Lymphadenectomy for Upper Tract Urothelial Carcinoma: A Systematic Review


Abstract
:1. Introduction
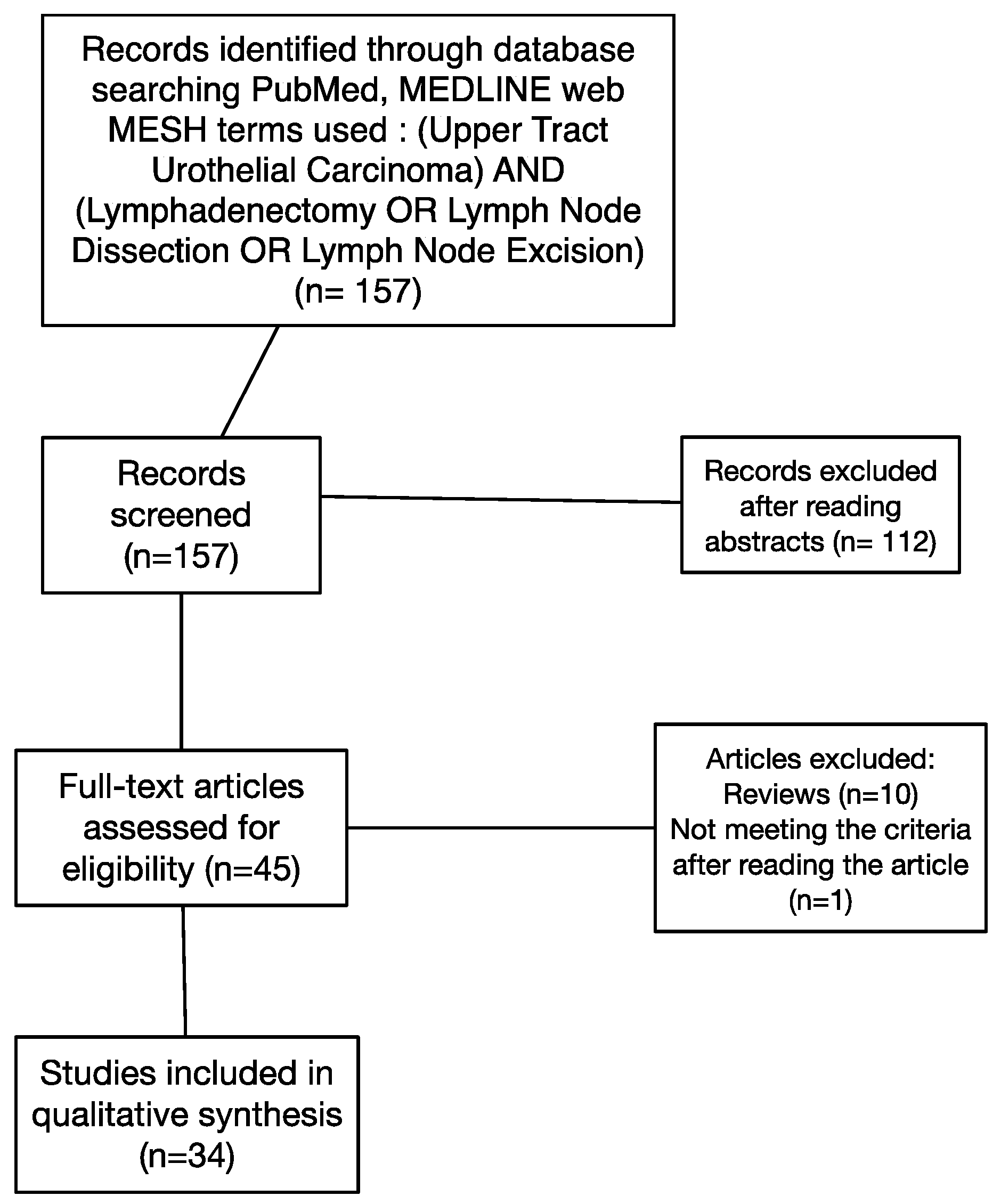
2. Materials and Methods
3. Results—Evidence Synthesis
3.1. Indication of Lymph Nodes Dissection (LND) in the Surgical Management of UTUC
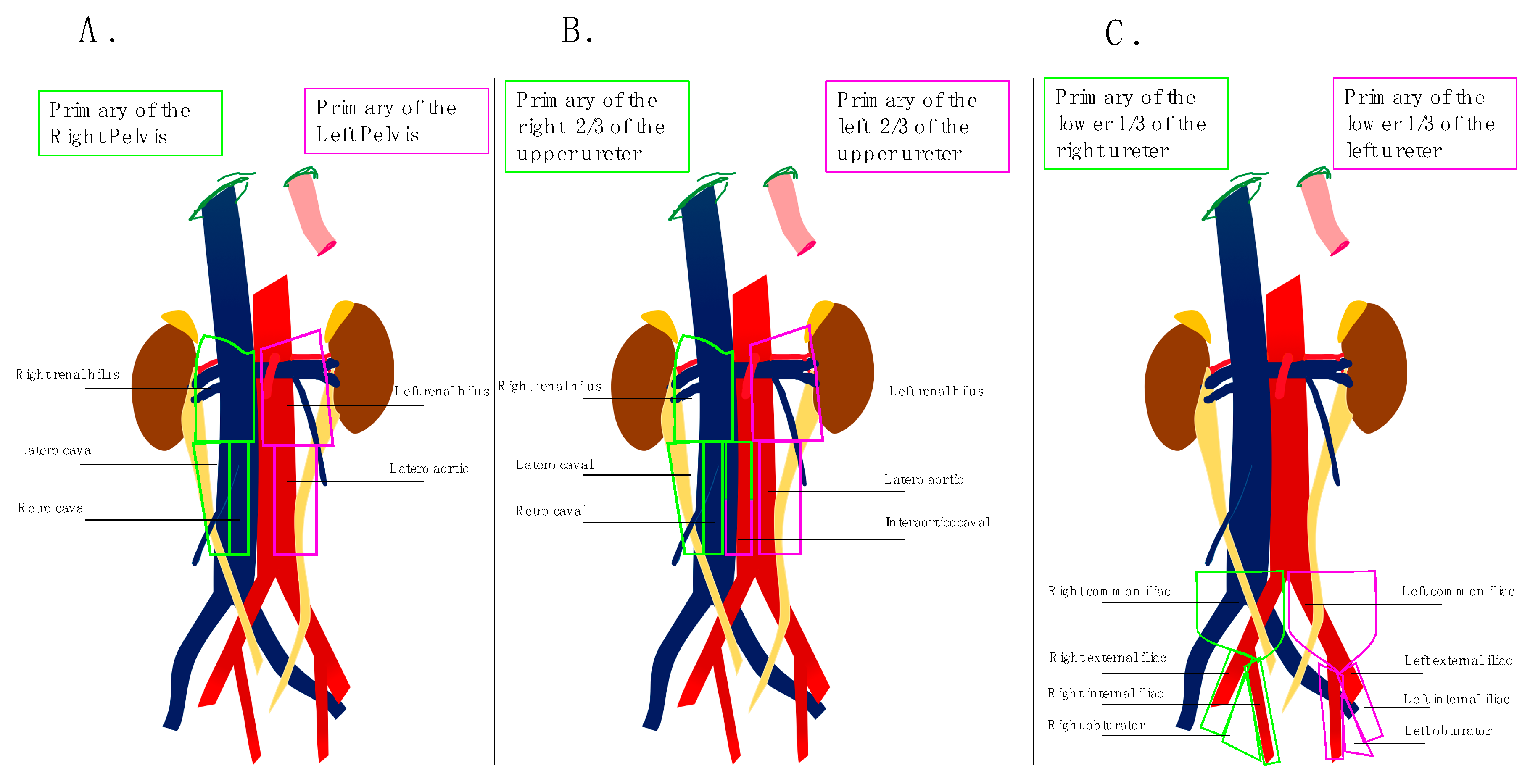
3.2. Definition of Anatomical Templates
3.3. Staging Role of Lymph Node Dissection
3.4. Therapeutic Role of Lymph Node Dissection
3.5. Number of Lymph Nodes Needed to be Removed
3.6. Role of Lymph Node Density
3.7. Impact of Surgical Approach on Lymph Node Dissection
3.8. Safety of Lymph Node Dissection
4. Key Concepts
- −
- Lymph node dissection performance tends to increase;
- −
- Lymph node dissection is usually performed for high risk UTUC;
- −
- Lymph node dissection might benefit for ≥T3 and high-grade patients both in cN0 and cN+ patients;
- −
- Lymph node dissection should follow a strict anatomical template depending on the location of primitive tumor;
- −
- Performing LND is safe and does not increase surgical complications;
- −
- Surgical approach does not seem to have major influence on the LND performance.;
- −
- LND might improve staging;
- −
- LND should remove eight lymphnodes;
- −
- Lymph node density might be a more precise index to predict outcome than lymph node count.
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2016. CA Cancer J. Clin. 2016, 66, 7–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zigeuner, R.; Pummer, K. Urothelial Carcinoma of the Upper Urinary Tract: Surgical Approach and Prognostic Factors. Eur. Urol. 2008, 53, 720–731. [Google Scholar] [CrossRef] [PubMed]
- Lughezzani, G.; Burger, M.; Margulis, V.; Matin, S.F.; Novara, G.; Roupret, M.; Shariat, S.F.; Wood, C.G.; Zigeuner, R. Prognostic Factors in Upper Urinary Tract Urothelial Carcinomas: A Comprehensive Review of the Current Literature. Eur. Urol. 2012, 62, 100–114. [Google Scholar] [CrossRef] [PubMed]
- Rouprêt, M.; Babjuk, M.; Compérat, E.; Zigeuner, R.; Sylvester, R.J.; Burger, M.; Cowan, N.C.; Gontero, P.; Van Rhijn, B.W.G.; Mostafid, A.H.; et al. European Association of Urology Guidelines on Upper Urinary Tract Urothelial Carcinoma: 2017 Update. Eur. Urol. 2018, 73, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Skinner, D.G. Technique of nephroureterectomy with regional lymph node dissection. Urol. Clin. N. Am. 1978, 5, 252–260. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, T.P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Rajput, M.Z.; Kamat, A.M.; Clavell-Hernandez, J.; Siefker-Radtke, A.O.; Grossman, H.B.; Dinney, C.P.N.; Matin, S.F. Perioperative outcomes of laparoscopic radical nephroureterectomy and regional lymphadenectomy in patients with upper urinary tract urothelial carcinoma after neoadjuvant chemotherapy. Urology 2011, 78, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Matin, S.F.; Margulis, V.; Kamat, A.; Wood, C.G.; Grossman, H.B.; Brown, G.A.; Dinney, C.P.N.; Millikan, R.; Siefker-Radtke, A.O. Incidence of downstaging and complete remission after neoadjuvant chemotherapy for high-risk upper tract transitional cell carcinoma. Cancer 2010, 116, 3127–3134. [Google Scholar] [CrossRef]
- Roscigno, M.; Shariat, S.F.; Margulis, V.; Karakiewicz, P.; Remzi, M.; Kikuchi, E.; Zigeuner, R.; Weizer, A.; Sagalowsky, A.; Bensalah, K.; et al. The extent of lymphadenectomy seems to be associated with better survival in patients with nonmetastatic upper-tract urothelial carcinoma: How many lymph nodes should be removed? Eur. Urol. 2009, 56, 512–518. [Google Scholar] [CrossRef]
- Secin, F.P.; Koppie, T.M.; Salamanca, J.I.M.; Bokhari, S.; Raj, G.V.; Olgac, S.; Serio, A.; Vickers, A.; Bochner, B.H. Evaluation of regional lymph node dissection in patients with upper urinary tract urothelial cancer. Int. J. Urol. 2007, 14, 26–32. [Google Scholar] [CrossRef]
- Rao, S.R.; Correa, J.J.; Sexton, W.J.; Pow-Sang, J.M.; Dickinson, S.I.; Lin, H.Y.; Spiess, P.E. Prospective clinical trial of the feasibility and safety of modified retroperitoneal lymph node dissection at time of nephroureterectomy for upper tract urothelial carcinoma. BJU Int. 2012, 110, E475–E480. [Google Scholar] [CrossRef] [PubMed]
- Furuse, H.; Matsushita, Y.; Yajima, T.; Kato, T.; Suzuki, T.; Matsumoto, R.; Motoyama, D.; Sugiyama, T.; Otsuka, A.; Ozono, S. Systematic regional lymph node dissection for upper tract urothelial carcinoma improves patient survival. Jpn. J. Clin. Oncol. 2017, 47, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Chappidi, M.R.; Kates, M.; Johnson, M.H.; Hahn, N.M.; Bivalacqua, T.J.; Pierorazio, P.M. Lymph node yield and tumor location in patients with upper tract urothelial carcinoma undergoing nephroureterectomy affects survival: A U.S. population-based analysis (2004–2012). Urol. Oncol. 2016, 34, 531.e15–531.e24. [Google Scholar] [CrossRef] [PubMed]
- Akaza, H.; Koiso, K.; Niijima, T. Clinical evaluation of urothelial tumors of the renal pelvis and ureter based on a new classification system. Cancer 1987, 59, 1369–1375. [Google Scholar] [CrossRef]
- Komatsu, H.; Tanabe, N.; Kubodera, S.; Maezawa, H.; Ueno, A. The role of lymphadenectomy in the treatment of transitional cell carcinoma of the upper urinary tract. J. Urol. 1997, 157, 1622–1624. [Google Scholar] [CrossRef]
- Miyake, H.; Hara, I.; Gohji, K.; Arakawa, S.; Kamidono, S. The significance of lymphadenectomy in transitional cell carcinoma of the upper urinary tract. Br. J. Urol. 1998, 82, 494–498. [Google Scholar] [CrossRef] [PubMed]
- Kondo, T.; Nakazawa, H.; Ito, F.; Hashimoto, Y.; Toma, H.; Tanabe, K. Primary site and incidence of lymph node metastases in urothelial carcinoma of upper urinary tract. Urology 2007, 69, 265–269. [Google Scholar] [CrossRef]
- Brausi, M.A.; Gavioli, M.; De Luca, G.; Verrini, G.; Peracchia, G.; Simonini, G.; Viola, M. Retroperitoneal lymph node dissection (RPLD) in conjunction with nephroureterectomy in the treatment of infiltrative transitional cell carcinoma (TCC) of the upper urinary tract: Impact on survival. Eur. Urol. 2007, 52, 1414–1418. [Google Scholar] [CrossRef] [PubMed]
- Abe, T.; Takada, N.; Matsumoto, R.; Osawa, T.; Sazawa, A.; Maruyama, S.; Tsuchiya, K.; Harabayashi, T.; Minami, K.; Nagamori, S.; et al. Outcome of regional lymphadenectomy in accordance with primary tumor location on laparoscopic nephroureterectomy for urothelial carcinoma of the upper urinary tract: A prospective study. J. Endourol. 2015, 29, 304–309. [Google Scholar] [CrossRef] [PubMed]
- Melquist, J.J.; Redrow, G.; Delacroix, S.; Park, A.; Faria, E.E.; Karam, J.A.; Matin, S.F. Comparison of Single-docking Robotic-assisted and Traditional Laparoscopy for Retroperitoneal Lymph Node Dissection during Nephroureterectomy with Bladder Cuff Excision for Upper-Tract Urothelial Carcinoma. Urology 2016, 87, 216–223. [Google Scholar] [CrossRef] [PubMed]
- Kondo, T.; Nakazawa, H.; Ito, F.; Hashimoto, Y.; Toma, H.; Tanabe, K. Impact of the extent of regional lymphadenectomy on the survival of patients with urothelial carcinoma of the upper urinary tract. J. Urol. 2007, 178, 1212–1217. [Google Scholar] [CrossRef] [PubMed]
- Kondo, T.; Tanabe, K. Role of lymphadenectomy in the management of urothelial carcinoma of the bladder and the upper urinary tract. Int. J. Urol. 2012, 19, 710–721. [Google Scholar] [CrossRef] [PubMed]
- Assouad, J.; Riquet, M.; Foucault, C.; Hidden, G.; Delmas, V. Renal lymphatic drainage and thoracic duct connections: Implications for cancer spread. Lymphology 2006, 39, 26–32. [Google Scholar] [PubMed]
- Roscigno, M.; Shariat, S.F.; Margulis, V.; Karakiewicz, P.; Remzi, M.; Kikuchi, E.; Langner, C.; Lotan, Y.; Weizer, A.; Bensalah, K.; et al. Impact of lymph node dissection on cancer specific survival in patients with upper tract urothelial carcinoma treated with radical nephroureterectomy. J. Urol. 2009, 181, 2482–2489. [Google Scholar] [CrossRef] [PubMed]
- Brown, G.A.; Busby, J.E.; Wood, C.G.; Pisters, L.L.; Dinney, C.P.N.; Swanson, D.A.; Grossman, H.B.; Pettaway, C.A.; Munsell, M.F.; Kamat, A.M.; et al. Nephroureterectomy for treating upper urinary tract transitional cell carcinoma: Time to change the treatment paradigm? BJU Int. 2006, 98, 1176–1180. [Google Scholar] [CrossRef] [PubMed]
- Novara, G.; Matsumoto, K.; Kassouf, W.; Walton, T.J.; Fritsche, H.M.; Bastian, P.J.; Martínez-Salamanca, J.I.; Seitz, C.; Lemberger, R.J.; Burger, M.; et al. Prognostic role of lymphovascular invasion in patients with urothelial carcinoma of the upper urinary tract: An international validation study. Eur. Urol. 2010, 57, 1064–1071. [Google Scholar] [CrossRef] [PubMed]
- Cho, K.S.; Choi, H.M.; Koo, K.; Park, S.J.; Rha, K.H.; Choi, Y.D.; Chung, B.H.; Cho, N.H.; Yang, S.C.; Hong, S.J. Clinical significance of lymph node dissection in patients with muscle-invasive upper urinary tract transitional cell carcinoma treated with nephroureterectomy. J. Korean Med. Sci. 2009, 24, 674–678. [Google Scholar] [CrossRef]
- Lughezzani, G.; Jeldres, C.; Isbarn, H.; Shariat, S.F.; Sun, M.; Pharand, D.; Widmer, H.; Arjane, P.; Graefen, M.; Montorsi, F.; et al. A critical appraisal of the value of lymph node dissection at nephroureterectomy for upper tract urothelial carcinoma. Urology 2010, 75, 118–124. [Google Scholar] [CrossRef]
- Mason, R.J.; Kassouf, W.; Bell, D.G.; Lacombe, L.; Kapoor, A.; Jacobsen, N.; Fairey, A.; Izawa, J.; Black, P.; Tanguay, S.; et al. The contemporary role of lymph node dissection during nephroureterectomy in the management of upper urinary tract urothelial carcinoma: The Canadian experience. Urology 2012, 79, 840–845. [Google Scholar] [CrossRef]
- Burger, M.; Shariat, S.F.; Fritsche, H.M.; Martinez-Salamanca, J.I.; Matsumoto, K.; Chromecki, T.F.; Ficarra, V.; Kassouf, W.; Seitz, C.; Pycha, A.; et al. No overt influence of lymphadenectomy on cancer-specific survival in organ-confined versus locally advanced upper urinary tract urothelial carcinoma undergoing radical nephroureterectomy: A retrospective international, multi-institutional study. World J. Urol. 2011, 29, 465–472. [Google Scholar] [CrossRef]
- Yoo, S.; You, D.; Jeong, I.G.; Hong, B.; Hong, J.H.; Ahn, H.; Kim, C.S. Does lymph node dissection during nephroureterectomy affect oncological outcomes in upper tract urothelial carcinoma patients without suspicious lymph node metastasis on preoperative imaging studies? World J. Urol. 2017, 35, 665–673. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, M.; Matsumoto, K.; Sakaguchi, K.; Ishii, D.; Tabata, K.I.; Kurosawa, K.; Urakami, S.; Okaneya, T.; Iwamura, M. Effect of Lymphadenectomy during Radical Nephroureterectomy in Locally Advanced Upper Tract Urothelial Carcinoma. Clin. Genitourin. Cancer 2017, 15, 556–562. [Google Scholar] [CrossRef] [PubMed]
- Inokuchi, J.; Kuroiwa, K.; Kakehi, Y.; Sugimoto, M.; Tanigawa, T.; Fujimoto, H.; Gotoh, M.; Masumori, N.; Ogawa, O.; Eto, M.; et al. Role of lymph node dissection during radical nephroureterectomy for upper urinary tract urothelial cancer: Multi-institutional large retrospective study JCOG1110A. World J. Urol. 2017, 35, 1737–1744. [Google Scholar] [CrossRef] [PubMed]
- Kondo, T.; Hashimoto, Y.; Kobayashi, H.; Iizuka, J.; Nakazawa, H.; Ito, F.; Tanabe, K. Template-based lymphadenectomy in urothelial carcinoma of the upper urinary tract: Impact on patient survival. Int. J. Urol. 2010, 17, 848–854. [Google Scholar] [CrossRef]
- Capitanio, U.; Suardi, N.; Shariat, S.F.; Lotan, Y.; Palapattu, G.S.; Bastian, P.J.; Gupta, A.; Vazina, A.; Schoenberg, M.; Lerner, S.P.; et al. Assessing the minimum number of lymph nodes needed at radical cystectomy in patients with bladder cancer. BJU Int. 2009, 103, 1359–1362. [Google Scholar] [CrossRef]
- Roscigno, M.; Shariat, S.F.; Freschi, M.; Margulis, V.; Karakiewizc, P.; Suardi, N.; Remzi, M.; Zigeuner, R.; Bolenz, C.; Kikuchi, E.; et al. Assessment of the minimum number of lymph nodes needed to detect lymph node invasion at radical nephroureterectomy in patients with upper tract urothelial cancer. Urology 2009, 74, 1070–1074. [Google Scholar] [CrossRef]
- Roscigno, M.; Cozzarini, C.; Bertini, R.; Scattoni, V.; Freschi, M.; Da Pozzo, L.F.; Briganti, A.; Gallina, A.; Capitanio, U.; Colombo, R.; et al. Prognostic value of lymph node dissection in patients with muscle-invasive transitional cell carcinoma of the upper urinary tract. Eur. Urol. 2008, 53, 794–802. [Google Scholar] [CrossRef]
- Dorin, R.P.; Daneshmand, S.; Eisenberg, M.S.; Chandrasoma, S.; Cai, J.; Miranda, G.; Nichols, P.W.; Skinner, D.G.; Skinner, E.C. Lymph node dissection technique is more important than lymph node count in identifying nodal metastases in radical cystectomy patients: A comparative mapping study. Eur. Urol. 2011, 60, 946–952. [Google Scholar] [CrossRef]
- Xylinas, E.; Rink, M.; Margulis, V.; Faison, T.; Comploj, E.; Novara, G.; Raman, J.D.; Lotan, Y.; Guillonneau, B.; Weizer, A.; et al. Prediction of true nodal status in patients with pathological lymph node negative upper tract urothelial carcinoma at radical nephroureterectomy. J. Urol. 2013, 189, 468–473. [Google Scholar] [CrossRef]
- Xylinas, E.; Kluth, L.; Rieken, M.; Rouprêt, M.; Al Hussein Al Awamlh, B.; Clozel, T.; Sun, M.; Karakiewicz, P.I.; Gonen, M.; Shariat, S.F. External validation of the pathological nodal staging score in upper tract urothelial carcinoma: A population-based study. Urol. Oncol. 2017, 35, 33.e21–33.e26. [Google Scholar] [CrossRef]
- Bolenz, C.; Shariat, S.F.; Fernández, M.I.; Margulis, V.; Lotan, Y.; Karakiewicz, P.; Remzi, M.; Kikuchi, E.; Zigeuner, R.; Weizer, A.; et al. Risk stratification of patients with nodal involvement in upper tract urothelial carcinoma: Value of lymph-node density. BJU Int. 2009, 103, 302–306. [Google Scholar] [CrossRef] [PubMed]
- Pearce, S.M.; Pariser, J.J.; Patel, S.G.; Steinberg, G.D.; Shalhav, A.L.; Smith, N.D. The effect of surgical approach on performance of lymphadenectomy and perioperative morbidity for radical nephroureterectomy. Urol. Oncol. 2016, 34, 121.e15–121.e21. [Google Scholar] [CrossRef] [PubMed]
- Abe, T.; Kondo, T.; Harabayashi, T.; Takada, N.; Matsumoto, R.; Osawa, T.; Minami, K.; Nagamori, S.; Maruyama, S.; Murai, S.; et al. Comparative study of lymph node dissection, and oncological outcomes of laparoscopic and open radical nephroureterectomy for patients with urothelial carcinoma of the upper urinary tract undergoing regional lymph node dissection. Jpn. J. Clin. Oncol. 2018, 48, 1001–1011. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, J.F.; Packiam, V.T.; Boysen, W.R.; Johnson, S.C.; Smith, Z.L.; Smith, N.D.; Shalhav, A.L.; Steinberg, G.D. Utilization and Outcomes of Nephroureterectomy for Upper Tract Urothelial Carcinoma by Surgical Approach. J. Endourol. 2017, 31, 661–665. [Google Scholar] [CrossRef] [PubMed]
- Lenis, A.T.; Donin, N.M.; Faiena, I.; Salmasi, A.; Johnson, D.C.; Drakaki, A.; Gollapudi, K.; Blumberg, J.; Belldegrun, A.; Pantuck, A.; et al. Role of surgical approach on lymph node dissection yield and survival in patients with upper tract urothelial carcinoma. Urol. Oncol. 2018, 36, e1–e9. [Google Scholar] [CrossRef] [PubMed]
- Kido, K.; Hatakeyama, S.; Fujita, N.; Yamamoto, H.; Tobisawa, Y.; Yoneyama, T.; Yoneyama, T.; Hashimoto, Y.; Koie, T.; Iwabuchi, I.; et al. Oncologic outcomes for open and laparoscopic radical nephroureterectomy in patients with upper tract urothelial carcinoma. Int. J. Clin. Oncol. 2018, 23, 726–733. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Study (Year) | Right | Left | ||||||
|---|---|---|---|---|---|---|---|---|
| Renal Pelvis | Upper Ureter | Middle Ureter | Lower Ureter | Renal Pelvis | Upper Ureter | Middle Ureter | Lower Ureter | |
| Komatsu et al. [15] (1997) | Right side from the midline of the anterior surface of the aorta between the renal hilus and the aortic bifurcation | Right side from the midline of the anterior surface of the aorta between the renal hilus and the bifurcation of the common iliac artery | Right common iliac, external iliac, internal iliac, and obturator nodes | Left side from the midline of the anterior surface of the aorta between the renal hilus and the aortic bifurcation | Left side from the midline of the anterior surface of the aorta between the renal hilus and the bifurcation of the common iliac artery | Left common iliac, external iliac, internal iliac, and obturator nodes | ||
| Miyake et al. [16] (1998) | From the vena cava, between the renal hilus and the inferior mesenteric artery | From the vena-cava, between the renal hilus and bifurcation of the common iliac artery | Right pelvic nodes | From the para-aorta, between the renal hilus and the inferior mesenteric artery | From the para-aorta, between the renal hilus and bifurcation of the common iliac artery | Left pelvic nodes | ||
| Kondo et al. [17] (2007) | Right renal hilar, paracaval, and retrocaval nodes | Right renal hilar, paracaval, retrocaval nodes, and interaorticocaval nodes | Right common iliac, external iliac, obturator and internal iliac nodes | Left renal hilar, paracaval and retrocaval nodes | Left renal hilar, para-aortic nodes | Left common iliac, external iliac, obturator and internal iliac nodes | ||
| Brausi et al. [18] (2007) | Para-aortic, paracaval, or interaortocaval nodes from the renal hilus to the inferior mesenteric artery | Para-aortic, paracaval, or interaortocaval nodes from the renal hilus to the common iliac artery | Right pelvic nodes | Para-aortic, paracaval, or interaortocaval nodes from the renal hilus to the common iliac artery | Para-aortic, paracaval, or interaortocaval nodes from the renal hilus to the common iliac artery | Left pelvic nodes | ||
| Rajput et al. [7] (2011) | Retroperitoneal LND | Right pelvic nodes | Retroperitoneal LND | Left pelvic nodes | ||||
| Rao et al. [11] (2012) | Right perihilar lymph nodes, paracaval lymph nodes, right pelvic lymph nodes (common external and obturator lymph nodes). Removal of interaortocaval nodes was left to the discretion of the surgeon, depending on the presence of positive paracaval nodes as determined preoperatively or on intra-operative frozen section. | Left perihilar lymph nodes, para aortic lymph nodes, left pelvic lymph nodes (common external and obturator lymph nodes). Removal of interaortocaval nodes was left to the discretion of the surgeon, depending on the presence of positive para aortic nodes as determined preoperatively or on intra-operative frozen section. | ||||||
| Matin et al. [8] (2015) | Right hilum to vena cava bifurcation, including paracaval (including precaval region) and retrocaval nodes. Additional dissection of interaorticocaval and common iliac nodes was performed when suspicious nodes were identified in these regions on preoperative imaging or upon visual inspection intraoperatively. | Para-aortic in addition to right common and external iliac nodes. Additional paracaval or para-aortic was performed based on imaging intraoperative inspection or surgeon discretion. | Right pelvic lymphadenectomy (common, external, internal, and obturator). Additional paracaval or para-aortic was performed based on imaging intraoperative inspection or surgeon discretion. | Left hilum to origin of inferior mesenteric artery, including para-aortic nodes (including preaortic nodes). Additional dissection of interaorticocaval and common iliac nodes was performed when suspicious nodes were identified in these regions on preoperative imaging or upon visual inspection intraoperatively. | Para-aortic in addition to left common and external iliac nodes. Additional paracaval or para-aortic was performed based on imaging intraoperative inspection or surgeon discretion. | Right pelvic lymphadenectomy (common, external, internal, and obturator). Additional paracaval or para-aortic was performed based on imaging intraoperative inspection or surgeon discretion. | ||
| Abe et al. [19] (2015) | Right renal hilar, paracaval, retrocaval plus interaortocaval | Right obturator, common iliac, external iliac plus internal iliac | Left renal hilar plus para-aortic | Left obturator, common iliac, external iliac plus internal iliac | ||||
| Melquist et al. [20] (2016) | Hilar and precaval-paracaval-retrocaval regions plus interaortocaval dissection when technically possible. | Hilar with preaortic-paraaortic-retroaortic tissues plus interaortocaval dissection when technically possible. | ||||||
| Furuse et al. [12] (2016) | Renal hilum, paracaval, retrocaval (including interaortocaval whenever possible) | Renal hilum, common iliac, paracaval, retrocaval (including interaortocaval whenever possible) | Common-external-internal iliac, obturator | Renal hilum, para-aortic | Renal hilum, common iliac, para-aortic | Common-external-internal iliac, obturator | ||
| Study | Year | Study Interval | Number of Patients | Nodal Status (N° of Patients) | 2-yr CSS, % | 5-yr CSS, % | CSS: pN0 vs. pNx pN0 vs. pN+ pNx vs. pN+ | 2-yr DFS, % | 5-yr DFS, % | DFS: pN0 vs. pNx pN0 vs. pN+ pNx vs. pN+ | Median Number of Removed Nodes (IQ) | Median Follow-Up in Months (Range) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Komatsu et al. [15] | 1997 | 1985–1993 | 36 | pN0 (25) PN+ (11) | - | 100 21 | - - | - - | - - | - - | - | 55 (3–135) |
| Miyake et al. [16] | 1998 | 1986–1995 | 72 | pN0 (22) pNx (37) pN+(13) | - | 64 50 0 | - - - | - - - | - - - | - - - | - | - |
| Brown et al. [25] | 2006 | 1986–2004 | 184 | pN0 (105) pNx (119) pN+ (28) | - | 80 77 35 | p = 0.58 - - | - - - | - - - | p = 0.85 - - | - | - |
| Kondo et al. [17] | 2007 | 1989–2005 | 181 | pN0 (139) pNx/PN+ (32/10) | - - | 85.2 15.5 | - - | - - | - - | - - | 6 (2–30) | - |
| Brausi et al. [18] | 2007 | 1980–2002 | 82 | pN0/pN+ (24/16) pNx (42) | 81.6 44.8 | - - | - - | 64.3 46.3 | - - | - - | - | - |
| Secin et al. [10] | 2007 | 1985–2004 | 255 | pN0 (105) pNx (119) PN+ (28) | - - - | 56 73 0 | - - - | - - - | - - - | - - - | 4 (2–10) | 37 (-) |
| Novara et al. [26] | 2007 | 1989–2005 | 269 | pN0 (242) PN+ (27) | - - | 82 12 | - - | - - | - - | - - | - | - |
| Roscigno et al. [9] | 2008 | 1986–2003 | 132 | pN0 (69) pNx (37) PN+ (26) | - - - | 73 48 39 | p= 0.001 - p = 0.476 | - - - | 72 39 35 | p= 0.001 p= 0.001 p= 0.001 | 8 (2–24) | 42 (2–191) |
| Cho et al. [27] | 2008 | 1986–2005 | 152 | pN0 (54) pNx (89) PN+ (9) | - - - | 72 67 63 | p > 0.05 - - | - - - | 91 80 71 | HR 2.45 (0.26–22.47) HR 3.91 (1.35–11.32) - | 6 (1–35) | - |
| Roscigno et al. [24] | 2009 | 1987–2007 | 1130 | pN0 (412) pNx (578) PN+ (140) | - - - | 77 69 35 | p= 0.024 - p< 0.001 | - - - | 71 66 29 | p= 0.045 - p< 0.001 | - | 45 (1–250) |
| Lughezzani et al. [28] | 2010 | 1988–2004 | 2842 | pN0 (1835) pNx (747) PN+ (242) | - - - | 81.2 77.8 34.2 | p = 0.09 p < 0.001 p < 0.001 | - - - | - - - | - - - | - | 43 (1–203) |
| Mason et al. [29] | 2011 | 1990–2010 | 1029 | pN0 (199) pNx (753) PN+ (77) | - - - | 72.1 74.7 29.8 | HR 0.96 (0.64–1.44) HR 2.97 (1.47–6.01) HR 2.70 (1.56–4.69) | – - - | 39 41 7 | HR 1.23 (0.78–1.96) HR 2.94 (1.32–6.55) HR 2.83 (1.54–5.18) | Mean: 4,3 | 19.8 (7.2–53.8) |
| Burger et al. [30] | 2011 | 1987–2008 | 785 | pN0 (136) pNx (595) pN+ (54) | - - - | 79 77.4 26.7 | p = 0.945 p < 0.001 - | - - - | 71.6 76.9 21.3 | p = 0.586 p < 0.001 - | 3 (2–6) | 34 (15–65) |
| Yoo et al. [31] | 2016 | 1998–2012 | 418 | pN0 (116) pNx (286) pN+ (16) | - - - | OS = 80.2 OS = 71.7 OS = 12.5 | p = 0.230 - - | - - - | 76.4 73.4 93.7 | p = 0.682 - - | 7 (3–10) | 69 (-) |
| Ikeda et al. [32] | 2017 | 1985–2013 | 404 | pN0 (182) pNx (177) pN+ (40) | - - - | 84.5 73.3 43.6 | p< 0.001 p< 0.001 - | - - - | 78.3 61.9 33.2 | p= 0.001 p< 0.001 - | 6 (3–10) | 43 (17–89) |
| Inokuchi et al. [33] | 2017 | 1995–2009 | 2037 | pN0 (955) pNx (859) pN+ (223) | - - - | OS = 69.3 OS = 60.5 OS = 30 | HR 1.03 (0.83–1.27) HR 5.67 (4.56–7.05) - | - - - | - - - | - - - | 6 (3–11) | 45.8 (21.8–75.9) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duquesne, I.; Ouzaid, I.; Loriot, Y.; Moschini, M.; Xylinas, E. Lymphadenectomy for Upper Tract Urothelial Carcinoma: A Systematic Review. J. Clin. Med. 2019, 8, 1190. https://doi.org/10.3390/jcm8081190
Duquesne I, Ouzaid I, Loriot Y, Moschini M, Xylinas E. Lymphadenectomy for Upper Tract Urothelial Carcinoma: A Systematic Review. Journal of Clinical Medicine. 2019; 8(8):1190. https://doi.org/10.3390/jcm8081190
Chicago/Turabian StyleDuquesne, Igor, Idir Ouzaid, Yohann Loriot, Marco Moschini, and Evanguelos Xylinas. 2019. "Lymphadenectomy for Upper Tract Urothelial Carcinoma: A Systematic Review" Journal of Clinical Medicine 8, no. 8: 1190. https://doi.org/10.3390/jcm8081190
APA StyleDuquesne, I., Ouzaid, I., Loriot, Y., Moschini, M., & Xylinas, E. (2019). Lymphadenectomy for Upper Tract Urothelial Carcinoma: A Systematic Review. Journal of Clinical Medicine, 8(8), 1190. https://doi.org/10.3390/jcm8081190