The Role of a “Treat-to-Target” Approach in the Long-Term Renal Outcomes of Patients with Gout


Abstract
:1. Introduction
2. Methods
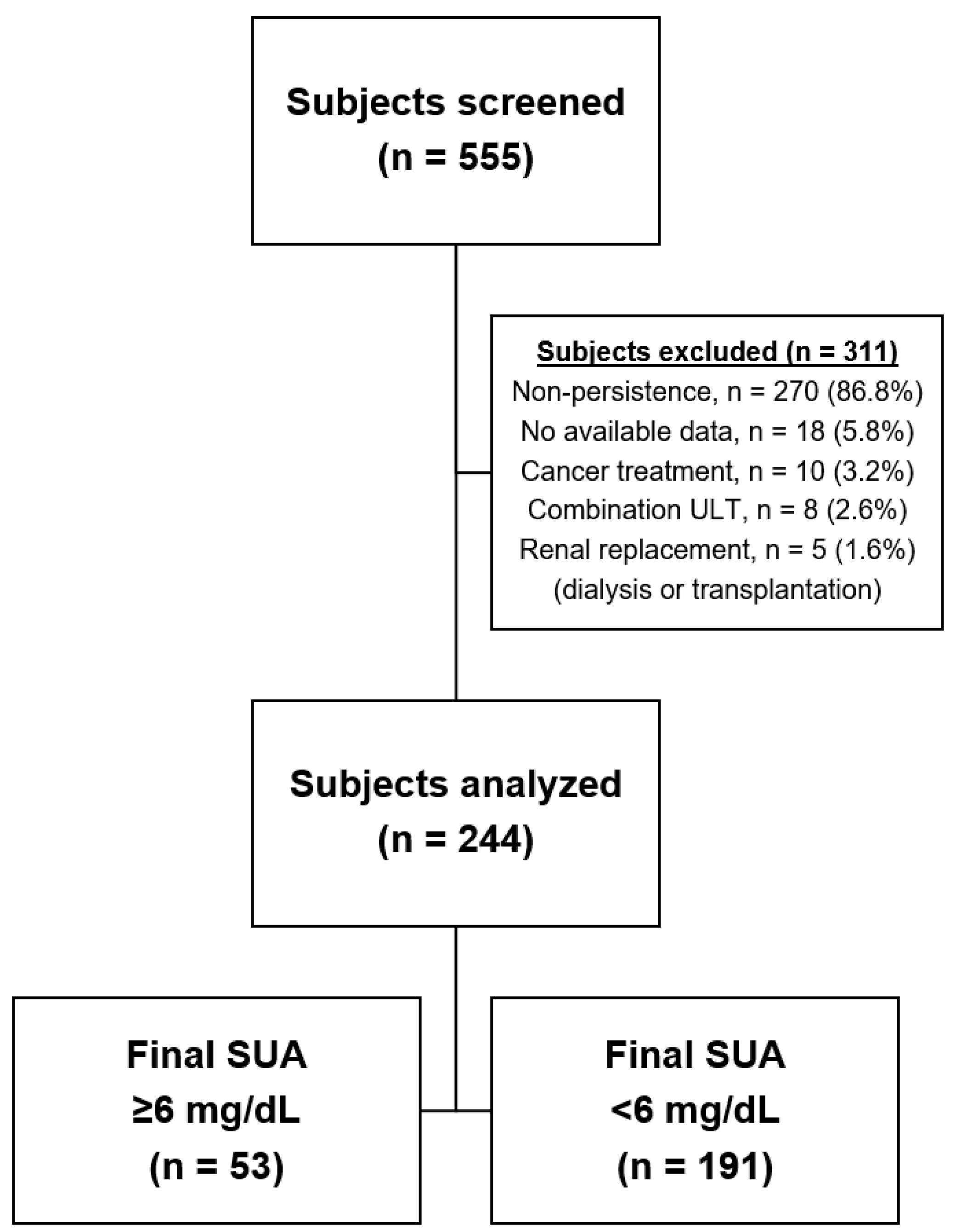
2.1. Patients
2.2. Study Design
2.3. Outcomes
2.4. Statistical Analysis
2.5. Ethical Considerations
3. Results
3.1. Subject Characteristics
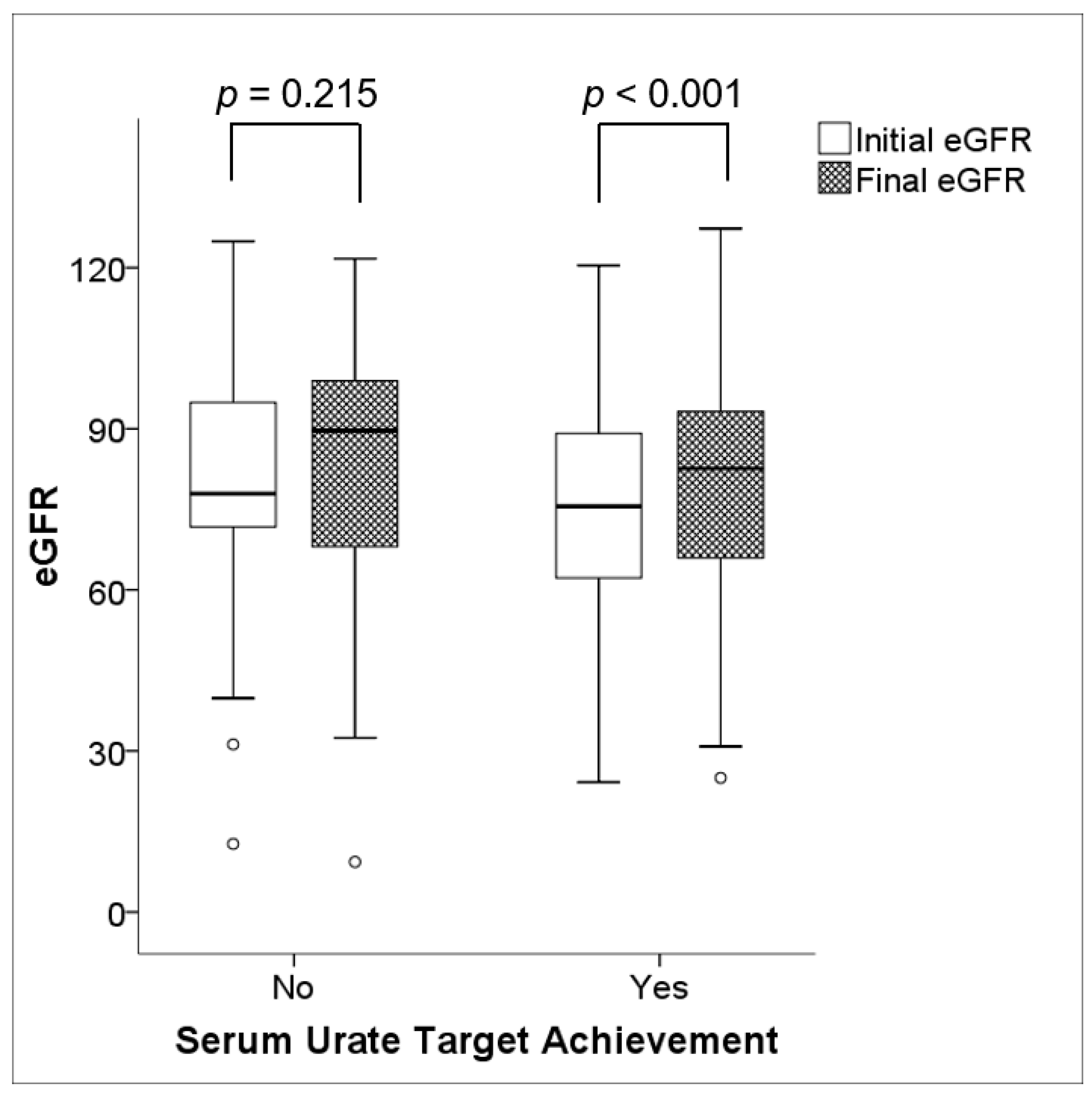
3.2. Long-Term Renal Outcomes
3.3. Predictors of the Improvement in Renal Function
3.4. Adverse Events
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Kuo, C.F.; Grainge, M.J.; Zhang, W.; Doherty, M. Global epidemiology of gout: Prevalence, incidence and risk factors. Nat. Rev. Rheumatol. 2015, 11, 649–662. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Pandya, B.J.; Choi, H.K. Comorbidities of gout and hyperuricemia in the US general population: NHANES 2007-2008. Am. J. Med. 2012, 125, 679–687. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, E. Reduced glomerular function and prevalence of gout: NHANES 2009-10. PLoS ONE 2012, 7, e50046. [Google Scholar] [CrossRef] [PubMed]
- Roughley, M.J.; Belcher, J.; Mallen, C.D.; Roddy, E. Gout and risk of chronic kidney disease and nephrolithiasis: Meta-analysis of observational studies. Arthritis Res. Ther. 2015, 17, 90. [Google Scholar] [CrossRef] [PubMed]
- Roughley, M.; Sultan, A.A.; Clarson, L.; Muller, S.; Whittle, R.; Belcher, J.; Mallen, C.D.; Roddy, E. Risk of chronic kidney disease in patients with gout and the impact of urate lowering therapy: A population-based cohort study. Arthritis Res. Ther. 2018, 20, 243. [Google Scholar] [CrossRef]
- Yu, K.H.; Kuo, C.F.; Luo, S.F.; See, L.C.; Chou, I.J.; Chang, H.C.; Chiou, M.J. Risk of end-stage renal disease associated with gout: A nationwide population study. Arthritis Res. Ther. 2012, 14, R83. [Google Scholar] [CrossRef] [PubMed]
- Mandal, A.K.; Mount, D.B. The molecular physiology of uric acid homeostasis. Annu. Rev. Physiol. 2015, 77, 323–345. [Google Scholar] [CrossRef]
- Perez-Ruiz, F.; Calabozo, M.; Erauskin, G.G.; Ruibal, A.; Herrero-Beites, A.M. Renal underexcretion of uric acid is present in patients with apparent high urinary uric acid output. Arthritis Care Res. 2002, 47, 610–613. [Google Scholar] [CrossRef]
- Kang, D.H.; Nakagawa, T.; Feng, L.; Watanabe, S.; Han, L.; Mazzali, M.; Truong, L.; Harris, R.; Johnson, R.J. A role for uric acid in the progression of renal disease. J. Am. Soc. Nephrol. 2002, 13, 2888–2897. [Google Scholar] [CrossRef]
- Obermayr, R.P.; Temml, C.; Gutjahr, G.; Knechtelsdorfer, M.; Oberbauer, R.; Klauser-Braun, R. Elevated uric acid increases the risk for kidney disease. J. Am. Soc. Nephrol. 2008, 19, 2407–2413. [Google Scholar] [CrossRef]
- Ejaz, A.A.; Mu, W.; Kang, D.H.; Roncal, C.; Sautin, Y.Y.; Henderson, G.; Tabah-Fisch, I.; Keller, B.; Beaver, T.M.; Nakagawa, T.; et al. Could uric acid have a role in acute renal failure? Clin. J. Am. Soc. Nephrol. 2007, 2, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Ben-Dov, I.Z.; Kark, J.D. Serum uric acid is a GFR-independent long-term predictor of acute and chronic renal insufficiency: The Jerusalem Lipid Research Clinic cohort study. Nephrol. Dial. Transplant. 2011, 26, 2558–2566. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Lozada, L.G.; Tapia, E.; Santamaria, J.; Avila-Casado, C.; Soto, V.; Nepomuceno, T.; Rodriguez-Iturbe, B.; Johnson, R.J.; Herrera-Acosta, J. Mild hyperuricemia induces vasoconstriction and maintains glomerular hypertension in normal and remnant kidney rats. Kidney Int. 2005, 67, 237–247. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Yang, C.; Zhao, Y.; Zeng, X.; Liu, F.; Fu, P. Is hyperuricemia an independent risk factor for new-onset chronic kidney disease? A systematic review and meta-analysis based on observational cohort studies. BMC Nephrol. 2014, 15, 122. [Google Scholar] [CrossRef] [PubMed]
- Sircar, D.; Chatterjee, S.; Waikhom, R.; Golay, V.; Raychaudhury, A.; Chatterjee, S.; Pandey, R. Efficacy of Febuxostat for Slowing the GFR Decline in Patients with CKD and Asymptomatic Hyperuricemia: A 6-Month, Double-Blind, Randomized, Placebo-Controlled Trial. Am. J. Kidney Dis. 2015, 66, 945–950. [Google Scholar] [CrossRef] [PubMed]
- Goicoechea, M.; Garcia de Vinuesa, S.; Verdalles, U.; Verde, E.; Macias, N.; Santos, A.; Perez de Jose, A.; Cedeno, S.; Linares, T.; Luno, J. Allopurinol and progression of CKD and cardiovascular events: Long-term follow-up of a randomized clinical trial. Am. J. Kidney Dis. 2015, 65, 543–549. [Google Scholar] [CrossRef] [PubMed]
- Siu, Y.P.; Leung, K.T.; Tong, M.K.; Kwan, T.H. Use of allopurinol in slowing the progression of renal disease through its ability to lower serum uric acid level. Am. J. Kidney Dis. 2006, 47, 51–59. [Google Scholar] [CrossRef]
- Perez-Ruiz, F. Treating to target: A strategy to cure gout. Rheumatology 2009, 48 (Suppl. 2), ii9–ii14. [Google Scholar] [CrossRef]
- Khanna, D.; Fitzgerald, J.D.; Khanna, P.P.; Bae, S.; Singh, M.K.; Neogi, T.; Pillinger, M.H.; Merill, J.; Lee, S.; Prakash, S.; et al. 2012 American College of Rheumatology guidelines for management of gout. Part 1: Systematic nonpharmacologic and pharmacologic therapeutic approaches to hyperuricemia. Arthritis Care Res. 2012, 64, 1431–1446. [Google Scholar] [CrossRef] [Green Version]
- Richette, P.; Doherty, M.; Pascual, E.; Barskova, V.; Becce, F.; Castaneda-Sanabria, J.; Coyfish, M.; Guillo, S.; Jansen, T.L.; Janssens, H.; et al. 2016 updated EULAR evidence-based recommendations for the management of gout. Ann. Rheum. Dis. 2017, 76, 29–42. [Google Scholar] [CrossRef]
- Qaseem, A.; Harris, R.P.; Forciea, M.A.; Clinical Guidelines Committee of the American College of Physicians. Management of Acute and Recurrent Gout: A Clinical Practice Guideline from the American College of Physicians. Ann. Intern. Med. 2017, 166, 58–68. [Google Scholar] [CrossRef]
- Gibson, T.; Rodgers, V.; Potter, C.; Simmonds, H.A. Allopurinol treatment and its effect on renal function in gout: A controlled study. Ann. Rheum. Dis. 1982, 41, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Whelton, A.; Macdonald, P.A.; Zhao, L.; Hunt, B.; Gunawardhana, L. Renal function in gout: Long-term treatment effects of febuxostat. J. Clin. Rheumatol. 2011, 17, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.A.; Seo, Y.I.; Song, Y.W. Four-week effects of allopurinol and febuxostat treatments on blood pressure and serum creatinine level in gouty men. J. Korean Med. Sci. 2014, 29, 1077–1081. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Wei, L.; Chen, H.; Zhang, Z.; Yu, Q.; Ji, Z.; Jiang, L. Influence of urate-lowering therapies on renal handling of uric acid. Clin. Rheumatol. 2016, 35, 133–141. [Google Scholar] [CrossRef]
- Saag, K.G.; Whelton, A.; Becker, M.A.; MacDonald, P.; Hunt, B.; Gunawardhana, L. Impact of Febuxostat on Renal Function in Gout Patients with Moderate-to-Severe Renal Impairment. Arthritis Rheumatol. 2016, 68, 2035–2043. [Google Scholar] [CrossRef]
- Vargas-Santos, A.B.; Peloquin, C.E.; Zhang, Y.; Neogi, T. Association of Chronic Kidney Disease with Allopurinol Use in Gout Treatment. JAMA Intern. Med. 2018, 178, 1526–1533. [Google Scholar] [CrossRef]
- Zhang, W.; Doherty, M.; Bardin, T.; Pascual, E.; Barskova, V.; Conaghan, P.; Gerster, J.; Jacobs, J.; Leeb, B.; Liote, F.; et al. EULAR evidence based recommendations for gout. Part II: Management. Report of a task force of the EULAR Standing Committee for International Clinical Studies Including Therapeutics (ESCISIT). Ann. Rheum. Dis. 2006, 65, 1312–1324. [Google Scholar] [CrossRef]
- Levey, A.S.; Coresh, J.; Balk, E.; Kausz, A.T.; Levin, A.; Steffes, M.W.; Hogg, R.J.; Perrone, R.D.; Lau, J.; Eknoyan, G.; et al. National Kidney Foundation practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Ann. Intern. Med. 2003, 139, 137–147. [Google Scholar] [CrossRef]
- Stevens, P.E.; Levin, A. Kidney Disease: Improving Global Outcomes Chronic Kidney Disease Guideline Development Work Group Members. Evaluation and management of chronic kidney disease: Synopsis of the kidney disease: Improving global outcomes 2012 clinical practice guideline. Ann. Intern. Med. 2013, 158, 825–830. [Google Scholar] [CrossRef]
- Palevsky, P.M.; Liu, K.D.; Brophy, P.D.; Chawla, L.S.; Parikh, C.R.; Thakar, C.V.; Tolwani, A.J.; Waikar, S.S.; Weisbord, S.D. KDOQI US commentary on the 2012 KDIGO clinical practice guideline for acute kidney injury. Am. J. Kidney Dis. 2013, 61, 649–672. [Google Scholar] [CrossRef]
- Li-Yu, J.; Clayburne, G.; Sieck, M.; Beutler, A.; Rull, M.; Eisner, E.; Schumacher, H.R., Jr. Treatment of chronic gout. Can we determine when urate stores are depleted enough to prevent attacks of gout? J. Rheumatol. 2001, 28, 577–580. [Google Scholar]
- Shoji, A.; Yamanaka, H.; Kamatani, N. A retrospective study of the relationship between serum urate level and recurrent attacks of gouty arthritis: Evidence for reduction of recurrent gouty arthritis with antihyperuricemic therapy. Arthritis Rheum. 2004, 51, 321–325. [Google Scholar] [CrossRef]
- Schumacher, H.R., Jr.; Becker, M.A.; Lloyd, E.; MacDonald, P.A.; Lademacher, C. Febuxostat in the treatment of gout: 5-yr findings of the FOCUS efficacy and safety study. Rheumatology 2009, 48, 188–194. [Google Scholar] [CrossRef]
- Kuo, C.F.; Luo, S.F.; See, L.C.; Ko, Y.S.; Chen, Y.M.; Hwang, J.S.; Chou, I.J.; Chang, H.C.; Chen, H.W.; Yu, K.H. Hyperuricaemia and accelerated reduction in renal function. Scand. J. Rheumatol. 2011, 40, 116–121. [Google Scholar] [CrossRef]
- Cohen, E.; Nardi, Y.; Krause, I.; Goldberg, E.; Milo, G.; Garty, M.; Krause, I. A longitudinal assessment of the natural rate of decline in renal function with age. J. Nephrol. 2014, 27, 635–641. [Google Scholar] [CrossRef]
- Kim, Y.; Shin, S.; Kim, K.; Choi, S.; Lee, K. Effect of Urate Lowering Therapy on Renal Disease Progression in Hyperuricemic Patients with Chronic Kidney Disease. J. Rheumatol. 2015, 42, 2143–2148. [Google Scholar] [CrossRef]
- Levy, G.; Shi, J.M.; Cheetham, T.C.; Rashid, N. Urate-Lowering Therapy in Moderate to Severe Chronic Kidney Disease. Perm. J. 2018, 22, 17–142. [Google Scholar] [CrossRef]
- Levy, G.D.; Rashid, N.; Niu, F.; Cheetham, T.C. Effect of urate-lowering therapies on renal disease progression in patients with hyperuricemia. J. Rheumatol. 2014, 41, 955–962. [Google Scholar] [CrossRef]
- Eriksen, B.O.; Ingebretsen, O.C. The progression of chronic kidney disease: A 10-year population-based study of the effects of gender and age. Kidney Int. 2006, 69, 375–382. [Google Scholar] [CrossRef] [Green Version]
- Fraser, S.D.; Roderick, P.J.; May, C.R.; McIntyre, N.; McIntyre, C.; Fluck, R.J.; Shardlow, A.; Taal, M.W. The burden of comorbidity in people with chronic kidney disease stage 3: A cohort study. BMC Nephrol. 2015, 16, 193. [Google Scholar] [CrossRef]
- Mohammed, E.; Browne, L.D.; Kumar, A.U.A.; Adeeb, F.; Fraser, A.D.; Stack, A.G. Prevalence and treatment of gout among patients with chronic kidney disease in the Irish health system: A national study. PLoS ONE 2019, 14, e0210487. [Google Scholar] [CrossRef]
- Jing, J.; Kielstein, J.T.; Schultheiss, U.T.; Sitter, T.; Titze, S.I.; Schaeffner, E.S.; McAdams-DeMarco, M.; Kronenberg, F.; Eckardt, K.U.; Kottgen, A.; et al. Prevalence and correlates of gout in a large cohort of patients with chronic kidney disease: The German Chronic Kidney Disease (GCKD) study. Nephrol. Dial. Transplant. 2015, 30, 613–621. [Google Scholar] [CrossRef]
- Zhang, Q.L.; Rothenbacher, D. Prevalence of chronic kidney disease in population-based studies: Systematic review. BMC Public Health 2008, 8, 117. [Google Scholar] [CrossRef]
- Rashid, N.; Coburn, B.W.; Wu, Y.L.; Cheetham, T.C.; Curtis, J.R.; Saag, K.G.; Mikuls, T.R. Modifiable factors associated with allopurinol adherence and outcomes among patients with gout in an integrated healthcare system. J. Rheumatol. 2015, 42, 504–512. [Google Scholar] [CrossRef]
- Coburn, B.W.; Bendlin, K.A.; Sayles, H.; Meza, J.; Russell, C.L.; Mikuls, T.R. Allopurinol Medication Adherence as a Mediator of Optimal Outcomes in Gout Management. J. Clin. Rheumatol. 2017, 23, 317–323. [Google Scholar] [CrossRef]
- Corbett, E.J.M.; Pentony, P.; McGill, N.W. Achieving serum urate targets in gout: An audit in a gout-oriented rheumatology practice. Int. J. Rheum. Dis. 2017, 20, 894–897. [Google Scholar] [CrossRef]
- Yin, R.; Li, L.; Zhang, G.; Cui, Y.; Zhang, L.; Zhang, Q.; Fu, T.; Cao, H.; Li, L.; Gu, Z. Rate of adherence to urate-lowering therapy among patients with gout: A systematic review and meta-analysis. BMJ Open 2018, 8, e017542. [Google Scholar] [CrossRef]
- Scheepers, L.; Burden, A.M.; Arts, I.C.W.; Spaetgens, B.; Souverein, P.; de Vries, F.; Boonen, A. Medication adherence among gout patients initiated allopurinol: A retrospective cohort study in the Clinical Practice Research Datalink (CPRD). Rheumatology 2018, 57, 1641–1650. [Google Scholar] [CrossRef]
- Stamp, L.K.; Merriman, T.R.; Barclay, M.L.; Singh, J.A.; Roberts, R.L.; Wright, D.F.; Dalbeth, N. Impaired response or insufficient dosage? Examining the potential causes of “inadequate response” to allopurinol in the treatment of gout. Semin. Arthritis Rheum. 2014, 44, 170–174. [Google Scholar] [CrossRef]
- Stamp, L.K.; Day, R.O.; Yun, J. Allopurinol hypersensitivity: Investigating the cause and minimizing the risk. Nat. Rev. Rheumatol. 2016, 12, 235–242. [Google Scholar] [CrossRef]
- Stamp, L.K.; Chapman, P.T.; Barclay, M.L.; Horne, A.; Frampton, C.; Tan, P.; Drake, J.; Dalbeth, N. A randomised controlled trial of the efficacy and safety of allopurinol dose escalation to achieve target serum urate in people with gout. Ann. Rheum. Dis. 2017, 76, 1522–1528. [Google Scholar] [CrossRef]
- Stamp, L.K.; Taylor, W.J.; Jones, P.B.; Dockerty, J.L.; Drake, J.; Frampton, C.; Dalbeth, N. Starting dose is a risk factor for allopurinol hypersensitivity syndrome: A proposed safe starting dose of allopurinol. Arthritis Rheum. 2012, 64, 2529–2536. [Google Scholar] [CrossRef]
- Jennings, C.G.; Mackenzie, I.S.; Flynn, R.; Ford, I.; Nuki, G.; De Caterina, R.; Riches, P.L.; Ralston, S.H.; MacDonald, T.M.; FAST Study Group. Up-titration of allopurinol in patients with gout. Semin. Arthritis Rheum. 2014, 44, 25–30. [Google Scholar] [CrossRef]
- Becker, M.A.; Fitz-Patrick, D.; Choi, H.K.; Dalbeth, N.; Storgard, C.; Cravets, M.; Baumgartner, S. An open-label, 6-month study of allopurinol safety in gout: The LASSO study. Semin. Arthritis Rheum. 2015, 45, 174–183. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.W.; Kwak, S.G.; Park, S.H. Prescription pattern of urate-lowering therapy in Korean gout patients: Data from the national health claims database. Korean J. Intern. Med. 2018, 33, 228–229. [Google Scholar] [CrossRef]
- Chou, H.W.; Chiu, H.T.; Tsai, C.W.; Ting, I.W.; Yeh, H.C.; Huang, H.C.; Kuo, C.C.; Group, C.K.R. Comparative effectiveness of allopurinol, febuxostat and benzbromarone on renal function in chronic kidney disease patients with hyperuricemia: A 13-year inception cohort study. Nephrol. Dial. Transplant. 2018, 33, 1620–1627. [Google Scholar] [CrossRef]
- Li, S.; Yang, H.; Guo, Y.; Wei, F.; Yang, X.; Li, D.; Li, M.; Xu, W.; Li, W.; Sun, L.; et al. Comparative efficacy and safety of urate-lowering therapy for the treatment of hyperuricemia: A systematic review and network meta-analysis. Sci. Rep. 2016, 6, 33082. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Allopurinol (n = 42) | Febuxostat (n = 145) | Benzbromarone (n = 57) | Overall (n = 244) | p Value |
|---|---|---|---|---|---|
| Male sex, number (%) | 39 (92.9) | 140 (96.6) | 57 (100.0) | 236 (96.7) | 0.113 |
| Age, years | 55.1 ± 15.8 | 49.5 ± 13.5 | 51.4 ± 14.5 | 50.9 ± 14.2 | 0.073 |
| Age of ≥65 years, number (%) | 12 (28.6) | 19 (13.1) | 12 (21.1) | 43 (17.6) | 0.051 |
| BMI *, kg/m2 | 25.6 ± 2.8 | 26.2 ± 2.9 | 26.9 ± 3.8 | 26.2 ± 3.1 | 0.202 |
| Serum urate, mg/dL | 7.5 ± 1.8 | 7.9 ± 2.2 | 8.3 ± 1.7 | 7.9 ± 2.0 | 0.140 |
| Serum creatinine, mg/dL | 1.13 ± 0.60 | 1.03 ± 0.23 | 1.19 ± 0.22 | 1.08 ± 0.33 | <0.001 |
| eGFR, mL/min/1.73 m2 | 75.69 ± 21.20 | 81.30 ± 19.14 | 67.57 ± 15.48 | 77.12 ± 19.50 | <0.001 |
| Comorbidity, number (%) | |||||
| Hypertension | 20 (47.6) | 55 (37.9) | 27 (47.4) | 102 (41.8) | 0.355 |
| Diabetes mellitus | 2 (4.8) | 11 (7.6) | 4 (7.0) | 17 (7.0) | 0.939 |
| Ischemic heart disease | 2 (4.8) | 2 (1.4) | 0 (0) | 4 (1.6) | 0.179 |
| Valvular heart disease | 1 (2.4) | 2 (1.4) | 1 (1.8) | 4 (1.6) | 0.803 |
| Arrhythmia | 1 (2.4) | 2 (1.4) | 1 (1.8) | 4 (1.6) | 0.803 |
| Stroke | 5 (11.9) | 6 (4.1) | 2 (3.5) | 13 (5.3) | 0.129 |
| Epilepsy | 0 (0) | 1 (0.7) | 0 (0) | 1 (0.4) | 1.000 |
| Concomitant medication †, number (%) | |||||
| ACE inhibitors | 1 (2.7) | 0 (0) | 1 (2.0) | 2 (1.0) | 0.168 |
| Angiotensin receptor blockers | 6 (16.2) | 20 (16.3) | 9 (18.4) | 35 (16.7) | 0.966 |
| Beta-blockers | 4 (10.8) | 6 (4.9) | 3 (6.1) | 13 (6.2) | 0.410 |
| Calcium channel blockers | 4 (10.8) | 17 (13.8) | 8 (16.3) | 29 (13.9) | 0.788 |
| Diuretics | 2 (5.4) | 10 (8.1) | 6 (12.2) | 18 (8.6) | 0.545 |
| Median ULT duration, months (IQR) | 27.1 (15.2, 39.9) | 22.3 (16.6, 35.1) | 32.0 (22.5, 47.2) | 25.3 (17.5, 36.9) | 0.001 |
| Characteristics | Final Serum Urate ≥ 6 mg/dL (n = 53) | Final Serum Urate < 6 mg/dL (n = 191) | p Value |
|---|---|---|---|
| Male sex, number (%) | 52 (98.1) | 184 (96.3) | 1.000 |
| Age, years | 46.3 ± 14.8 | 52.2 ± 13.9 | 0.008 |
| BMI, kg/m2 | 26.7 ± 3.3 | 26.1 ± 3.0 | 0.342 |
| Serum urate, mg/dL | 8.2 ± 1.9 | 7.9 ± 2.0 | 0.270 |
| Serum creatinine, mg/dL | 1.12 ± 0.55 | 1.07 ± 0.23 | 0.341 |
| eGFR, mL/min/1.73 m2 | 79.72 ± 21.80 | 76.40 ± 18.81 | 0.274 |
| XOI users, number (%) | 40 (75.5) | 147 (77.0) | 0.855 |
| Median ULT duration, months (IQR) | 22.5 (16.0, 32.8) | 26.7 (18.2, 37.9) | 0.055 |
| Category | Number (%) | ΔeGFR during ULT | p Value | |
|---|---|---|---|---|
| Final Serum Urate ≥ 6 mg/dL | Final Serum Urate < 6 mg/dL | |||
| Normal (eGFR ≥90) | 65 (26.6) | −4.46 ± 9.71 | −1.36 ± 14.12 | 0.385 |
| Mild renal impairment (eGFR 60–89) | 130 (53.3) | 9.31 ± 18.89 | 5.69 ± 11.60 | 0.366 |
| Moderate renal impairment (eGFR 30–59) | 47 (19.3) | −0.35 ± 3.87 | 5.33 ± 11.64 | 0.019 |
| Total | 244 (100.0) | 2.68 ± 15.53 | 3.90 ± 12.53 | 0.554 |
| Variables | Univariable ModelOR (95% CI) | p Value | Multivariable ModelOR (95% CI) | p Value |
|---|---|---|---|---|
| Age: ≥65 years | 0.64 (0.33, 1.24) | 0.182 | 0.31 (0.13, 0.75) | 0.009 |
| BMI: ≥30 kg/m2 | 0.63 (0.24, 1.66) | 0.348 | ||
| Hypertension | 0.97 (0.58, 1.63) | 0.905 | ||
| Diabetes mellitus | 0.94 (0.35, 2.56) | 0.901 | ||
| Baseline renal function (reference: normal) | ||||
| eGFR: 60–89 mL/min/1.73 m2 | 2.14 (1.17, 3.94) | 0.014 | 2.39 (1.22, 4.68) | 0.012 |
| eGFR: 30–59 mL/min/1.73 m2 | 1.77 (0.82, 3.79) | 0.144 | 2.44 (0.96, 6.21) | 0.060 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, W.-J.; Song, J.S.; Choi, S.T. The Role of a “Treat-to-Target” Approach in the Long-Term Renal Outcomes of Patients with Gout. J. Clin. Med. 2019, 8, 1067. https://doi.org/10.3390/jcm8071067
Kim W-J, Song JS, Choi ST. The Role of a “Treat-to-Target” Approach in the Long-Term Renal Outcomes of Patients with Gout. Journal of Clinical Medicine. 2019; 8(7):1067. https://doi.org/10.3390/jcm8071067
Chicago/Turabian StyleKim, Woo-Joong, Jung Soo Song, and Sang Tae Choi. 2019. "The Role of a “Treat-to-Target” Approach in the Long-Term Renal Outcomes of Patients with Gout" Journal of Clinical Medicine 8, no. 7: 1067. https://doi.org/10.3390/jcm8071067