Helicobacter pylori Eradication According to Sequencing-Based 23S Ribosomal RNA Point Mutation Associated with Clarithromycin Resistance

 ,
,
Abstract
:1. Introduction
2. Methods
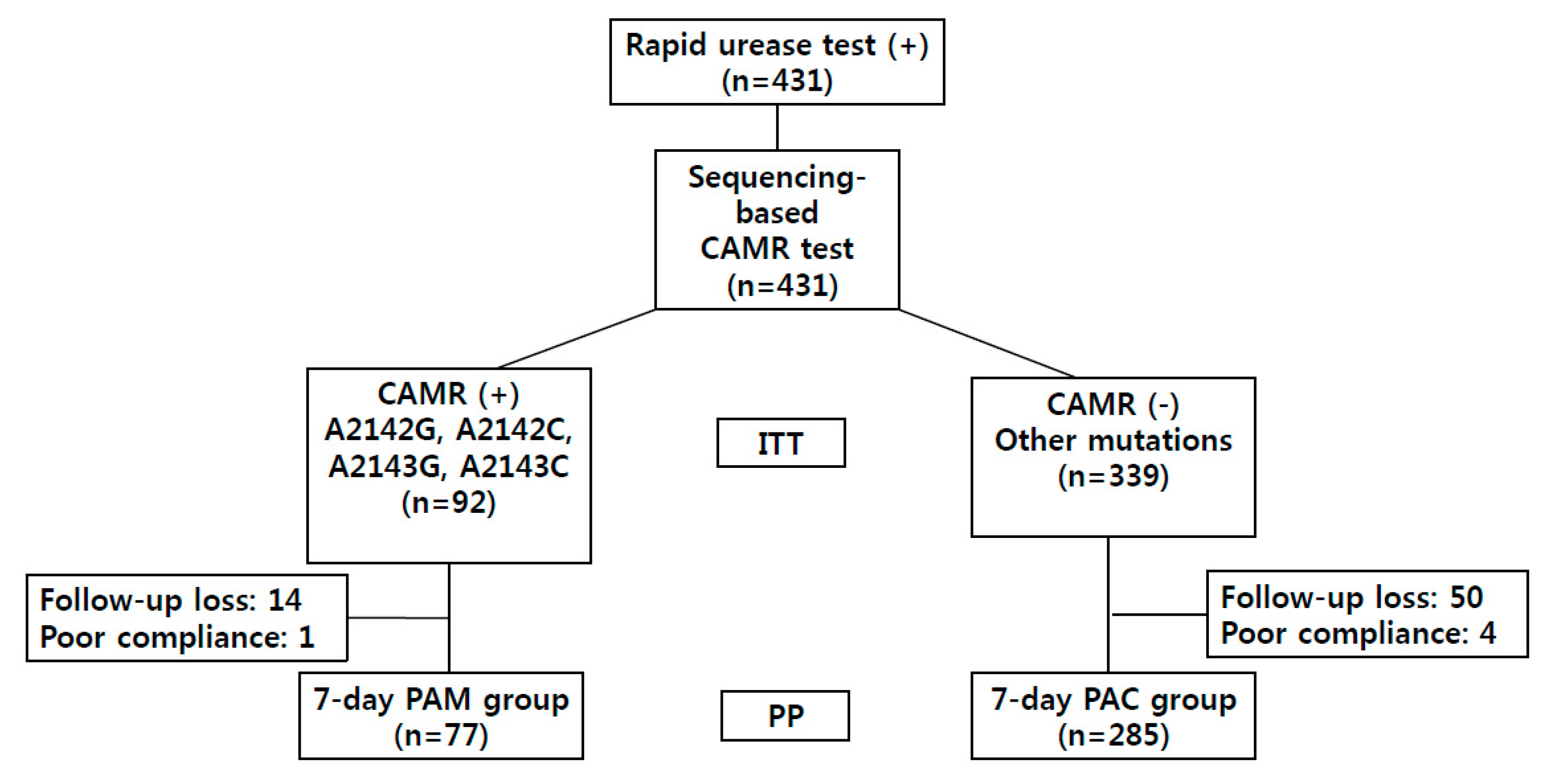
2.1. Patients
2.2. Detection of CAMR-Related Point Mutations
2.3. Analysis of CAMR-Related Point Mutations
2.4. Study Design and Treatment Regimen
2.5. Outcome Assessment
2.6. Statistical Analysis
3. Results
3.1. Clinical Characteristics of Study Patients
3.2. Distribution of CAMR-Related Point Mutations
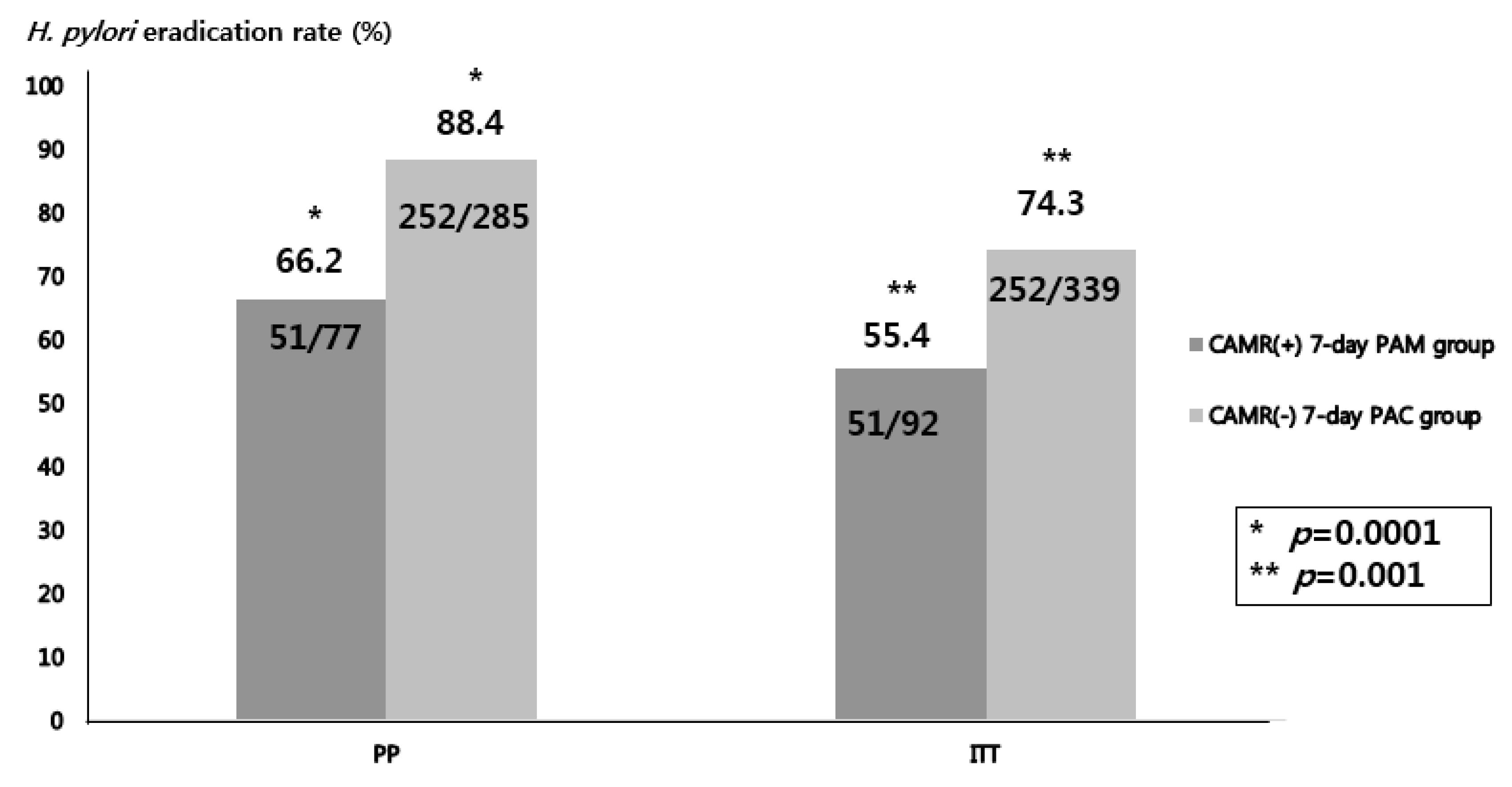
3.3. Efficacy of Seven-Day H. pylori Eradication Regimen Tailored to Detected CAMR-Related Point Mutations
3.4. H. Pylori Eradication Rates According to CAMR-Related Point Mutations
4. Discussion
Author Contributions
Conflicts of Interest
References
- Malfertheiner, P.; Megraud, F.; O’Morain, C.A.; Gisbert, J.P.; Kuipers, E.J.; Axon, A.T.; Bazzoli, F.; Gasbarrini, A.; Atherton, J.; Graham, D.Y.; et al. Management of Helicobacter pylori infection-the Maastricht V/Florence Consensus Report. Gut 2017, 66, 6–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sugano, K.; Tack, J.; Kuipers, E.J.; Graham, D.Y.; El-Omar, E.M.; Miura, S.; Haruma, K.; Asaka, M.; Uemura, N.; Malfertheiner, P. Kyoto global consensus report on Helicobacter pylori gastritis. Gut 2015, 64, 1353–1367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rokkas, T.; Pistiolas, D.; Sechopoulos, P.; Robotis, I.; Margantinis, G. The long-term impact of Helicobacter pylori eradication on gastric histology: A systematic review and meta-analysis. Helicobacter 2007, 12, 32–38. [Google Scholar] [CrossRef]
- Wang, J.; Xu, L.; Shi, R.; Huang, X.; Li, S.W.; Huang, Z.; Zhang, G. Gastric atrophy and intestinal metaplasia before and after Helicobacter pylori eradication: A meta-analysis. Digestion 2011, 83, 253–260. [Google Scholar] [CrossRef]
- Choi, I.J.; Kook, M.C.; Kim, Y.I.; Cho, S.J.; Lee, J.Y.; Kim, C.G.; Park, B.; Nam, B.H. Helicobacter pylori Therapy for the Prevention of Metachronous Gastric Cancer. N. Engl. J. Med. 2018, 378, 1085–1095. [Google Scholar] [CrossRef]
- Lee, Y.C.; Chiang, T.H.; Chou, C.K.; Tu, Y.K.; Liao, W.C.; Wu, M.S.; Graham, D.Y. Association Between Helicobacter pylori Eradication and Gastric Cancer Incidence: A Systematic Review and Meta-analysis. Gastroenterology 2016, 150, 1113–1124.e5. [Google Scholar] [CrossRef] [Green Version]
- Rokkas, T.; Rokka, A.; Portincasa, P. A systematic review and meta-analysis of the role of Helicobacter pylori eradication in preventing gastric cancer. Ann. Gastroenterol. 2017, 30, 414–423. [Google Scholar] [CrossRef]
- Kim, S.G.; Jung, H.K.; Lee, H.L.; Jang, J.Y.; Lee, H.; Kim, C.G.; Shin, W.G.; Shin, E.S.; Lee, Y.C. Guidelines for the diagnosis and treatment of Helicobacter pylori infection in Korea, 2013 revised edition. J. Gastroenterol. Hepatol. 2014, 29, 1371–1386. [Google Scholar] [CrossRef]
- Shin, W.G.; Lee, S.W.; Baik, G.H.; Huh, K.C.; Lee, S.I.; Chung, J.W.; Jung, W.T.; Park, M.I.; Jung, H.K.; Kim, H.U.; et al. Eradication Rates of Helicobacter pylori in Korea Over the Past 10 years and Correlation of the Amount of Antibiotics Use: Nationwide Survey. Helicobacter 2016, 21, 266–278. [Google Scholar] [CrossRef]
- Hwang, T.J.; Kim, N.; Kim, H.B.; Lee, B.H.; Nam, R.H.; Park, J.H.; Lee, M.K.; Park, Y.S.; Lee, D.H.; Jung, H.C.; et al. Change in antibiotic resistance of Helicobacter pylori strains and the effect of A2143G point mutation of 23S rRNA on the eradication of H. pylori in a single center of Korea. J. Clin. Gastroenterol. 2010, 44, 536–543. [Google Scholar] [CrossRef]
- Lee, J.W.; Kim, N.; Kim, J.M.; Nam, R.H.; Chang, H.; Kim, J.Y.; Shin, C.M.; Park, Y.S.; Lee, D.H.; Jung, H.C. Prevalence of primary and secondary antimicrobial resistance of Helicobacter pylori in Korea from 2003 through 2012. Helicobacter 2013, 18, 206–214. [Google Scholar] [CrossRef] [PubMed]
- Chung, W.C.; Jeon, E.J.; Oh, J.H.; Park, J.M.; Kim, T.H.; Cheung, D.Y.; Kim, B.W.; Kim, S.S.; Kim, J.I. Dual-priming oligonucleotide-based multiplex PCR using tissue samples from the rapid urease test kit for the detection of Helicobacter pylori in bleeding peptic ulcers. Dig. Liver Dis. 2016, 48, 899–903. [Google Scholar] [CrossRef] [PubMed]
- Gerrits, M.M.; van Vliet, A.H.; Kuipers, E.J.; Kusters, J.G. Helicobacter pylori and antimicrobial resistance: Molecular mechanisms and clinical implications. Lancet Infect. Dis. 2006, 6, 699–709. [Google Scholar] [CrossRef]
- Ierardi, E.; Giorgio, F.; Iannone, A.; Losurdo, G.; Principi, M.; Barone, M.; Pisani, A.; Di Leo, A. Noninvasive molecular analysis of Helicobacter pylori: Is it time for tailored first-line therapy? World J. Gastroenterol. 2017, 23, 2453–2458. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.M.; Kim, J.S.; Kim, N.; Kim, Y.J.; Kim, I.Y.; Chee, Y.J.; Lee, C.H.; Jung, H.C. Gene mutations of 23S rRNA associated with clarithromycin resistance in Helicobacter pylori strains isolated from Korean patients. J. Microbiol. Biotechnol. 2008, 18, 1584–1589. [Google Scholar] [PubMed]
- Umegaki, N.; Shimoyama, T.; Nishiya, D.; Suto, T.; Fukuda, S.; Munakata, A. Clarithromycin-resistance and point mutations in the 23S rRNA gene in Helicobacter pylori isolates from Japan. J. Gastroenterol. Hepatol. 2000, 15, 906–909. [Google Scholar] [CrossRef]
- Malfertheiner, P. Helicobacter pylori Treatment for Gastric Cancer Prevention. N. Engl. J. Med. 2018, 378, 1154–1156. [Google Scholar] [CrossRef]
- Lopez-Gongora, S.; Puig, I.; Calvet, X.; Villoria, A.; Baylina, M.; Munoz, N.; Sanchez-Delgado, J.; Suarez, D.; Garcia-Hernando, V.; Gisbert, J.P. Systematic review and meta-analysis: Susceptibility-guided versus empirical antibiotic treatment for Helicobacter pylori infection. J. Antimicrob. Chemother. 2015, 70, 2447–2455. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.J.; Kim, J.I.; Cheung, D.Y.; Kim, T.H.; Jun, E.J.; Oh, J.H.; Chung, W.C.; Kim, B.W.; Kim, S.S.; Park, S.H.; et al. Eradication of Helicobacter pylori according to 23S ribosomal RNA point mutations associated with clarithromycin resistance. J. Infect. Dis. 2013, 208, 1123–1130. [Google Scholar] [CrossRef] [Green Version]
- Liou, J.M.; Chen, C.C.; Chang, C.Y.; Chen, M.J.; Fang, Y.J.; Lee, J.Y.; Chen, C.C.; Hsu, S.J.; Hsu, Y.C.; Tseng, C.H.; et al. Efficacy of genotypic resistance-guided sequential therapy in the third-line treatment of refractory Helicobacter pylori infection: A multicentre clinical trial. J. Antimicrob. Chemother. 2013, 68, 450–456. [Google Scholar] [CrossRef] [Green Version]
- Cho, J.H.; Jeon, S.R.; Kim, H.G.; Jin, S.Y.; Park, S. Cost-effectiveness of a tailored Helicobacter pylori eradication strategy based on the presence of a 23S ribosomal RNA point mutation that causes clarithromycin resistance in Korean patients. J. Gastroenterol. Hepatol. 2019, 34, 700–706. [Google Scholar] [CrossRef] [PubMed]
- Park, C.G.; Kim, S.; Lee, E.J.; Jeon, H.S.; Han, S. Clinical relevance of point mutations in the 23S rRNA gene in Helicobacter pylori eradication: A prospective, observational study. Medicine 2018, 97, e11835. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.S.; Kang, J.O.; Eun, C.S.; Han, D.S.; Choi, T.Y. Mutations in the 23S rRNA gene of Helicobacter pylori associated with clarithromycin resistance. J. Korean Med. Sci. 2002, 17, 599–603. [Google Scholar] [CrossRef] [Green Version]
- Nishizawa, T.; Suzuki, H.; Tsugawa, H.; Muraoka, H.; Matsuzaki, J.; Hirata, K.; Ikeda, F.; Takahashi, M.; Hibi, T. Enhancement of amoxicillin resistance after unsuccessful Helicobacter pylori eradication. Antimicrob. Agents Chemother. 2011, 55, 3012–3014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.H.; Ahn, J.Y.; Choi, K.D.; Jung, H.Y.; Kim, J.M.; Baik, G.H.; Kim, B.W.; Park, J.C.; Jung, H.K.; Cho, S.J.; et al. Korean College of Helicobacter; Upper Gastrointestinal Research., Nationwide antibiotic resistance mapping of Helicobacter pylori in Korea: A prospective multicenter study. Helicobacter 2019, 24, e12592. [Google Scholar] [CrossRef]
- Versalovic, J.; Osato, M.S.; Spakovsky, K.; Dore, M.P.; Reddy, R.; Stone, G.G.; Shortridge, D.; Flamm, R.K.; Tanaka, S.K.; Graham, D.Y. Point mutations in the 23S rRNA gene of Helicobacter pylori associated with different levels of clarithromycin resistance. J. Antimicrob. Chemother. 1997, 40, 283–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Francesco, V.; Zullo, A.; Ierardi, E.; Giorgio, F.; Perna, F.; Hassan, C.; Morini, S.; Panella, C.; Vaira, D. Phenotypic and genotypic Helicobacter pylori clarithromycin resistance and therapeutic outcome: Benefits and limits. J. Antimicrob. Chemother. 2010, 65, 327–332. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variables | |
|---|---|
| Age, mean ± SD (range) | 54.7 ± 13.6 (19–85) |
| Male, n (%) | 236 (65.2) |
| Clinical diagnosis, n (%) | |
| Nodular gastritis | 16 (4.4) |
| Chronic atrophic gastritis | 8 (2.2) |
| Peptic ulcer | 272 (75.1) |
| Gastric adenoma | 48 (13.3) |
| Gastric adenocarcinoma | 18 (5) |
| Point Mutation | Number (%) |
|---|---|
| Clinically significant mutation | 92 (21.3) |
| A2142G | 4 (0.9) |
| A2142C | 1 (0.2) |
| A2143G | 84 (19.5) |
| A2142G + A2143G | 3 (0.7) |
| Clinically insignificant mutation | 289 (67.1) |
| T2182C | 283 (65.7) |
| others | 6 (1.4) |
| No point mutation | 50 (11.6) |
| Point Mutation | Eradication Rate (%) |
|---|---|
| Overall | 303/362 (83.7) |
| none | 35/42 (83.3) |
| A2142G | 1/4 (25) |
| A2142C | 1/1 (100) |
| A2143G | 47/70 (67.1) |
| A2142G+A2143G | 2/2 (100) |
| T2182C | 212/238 (89.1) |
| Others (A2223G, C2195T) | 5/5 (100) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seo, S.I.; Do, B.J.; Kang, J.G.; Kim, H.S.; Jang, M.K.; Kim, H.Y.; Shin, W.G. Helicobacter pylori Eradication According to Sequencing-Based 23S Ribosomal RNA Point Mutation Associated with Clarithromycin Resistance. J. Clin. Med. 2020, 9, 54. https://doi.org/10.3390/jcm9010054
Seo SI, Do BJ, Kang JG, Kim HS, Jang MK, Kim HY, Shin WG. Helicobacter pylori Eradication According to Sequencing-Based 23S Ribosomal RNA Point Mutation Associated with Clarithromycin Resistance. Journal of Clinical Medicine. 2020; 9(1):54. https://doi.org/10.3390/jcm9010054
Chicago/Turabian StyleSeo, Seung In, Byoung Joo Do, Jin Gu Kang, Hyoung Su Kim, Myoung Kuk Jang, Hak Yang Kim, and Woon Geon Shin. 2020. "Helicobacter pylori Eradication According to Sequencing-Based 23S Ribosomal RNA Point Mutation Associated with Clarithromycin Resistance" Journal of Clinical Medicine 9, no. 1: 54. https://doi.org/10.3390/jcm9010054
APA StyleSeo, S. I., Do, B. J., Kang, J. G., Kim, H. S., Jang, M. K., Kim, H. Y., & Shin, W. G. (2020). Helicobacter pylori Eradication According to Sequencing-Based 23S Ribosomal RNA Point Mutation Associated with Clarithromycin Resistance. Journal of Clinical Medicine, 9(1), 54. https://doi.org/10.3390/jcm9010054