1. Introduction
Gastroenteropancreatic neuroendocrine neoplasms (GEP-NENs) gain increased clinical significance since their incidence is continuously increasing [
1]. GEP-NENs are nowadays as common as testicular tumors, gliomas, and multiple myeloma [
2]. Surgery remains the gold standard for cure [
3,
4], but GEP-NENs are often diagnosed at an advanced stage making therapy challenging [
2]. Tumor grading directly influences the therapeutic approach and even stage IV patients with well to moderately differentiated tumors might have beneficial survival rates [
5]. Biotherapy with somatostatin analogs is the first line of systemic treatment for well-differentiated GEP-NENs [
6,
7,
8], for poorly differentiated neuroendocrine carcinomas (NECs) the use of systemic chemotherapy is recommended [
9]. Targeted therapy has been evolved for the treatment of GEP-NENs [
9,
10]. Nonetheless, more research is needed in order to easily decide which therapy is best and to monitor treatment efficacy. Thus, optimal management of GEP-NEN patients is still challenging and predicting the therapeutic value of a single agent would be desirable.
Pathologic de-novo angiogenesis is a key step in cancer development since it facilitates local tumor progression and further leads to distant metastases [
11,
12]. Vascular endothelial growth factor (VEGF) is a key player in angiogenesis and fosters angiogenesis by binding to a distinct cell surface receptor (VEGFR 1-3). GEP-NENs are highly vascularized tumors and it was demonstrated that VEGF is expressed on GEP-NENs [
13]. VEGF and VEGFR have been extensively studied and efforts have been made to inhibit the VEGF/R pathway. Therefore, the multi-kinase inhibitor sunitinib, targeting, inter alia, VEGFR, is approved for the treatment of advanced pancreatic neuroendocrine neoplasms (pNENs) [
14]. However, treatment with sunitinib might lead to essential side effects and a more tailored therapeutic approach inhibiting for instance only one or two kinases might be less noxious [
15]. In this respect, increasing evidence suggests that the combination of VEGF/R inhibitors and novel checkpoint inhibitors might be prognostic beneficial [
16,
17]. Nonetheless, a comprehensive analysis of the expression rates of VEGFR 1-3 and immune checkpoint markers has not been investigated so far. Moreover, the predictive value of the expression levels of VEGF and VEGFR is inconsistent [
18,
19] and a detailed analysis of the association of VEGFR 1-3 and its prognostic role in GEP-NENs has not been conducted so far.
Thus, the present study aimed to evaluate the expression rates of VEGFR 1-3 and to analyze a potential association to immune checkpoint markers in GEP-NENs. Furthermore, the prognostic value of these markers was investigated.
4. Discussion
GEP-NENs are highly vascularized tumors, thus pathologic de-novo angiogenesis is an important characteristic feature of this entity. Furthermore, neuroendocrine cells of the digestive tract are capable of producing VEGF, which is mandatory for microvessel stability in GEP-NENs [
13,
27]. The coexpression of VEGF and its receptors in tumors seem to directly lead to a higher developed vascular architecture [
28]. In this respect, the present study provides a detailed analysis of the most comprehensive patient collective regarding the expression of VEGFR 1-3 in GEP-NENs. VEGFRs are a family of tyrosine kinase receptors consisting of three members: VEGFR 1 or Flt-1 (fms-like TK1); VEGFR 2 or KDR (kinase insert domain-containing receptor TK); VEGFR 3 or Flt-4 (fms-like TK4) [
29].
The expression levels of the three VEGFRs do not represent a prognostic factor. Nevertheless, the definition of its expression levels might be beneficial for certain patients since there was a significant correlation of the expression levels of VEGFR 1-3 with tumor stage. Treatment with multikinase inhibitors consists commonly of a combination with different regimens such as the inhibitor (bevacizumab, sunitinib) plus somatostatin analogs and chemotherapy, respectively [
14,
30]. This therapeutic approach is commonly associated with clinically relevant side effects and thus the adherence to the therapy might be reduced up to 54% [
31]. Additionally, monotherapy with VEGFR-inhibitors also can lead to a wide spectrum of severe adverse reactions. Especially cardiovascular side effects are commonly seen and should be thoroughly monitored [
32,
33]. Decreased adherence in turn results in a reduced therapeutic effect. Thus, the results of the present study might help to define patients who might benefit from anti-VEGFR therapy. Subsequently adherence might increase. Moreover, by assessing parameters in CT scans a prognostic relevant distinction of patients seems to be feasible. This non-invasive approach is at least in part “dynamic” and allows evaluating the tumor heterogeneity over time without the need of a further biopsy [
34]. Evaluating treatment efficacy seems possible and might further help to increase adherence.
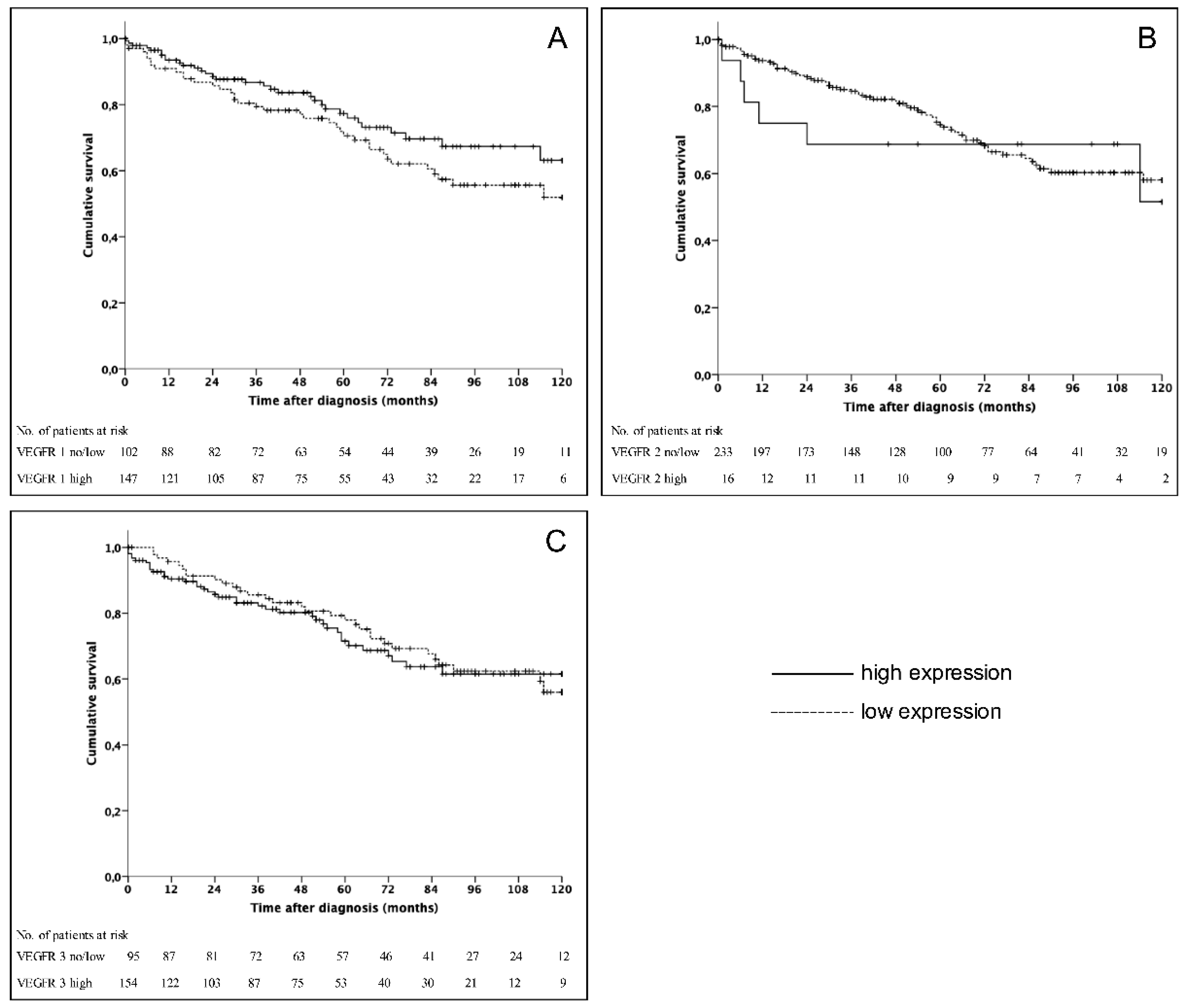
There was no significant association of the expression levels of VEGFR 1-3 and overall survival. Nonetheless, these results are in line with previous studies on other gastrointestinal malignancies [
35,
36]. This might in part be explained by the fact that well- to moderately differentiated GEP-NENs have a favorable overall survival even in the presence of distant metastases and that there was no significant correlation between tumor grading and the expression of VEGFRs. Furthermore, neuroendocrine carcinomas seem to have a different VEGF homeostasis [
15].
In our study VEGFR 1 and 3 were highly expressed in 59% and 61.8%, respectively, whereas only 6.4% of GEP-NENs showed VEGFR 2 positivity. Nonetheless, VEGFR 2 expression rates in GEP-NENs have been reported to be up to 60%. However, this study analyzed only 20 samples regarding the expression rate of VEGFR 2 [
37]. Studies on small intestine NENs and other tumor entities, such as leiomyoma and soft tissue sarcoma, revealed also a difference in the expression rates of the three VEGFR receptors [
24,
38,
39]. Moreover, since the majority of patients underwent surgery, a possible selection bias further influences the results additionally neglecting the potential influence of systemic treatment. Additionally, pNENs had a statistically significant higher expression of VEGFR 1 and 3 compared to other gastrointestinal NENs.
The formation of distant metastases of pNENs seems to be directly influenced by VEGF [
40]. Thus, a therapeutic approach inhibiting this pathway appears to be promising. Therefore, the multikinase inhibitor sunitinib and the monoclonal antibody bevacizumab have both been evaluated in clinical trials including patients with advanced pNENs [
41,
42]. Sunitinib, which irreversibly blocks tyrosine kinases such as VEGFR 2 and 3 and platelet-derived growth factor receptor (PDGFR), showed a prolonged progression free survival compared to placebo [
14]. Bevacizumab blocks binding to VEGFRs by specifically binding VEGF in the blood stream. Clinical trials demonstrated beneficial effects of bevacizumab in the treatment of pNENs [
30,
43,
44]. Taken together, the results of the present study may at least in part explain why GEP-NENs only in part response to anti-VEGF(R) therapy. Nonetheless, these findings also suggest that there is a specific population of GEP-NEN patients who will respond to a multikinase inhibitor therapy. Identification of benefitting subgroups might be feasible by immunohistochemistry as demonstrated.
Moreover, the identification of subgroups by using biomarkers is an evolving field in oncology and personalized therapy its goal [
8,
45]. Thus, staining for VEGFR seems to be a promising approach to detect patients who might profit from a multikinase inhibitor like pazopanib [
33], cabozantinib [
46,
47], lenvatinib [
46,
47] or a highly selective VEGFR inhibitor such as axitinib [
48]. However, up until now no specific VEGFR seems to be appropriate selecting patients for anti-angiogenic treatment. Axitinib is an orally bioavailable specific inhibitor of VEGFR 1-3 and currently approved for the therapy of advanced renal cell carcinoma. In a phase II study Strosberg et al. demonstrated antitumor activity of axitinib and a prolonged progression free survival of at least 14.6 months in patients with advanced GEP-NENs [
48]. However, this novel tyrosine kinase inhibitor was associated with a high rate of toxicity. Therefore, the results of the present study might help to stratify patients who most probably will benefit from a therapy with axitinib in a future study.
Recently it has been demonstrated in renal cell cancer that the combination of axitinib and the PD-1 inhibitor embrolizumab results in significantly longer survival rates compared to monotherapy with sunitinib [
49]. Treatment of GEP-NEN patients with immune checkpoint markers is currently under investigation and promising early results have been published [
23,
50]. Therefore, a further subject of the present analysis was to evaluate a potential coexpression of VEGFRs and immune checkpoint markers. It could be demonstrated that a high expression of PD-L1 is associated with VEGFR positivity in 9.8–25%. In this respect, further prospective studies are needed to evaluate a combination therapy approach in GEP-NEN patients by for example combining anti-VEGF compounds with anti-PD(L)-1 checkpoint inhibitors. Our data provide evidence that there may be a significant cross-talk between the VEGF/R and PD-1 pathway in GEP-NENs; this observation will add a scientific rationale for investigating combination approaches, as recently shown in hepatocellular carcinoma for the efficacy of the novel combination of bevacizumab and atezolizumab [
17]. Currently a phase II study (NCT03290079) is recruiting patients with advanced GEP-NENs analyzing the efficacy of the combination of the anti-angiogenic agent lenvatinib with the checkpoint inhibitor pembrolizumab. This combination therapy has already proofed to be beneficial in various solid tumors, such as renal cell carcinoma, endometrial cancer, and urothelial cancer [
16]. Moreover, the combination of Fosbretabulin, a compound in a class of agents termed vascular disrupting agents, with the approved Everolimus seems to be beneficial in the treatment of metastatic GEP-NEN patients in a phase 1 study [
51].
Although this is a retrospective analysis, the largest cohort of patients with GEP-NENs regarding the expression of VEGFR 1-3 could be analyzed. Moreover, more than 90% of the analyzed patients underwent surgery representing a selection bias. However, anti-angiogenic treatment is considered primarily for patients with advanced disease and these patients are most probably no candidates for surgical resection. Thus, the present findings have to be interpreted with caution. Due to the sample size and the comprehensive analysis, this study gives a proficient overview of GEP-NENs. Furthermore, since patients were included during 18 years, the understanding and therapy of GEP-NENs have changed. Moreover, not every patient included has been treated at the Ludwig-Maximilans-University Munich. Thus, data on medical treatment could not be considered for survival analyses.
In conclusion, within this study a large well-characterized patient collective was classified for the first time according to the expression levels of VEGFR 1-3 and correlated to clinicopathological parameters. However, there was no prognostic benefit of a VEGFR based classification in GEP-NENs. Nonetheless, the present study provides evidence that a combination therapy of immune checkpoint markers and VEGFR inhibitors might be a promising approach. However, further prospective studies are necessary to evaluate the possible stratification of GEP-NENs regarding VEGFRs and the clinical value.

 ,
, 

{kind=link}
{kind=link}