The Effect of Virtual Reality on Preoperative Anxiety: A Meta-Analysis of Randomized Controlled Trials


Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Study Selection
2.3. Data Extraction and Risk of Bias Assessment
2.4. Data Synthesis and Meta-Analysis
3. Results
3.1. Description of Studies
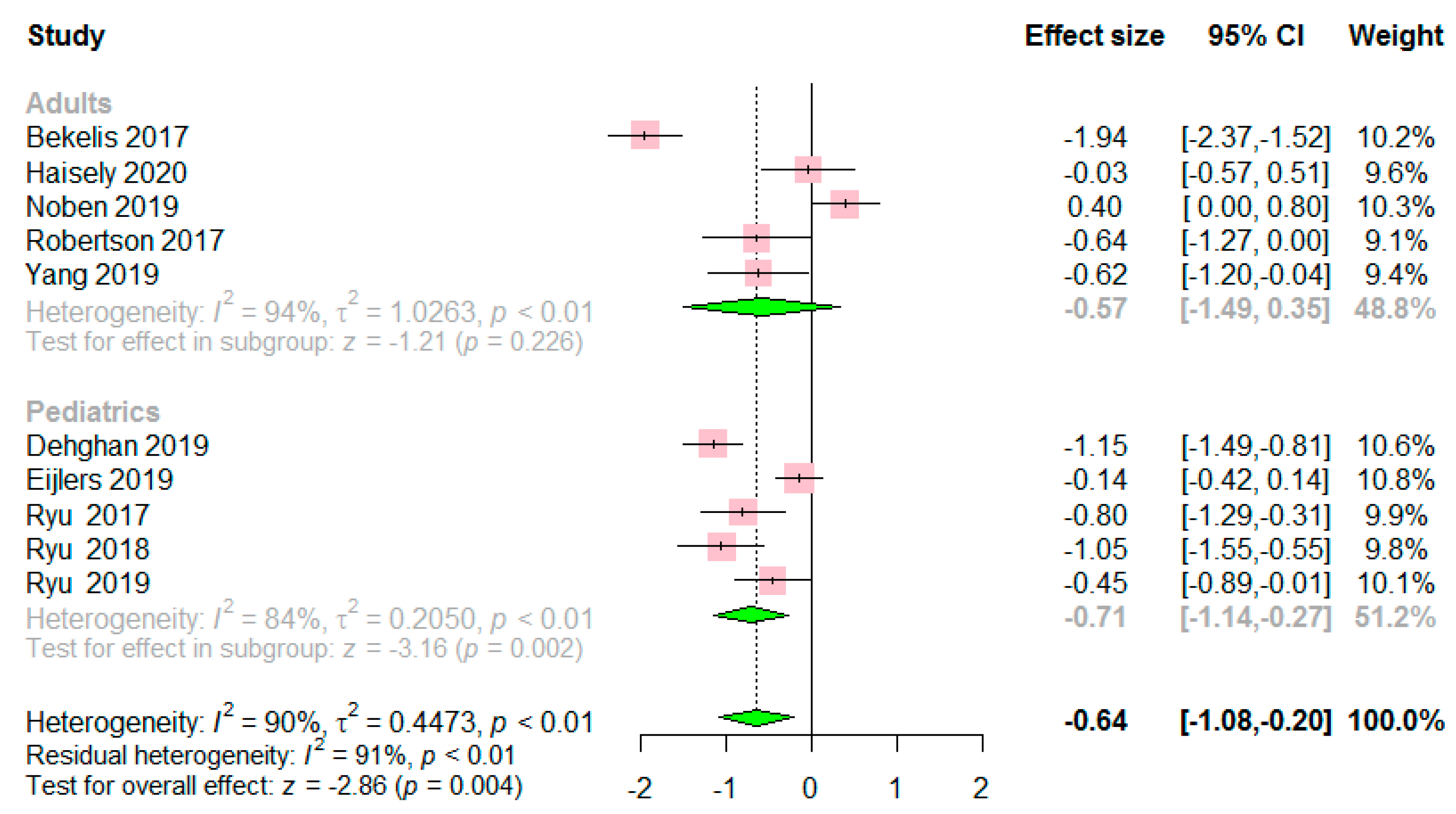
3.2. Preoperative Anxiety Score
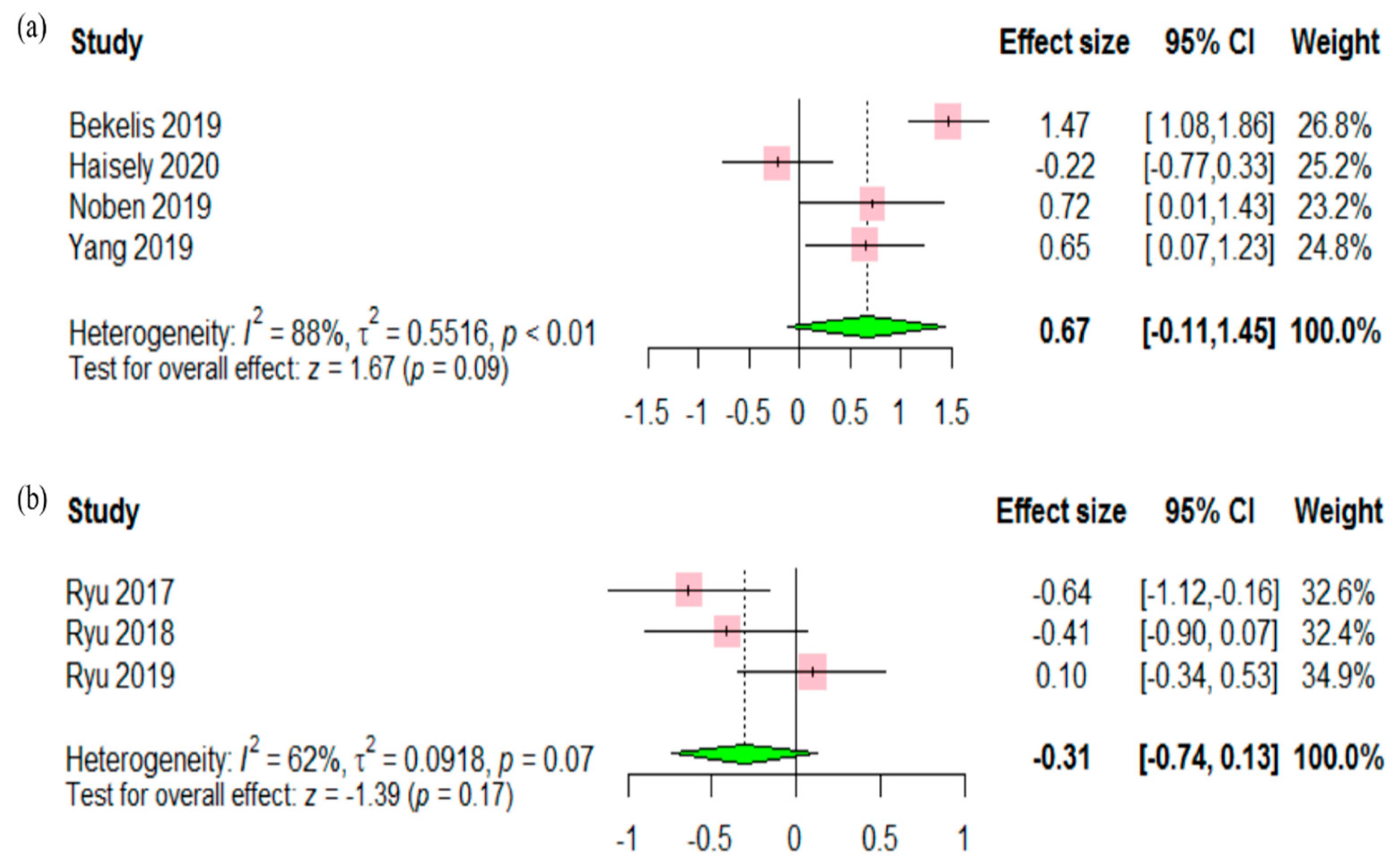
3.3. Satisfaction and Behavior Disturbance
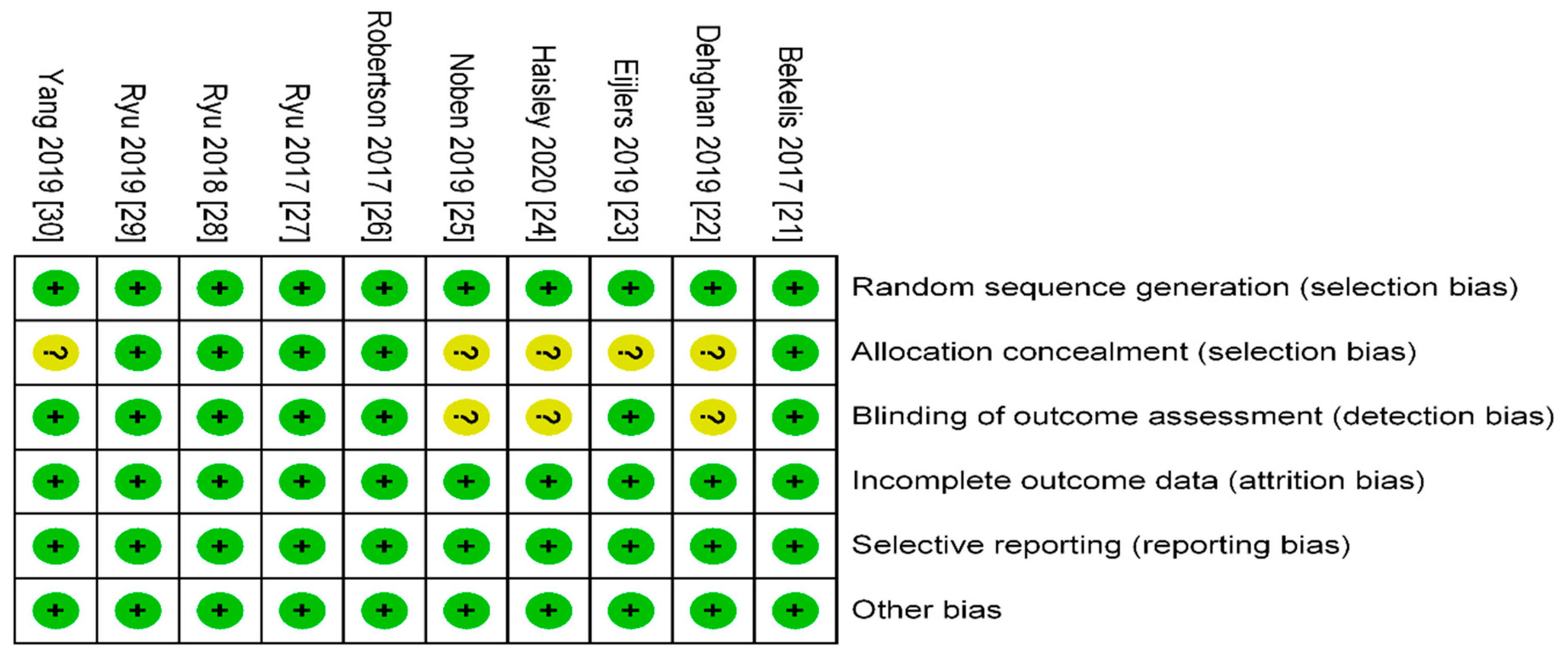
3.4. Risk of Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Chen, S.B.; Hu, H.; Gao, Y.S.; He, H.Y.; Jin, D.X.; Zhang, C.Q. Prevalence of clinical anxiety, clinical depression and associated risk factors in chinese young and middle-aged patients with osteonecrosis of the femoral head. PLoS ONE 2015, 10, e0120234. [Google Scholar] [CrossRef] [PubMed]
- Erkilic, E.; Kesimci, E.; Soykut, C.; Doger, C.; Gumus, T.; Kanbak, O. Factors associated with preoperative anxiety levels of Turkish surgical patients: From a single center in Ankara. Patient Prefer Adherence 2017, 11, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Weissman, C. The metabolic response to stress: An overview and update. Anesthesiology 1990, 73, 308–327. [Google Scholar] [CrossRef] [PubMed]
- Mulugeta, H.; Ayana, M.; Sintayehu, M.; Dessie, G.; Zewdu, T. Preoperative anxiety and associated factors among adult surgical patients in Debre Markos and Felege Hiwot referral hospitals, Northwest Ethiopia. BMC Anesthesiol. 2018, 18, 155. [Google Scholar] [CrossRef] [PubMed]
- Maranets, I.; Kain, Z.N. Preoperative anxiety and intraoperative anesthetic requirements. Anesth. Analg. 1999, 89, 1346–1351. [Google Scholar] [CrossRef]
- Ali, A.; Altun, D.; Oguz, B.H.; Ilhan, M.; Demircan, F.; Koltka, K. The effect of preoperative anxiety on postoperative analgesia and anesthesia recovery in patients undergoing laparascopic cholecystectomy. J. Anesth. 2014, 28, 222–227. [Google Scholar] [CrossRef]
- Székely, G.; Satava, R.M. Virtual reality in medicine. Interview by Judy Jones. BMJ 1999, 319, 1305. [Google Scholar] [CrossRef] [Green Version]
- Sjöling, M.; Nordahl, G.; Olofsson, N.; Asplund, K. The impact of preoperative information on state anxiety, postoperative pain and satisfaction with pain management. Patient Educ. Couns. 2003, 51, 169–176. [Google Scholar] [CrossRef]
- Jlala, H.A.; French, J.L.; Foxall, G.L.; Hardman, J.G.; Bedforth, N.M. Effect of preoperative multimedia information on perioperative anxiety in patients undergoing procedures under regional anaesthesia. Br. J. Anaesth. 2010, 104, 369–374. [Google Scholar] [CrossRef] [Green Version]
- de Carvalho, M.R.; Freire, R.C.; Nardi, A.E. Virtual reality as a mechanism for exposure therapy. World J. Biol. Psychiatry 2010, 11, 220–230. [Google Scholar] [CrossRef]
- Maples-Keller, J.L.; Bunnell, B.E.; Kim, S.-J.; Rothbaum, B.O. The Use of Virtual Reality Technology in the Treatment of Anxiety and Other Psychiatric Disorders. Harv. Rev. Psychiatry 2017, 25, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, H.G.; Garcia-Palacios, A.; Patterson, D.R.; Jensen, M.; Furness, T., 3rd; Ammons, W.F., Jr. The effectiveness of virtual reality for dental pain control: A case study. Cyberpsychol. Behav. 2001, 4, 527–535. [Google Scholar] [CrossRef] [PubMed]
- Eijlers, R.; Utens, E.; Staals, L.M.; de Nijs, P.F.A.; Berghmans, J.M.; Wijnen, R.M.H.; Hillegers, M.H.J.; Dierckx, B.; Legerstee, J.S. Systematic Review and Meta-analysis of Virtual Reality in Pediatrics: Effects on Pain and Anxiety. Anesth. Analg. 2019, 129, 1344–1353. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [Green Version]
- Practical Meta-Analysis Effect Size Calculator. Available online: Campbellcollaboration.org/escalc.html/EffectSizeCalculator-Home.php (accessed on 12 June 2020).
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0; The Cochrane Collaboration: Chichester, UK, 2011. [Google Scholar]
- R Core Team. A Language and Environment for Statistical Computing. In R FOUNDATION for Statistical Computing; R Core Team: Vienna, Austria, 2013; Available online: https://www.R-project.org (accessed on 2 July 2020).
- Schwarzer, G. Meta: An R package for meta-analysis. R News 2007, 7, 40–45. [Google Scholar]
- Bekelis, K.; Calnan, D.; Simmons, N.; MacKenzie, T.A.; Kakoulides, G. Effect of an Immersive Preoperative Virtual Reality Experience on Patient Reported Outcomes: A Randomized Controlled Trial. Ann. Surg. 2017, 265, 1068–1073. [Google Scholar] [CrossRef]
- Dehghan, F.; Jalali, R.; Bashiri, H. The effect of virtual reality technology on preoperative anxiety in children: A Solomon four-group randomized clinical trial. Perioper. Med. 2019, 8. [Google Scholar] [CrossRef] [Green Version]
- Eijlers, R.; Dierckx, B.; Staals, L.M.; Berghmans, J.M.; Van Der Schroeff, M.P.; Strabbing, E.M.; Wijnen, R.M.H.; Hillegers, M.H.J.; Legerstee, J.S.; Utens, E. Virtual reality exposure before elective day care surgery to reduce anxiety and pain in children: A randomised controlled trial. Eur. J. Anaesthesiol. 2019, 36, 728–737. [Google Scholar] [CrossRef]
- Haisley, K.R.; Straw, O.J.; Müller, D.T.; Antiporda, M.A.; Zihni, A.M.; Reavis, K.M.; Bradley, D.D.; Dunst, C.M. Feasibility of implementing a virtual reality program as an adjuvant tool for peri-operative pain control; Results of a randomized controlled trial in minimally invasive foregut surgery. Complement. Ther. Med. 2020, 49. [Google Scholar] [CrossRef] [PubMed]
- Noben, L.; Goossens, S.; Truijens, S.E.M.; van Berckel, M.M.G.; Perquin, C.W.; Slooter, G.D.; van Rooijen, S.J. A Virtual Reality Video to Improve Information Provision and Reduce Anxiety Before Cesarean Delivery: Randomized Controlled Trial. JMIR Ment. Health 2019, 6, e15872. [Google Scholar] [CrossRef] [PubMed]
- Robertson, A.; Khan, R.; Fick, D.; Robertson, W.B.; Gunaratne, D.R.; Yapa, S.; Bowden, V.; Hoffman, H.; Rajan, R. The effect of Virtual Reality in reducing preoperative anxiety in patients prior to arthroscopic knee surgery: A randomised controlled trial. In Proceedings of the 2017 IEEE 5th International Conference on Serious Games and Applications for Health, Perth, Australia, 2–4 April 2017. [Google Scholar]
- Ryu, J.H.; Park, S.J.; Park, J.W.; Kim, J.W.; Yoo, H.J.; Kim, T.W.; Hong, J.S.; Han, S.H. Randomized clinical trial of immersive virtual reality tour of the operating theatre in children before anaesthesia. Br. J. Surg. 2017, 104, 1628–1633. [Google Scholar] [CrossRef] [PubMed]
- Ryu, J.H.; Park, J.W.; Nahm, F.S.; Jeon, Y.T.; Oh, A.Y.; Lee, H.J.; Kim, J.H.; Han, S.H. The effect of gamification through a virtual reality on preoperative anxiety in pediatric patients undergoing general anesthesia: A prospective, randomized, and controlled trial. J. Clin. Med. 2018, 7, 284. [Google Scholar] [CrossRef] [Green Version]
- Ryu, J.H.; Oh, A.Y.; Yoo, H.J.; Kim, J.H.; Park, J.W.; Han, S.H. The effect of an immersive virtual reality tour of the operating theater on emergence delirium in children undergoing general anesthesia: A randomized controlled trial. Paediatr. Anaesth. 2019, 29, 98–105. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.H.; Ryu, J.J.; Nam, E.; Lee, H.S.; Lee, J.K. Effects of Preoperative Virtual Reality Magnetic Resonance Imaging on Preoperative Anxiety in Patients Undergoing Arthroscopic Knee Surgery: A Randomized Controlled Study. Arthroscopy 2019, 35, 2394–2399. [Google Scholar] [CrossRef]
- Balk, E.M.; Earley, A.; Patel, K.; Trikalinos, T.A.; Dahabreh, I.J. Empirical Assessment of Within-Arm Correlation Imputation in Trials of Continuous Outcomes; Methods Research Report Prepared by the Tufts Evidence-based Practice Center under Contract No. 290-2007-10055-1, AHRQ Publication No. 12(13)-EHC141-EF; Agency for Healthcare Reesearch and Quality: Rockville, MD, USA, 2012. [Google Scholar]
- Han, S.-H.; Park, J.-W.; Choi, S.I.; Kim, J.Y.; Lee, H.; Yoo, H.-J.; Ryu, J.-H. Effect of Immersive Virtual Reality Education Before Chest Radiography on Anxiety and Distress Among Pediatric Patients: A Randomized Clinical Trial. JAMA Pediatr. 2019, 173, 1026–1031. [Google Scholar] [CrossRef]
- Ganry, L.; Hersant, B.; Sidahmed-Mezi, M.; Dhonneur, G.; Meningaud, J.P. Using virtual reality to control preoperative anxiety in ambulatory surgery patients: A pilot study in maxillofacial and plastic surgery. J. Stomatol. Oral. Maxillofac. Surg. 2018, 119, 257–261. [Google Scholar] [CrossRef]
- Mosso, J.L.; Gorini, A.; De La Cerda, G.; Obrador, T.; Almazan, A.; Mosso, D.; Nieto, J.J.; Riva, G. Virtual reality on mobile phones to reduce anxiety in outpatient surgery. Stud. Health Technol. Inform. 2009, 142, 195–200. [Google Scholar]
- North, M.M.; North, S.M. Virtual reality therapy. In Computer-Assisted and Web-Based Innovations in Psychology, Special Education, and Health; James, K.L., Aron, J.F., Eds.; Elsevier: London, UK, 2016; pp. 141–156. [Google Scholar]
- Riva, G. Virtual environments in clinical psychology. Psychother. Theory Res. Pract. Train. 2003, 40, 68–76. [Google Scholar] [CrossRef] [Green Version]
- Hoffman, H.G. Virtual-reality therapy. Sci. Am. 2004, 291, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Klassen, J.A.; Liang, Y.; Tjosvold, L.; Klassen, T.P.; Hartling, L. Music for pain and anxiety in children undergoing medical procedures: A systematic review of randomized controlled trials. Ambul. Pediatr. 2008, 8, 117–128. [Google Scholar] [CrossRef] [PubMed]
- Uman, L.S.; Birnie, K.A.; Noel, M.; Parker, J.A.; Chambers, C.T.; McGrath, P.J.; Kisely, S.R. Psychological interventions for needle-related procedural pain and distress in children and adolescents. Cochrane Database Syst. Rev. 2013, CD005179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davidson, A.J.; Shrivastava, P.P.; Jamsen, K.; Huang, G.H.; Czarnecki, C.; Gibson, M.A.; Stewart, S.A.; Stargatt, R. Risk factors for anxiety at induction of anesthesia in children: A prospective cohort study. Paediatr. Anaesth. 2006, 16, 919–927. [Google Scholar] [CrossRef]
- Chorney, J.M.; Kain, Z.N. Behavioral analysis of children’s response to induction of anesthesia. Anesth. Analg. 2009, 109, 1434–1440. [Google Scholar] [CrossRef]
- Paryab, M.; Hosseinbor, M. Dental anxiety and behavioral problems: A study of prevalence and related factors among a group of Iranian children aged 6–12. J. Indian Soc. Pedod. Prev. Dent. 2013, 31, 82–86. [Google Scholar] [CrossRef]
- Bolton, D.; Dearsley, P.; Madronal-Luque, R.; Baron-Cohen, S. Magical thinking in childhood and adolescence: Development and relation to obsessive compulsion. Br. J. Dev. Psychol. 2002, 20, 479–494. [Google Scholar] [CrossRef]
- Lillard, A.S. Pretend play skills and the child’s theory of mind. Child Dev. 1993, 64, 348–371. [Google Scholar] [CrossRef]
- Seide, S.E.; Röver, C.; Friede, T. Likelihood-based random-effects meta-analysis with few studies: Empirical and simulation studies. BMC Med. Res. Methodol. 2019, 19, 16. [Google Scholar] [CrossRef]
- Guolo, A.; Varin, C. Random-effects meta-analysis: The number of studies matters. Stat. Methods Med. Res. 2017, 26, 1500–1518. [Google Scholar] [CrossRef]
- Lahti, S.; Suominen, A.; Freeman, R.; Lahteenoja, T.; Humphris, G. Virtual Reality Relaxation to Decrease Dental Anxiety: Immediate Effect Randomized Clinical Trial. JDR Clin. Trans. Res. 2020, 2380084420901679. [Google Scholar] [CrossRef] [PubMed]
- Matthias, A.T.; Samarasekera, D.N. Preoperative anxiety in surgical patients-experience of a single unit. Acta Anaesthesiol. Taiwan 2012, 50, 3–6. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Sample Size (VR/Control) | Age | Anxiety Measure | Surgery | |
|---|---|---|---|---|---|
| VR | Control | ||||
| Bekelis 2017 [21] | 64/63 | 57.3 | 53.4 | APAIS | Craniotomy or spine surgery |
| Dehghan 2019 [22] | 20/20 | 7.35 | YPAS | Abdominal surgery | |
| Eijlers 2019 [23] | 94/97 | 8.3 | 7.5 | mYPAS | Maxillofacial, dental, Ear-Nose-Throat surgery |
| Haisley 2020 [24] | 26/26 | 65.5 | 61.5 | NRS | Minimally invasive foregut |
| Noben 2019 [25] | 49/48 | 32.6 | 33.12 | VAS | Cesarean delivery |
| Robertson 2017 [26] | 20/20 | 47 | HADS | Arthroscopic knee surgery | |
| Ryu 2017 [27] | 34/35 | 6 | 6 | mYPAS | Elective surgery |
| Ryu 2018 [28] | 34/35 | 5 | 6 | mYPAS | Elective day surgery |
| Ryu 2019 [29] | 41/39 | 6 | 6 | mYPAS | Elective surgery |
| Yang 2019 [30] | 24/24 | 32.5 | 38.0 | APAIS | Arthroscopic knee surgery |
| Variables | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p Value | OR | 95% CI | p Value | |
| Age | 0.00 | −0.02 to 0.02 | 0.97 | |||
| Female | 2.07 | 0.46 to 3.69 | 0.01 | 1.63 | 0.21 to 3.05 | 0.02 |
| Sample size | 0.00 | −0.01 to 0.01 | 0.82 | |||
| Publication year | 0.39 | 0.03 to 0.75 | 0.03 | 0.28 | −0.03 to 0.58 | 0.07 |
| Pediatric | −0.15 | −1.09 to 0.80 | 0.76 | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koo, C.-H.; Park, J.-W.; Ryu, J.-H.; Han, S.-H. The Effect of Virtual Reality on Preoperative Anxiety: A Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2020, 9, 3151. https://doi.org/10.3390/jcm9103151
Koo C-H, Park J-W, Ryu J-H, Han S-H. The Effect of Virtual Reality on Preoperative Anxiety: A Meta-Analysis of Randomized Controlled Trials. Journal of Clinical Medicine. 2020; 9(10):3151. https://doi.org/10.3390/jcm9103151
Chicago/Turabian StyleKoo, Chang-Hoon, Jin-Woo Park, Jung-Hee Ryu, and Sung-Hee Han. 2020. "The Effect of Virtual Reality on Preoperative Anxiety: A Meta-Analysis of Randomized Controlled Trials" Journal of Clinical Medicine 9, no. 10: 3151. https://doi.org/10.3390/jcm9103151
APA StyleKoo, C.-H., Park, J.-W., Ryu, J.-H., & Han, S.-H. (2020). The Effect of Virtual Reality on Preoperative Anxiety: A Meta-Analysis of Randomized Controlled Trials. Journal of Clinical Medicine, 9(10), 3151. https://doi.org/10.3390/jcm9103151