Association between Thyroid-Stimulating Hormone Level after Total Thyroidectomy and Hypercholesterolemia in Female Patients with Differentiated Thyroid Cancer: A Retrospective Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Data and Measurements
2.3. Statistical Analyses
3. Results
3.1. Demographics and Descriptive Statistics
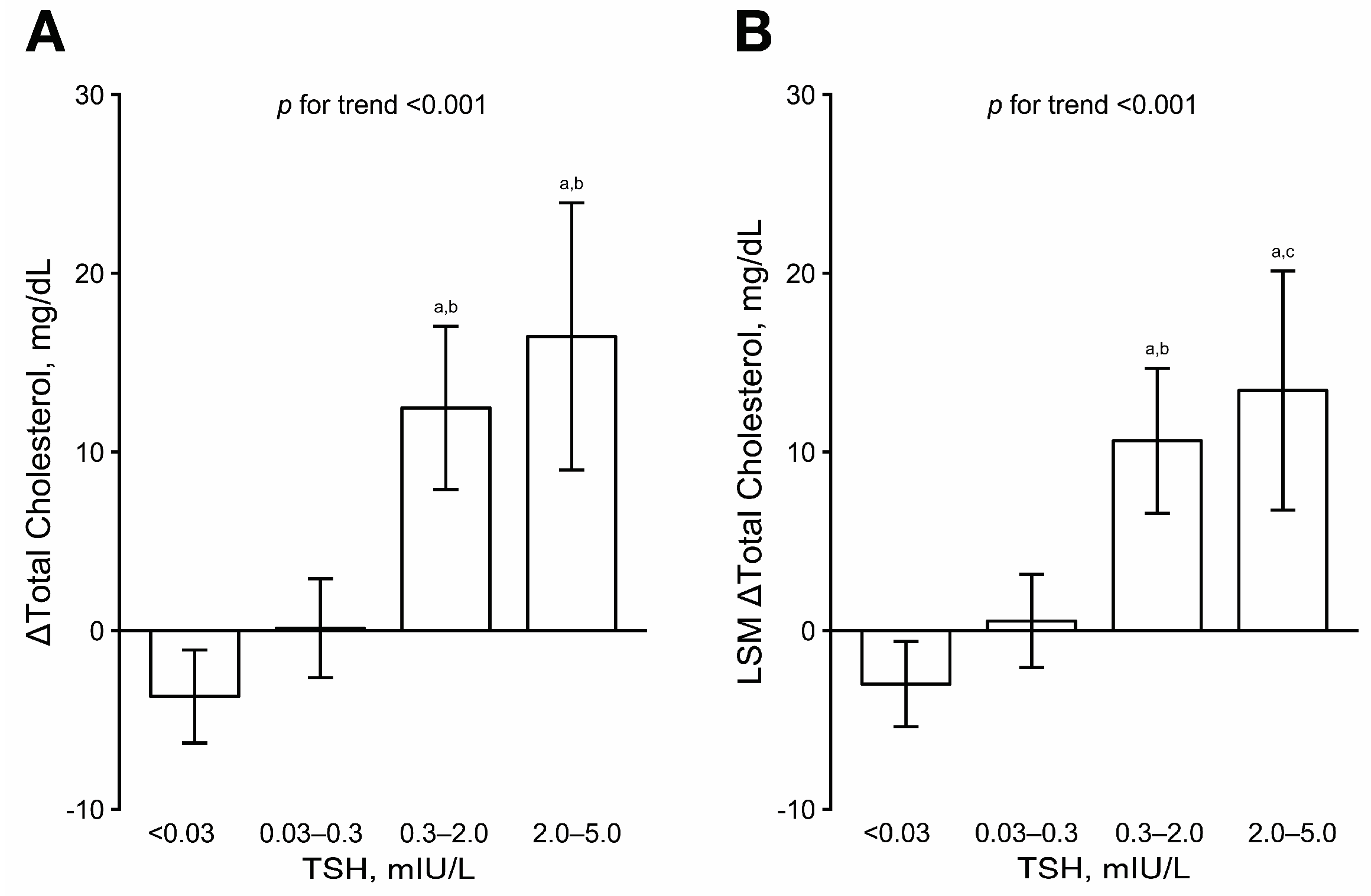
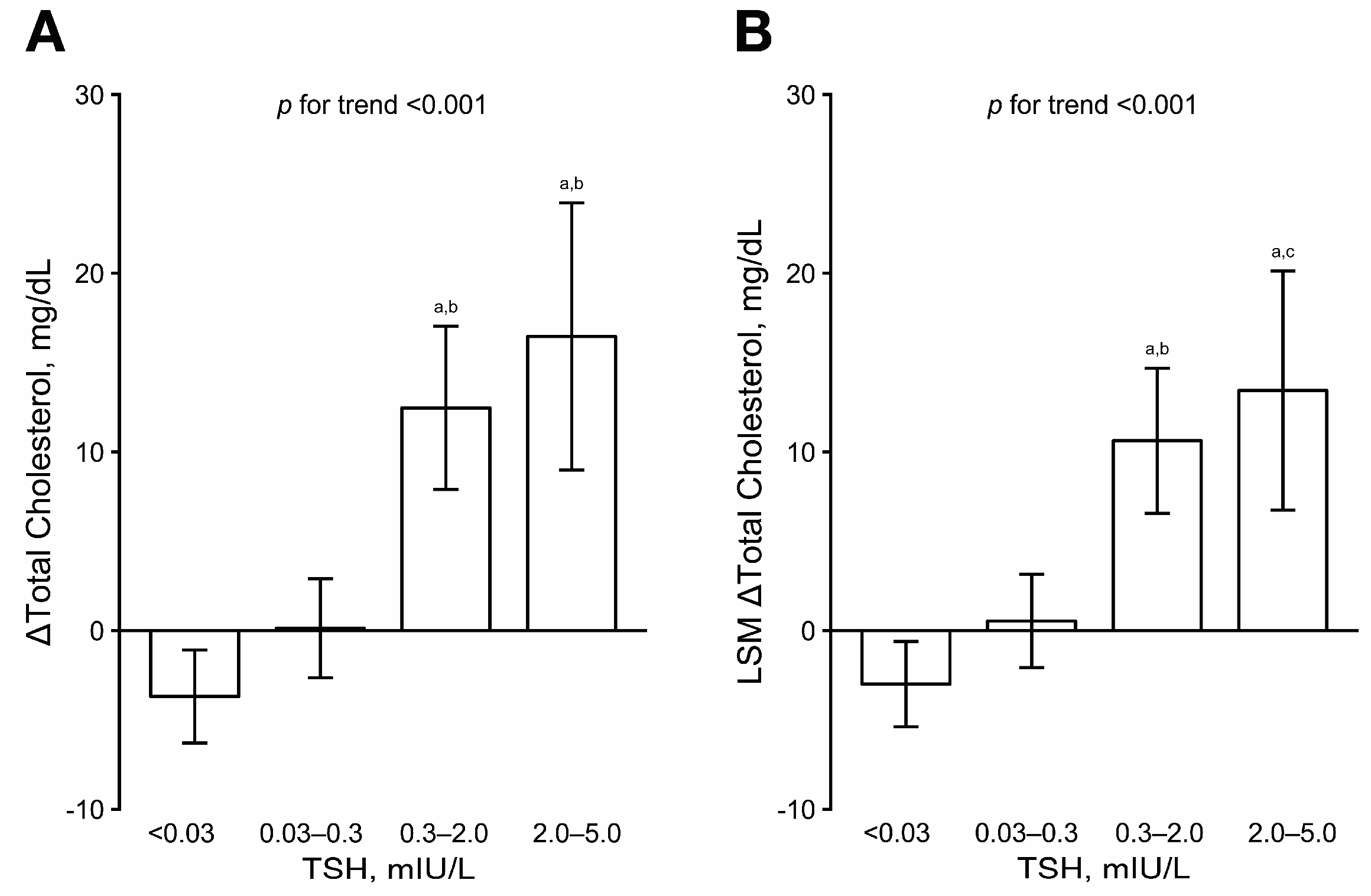
3.2. TSH and Total Cholesterol Level before and after Thyroidectomy
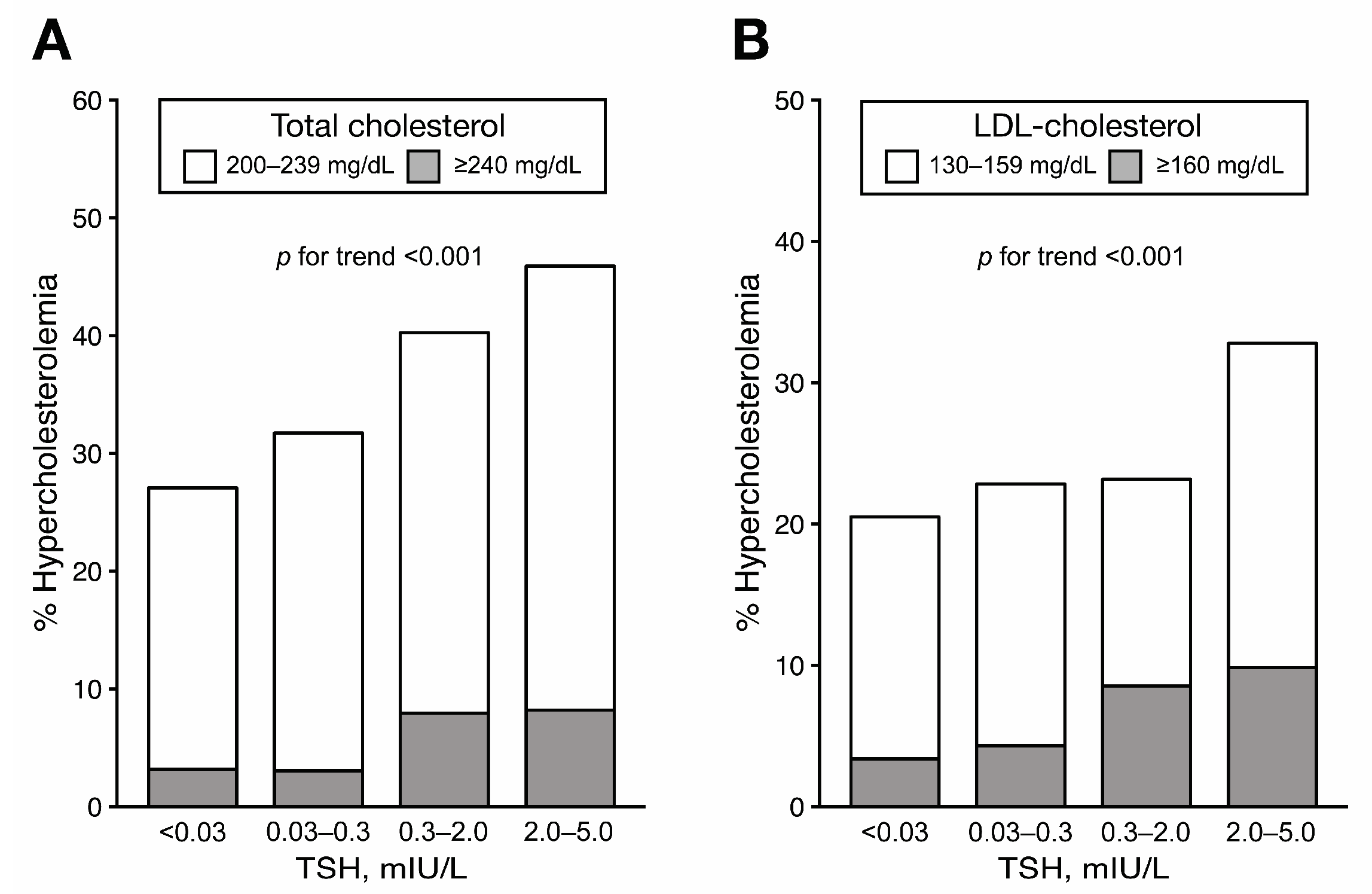
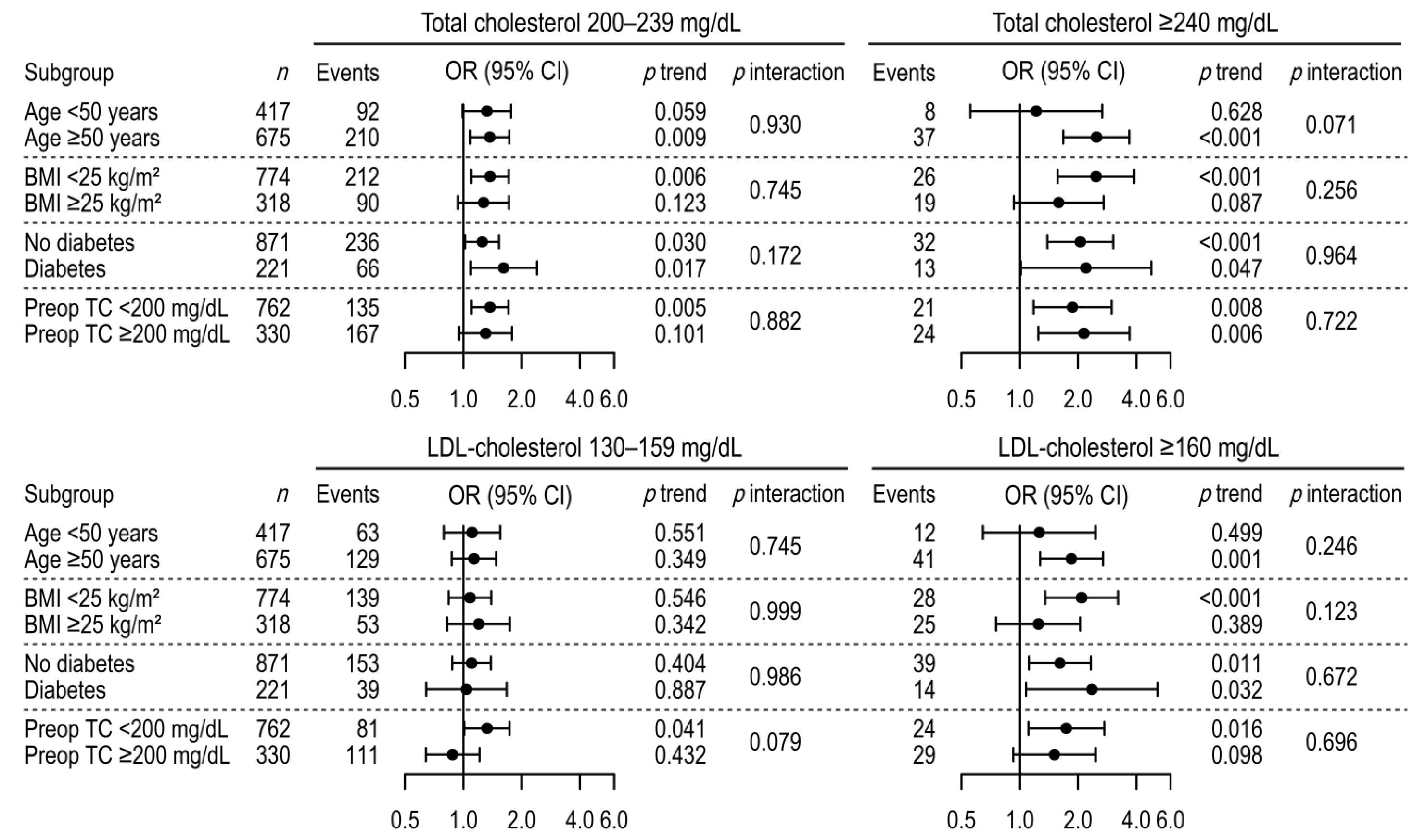
3.3. Association between TSH Level and Hypercholesterolemia after Thyroidectomy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- Fitzmaurice, C.; Dicker, D.; Pain, A.; Hamavid, H.; Moradi-Lakeh, M.; MacIntyre, M.F.; Allen, C.; Hansen, G.; Woodbrook, R.; Wolfe, C.; et al. The Global Burden of Cancer 2013. JAMA Oncol. 2015, 1, 505–527. [Google Scholar] [CrossRef] [PubMed]
- Biondi, B.; Cooper, D.S. Benefits of thyrotropin suppression versus the risks of adverse effects in differentiated thyroid cancer. Thyroid 2010, 20, 135–146. [Google Scholar] [CrossRef] [PubMed]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yi, K.H.; Lee, E.K.; Kang, H.-C.; Koh, Y.; Kim, S.W.; Kim, I.J.; Na, D.G.; Nam, K.-H.; Park, S.Y.; Park, J.W. 2016 Revised Korean thyroid association management guidelines for patients with thyroid nodules and thyroid cancer. Int. J. Thyroidol. 2016, 9, 59–126. [Google Scholar] [CrossRef]
- Peterson, S.J.; McAninch, E.A.; Bianco, A.C. Is a Normal TSH Synonymous With “Euthyroidism” in Levothyroxine Monotherapy? J. Clin. Endocrinol. Metab. 2016, 101, 4964–4973. [Google Scholar] [CrossRef] [PubMed]
- McAninch, E.A.; Rajan, K.B.; Miller, C.H.; Bianco, A.C. Systemic Thyroid Hormone Status during Levothyroxine Therapy in Hypothyroidism: A Systematic Review and Meta-Analysis. J. Clin. Endocrinol. Metab. 2018, 103, 4533–4542. [Google Scholar] [CrossRef] [PubMed]
- Ito, M.; Miyauchi, A.; Hisakado, M.; Yoshioka, W.; Ide, A.; Kudo, T.; Nishihara, E.; Kihara, M.; Ito, Y.; Kobayashi, K.; et al. Biochemical Markers Reflecting Thyroid Function in Athyreotic Patients on Levothyroxine Monotherapy. Thyroid 2017, 27, 484–490. [Google Scholar] [CrossRef] [Green Version]
- Ito, M.; Miyauchi, A.; Morita, S.; Kudo, T.; Nishihara, E.; Kihara, M.; Takamura, Y.; Ito, Y.; Kobayashi, K.; Miya, A.; et al. TSH-suppressive doses of levothyroxine are required to achieve preoperative native serum triiodothyronine levels in patients who have undergone total thyroidectomy. Eur. J. Endocrinol. 2012, 167, 373–378. [Google Scholar] [CrossRef] [Green Version]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar]
- 2015 Korean Guidelines for the Management of Dyslipidemia: Executive Summary (English Translation). Korean Circ. J. 2016, 46, 275–306. [CrossRef] [Green Version]
- National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 2002, 106, 3143–3421. [Google Scholar] [CrossRef]
- Baloch, Z.; Carayon, P.; Conte-Devolx, B.; Demers, L.M.; Feldt-Rasmussen, U.; Henry, J.F.; LiVosli, V.A.; Niccoli-Sire, P.; John, R.; Ruf, J.; et al. Laboratory medicine practice guidelines. Laboratory support for the diagnosis and monitoring of thyroid disease. Thyroid 2003, 13, 3–126. [Google Scholar] [CrossRef] [PubMed]
- Biondi, B. Persistent Dyslipidemia in Patients with Hypothyroidism: A Good Marker for Personalized Replacement Therapy? J. Clin. Endocrinol. Metab. 2019, 104, 624–627. [Google Scholar] [CrossRef] [PubMed]
- Hoermann, R.; Midgley, J.E.; Giacobino, A.; Eckl, W.A.; Wahl, H.G.; Dietrich, J.W.; Larisch, R. Homeostatic equilibria between free thyroid hormones and pituitary thyrotropin are modulated by various influences including age, body mass index and treatment. Clin. Endocrinol. 2014, 81, 907–915. [Google Scholar] [CrossRef] [PubMed]
- Gullo, D.; Latina, A.; Frasca, F.; Le Moli, R.; Pellegriti, G.; Vigneri, R. Levothyroxine monotherapy cannot guarantee euthyroidism in all athyreotic patients. PLoS ONE 2011, 6, e22552. [Google Scholar] [CrossRef]
- Pearce, E.N. Update in lipid alterations in subclinical hypothyroidism. J. Clin. Endocrinol. Metab. 2012, 97, 326–333. [Google Scholar] [CrossRef] [PubMed]
- Duntas, L.H.; Brenta, G. The effect of thyroid disorders on lipid levels and metabolism. Med. Clin. N. Am. 2012, 96, 269–281. [Google Scholar] [CrossRef]
- Biondi, B.; Wartofsky, L. Treatment with thyroid hormone. Endocr. Rev. 2014, 35, 433–512. [Google Scholar] [CrossRef]
- Ross, D.S.; Burch, H.B.; Cooper, D.S.; Greenlee, M.C.; Laurberg, P.; Maia, A.L.; Rivkees, S.A.; Samuels, M.; Sosa, J.A.; Stan, M.N.; et al. 2016 American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism and Other Causes of Thyrotoxicosis. Thyroid 2016, 26, 1343–1421. [Google Scholar] [CrossRef]
- Klein Hesselink, E.N.; Klein Hesselink, M.S.; de Bock, G.H.; Gansevoort, R.T.; Bakker, S.J.; Vredeveld, E.J.; van der Horst-Schrivers, A.N.; van der Horst, I.C.; Kamphuisen, P.W.; Plukker, J.T.; et al. Long-term cardiovascular mortality in patients with differentiated thyroid carcinoma: An observational study. J. Clin. Oncol. 2013, 31, 4046–4053. [Google Scholar] [CrossRef]
- Flynn, R.W.; Bonellie, S.R.; Jung, R.T.; MacDonald, T.M.; Morris, A.D.; Leese, G.P. Serum thyroid-stimulating hormone concentration and morbidity from cardiovascular disease and fractures in patients on long-term thyroxine therapy. J. Clin. Endocrinol. Metab. 2010, 95, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Shin, D.Y.; Kim, K.J.; Cho, Y.; Park, K.H.; Hwang, S.; Chung, W.Y.; Lee, E.J. Body Mass Index Is Associated with Hypercholesterolemia following Thyroid Hormone Withdrawal in Thyroidectomized Patients. Int. J. Endocrinol. 2014, 2014, 649016. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Meng, Z.; Tan, J.; Liu, M.; Jia, Q.; Zhang, G.; He, Y.; Zhang, Q.; Liu, L.; Song, K.; et al. Gender impact on the correlation between thyroid function and serum lipids in patients with differentiated thyroid cancer. Exp. Ther. Med. 2016, 12, 2873–2880. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sigal, G.A.; Tavoni, T.M.; Silva, B.M.O.; Kalil Filho, R.; Brandao, L.G.; Maranhao, R.C. Effects of Short-Term Hypothyroidism on the Lipid Transfer to High-Density Lipoprotein and Other Parameters Related to Lipoprotein Metabolism in Patients Submitted to Thyroidectomy for Thyroid Cancer. Thyroid 2019, 29, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Papadakis, G.; Kalaitzidou, S.; Triantafillou, E.; Drosou, A.; Kakava, K.; Dogkas, N.; Pappa, T.; Kaltzidou, V.; Tertipi, A.; Villiotou, V.; et al. Biochemical Effects of Levothyroxine Withdrawal in Patients with Differentiated Thyroid Cancer. Anticancer Res. 2015, 35, 6933–6940. [Google Scholar] [CrossRef] [PubMed]
- Pontius, L.N.; Oyekunle, T.O.; Thomas, S.M.; Stang, M.T.; Scheri, R.P.; Roman, S.A.; Sosa, J.A. Projecting Survival in Papillary Thyroid Cancer: A Comparison of the Seventh and Eighth Editions of the American Joint Commission on Cancer/Union for International Cancer Control Staging Systems in Two Contemporary National Patient Cohorts. Thyroid 2017, 27, 1408–1416. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.M.; Danaei, G.; Pelizzari, P.M.; Lin, J.K.; Cowan, M.J.; Stevens, G.A.; Farzadfar, F.; Khang, Y.H.; Lu, Y.; Riley, L.M.; et al. The age associations of blood pressure, cholesterol, and glucose: Analysis of health examination surveys from international populations. Circulation 2012, 125, 2204–2211. [Google Scholar] [CrossRef]
- Andersson, C.; Lyass, A.; Vasan, R.S.; Massaro, J.M.; D’Agostino, R.B., Sr.; Robins, S.J. Long-term risk of cardiovascular events across a spectrum of adverse major plasma lipid combinations in the Framingham Heart Study. Am. Heart J. 2014, 168, 878–883.e1. [Google Scholar] [CrossRef]
- Oh, H.S.; Kwon, H.; Ahn, J.; Song, E.; Park, S.; Kim, M.; Han, M.; Jeon, M.J.; Kim, W.G.; Kim, W.B.; et al. Association Between Thyroid Dysfunction and Lipid Profiles Differs According to Age and Sex: Results from the Korean National Health and Nutrition Examination Survey. Thyroid 2018, 28, 849–856. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Variables | TSH, mIU/L | p Value | |||
|---|---|---|---|---|---|
| <0.03 | 0.03–0.3 | 0.3–2 | 2–5 | ||
| (n = 473) | (n = 394) | (n = 164) | (n = 61) | ||
| Age at surgery, years | 50.6 ± 10 | 51.2 ± 11.2 | 47.6 ± 12 | 47.6 ± 12 | 0.001 |
| Age at follow-up, years | 52.7 ± 10.1 | 53.4 ± 11.2 | 50 ± 11.9 | 50.3 ± 11.8 | 0.002 |
| Follow-up, years | 2.2 ± 0.9 | 2.2 ± 0.9 | 2.3 ± 0.9 | 2.7 ± 1 | <0.001 |
| History of hypertension | 145 (30.7%) | 161 (40.9%) | 48 (29.3%) | 21 (34.4%) | 0.007 |
| History of diabetes | 87 (18.4%) | 79 (20.1%) | 32 (19.5%) | 10 (16.4%) | 0.876 |
| Ever smokers | 26 (5.5%) | 22 (5.6%) | 11 (6.7%) | 5 (8.2%) | 0.805 |
| Preoperative TSH * | 1.89 ± 1.02 | 1.99 ± 1.01 | 1.9 ± 0.99 | 1.79 ± 1.08 | 0.385 |
| Preoperative cholesterol | 184.83 ± 28.49 | 184.34 ± 27.82 | 178.74 ± 27.6 | 177.23 ± 27.3 | 0.028 |
| Body mass index, kg/m² | 23.44 ± 3.07 | 23.98 ± 3.49 | 23.82 ± 3.67 | 24.03 ± 3.57 | 0.101 |
| Systolic blood pressure, mmHg | 124.73 ± 14.99 | 125.08 ± 15.46 | 123.66 ± 16.05 | 122.07 ± 13.3 | 0.438 |
| Free T4, ng/dL † | 1.55 ± 0.26 | 1.44 ± 0.32 | 1.31 ± 0.23 | 1.18 ± 0.23 | <0.001 |
| TSH, mIU/L | 0.02 ± 0 | 0.09 ± 0.06 | 0.84 ± 0.45 | 3.16 ± 0.88 | <0.001 |
| Glucose, mg/dL | 98.92 ± 19.58 | 101.29 ± 24.18 | 100.13 ± 20.71 | 94.7 ± 13.03 | 0.099 |
| Total cholesterol, mg/dL | 181.14 ± 30.79 | 184.47 ± 30.57 | 191.2 ± 32.44 | 193.69 ± 33.65 | <0.001 |
| Total cholesterol, mg/dL | 0.001 | ||||
| <200 | 345 (72.9%) | 269 (68.3%) | 98 (59.8%) | 33 (54.1%) | |
| 200–239 | 113 (23.9%) | 113 (28.7%) | 53 (32.3%) | 23 (37.7%) | |
| ≥240 | 15 (3.2%) | 12 (3.1%) | 13 (7.9%) | 5 (8.2%) | |
| ∆Total cholesterol, mg/dL | −3.69 ± 28.85 | 0.13 ± 28.09 | 12.46 ± 29.84 | 16.46 ± 29.78 | <0.001 |
| Triglyceride, mg/dL | 110.5 ± 56.54 | 114.8 ± 60.05 | 110.1 ± 61.73 | 132.18 ± 70.88 | 0.048 |
| HDL-cholesterol, mg/dL | 51.7 ± 11.72 | 51.2 ± 11.74 | 53.92 ± 11.24 | 51.49 ± 9.55 | 0.084 |
| LDL-cholesterol, mg/dL | 107.34 ± 28.4 | 110.32 ± 28.12 | 115.26 ± 29.44 | 115.76 ± 31.14 | 0.007 |
| LDL-cholesterol, mg/dL | 0.04 | ||||
| <130 | 376 (79.5%) | 304 (77.2%) | 126 (76.8%) | 41 (67.2%) | |
| 130–159 | 81 (17.1%) | 73 (18.5%) | 24 (14.6%) | 14 (23%) | |
| ≥160 | 16 (3.4%) | 17 (4.3%) | 14 (8.5%) | 6 (9.8%) | |
| Model | n | β (SE) | p Value |
|---|---|---|---|
| Model 1 | 1092 | 6.45 (1.11) | <0.001 |
| Model 2 | 1092 | 5.15 (1.03) | <0.001 |
| Model 3 | 1092 | 5.15 (1.03) | <0.001 |
| Model | TSH, mIU/L | n | Total Cholesterol Level 200–239 mg/dL | Total Cholesterol Level ≥240 mg/dL | ||||||
| Events | OR (95% CI) | p Value | p for Trend | Events | OR (95% CI) | p Value | p for Trend | |||
| Model 1 | <0.03 | 473 | 113 | 0.78 (0.57–1.06) | 0.111 | 15 | 0.97 (0.45–2.12) | 0.948 | ||
| 0.03–0.3 | 394 | 113 | 1 (reference) | 12 | 1 (reference) | |||||
| 0.3–2 | 164 | 53 | 1.29 (0.86–1.92) | 0.216 | 13 | 2.97 (1.31–6.74) | 0.009 | |||
| 2–5 | 61 | 23 | 1.66 (0.93–2.95) | 0.085 | 0.102 | 5 | 3.4 (1.13–10.25) | 0.03 | 0.003 | |
| Model 2 | <0.03 | 473 | 113 | 0.73 (0.52–1.02) | 0.064 | 15 | 0.93 (0.42–2.07) | 0.854 | ||
| 0.03–0.3 | 394 | 113 | 1 (reference) | 12 | 1 (reference) | |||||
| 0.3–2 | 164 | 53 | 1.84 (1.18–2.87) | 0.008 | 13 | 4.9 (2.05–11.72) | <0.001 | |||
| 2–5 | 61 | 23 | 2.61 (1.37–4.98) | 0.004 | 0.002 | 5 | 6.21 (1.89–20.34) | 0.003 | <0.001 | |
| Model 3 | <0.03 | 473 | 113 | 0.74 (0.52–1.03) | 0.078 | 15 | 1.04 (0.46–2.32) | 0.930 | ||
| 0.03–0.3 | 394 | 113 | 1 (reference) | 12 | 1 (reference) | |||||
| 0.3–2 | 164 | 53 | 1.86 (1.19–2.92) | 0.007 | 13 | 5.08 (2.14–12.06) | <0.001 | |||
| 2–5 | 61 | 23 | 2.85 (1.47–5.53) | 0.002 | 0.001 | 5 | 6.95 (2.13–22.72) | 0.001 | <0.001 | |
| Model | TSH, mIU/L | n | LDL-Cholesterol Level 130–159 mg/dL | LDL-Cholesterol Level ≥160 mg/dL | ||||||
| Events | OR (95% CI) | p Value | p for Trend | Events | OR (95% CI) | p Value | p for Trend | |||
| Model 1 | <0.03 | 473 | 81 | 0.9 (0.63–1.27) | 0.544 | 16 | 0.76 (0.38–1.53) | 0.444 | ||
| 0.03–0.3 | 394 | 73 | 1 (reference) | 17 | 1 (reference) | |||||
| 0.3–2 | 164 | 24 | 0.79 (0.48–1.32) | 0.369 | 14 | 1.99 (0.95–4.15) | 0.068 | |||
| 2–5 | 61 | 14 | 1.42 (0.74–2.75) | 0.295 | 0.953 | 6 | 2.62 (0.98–7.02) | 0.056 | 0.02 | |
| Model 2 | <0.03 | 473 | 81 | 0.84 (0.58–1.23) | 0.377 | 16 | 0.73 (0.36–1.5) | 0.396 | ||
| 0.03–0.3 | 394 | 73 | 1 (reference) | 17 | 1 (reference) | |||||
| 0.3–2 | 164 | 24 | 0.99 (0.58–1.7) | 0.972 | 14 | 2.66 (1.22–5.78) | 0.014 | |||
| 2–5 | 61 | 14 | 2.04 (0.99–4.18) | 0.053 | 0.306 | 6 | 3.9 (1.36–11.19) | 0.012 | 0.003 | |
| Model 3 | <0.03 | 473 | 81 | 0.84 (0.57–1.22) | 0.357 | 16 | 0.85 (0.41–1.78) | 0.668 | ||
| 0.03–0.3 | 394 | 73 | 1 (reference) | 17 | 1 (reference) | |||||
| 0.3–2 | 164 | 24 | 1 (0.58–1.71) | 0.991 | 14 | 2.76 (1.24–6.12) | 0.012 | |||
| 2–5 | 61 | 14 | 2.08 (1.01–4.31) | 0.048 | 0.298 | 6 | 4.17 (1.41–12.34) | 0.01 | 0.002 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, Y.K.; Lee, H.; Han, S.; Jung, H.; Shin, D.Y.; Nam, K.-H.; Chung, W.Y.; Lee, E.J. Association between Thyroid-Stimulating Hormone Level after Total Thyroidectomy and Hypercholesterolemia in Female Patients with Differentiated Thyroid Cancer: A Retrospective Study. J. Clin. Med. 2019, 8, 1106. https://doi.org/10.3390/jcm8081106
Lee YK, Lee H, Han S, Jung H, Shin DY, Nam K-H, Chung WY, Lee EJ. Association between Thyroid-Stimulating Hormone Level after Total Thyroidectomy and Hypercholesterolemia in Female Patients with Differentiated Thyroid Cancer: A Retrospective Study. Journal of Clinical Medicine. 2019; 8(8):1106. https://doi.org/10.3390/jcm8081106
Chicago/Turabian StyleLee, Young Ki, Hokyou Lee, Seunghee Han, Hyein Jung, Dong Yeob Shin, Kee-Hyun Nam, Woong Youn Chung, and Eun Jig Lee. 2019. "Association between Thyroid-Stimulating Hormone Level after Total Thyroidectomy and Hypercholesterolemia in Female Patients with Differentiated Thyroid Cancer: A Retrospective Study" Journal of Clinical Medicine 8, no. 8: 1106. https://doi.org/10.3390/jcm8081106