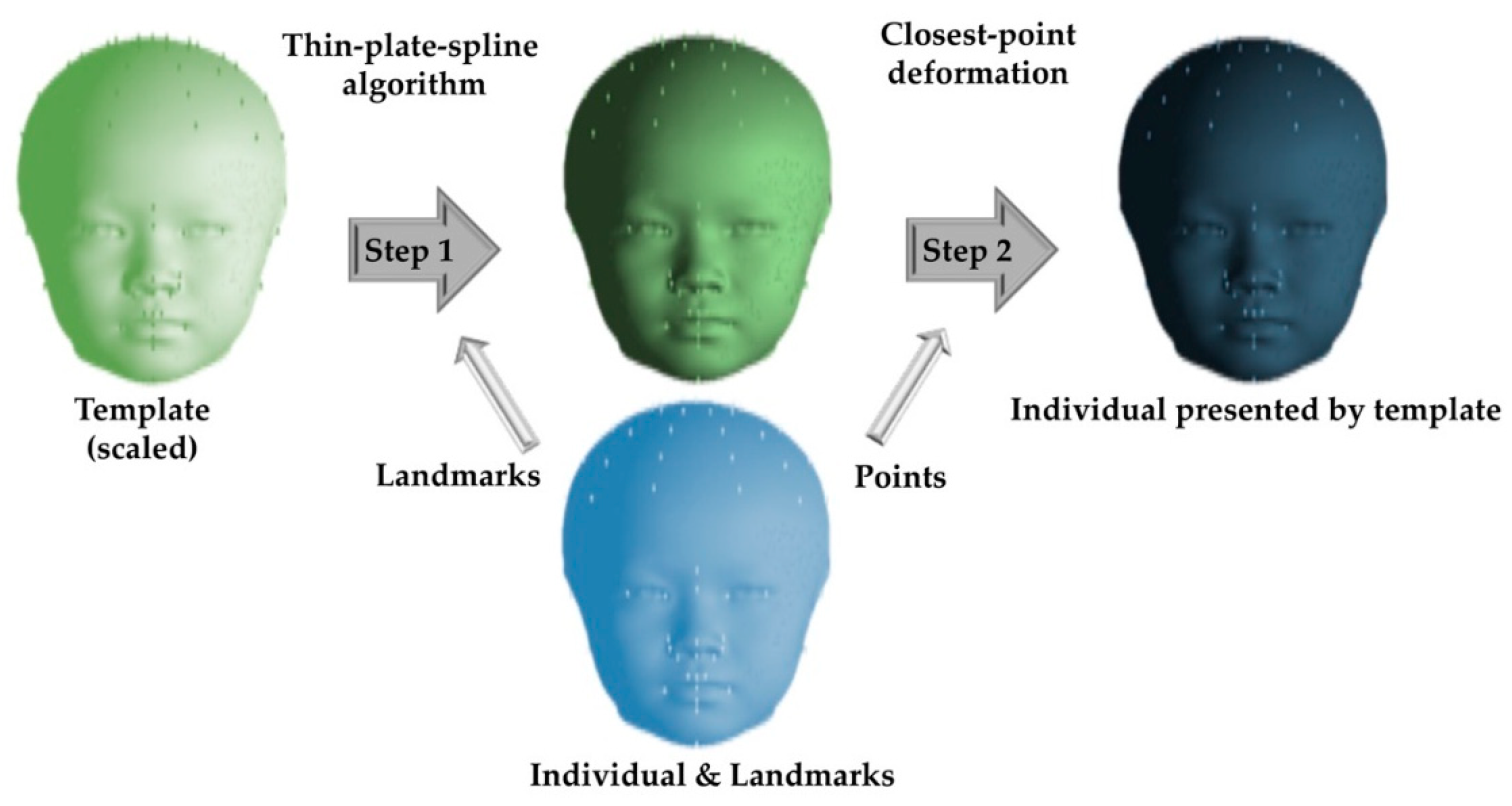
2.2. 3D Data Processing
2.3. Levels of Facial Fluctuating Asymmetry
2.4. Stimuli Processing
2.5. Panel Assessment
2.6. Statistical Analysis
3. Results
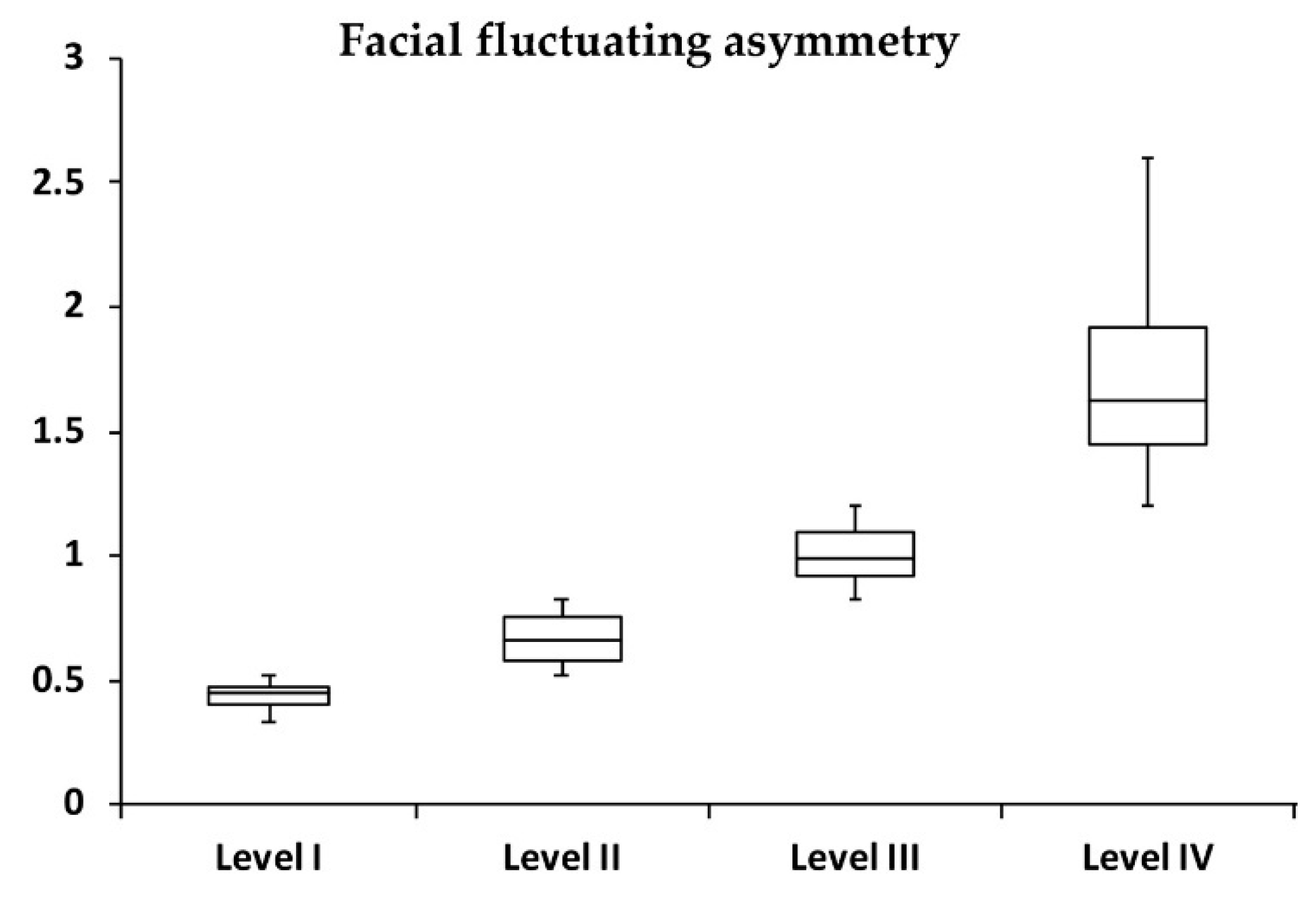
3.1. Levels of Facial Fluctuating Asymmetry
3.2. Panel Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lima-de-Faria, A. The atomic basis of biological symmetry and periodicity. Biosystems 1997, 43, 115–135. [Google Scholar] [CrossRef]
- Gangestad, S.W.; Thornhill, R.; Yeo, R.A. Facial attractiveness, developmental stability, and fluctuating asymmetry. Ethol. Sociobiol. 1994, 15, 73–85. [Google Scholar] [CrossRef]
- Cheong, Y.W.; Lo, L.J. Facial asymmetry: Etiology, evaluation, and management. Chang Gung Med. J. 2011, 34, 341–351. [Google Scholar]
- Wang, T.T.; Wessels, L.; Hussain, G.; Merten, S. Discriminative thresholds in facial asymmetry: A review of the literature. Aesthet. Surg. J. 2017, 37, 375–385. [Google Scholar] [CrossRef]
- Jackson, T.H.; Mitroff, S.R.; Clark, K.; Proffit, W.R.; Lee, J.Y.; Nguyen, T.T. Face symmetry assessment abilities: Clinical implications for diagnosing asymmetry. Am. J. Orthod. Dentofacial Orthop. 2013, 144, 663–671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farkas, L.G.; Katic, J.; Forrest, K. International anthropometric study of facial morphology in various ethnic groups/races. J. Craniofac. Surg. 2005, 16, 615–646. [Google Scholar] [CrossRef]
- Lipira, A.B.; Sachanandani, N.S.; Govier, D.; Payne, A.; Wyas, S.; Kleeschulte, W.; Kane, A.A. Craniobank: An online collection of three-dimensional normative craniofacial images. Plast. Reconstr. Surg. 2010, 126, 70e–72e. [Google Scholar] [CrossRef]
- Taylor, H.O.; Morrison, C.S.; Linden, O.; Phillips, B.; Chang, J.; Byrne, M.E.; Sullivan, S.R.; Forrest, C.R. Quantitative facial asymmetry: Using three-dimensional photogrammetry to measure baseline facial surface symmetry. J. Craniofac. Surg. 2014, 25, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Cho, M.J.; Hallac, R.R.; Ramesh, J.; Seaward, J.R.; Hermann, N.V.; Darvann, T.A.; Lipira, A.; Kane, A.A. Quantifying Normal Craniofacial Form and Baseline Craniofacial Asymmetry in the Pediatric Population. Plast. Reconstr. Surg. 2018, 141, 380e–387e. [Google Scholar] [CrossRef] [PubMed]
- Rolfe, S.; Lee, S.I.; Shapiro, L. Associations Between Genetic Data and Quantitative Assessment of Normal Facial Asymmetry. Front. Genet. 2018, 9, 659. [Google Scholar] [CrossRef]
- Dang, R.R.; Calabrese, C.E.; Burashed, H.M.; Doyle, M.; Vernacchio, L.; Resnick, C.M. Craniofacial anthropometry: Normative data for caucasian infants. J. Craniofac. Surg. 2019. [Google Scholar] [CrossRef] [PubMed]
- Mercan, E.; Oestreich, M.; Fisher, D.M.; Allori, A.C.; Beals, S.P.; Samson, T.D.; Sitzman, T.J.; Matic, D.B.; Siebold, B.S.; Tse, R.W. Objective assessment of the unilateral cleft lip nasal deformity using three-dimensional stereophotogrammetry: Severity and outcome. Plast. Reconstr. Surg. 2018, 141, 547e–558e. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Liang, S.; Shapiro, L.; Tse, R. Measuring symmetry in children with cleft lip. Part 2: Quantification of nasolabial symmetry before and after cleft lip repair. Cleft. Palate Craniofac. J. 2016, 53, 705–713. [Google Scholar] [CrossRef] [PubMed]
- Tse, R.; Booth, L.; Keys, K.; Saltzman, B.; Stuhaug, E.; Kapadia, H.; Heike, C. Reliability of nasolabial anthropometric measures using three-dimensional stereophotogrammetry in infants with unrepaired unilateral cleft lip. Plast. Reconstr. Surg. 2014, 133, 530e–542e. [Google Scholar] [CrossRef]
- Heike, C.L.; Upson, K.; Stuhaug, E.; Weinberg, S.M. 3D digital stereophotogrammetry: A practical guide to facial image acquisition. Head Face Med. 2010, 6, 18. [Google Scholar] [CrossRef] [PubMed]
- Al-Omari, I.; Millett, D.T.; Ayoub, A.F. Methods of assessment of cleft-related facial deformity: A review. Cleft. Palate Craniofac. J. 2005, 42, 145–156. [Google Scholar] [CrossRef] [PubMed]
- Lo, L.J.; Wong, F.H.; Mardini, S.; Chen, Y.R.; Noordhoff, M.S. Assessment of bilateral cleft lip nose deformity: A comparison of results as judged by cleft surgeons and laypersons. Plast. Reconstr. Surg. 2002, 110, 733–738. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.F.; Dumrongwongsiri, S.; Lo, L.J. Perception of lip can’t as a sign of facial deformity: Assessment by laypersons and professionals on composite face photographs. Ann. Plast. Surg. 2019, 82, S140–S143. [Google Scholar] [CrossRef]
- Jarosz, K.F.; Bosio, J.A.; Bloomstein, R.; Jiang, S.S.; Vakharia, N.S.; Cangialosi, T.J. Perceptions of chin asymmetries among dental professionals and laypersons. Am. J. Orthod. Dentofacial Orthop. 2018, 154, 201–212. [Google Scholar] [CrossRef]
- Meyer-Marcotty, P.; Alpers, G.W.; Gerdes, A.B.M.; Stellzig-Eisenhauer, A. Impact of facial asymmetry in visual perception: A 3-dimensional data analysis. Am. J. Orthod. Dentofacial Orthop. 2010, 137, 168.e1–168.e8. [Google Scholar] [CrossRef]
- Meyer-Marcotty, P.; Stellzig-Eisenhauer, A.; Bareis, U.; Hartmann, J.; Kochel, J. Three-dimensional perception of facial asymmetry. Eur. J. Orthod. 2011, 33, 647–653. [Google Scholar] [CrossRef] [Green Version]
- McAvinchey, G.; Maxim, F.; Nix, B.; Djordjevic, J.; Linklater, R.; Landini, G. The perception of facial asymmetry using 3-dimensional simulated images. Angle Orthod. 2014, 84, 957–965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cassi, D.; Battistoni, G.; Magnifico, M.; Di Blasio, C.; Pedrazzi, G.; Di Blasio, A. Three-dimensional evaluation of facial asymmetry in patients with hemifacial microsomia using stereophotogrammetry. J. Craniomaxillofac. Surg. 2019, 47, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Liang, S.; Shapiro, L.; Tse, R. Measuring symmetry in children with cleft lip. Part 3: Quantifying nasal symmetry and nasal normalcy before and after unilateral cleft lip repair. Cleft. Palate Craniofac. J. 2017, 54, 602–611. [Google Scholar] [CrossRef]
- Denadai, R.; Buzzo, C.L.; Raposo-Amaral, C.A.; Raposo-Amaral, C.E. Facial contour symmetry outcomes after site-specific facial fat compartment augmentation with fat grafting in facial deformities. Plast. Reconstr. Surg. 2019, 143, 544–556. [Google Scholar] [CrossRef] [PubMed]
- Kokich, V.O.; Kokich, V.G.; Kiyak, H.A. Perceptions of dental professionals and laypersons to altered dental esthetics: Asymmetric and symmetric situations. Am. J. Orthod. Dentofacial Orthop. 2006, 130, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Kerr, W.J.S.; O’Donell, J.M. Panel perception of facial attractiveness. Br. J. Orthod. 1990, 17, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Denadai, R.; Raposo-Amaral, C.A.; Buzzo, C.L.; Raposo-Amaral, C.E. Isolated autologous free fat grafting for management of facial contour asymmetry in a subset of growing patients with craniofacial microsomia. Ann. Plast. Surg. 2016, 76, 288–294. [Google Scholar] [CrossRef] [PubMed]
- Bornstein, M.H.; Ferdinandsen, K.; Gross, C.G. Perception of symmetry in infancy. Dev. Psychol. 1981, 17, 82. [Google Scholar] [CrossRef]
- Rhodes, G.; Geddes, K.; Jeffery, L.; Dziurawiec, S.; Clark, A. Are average and symmetric faces attractive to infants? Discrimination and looking preferences. Perception 2002, 31, 315–321. [Google Scholar] [CrossRef] [Green Version]
- Saxton, T.K.; DeBruine, L.M.; Jones, B.C.; Little, A.C.; Craig Roberts, S.A. longitudinal study of adolescents’ judgments of the attractiveness of facial symmetry, averageness and sexual dimorphism. J. Evol. Psychol. 2011, 9, 43–55. [Google Scholar] [CrossRef]
- Vingilis-Jaremko, L.; Maurer, D. The influence of symmetry on children’s judgments of facial attractiveness. Perception 2013, 42, 302–320. [Google Scholar] [CrossRef]
- Farrera, A.; Villanueva, M.; Quinto-Sánchez, M.; González-José, R. The relationship between facial shape asymmetry and attractiveness in Mexican students. Am. J. Hum. Biol. 2015, 27, 387–396. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Xue, X.; Spelke, E.; Huang, L.; Zheng, W.; Peng, K. The aesthetic preference for symmetry dissociates from early-emerging attention to symmetry. Sci. Rep. 2018, 8, 6263. [Google Scholar] [CrossRef] [Green Version]
- Boothroyd, L.G.; Meins, E.; Vukovic, J.; Burt, D.M. Developmental changes in children’s facial preferences. Evol. Hum. Behav. 2014, 35, 376–383. [Google Scholar] [CrossRef]
- Bashour, M. History and current concepts in the analysis of facial attractiveness. Plast. Reconstr. Surg. 2006, 118, 741–756. [Google Scholar] [CrossRef] [PubMed]
- Baudouin, J.Y.; Tiberghien, G. Symmetry, averageness, and feature size in the facial attractiveness of women. Acta Psychol. (Amst). 2004, 117, 313–332. [Google Scholar] [CrossRef] [PubMed]
- Richman, L.C.; McCoy, T.E.; Conrad, A.L.; Nopoulos, P.C. Neuropsychological, behavioral, and academic sequelae of cleft: Early developmental, school age, and adolescent/young adult outcomes. Cleft. Palate Craniofac. J. 2012, 49, 387–396. [Google Scholar] [CrossRef] [PubMed]
- Horwood, J. Common visual defects and peer victimization in children. Invest. Ophthalmol. Vis. Sci. 2005, 46, 1177–1181. [Google Scholar] [CrossRef]
- Feragen, K.B.; Borge, A.I.; Rumsey, N. Social experience in 10-year-old children born with a cleft: Exploring psychosocial resilience. Cleft. Palate Craniofac. J. 2009, 46, 65–74. [Google Scholar] [CrossRef]
- Edwards, T.C.; Patrick, D.L.; Topolski, T.D.; Aspinall, C.L.; Mouradian, W.E.; Speltz, M.L. Approaches to craniofacial-specific quality of life assessment in adolescents. Cleft. Palate Craniofac. J. 2005, 42, 19–24. [Google Scholar] [CrossRef]
- Edwards, T.C.; Topolski, T.D.; Kapp-Simon, K.A.; Aspinall, C.L.; Patrick, D.L. What difference can a minute make? Social skills and first impressions of youth with craniofacial differences. Cleft. Palate Craniofac. J. 2011, 48, 91–97. [Google Scholar] [CrossRef]
- Strauss, R.P.; Ramsey, B.L.; Edwards, T.C.; Topolski, T.D.; Kapp-Simon, K.A.; Thomas, C.R.; Fenson, C.; Patrick, D.L. Stigma experiences in youth with facial differences: A multi-site study of adolescents and their mothers. Orthod. Craniofac. Res. 2007, 10, 96–103. [Google Scholar] [CrossRef] [PubMed]
- Lovegrove, E.; Rumsey, N. Ignoring it doesn’t make it stop: Adolescents, appearance, and bullying. Cleft. Palate Craniofac. J. 2005, 42, 33–44. [Google Scholar] [CrossRef] [PubMed]
- Masnari, O.; Landolt, M.A.; Roessler, J.; Weingaertner, S.K.; Neuhaus, K.; Meuli, M.; Schiestl, C. Self- and parent-perceived stigmatisation in children and adolescents with congenital or acquired facial differences. J. Plast. Reconstr. Aesthet. Surg. 2012, 65, 1664–1670. [Google Scholar] [CrossRef] [PubMed]
- Denadai, R.; Raposo-Amaral, C.A.; Buzzo, C.L.; Raposo-Amaral, C.E. Autologous free fat grafting for management of the facial contour asymmetry. J. Craniofac. Surg. 2018, 29, 878–886. [Google Scholar] [CrossRef] [PubMed]
- Denadai, R.; Raposo-Amaral, C.A.; Buzzo, C.L.; Raposo-Amaral, C.E. Isolated fat grafting for reconstruction of lower face volumetric asymmetry in skeletally immature patients: A clinical outcome study. Ann. Plast. Surg. 2019. [Google Scholar] [CrossRef]
- Krastev, T.K.; Beugels, J.; Hommes, J.; Piatkowski, A.; Mathijssen, I.; van der Hulst, R. Efficacy and safety of autologous fat transfer in facial reconstructive surgery: A systematic review and meta-analysis. JAMA Facial Plast. Surg. 2018, 20, 351–360. [Google Scholar] [CrossRef]
- Denadai, R.; Raposo-Amaral, C.A.; da Silva, S.A.; Buzzo, C.L.; Raposo-Amaral, C.E. Complementary fat graft retention rates are superior to initial rates in craniofacial contour reconstruction. Plast. Reconstr. Surg. 2019, 143, 823–835. [Google Scholar] [CrossRef] [PubMed]
- Tringale, K.R.; Lance, S.; Schoenbrunner, A.; Gosman, A.A. Sustained overcorrection after autologous facial fat grafting in the pediatric population: A Case Series. Ann. Plast. Surg. 2017, 78, S217–S221. [Google Scholar] [CrossRef]
- Denadai, R.; Raposo-Amaral, C.A.; Pinho, A.S.; Lameiro, T.M.; Buzzo, C.L.; Raposo-Amaral, C.E. Predictors of autologous free fat graft retention in the management of craniofacial contour deformities. Plast. Reconstr. Surg. 2017, 140, 50e–61e. [Google Scholar] [CrossRef] [PubMed]
- Guibert, M.; Franchi, G.; Ansari, E.; Billotet, B.; Diner, P.A.; Cassier, S.; Vazquez, M.P.; Picard, A.; Kadlub, N. Fat graft transfer in children’s facial malformations: A prospective three-dimensional evaluation. J. Plast. Reconstr. Aesthet. Surg. 2013, 66, 799–804. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameters | Individuals (n = 600) |
|---|---|
| Facial fluctuating asymmetry overall m ± sd | 0.96 ± 0.52 (0.327–2.602) |
| Male/Female n (%) | 300 (50)/300 (50) |
| Age (years) m ± sd | 7.98 ± 1.19 |
| 6–8 n (%) | 432 (72) |
| 9–12 n (%) | 168 (28) |
| Facial fluctuating asymmetric level I m ± sd | 0.44 ± 0.05 (0.327–0.518) |
| Male/Female n (%) | 78 (52)/72 (48) * |
| Age (years) m ± sd | 7.81 ± 1.16 * |
| 6–8 years n (%) | 115 (76.67) |
| 9–12 years n (%) | 35 (23.33) |
| Facial fluctuating asymmetric level II m ± sd | 0.67 ± 0.09 (0.519–0.827) |
| Male/Female n (%) | 70 (46.67)/80 (53.33) * |
| Age (years) m ± sd | 7.99 ± 1.14 * |
| 6–8 years n (%) | 115 (76.67) |
| 9–12 years n (%) | 35 (23.33) |
| Facial fluctuating asymmetric level IIII m ± sd | 1.01 ± 0.10 (0.830–1.119) |
| Male/Female n (%) | 75 (50)/75 (50) * |
| Age (years) m ± sd | 8.11 ± 1.32 * |
| 6–8 years n (%) | 103 (68.67) |
| 9–12 years n (%) | 47 (31.33) |
| Facial fluctuating asymmetric level IV m ± sd | 1.71 ± 0.36 (1.204–2.602) |
| Male/Female n (%) | 78 (52)/72 (48) * |
| Age (years) m ± sd | 7.99 ± 1.12 * |
| 6–8 years n (%) | 99 (66) |
| 9–12 years n (%) | 51 (34) |
| Facial Fluctuating Asymmetry | Categories of Raters | p-Value **,# | ||
|---|---|---|---|---|
| Plastic Surgeons | Adult Observers | Pre-Adolescent Observers | ||
| Overall | 2.60 ± 0.94 | 2.05 ± 1.10 | 2.74 ± 0.84 | >0.05 |
| Level I | 1.40 ± 1.14 | 1.26 ± 1.15 | 2.17 ± 1.17 | <0.05 ‡ |
| Level II | 2.65 ± 1.23 | 1.89 ± 1.15 | 2.38 ± 1.15 | >0.05 |
| Level III | 3.20 ± 1.06 | 2.53 ± 1.54 | 3.26 ± 1.23 | >0.05 |
| Level IV | 3.15 ± 1.35 | 2.53 ± 1.35 | 3.17 ± 1.15 | >0.05 |
| p-value *,# | <0.05 † | <0.05 † | <0.05 † | – |
| Categories of Raters | Intra-Rater Reliability (Cronbach’s Alpha Coefficient) | Inter-Rater Reliability (k) |
|---|---|---|
| Plastic surgeons | 0.792 | 0.136 |
| Adult observers | 0.864 | 0.105 |
| Pre-adolescent observers | 0.681 | 0.070 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chou, P.-Y.; Denadai, R.; Chen, S.-H.; Tseng, H.-J.; Hsu, C.-K.; Wang, S.-W.; Hallac, R.; Chen, C.-H.; Kane, A.A.; Lo, L.-J. Identifying Three-Dimensional Facial Fluctuating Asymmetry in Normal Pediatric Individuals: A Panel Assessment Outcome Study of Clinicians and Observers. J. Clin. Med. 2019, 8, 648. https://doi.org/10.3390/jcm8050648
Chou P-Y, Denadai R, Chen S-H, Tseng H-J, Hsu C-K, Wang S-W, Hallac R, Chen C-H, Kane AA, Lo L-J. Identifying Three-Dimensional Facial Fluctuating Asymmetry in Normal Pediatric Individuals: A Panel Assessment Outcome Study of Clinicians and Observers. Journal of Clinical Medicine. 2019; 8(5):648. https://doi.org/10.3390/jcm8050648
Chicago/Turabian StyleChou, Pang-Yun, Rafael Denadai, Shih-Heng Chen, Hsiao-Jung Tseng, Chih-Kai Hsu, Sheng-Wei Wang, Rami Hallac, Chih-Hao Chen, Alex A. Kane, and Lun-Jou Lo. 2019. "Identifying Three-Dimensional Facial Fluctuating Asymmetry in Normal Pediatric Individuals: A Panel Assessment Outcome Study of Clinicians and Observers" Journal of Clinical Medicine 8, no. 5: 648. https://doi.org/10.3390/jcm8050648
APA StyleChou, P.-Y., Denadai, R., Chen, S.-H., Tseng, H.-J., Hsu, C.-K., Wang, S.-W., Hallac, R., Chen, C.-H., Kane, A. A., & Lo, L.-J. (2019). Identifying Three-Dimensional Facial Fluctuating Asymmetry in Normal Pediatric Individuals: A Panel Assessment Outcome Study of Clinicians and Observers. Journal of Clinical Medicine, 8(5), 648. https://doi.org/10.3390/jcm8050648