Cardiovascular Protection of Hydroxychloroquine in Patients with Sjögren’s Syndrome




Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
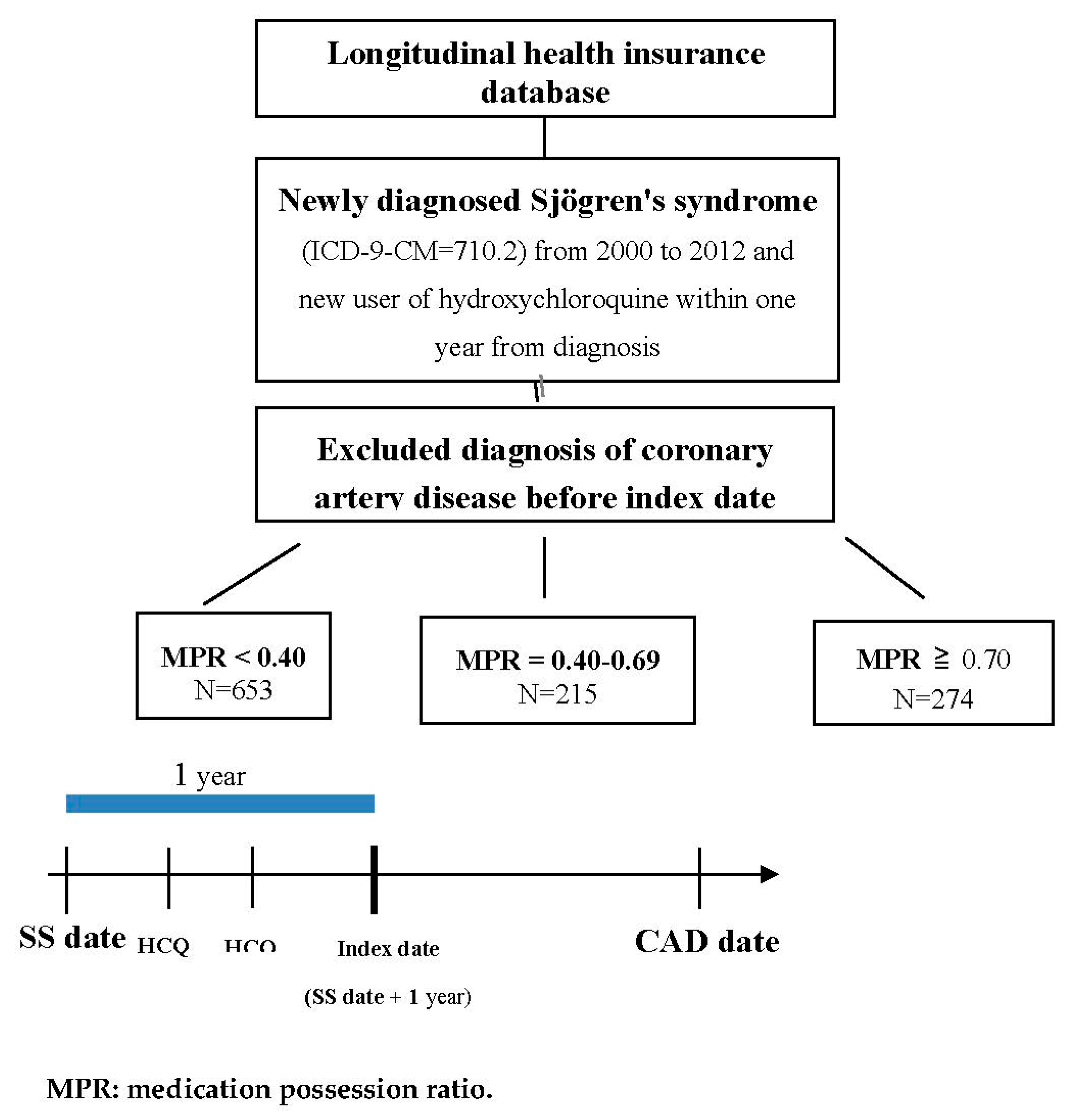
2.2. Study Population and Exposure
2.3. Outcome
2.4. Statistical Analysis
3. Results
3.1. Study Population
3.2. A Higher Incidence of CAD Developed in the SS Patients with a Lower MPR (<0.40) of HCQ, and There Was Significant Decreasing Cumulative Incidence of CAD in the SS Patients with a Higher MPR (≥0.70) of HCQ
3.3. Significant Cardiovascular Protection of HCQ in the 40–64 Age Group among the Patients with SS
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Mariette, X.; Criswell, L.A. Primary Sjogren’s Syndrome. N. Engl. J. Med. 2018, 378, 931–939. [Google Scholar] [CrossRef] [PubMed]
- Alunno, A.; Leone, M.C.; Giacomelli, R.; Gerli, R.; Carubbi, F. Lymphoma and Lymphomagenesis in Primary Sjogren’s Syndrome. Front. Med. 2018, 5, 102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartoloni, E.; Alunno, A.; Valentini, V.; Valentini, E.; La Paglia, G.C.M.; Leone, M.C.; Cafaro, G.; Marcucci, E.; Bonifacio, A.F.; Luccioli, F.; et al. The prevalence and relevance of traditional cardiovascular risk factors in primary Sjogren’s syndrome. Clin. Exp. Rheumatol. 2018, 36 (Suppl. 112), 113–120. [Google Scholar] [PubMed]
- Perez-De-Lis, M.; Akasbi, M.; Siso, A.; Diez-Cascon, P.; Brito-Zeron, P.; Diaz-Lagares, C.; Ortiz, J.; Perez-Alvarez, R.; Ramos-Casals, M.; Coca, A. Cardiovascular risk factors in primary Sjogren’s syndrome: A case-control study in 624 patients. Lupus 2010, 19, 941–948. [Google Scholar] [CrossRef] [PubMed]
- Yong, W.C.; Sanguankeo, A.; Upala, S. Association between primary Sjogren’s syndrome, arterial stiffness, and subclinical atherosclerosis: A systematic review and meta-analysis. Clin. Rheumatol. 2019, 38, 447–455. [Google Scholar] [CrossRef]
- Tully, P.J.; Harrison, N.J.; Cheung, P.; Cosh, S. Anxiety and Cardiovascular Disease Risk: A Review. Curr. Cardiol. Rep. 2016, 18, 120. [Google Scholar] [CrossRef]
- Wang, S.Q.; Zhang, L.W.; Wei, P.; Hua, H. Is hydroxychloroquine effective in treating primary Sjogren’s syndrome: A systematic review and meta-analysis. BMC Musculoskelet. Disord. 2017, 18, 186. [Google Scholar] [CrossRef] [Green Version]
- Gottenberg, J.E.; Ravaud, P.; Puéchal, X.; Le Guern, V.; Sibilia, J.; Goeb, V.; Larroche, C.; Dubost, J.J.; Rist, S.; Saraux, A.; et al. Effects of hydroxychloroquine on symptomatic improvement in primary Sjogren syndrome: The JOQUER randomized clinical trial. JAMA 2014, 312, 249–258. [Google Scholar] [CrossRef]
- Ammirati, E.; Bozzolo, E.P.; Contri, R.; Baragetti, A.; Palini, A.G.; Cianflone, D.; Banfi, M.; Uboldi, P.; Bottoni, G.; Scotti, I.; et al. Cardiometabolic and immune factors associated with increased common carotid artery intima-media thickness and cardiovascular disease in patients with systemic lupus erythematosus. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 751–759. [Google Scholar] [CrossRef]
- Yang, D.H.; Leong, P.Y.; Sia, S.K.; Wang, Y.H.; Wei, J.C.C. Long-Term Hydroxychloroquine Therapy and Risk of Coronary Artery Disease in Patients with Systemic Lupus Erythematosus. J. Clin. Med. 2019, 8, 796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rempenault, C.; Combe, B.; Barnetche, T.; Gaujoux-Viala, C.; Lukas, C.; Morel, J.; Hua, C. Metabolic and cardiovascular benefits of hydroxychloroquine in patients with rheumatoid arthritis: A systematic review and meta-analysis. Ann. Rheum. Dis. 2018, 77, 98–103. [Google Scholar] [CrossRef]
- Cai, X.; Luo, J.; Wei, T.; Qin, W.; Li, X.; Wang, X. Risk of Cardiovascular Involvement in Patients with Primary Sjogren’s Syndrome: A large-scale cross-sectional cohort study. Acta Reumatol. Port. 2019, 44, 71–77. [Google Scholar]
- Bartoloni, E.; Baldini, C.; Schillaci, G.; Quartuccio, L.; Priori, R.; Carubbi, F.; Bini, V.; Alunno, A.; Bombardieri, S.; De Vita, S.; et al. Cardiovascular disease risk burden in primary Sjogren’s syndrome: Results of a population-based multicentre cohort study. J. Intern. Med. 2015, 278, 185–192. [Google Scholar] [CrossRef]
- Zhang, Y.; Li, M.; Zhang, L.; Li, Q.; Yang, P.; Kong, X.; Duan, X.; Zhang, M.; Li, X.; Wang, Y.; et al. Association between comorbidities and extraglandular manifestations in primary Sjogren’s syndrome: A multicenter cross-sectional study. Clin. Rheumatol. 2020, 39, 2677–2688. [Google Scholar] [PubMed]
- Bartoloni, E.; Alunno, A.; Bistoni, O.; Caterbi, S.; Luccioli, F.; Santoboni, G.; Mirabelli, G.; Cannarile, F.; Gerli, R. Characterization of circulating endothelial microparticles and endothelial progenitor cells in primary Sjogren’s syndrome: New markers of chronic endothelial damage? Rheumatology 2015, 54, 536–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vassiliou, V.A.; Moyssakis, I.; Boki, K.A.; Moutsopoulos, H.M. Is the heart affected in primary Sjogren’s syndrome? An echocardiographic study. Clin. Exp. Rheumatol. 2008, 26, 109–112. [Google Scholar] [PubMed]
- Gerli, R.; Bartoloni Bocci, E.; Vaudo, G.; Marchesi, S.; Vitali, C.; Shoenfeld, Y. Traditional cardiovascular risk factors in primary Sjogren’s syndrome--role of dyslipidaemia. Rheumatology 2006, 45, 1580–1581. [Google Scholar] [CrossRef] [Green Version]
- Patrono, C. Cardiovascular effects of cyclooxygenase-2 inhibitors: A mechanistic and clinical perspective. Br. J. Clin. Pharmacol. 2016, 82, 957–964. [Google Scholar] [CrossRef]
- Ozen, G.; Pedro, S.; Michaud, K. The Risk of Cardiovascular Events Associated With Disease-modifying Antirheumatic Drugs in Rheumatoid Arthritis. J. Rheumatol. 2020. [Google Scholar] [CrossRef]
- Miranda, S.; Billoir, P.; Damian, L.; Thiebaut, P.A.; Schapman, D.; Le Besnerais, M.; Jouen, F.; Galas, L.; Levesque, H.; Le Cam-Duchez, V.; et al. Hydroxychloroquine reverses the prothrombotic state in a mouse model of antiphospholipid syndrome: Role of reduced inflammation and endothelial dysfunction. PLoS ONE 2019, 14, e0212614. [Google Scholar] [CrossRef]
- Chen, Y.M.; Lin, C.H.; Lan, T.H.; Chen, H.H.; Chang, S.N.; Chen, Y.H.; Wang, J.S.; Hung, W.T.; Lan, J.L.; Chen, D.Y. Hydroxychloroquine reduces risk of incident diabetes mellitus in lupus patients in a dose-dependent manner: A population-based cohort study. Rheumatology 2015, 54, 1244–1249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, S.J.; Wasko, M.C.M.; Antohe, J.L.; Sartorius, J.A.; Kirchner, H.L.; Dancea, S.; Bili, A. Hydroxychloroquine use associated with improvement in lipid profiles in rheumatoid arthritis patients. Arthritis Care Res. 2011, 63, 530–534. [Google Scholar] [CrossRef] [PubMed]
- Kerr, G.; Aujero, M.; Richards, J.; Sayles, H.; Davis, L.; Cannon, G.; Caplan, L.; Michaud, K.; Mikuls, T. Associations of hydroxychloroquine use with lipid profiles in rheumatoid arthritis: Pharmacologic implications. Arthritis Care Res. 2014, 66, 1619–1626. [Google Scholar] [CrossRef]
- Urbanski, G.; Caillon, A.; Poli, C.; Kauffenstein, G.; Begorre, M.A.; Loufrani, L.; Henrion, D.; Belizna, C. Hydroxychloroquine partially prevents endothelial dysfunction induced by anti-beta-2-GPI antibodies in an in vivo mouse model of antiphospholipid syndrome. PLoS ONE 2018, 13, e0206814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rainsford, K.D.; Parke, A.L.; Clifford-Rashotte, M.; Kean, W.F. Therapy and pharmacological properties of hydroxychloroquine and chloroquine in treatment of systemic lupus erythematosus, rheumatoid arthritis and related diseases. Inflammopharmacology 2015, 23, 231–269. [Google Scholar] [CrossRef] [PubMed]
- Fragoulis, G.E.; Zampeli, E.; Moutsopoulos, H.M. IgG4-related sialadenitis and Sjogren’s syndrome. Oral Dis. 2017, 23, 152–156. [Google Scholar] [CrossRef] [PubMed]
- Lanzillotta, M.; Mancuso, G.; Della-Torre, E. Advances in the diagnosis and management of IgG4 related disease. BMJ 2020, 369, m1067. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total | MPR < 0.40 (N = 653) | MPR = 0.40–0.69 (N = 215) | MPR ≥ 0.70 (N = 274) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | p | |
| Age | 0.891 | ||||||||
| <40 | 302 | 26.4 | 178 | 27.3 | 51 | 23.7 | 73 | 26.6 | |
| 40–64 | 677 | 59.3 | 384 | 58.8 | 131 | 60.9 | 162 | 59.1 | |
| ≥65 | 163 | 14.3 | 91 | 13.9 | 33 | 15.3 | 39 | 14.2 | |
| Mean ± SD | 49.5 ± 14.5 | 49.4 ± 14.4 | 49.8 ± 15.3 | 49.5 ± 13.9 | 0.935 | ||||
| Gender | 0.234 | ||||||||
| Female | 997 | 87.3 | 562 | 86.1 | 188 | 87.4 | 247 | 90.1 | |
| Male | 145 | 12.7 | 91 | 13.9 | 27 | 12.6 | 27 | 9.9 | |
| Hypertension | 143 | 12.5 | 89 | 13.6 | 29 | 13.5 | 25 | 9.1 | 0.149 |
| Hyperlipidemia | 79 | 6.9 | 51 | 7.8 | 19 | 8.8 | 9 | 3.3 | 0.022 |
| Diabetes | 68 | 6.0 | 35 | 5.4 | 19 | 8.8 | 14 | 5.1 | 0.139 |
| COPD | 22 | 1.9 | 15 | 2.3 | 2 | 0.9 | 5 | 1.8 | 0.445 |
| Stroke | 33 | 2.9 | 16 | 2.5 | 5 | 2.3 | 12 | 4.4 | 0.239 |
| Corticosteroids | 451 | 39.5 | 159 | 28.8 | 104 | 48.4 | 188 | 58.0 | <0.001 |
| NSAIDs | 787 | 68.9 | 434 | 66.5 | 149 | 69.3 | 204 | 74.5 | 0.056 |
| No. of CAD | Observed Person-Years | Incidence Density (Per 1000 Person-Years) | Crude HR | 95% C.I. | Adjusted HR † | 95% C.I. | |
|---|---|---|---|---|---|---|---|
| MPR of HCQ | |||||||
| <0.40 | 60 | 653 | 91.9 | 1 | 1 | ||
| 0.40–0.69 | 16 | 215 | 74.4 | 0.88 | 0.51–1.53 | 0.93 | 0.53–1.63 |
| ≥0.70 | 12 | 274 | 43.8 | 0.46 | 0.25–0.86 | 0.49 | 0.26–0.94 |
| Age | |||||||
| <40 | 8 | 1680 | 4.8 | 1 | 1 | ||
| 40–64 | 53 | 3270 | 16.2 | 3.37 | 1.60–7.10 | 2.99 | 1.41–6.35 |
| ≥65 | 27 | 624 | 43.3 | 8.93 | 4.04–19.7 | 4.69 | 1.99–11.03 |
| Gender | |||||||
| Female | 72 | 4850 | 14.8 | 1 | 1 | ||
| Male | 16 | 723 | 22.1 | 1.49 | 0.87–2.57 | 1.15 | 0.65–2.05 |
| Hypertension | |||||||
| No | 65 | 5071 | 12.8 | 1 | 1 | ||
| Yes | 23 | 502 | 45.8 | 3.49 | 2.16–5.65 | 1.98 | 1.17–3.36 |
| Hyperlipidemia | |||||||
| No | 74 | 5331 | 13.9 | 1 | 1 | ||
| Yes | 14 | 242 | 57.8 | 3.96 | 2.22–7.06 | 2.27 | 1.18–4.38 |
| Diabetes | |||||||
| No | 78 | 5327 | 14.6 | 1 | 1 | ||
| Yes | 10 | 246 | 40.6 | 2.70 | 1.39–5.22 | 1.41 | 0.69–2.89 |
| COPD | |||||||
| No | 81 | 5470 | 14.8 | 1 | 1 | ||
| Yes | 7 | 103 | 68.0 | 4.70 | 2.17–10.18 | 3.57 | 1.51–8.46 |
| Stroke | |||||||
| No | 83 | 5447 | 15.2 | 1 | 1 | ||
| Yes | 5 | 127 | 39.4 | 2.48 | 0.78–6.13 | 1.17 | 0.44–3.10 |
| Corticosteroids | |||||||
| No | 43 | 2926 | 14.7 | 1 | 1 | ||
| Yes | 45 | 2647 | 17.0 | 1.18 | 0.78–1.80 | 1.23 | 0.79–1.93 |
| NSAIDs | |||||||
| No | 10 | 831 | 12.0 | 1 | 1 | ||
| Yes | 78 | 4742 | 16.4 | 1.47 | 0.75–2.86 | 1.36 | 0.68–2.70 |
| N | No. of CAD | Crude HR | 95% C.I. | Adjusted HR † | 95% C.I. | |
|---|---|---|---|---|---|---|
| Age <40 † | ||||||
| MPR of HCQ | ||||||
| <0.40 | 178 | 7 | 1 | 1 | ||
| 0.40–0.69 | 51 | 1 | 0.48 | 0.06–3.88 | 0.40 | 0.05–3.49 |
| ≥0.70 | 73 | 0 | NA | NA | NA | NA |
| Age = 40–64 † | ||||||
| MPR of HCQ | ||||||
| <0.40 | 384 | 39 | 1 | 1 | ||
| 0.40–0.69 | 131 | 8 | 0.65 | 0.31–1.40 | 0.58 | 0.27–1.25 |
| ≥0.70 | 162 | 6 | 0.34 | 0.14–0.79 | 0.28 | 0.12–0.68 |
| Age ≥ 65 † | ||||||
| MPR of HCQ | ||||||
| <0.40 | 91 | 14 | 1 | 1 | ||
| 0.40–0.69 | 33 | 7 | 1.67 | 0.67–4.15 | 1.84 | 0.71–4.73 |
| ≥0.70 | 39 | 6 | 1.37 | 0.52–3.59 | 1.46 | 0.52–4.13 |
| Female ‡ | ||||||
| MPR of HCQ | ||||||
| <0.40 | 562 | 49 | 1 | 1 | ||
| 0.40–0.69 | 188 | 15 | 1.03 | 0.58–1.84 | 0.99 | 0.55–1.80 |
| ≥0.70 | 247 | 8 | 0.37 | 0.17–0.77 | 0.36 | 0.16–0.77 |
| Male ‡ | ||||||
| MPR of HCQ | ||||||
| <0.40 | 91 | 11 | 1 | 1 | ||
| 0.40–0.69 | 27 | 1 | 0.24 | 0.03–1.91 | 0.30 | 0.03–2.80 |
| ≥0.70 | 27 | 4 | 1.06 | 0.34–3.36 | 0.85 | 0.22–3.20 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, D.-H.; Wang, Y.-H.; Pan, L.-F.; Wei, J.C.-C. Cardiovascular Protection of Hydroxychloroquine in Patients with Sjögren’s Syndrome. J. Clin. Med. 2020, 9, 3469. https://doi.org/10.3390/jcm9113469
Yang D-H, Wang Y-H, Pan L-F, Wei JC-C. Cardiovascular Protection of Hydroxychloroquine in Patients with Sjögren’s Syndrome. Journal of Clinical Medicine. 2020; 9(11):3469. https://doi.org/10.3390/jcm9113469
Chicago/Turabian StyleYang, Deng-Ho, Yu-Hsun Wang, Lung-Fa Pan, and James Cheng-Chung Wei. 2020. "Cardiovascular Protection of Hydroxychloroquine in Patients with Sjögren’s Syndrome" Journal of Clinical Medicine 9, no. 11: 3469. https://doi.org/10.3390/jcm9113469
APA StyleYang, D.-H., Wang, Y.-H., Pan, L.-F., & Wei, J. C.-C. (2020). Cardiovascular Protection of Hydroxychloroquine in Patients with Sjögren’s Syndrome. Journal of Clinical Medicine, 9(11), 3469. https://doi.org/10.3390/jcm9113469