Single-Site Sutureless Partial Nephrectomy for Small Exophytic Renal Tumors

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient
2.2. Approach
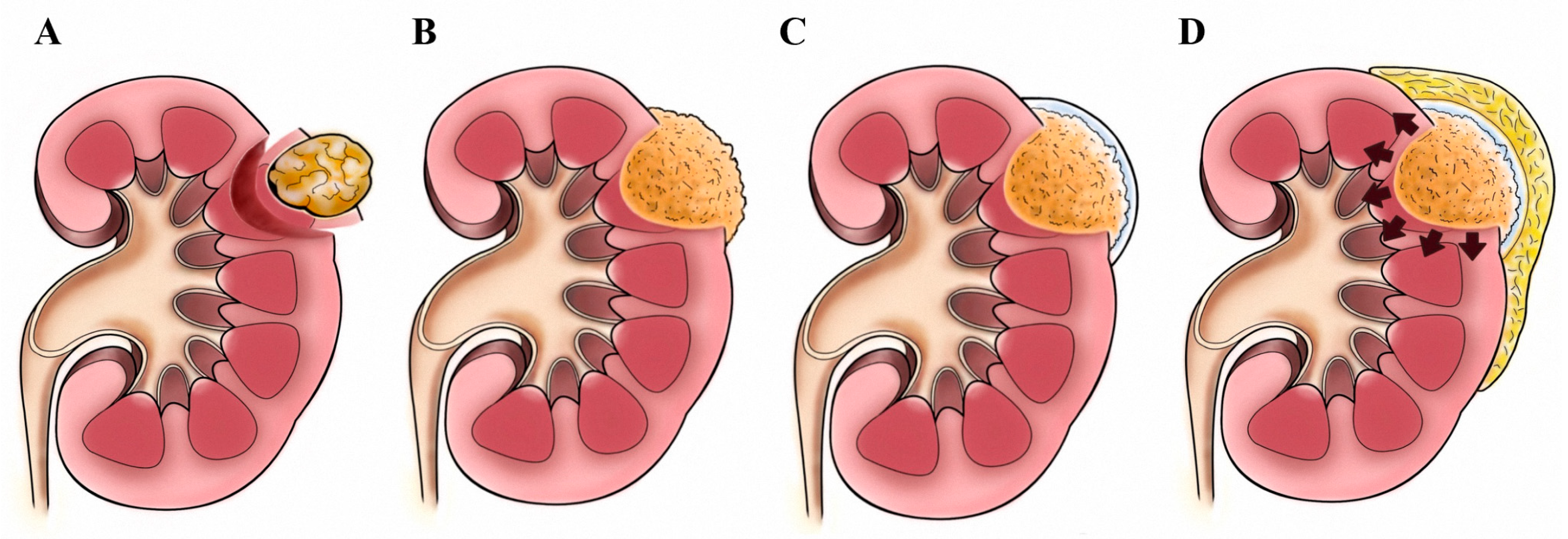
2.3. Tumor Excision: The “Pressure Cooker” Method
2.4. Statistical Methods
3. Results
3.1. Study Population
3.2. Surgical Outcomes
3.3. Histopathological Outcome
3.4. Renal Function and Hemoglobin Level
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Campbell, S.C.; Novick, A.C.; Belldegrun, A.; Blute, M.L.; Chow, G.K.; Derweesh, I.H.; Faraday, M.M.; Kaouk, J.H.; Leveillee, R.J.; Matin, S.F.; et al. Guideline for management of the clinical T1 renal mass. J. Urol. 2009, 182, 1271–1279. [Google Scholar] [CrossRef] [PubMed]
- Sorokin, I.; Feustel, P.J.; O’Malley, R.L. National utilization of partial nephrectomy pre- and post- AUA Guidelines: Is this as good as it gets? Clin. Genitourin. Cancer 2017, 15, 591–597. [Google Scholar] [CrossRef] [PubMed]
- Ljungberg, B.; Hanbury, D.C.; Kuczyk, M.A.; Merseburger, A.S.; Mulders, P.F.; Patard, J.J.; Sinescu, I.C. Renal cell carcinoma guideline. Eur. Urol. 2007, 51, 1502–1510. [Google Scholar] [CrossRef] [PubMed]
- Springer, C.; Hoda, M.R.; Fajkovic, H.; Pini, G.; Mohammed, N.; Fornara, P.; Greco, F. Laparoscopic vs open partial nephrectomy for T1 renal tumours: Evaluation of long-term oncological and functional outcomes in 340 patients. BJU Int. 2013, 111, 281–288. [Google Scholar] [CrossRef]
- Gill, I.S.; Abreu, S.C.; Desai, M.M.; Steinberg, A.P.; Ramani, A.P.; Ng, C.; Banks, K.; Novick ACKaouk, J.H. Laparoscopic ice slush renal hypothermia for partial nephrectomy: The initial experience. J. Urol. 2003, 170, 52–56. [Google Scholar] [CrossRef] [Green Version]
- Thompson, R.H.; Lane, B.R.; Lohse, C.M.; Leibovich, B.C.; Fergany, A.; Frank, I.; Gill, I.S.; Blute, M.L.; Campbell, S.C. Every minute counts when the renal hilum is clamped during partial nephrectomy. Eur. Urol. 2010, 58, 340–345. [Google Scholar] [CrossRef]
- Baumert, H.; Ballaro, A.; Shah, N.; Mansouri, D.; Zafar, N.; Molinié, V.; Neal, D. Reducing warm ischaemia time during laparoscopic partial nephrectomy: A prospective comparison of two renal closure techniques. Eur. Urol. 2007, 52, 1164–1169. [Google Scholar] [CrossRef]
- Peyronnet, B.; Baumert, H.; Mathieu, R.; Masson-Lecomte, A.; Grassano, Y.; Roumiguié, M.; Massoud, W.; Abd El Fattah, V.; Bruyère, F.; Droupy, S.; et al. Early unclamping technique during robot-assisted laparoscopic partial nephrectomy can minimise warm ischaemia without increasing morbidity. BJU Int. 2014, 114, 741–747. [Google Scholar] [CrossRef]
- Gill, I.S.; Eisenberg, M.S.; Aron, M.; Berger, A.; Ukimura, O.; Patil, M.B.; Campese, V.; Thangathurai, D.; Desai, M.M. “Zero ischemia” partial nephrectomy: Novel laparoscopic and robotic technique. Eur. Urol. 2011, 59, 128–134. [Google Scholar] [CrossRef]
- Dell’Atti, L.; Scarcella, S.; Manno, S.; Polito, M.; Galosi, A.B. Approach for renal tumors with low nephrometry score through unclamped sutureless laparoscopic enucleation technique: Functional and oncologic outcomes. Clin. Genitourin. Cancer 2018, 16, e1251–e1256. [Google Scholar] [CrossRef]
- Springer, C.; Veneziano, D.; Wimpissinger, F.; Inferrera, A.; Fornara, P.; Greco, F. Clampless laparoendoscopic single-site partial nephrectomy for renal cancer with low PADUA score: Technique and surgical outcomes. BJU Int. 2013, 111, 1091–1098. [Google Scholar] [CrossRef] [PubMed]
- Li, C.C.; Yeh, H.C.; Lee, H.Y.; Li, W.M.; Ke, H.L.; Hsu, A.H.S.; Lee, M.H.; Tsai, C.C.; Chueh, K.S.; Huang, C.N.; et al. Laparoscopic partial nephrectomy without intracorporeal suturing. Surg. Endosc. 2016, 30, 1585–1591. [Google Scholar] [CrossRef] [PubMed]
- Simone, G.; Papalia, R.; Guaglianone, S.; Gallucci, M. ‘Zero ischaemia’, sutureless laparoscopic partial nephrectomy for renal tumours with a low nephrometry score. BJU Int. 2012, 110, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Ota, T.; Komori, H.; Rii, J.; Ochi, A.; Suzuki, K.; Shiga, N.; Nishiyama, H. Soft coagulation in partial nephrectomy without renorrhaphy: Feasibility of a new technique and early outcomes. Int. J. Urol. 2014, 21, 244–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cindolo, L.; Berardinelli, F.; Gidaro, S.; Schips, L. Laparoendoscopic single-site partial nephrectomy without ischemia. J. Endourol. 2010, 24, 1997–2002. [Google Scholar] [CrossRef] [PubMed]
- Kihara, K.; Koga, F.; Fujii, Y.; Masuda, H.; Tatokoro, M.; Yokoyama, M.; Matsuoka, Y.; Numao, N.; Ishioka, J.; Saito, K. Gasless laparoendoscopic single-port clampless sutureless partial nephrectomy for peripheral renal tumors: Perioperative outcomes. Int. J. Urol. 2015, 22, 349–355. [Google Scholar] [CrossRef] [Green Version]
- Jain, S.; Nyirenda, T.; Yates, J.; Munver, R.J. Incidence of renal artery pseudoaneurysm following open and minimally invasive partial nephrectomy: A systematic review and comparative analysis. J. Urol. 2013, 189, 1643–1648. [Google Scholar] [CrossRef]
- Kutikov, A.; Uzzo, R.G. The, R.E.N.A.L. nephrometry score: A comprehensive standardized system for quantitating renal tumor size, location and depth. J. Urol. 2009, 182, 844–853. [Google Scholar] [CrossRef]
- McDougall, E.M.; Clayman, R.V.; Anderson, K. Laparoscopic wedge resection of a renal tumor: Initial experience. J. Laparoendosc. Surg. 1993, 3, 577–581. [Google Scholar] [CrossRef]
- Stifelman, M.D.; Caruso, R.P.; Nieder, A.M.; Taneja, S.S. Robot-assisted Laparoscopic Partial Nephrectomy. J. Soc. Laparoendosc. Surg. 2005, 9, 83–86. [Google Scholar]
- Ghani, K.R.; Sukumar, S.; Sammon, J.D.; Rogers, C.G.; Trinh, Q.D.; Menon, M. Practice patterns and outcomes of open and minimally invasive partial nephrectomy since the introduction of robotic partial nephrectomy: Results from the nationwide inpatient sample. J. Urol. 2014, 191, 907–912. [Google Scholar] [CrossRef] [PubMed]
- Hadjipavlou, M.; Khan, F.; Fowler, S.; Joyce, A.; Keeley, F.X.; Sriprasad, S. BAUS Sections of Endourology and Oncology. Partial vs radical nephrectomy for T1 renal tumours: An analysis from the British Association of Urological Surgeons Nephrectomy Audit. BJU Int. 2016, 117, 62–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leow, J.J.; Heah, N.H.; Chang, S.L.; Chong, Y.L.; Png, K.S. Outcomes of robotic versus laparoscopic partial nephrectomy: An updated meta-analysis of 4,919 patients. J. Urol. 2016, 196, 1371–1377. [Google Scholar] [CrossRef] [PubMed]
- Ploussard, G.; Haddad, R.; Loutochin, O.; Bera, R.; Cabrera, T.; Malibari, N.; Scarlata, E.; Derbekyan, V.; Bladou, F.; Anidjar, M. A combination of hemostatic agents may safely replace deep medullary suture during laparoscopic partial nephrectomy in a pig model. J. Urol. 2015, 193, 318–324. [Google Scholar] [CrossRef] [PubMed]
- Lipke, M.C.; Ha, S.P.; Fischer, C.D.; Rydberg, J.; Bonsib, S.M.; Sundaram, C.P. Pathologic characteristics of exophytic renal masses. J. Endourol. 2007, 21, 1489–1491. [Google Scholar] [CrossRef] [PubMed]
- Deng, J.; Li, L.; Xia, H.; Guo, J.; Wu, X.; Yang, X.; Hong, Y.; Chen, Q.; Hu, J. A comparison of the prognosis of papillary and clear cell renal cell carcinoma: Evidence from a meta-analysis. Medicine (Baltimore) 2019, 98, e16309. [Google Scholar] [CrossRef] [PubMed]
- Verma, S.K.; Mitchell, D.G.; Yang, R.; Roth, C.G.; O’Kane, P.; Verma, M.; Parker, L. Exophytic renal masses: Angular interface with renal parenchyma for distinguishing benign from malignant lesions at MR imaging. Radiology 2010, 255, 501–507. [Google Scholar] [CrossRef]
- Zhang, Z.; Zhao, J.; Dong, W.; Remer, E.; Li, J.; Demirjian, S.; Zabell, J.; Campbell, S.C. Acute kidney injury after partial nephrectomy: Role of parenchymal mass reduction and ischemia and impact on subsequent functional recovery. Eur. Urol. 2016, 69, 745–752. [Google Scholar] [CrossRef]
- Rosen, D.C.; Kannappan, M.; Paulucci, D.J.; Beksac, A.T.; Attalla, K.; Abaza, R.; Eun, D.D.; Bhandari, A.; Hemal, A.K.; Porter, J.; et al. Reevaluating warm ischemia time as a predictor of renal function outcomes after robotic partial nephrectomy. Urology 2018, 120, 156–161. [Google Scholar] [CrossRef]
- Lane, B.R.; Gill, I.S.; Fergany, A.F.; Larson, B.T.; Campbell, S.C. Limited warm ischemia during elective partial nephrectomy has only a marginal impact on renal functional outcomes. J. Urol. 2011, 185, 1598–1603. [Google Scholar] [CrossRef]
- Mir, M.C.; Pavan, N.; Parekh, D.J. Current paradigm for ischemia in kidney surgery. J. Urol. 2016, 195, 1655–1663. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Preoperative Variable | Total (N = 52) | Sutureless Group (N = 33) | Suture Group (N = 19) | p Value |
|---|---|---|---|---|
| Age (Mean ± SD), years | 57.1 ± 10.7 | 59.7 ± 11.1 | 52.5 ± 8.5 | 0.013 |
| Gender (female/male ratio) | 0.46 | 0.48 | 0.42 | 0.715 |
| BMI (Mean ± SD), kg/m2 | 26.8 ± 3.3 | 26.8 ± 3.2 | 26.7 ± 3.6 | 0.917 |
| Left/right kidney | 29/23 | 18/15 | 11/9 | 0.974 |
| ASA score (Mean ± SD) | 1.2 ± 0.4 | 1.2 ± 0.4 | 1.3 ± 0.5 | 0.366 |
| ECOG score (Mean ± SD) | 0.3 ± 0.4 | 0.3 ± 0.5 | 0.3 ± 0.4 | 0.751 |
| Tumor size (Mean ± SD), cm | 2.6 ± 1.1 | 2.7 ± 1.1 | 2.5 ± 1.0 | 0.538 |
| R.E.N.A.L. score (Mean ± SD) | 5.8 ± 1.5 | 5.7 ± 1.5 | 5.9 ± 1.7 | 0.626 |
| Preoperative eGFR, mL/min/m2 | 79.7 ± 21.1 | 76.6 ± 22.4 | 85.1 ± 18.1 | 0.146 |
| Preoperative hemoglobin, g/dL | 13.9 ± 1.4 | 13.9 ± 1.3 | 14.0 ± 1.5 | 0.884 |
| Intra-Operative and Postoperative Variable | Total (N = 52) | Sutureless Group (N = 33) | Suture Group (N = 19) | p Value |
|---|---|---|---|---|
| Operation time (Mean ± SD), min | 177.3 ± 40.9 | 167.9 ± 37.5 | 193.7 ± 42.5 | 0.035 |
| Renal artery control (clamped) | 45 (86.5%) | 27 (81.8%) | 18 (94.7%) | 0.189 |
| Warm ischemia time (Mean ± SD), min | 15.5 ± 7.1 | 11.8 ± 3.9 | 21.2 ± 7.2 | <0.001 |
| Blood loss (Mean ± SD), mL | 102.4 ± 97.2 | 104.0 ± 105.8 | 99.7 ± 83.6 | 0.881 |
| Transfusion | 3 (5.8%) | 1 (3.0%) | 2 (10.5%) | 0.264 |
| Conversion to conventional laparoscopy | 0 | 0 | 0 | |
| Hospital stay (Mean ± SD), day | 5.6 ± 1.3 | 5.6 ± 1.5 | 5.5 ± 1.6 | 0.848 |
| Postoperative eGFR, mL/min/m2 | 70.3 ± 25.2 | 69.6 ± 24.3 | 72.2 ± 21.8 | 0.340 |
| Postoperative hemoglobin, g/dL | 13.4 ± 1.4 | 13.3 ± 1.3 | 13.5 ± 1.5 | 0.642 |
| Skin incision (Mean ± SD), cm | 2.8 ± 1.2 | 2.8 ± 1.1 | 2.9 ± 1.4 | 0.771 |
| Histopathological Variable | Total (N = 52) | Sutureless Group (N = 33) | Suture Group (N = 19) |
|---|---|---|---|
| Clear cell RCC | |||
| pT1a | 22 (42.3%) | 14 (42.4%) | 8 (42.1%) |
| pT1b | 6 (11.5%) | 4 (12.1%) | 2 (10.5%) |
| Papillary RCC | |||
| pT1a | 5 (9.6%) | 3 (9.1%) | 2 (10.5%) |
| Chromophobe RCC | |||
| pT1a | 1 (1.9%) | 1 (3.0%) | 0 (0%) |
| Angiomyolipoma | 10 (19.2%) | 8 (24.2%) | 2 (10.5%) |
| Oncocytoma | 5 (9.6%) | 3 (9.1%) | 2 (10.5%) |
| Complications | |||
| Prolong urine leakage | 2 (3.8%) | 2 (6.1%) | 0 (0%) |
| Positive surgical margin | 2 (3.8%) | 2 (6.1%) | 0 (0%) |
| Cancer recurrence | 0 (0%) | 0 (0%) | 0 (0%) |
| Duration of follow-up (Mean ± SD), months | 29.3 ± 12.2 | 27.5 ± 10.4 | 35.2 ± 14.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, C.-C.; Chien, T.-M.; Huang, S.-P.; Yeh, H.-C.; Lee, H.-Y.; Ke, H.-L.; Wen, S.-C.; Chang, W.-C.; Juan, Y.-S.; Chou, Y.-H.; et al. Single-Site Sutureless Partial Nephrectomy for Small Exophytic Renal Tumors. J. Clin. Med. 2020, 9, 3658. https://doi.org/10.3390/jcm9113658
Li C-C, Chien T-M, Huang S-P, Yeh H-C, Lee H-Y, Ke H-L, Wen S-C, Chang W-C, Juan Y-S, Chou Y-H, et al. Single-Site Sutureless Partial Nephrectomy for Small Exophytic Renal Tumors. Journal of Clinical Medicine. 2020; 9(11):3658. https://doi.org/10.3390/jcm9113658
Chicago/Turabian StyleLi, Ching-Chia, Tsu-Ming Chien, Shu-Pin Huang, Hsin-Chih Yeh, Hsiang-Ying Lee, Hung-Lung Ke, Sheng-Chen Wen, Wei-Che Chang, Yung-Shun Juan, Yii-Her Chou, and et al. 2020. "Single-Site Sutureless Partial Nephrectomy for Small Exophytic Renal Tumors" Journal of Clinical Medicine 9, no. 11: 3658. https://doi.org/10.3390/jcm9113658