Reduced Kidney Function and Relative Hypocalciuria—Observational, Cross-Sectional, Population-Based Data

 , ,
, ,  , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Measurements in the Gubbio Study Dataset
2.2. Measurements in the Moli-Sani Study Dataset
2.3. Statistical Analyses
3. Results
3.1. Descriptive Statistics
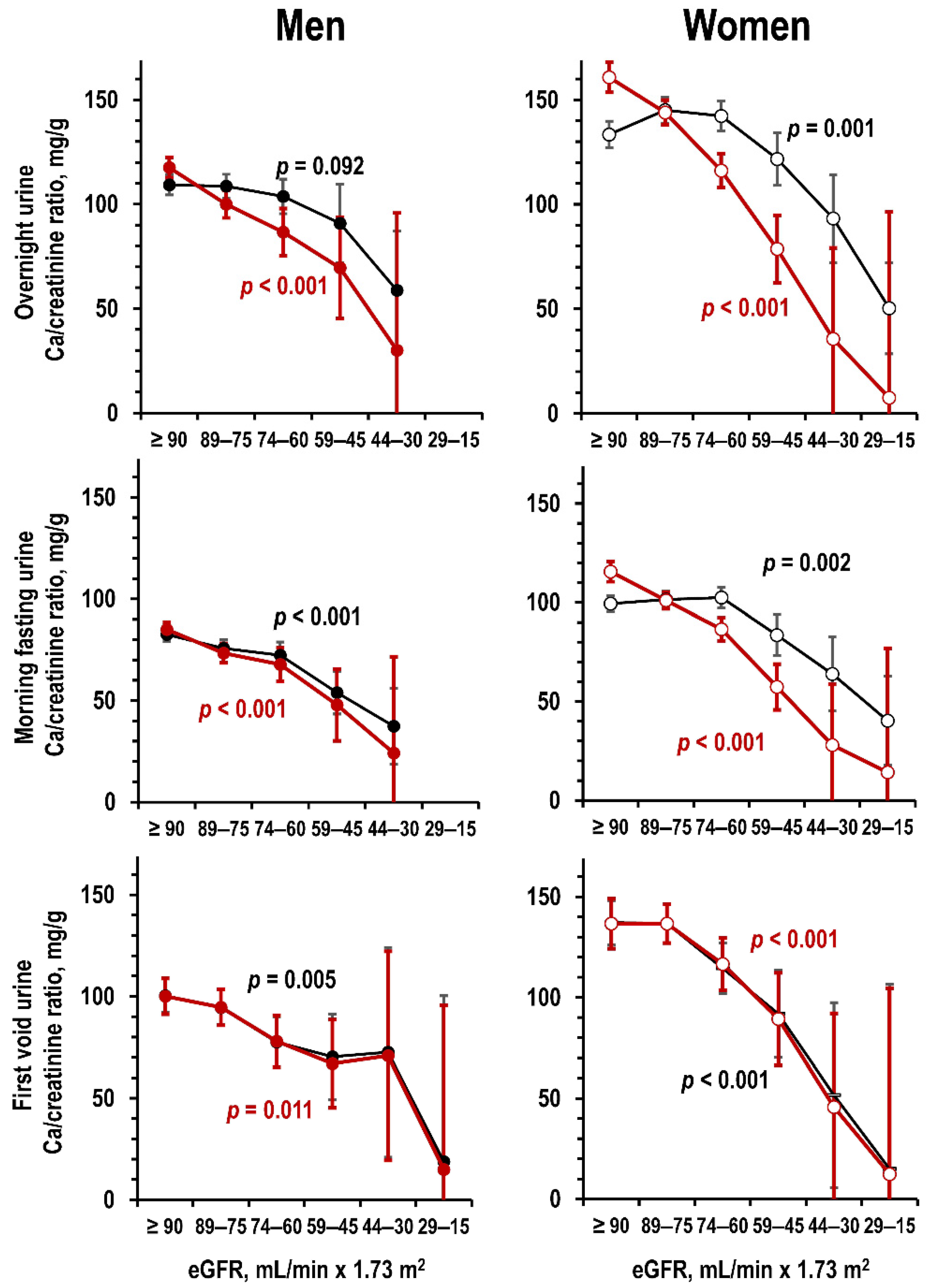
3.2. Kidney Function and Urine Ca
3.3. Kidney Function and Kidney Ca Handling
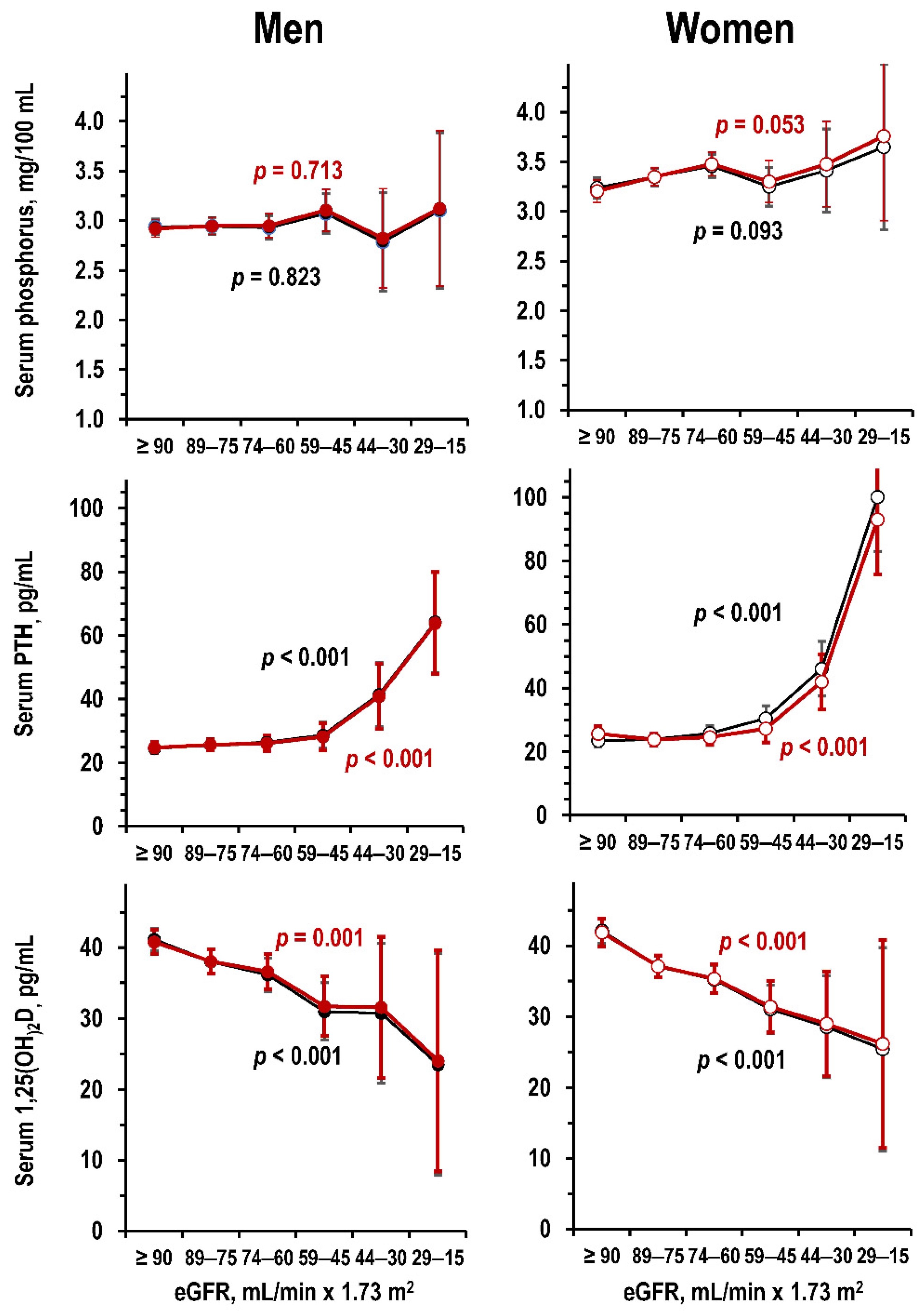
3.4. Kidney Function and Metabolic Markers of CKD-MBD
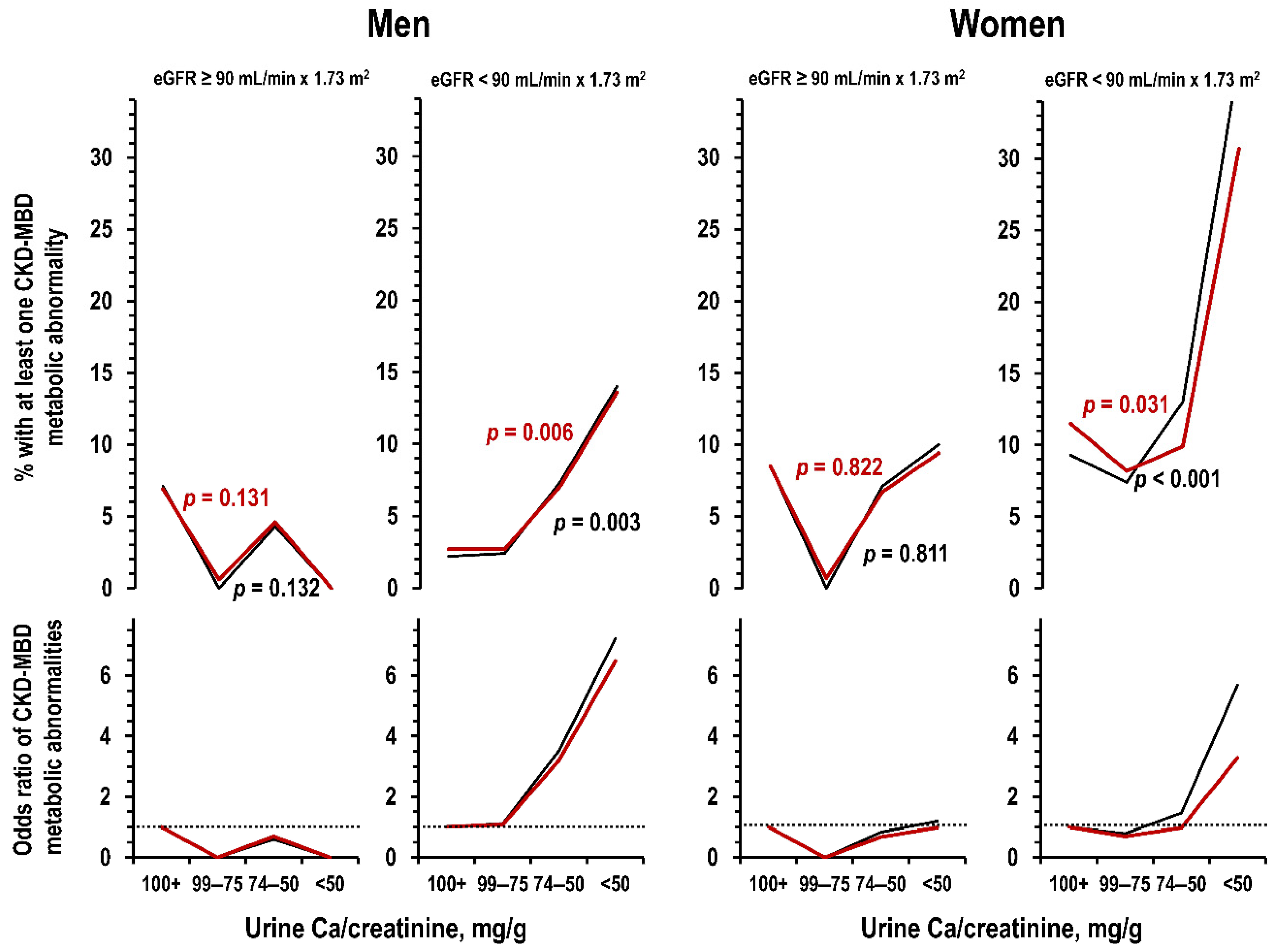
3.5. Urine Ca and CKD-MBD Metabolic Abnormalities
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD–MBD Work Group. KDIGO clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of chronic kidney disease–mineral and bone disorder (CKD–BD). Kidney Int. Suppl. 2009, 113, S1–S130. [Google Scholar] [CrossRef]
- Kestenbaum, B.; Drüeke, T.B. Disorders of calcium, phosphate, and magnesium metabolism. In Comprehensive Clinical Nephrology, 4th ed.; Floege, J., Johnson, R., Feehally, J., Eds.; Elsevier Saunders: St. Louis, MO, USA, 2010; Volume 1, pp. 130–148. [Google Scholar]
- Marco Mayayo, M.P.; Martínez, I.; Rué i Monné, M.; Borràs, M.; Martín Ramos, M.L.; Sarró, F.; Valdivielso Revilla, J.M.; Fernández i Giráldez, E. Mineral metabolism parameters throughout chronic kidney disease stages 1-5—Achievement of K/DOQI target ranges. Nephrol. Dial. Transplant. 2007, 22, 1171–1176. [Google Scholar] [CrossRef] [Green Version]
- Ramalho, J.; Petrillo, E.M.; Takeichi, A.P.M.; Moyses, R.M.A.; Titan, S.M. Calcitriol and FGF-23, but neither PTH nor sclerostin, are associated with calciuria in CKD. Int. Urol. Nephrol. 2019, 51, 1823–1829. [Google Scholar] [CrossRef] [PubMed]
- Kadlec, A.O.; Greco, K.A.; Fridirici, Z.C.; Gerber, D.; Turk, T.M.T. Effect of renal function on urinary mineral excretion and stone composition. Urology 2011, 78, 744–747. [Google Scholar] [CrossRef] [PubMed]
- Gershman, B.; Sheth, S.; Dretler, S.P.; Herrick, B.; Lang, K.; Pais, V.M., Jr.; Eisner, B.H. Relationship between glomerular filtration rate and 24-h urine composition in patients with nephrolithiasis. Urology 2012, 80, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Lemann, J., Jr.; Worcester, E.M.; Gray, R.W. Hypercalciuria and stones. Am. J. Kidney Dis. 1991, 17, 386–391. [Google Scholar] [CrossRef]
- Pak, C.Y.; Kaplan, R.; Bone, H.; Townsend, J.; Waters, O. A simple test for the diagnosis of absorptive, resorptive and renal hypercalciurias. N. Engl. J. Med. 1975, 292, 497–500. [Google Scholar] [CrossRef]
- Cirillo, M.; Terradura-Vagnarelli, O.; Mancini, M.; Menotti, A.; Zanchetti, A.; Laurenzi, M. Cohort profile: The Gubbio population study. Int. J. Epidemiol. 2014, 43, 713–720. [Google Scholar] [CrossRef] [Green Version]
- Cirillo, M.; Zingone, F.; Lombardi, C.; Cavallo, P.; Zanchetti, A.; Bilancio, G. Population-based dose-response curve of glomerular filtration rate to dietary protein intake. Nephrol. Dial. Transplant. 2015, 30, 1156–1162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cirillo, M.; Ciacci, C.; De Santo, N.G. Age, renal tubular phosphate reabsorption, and serum phosphate levels in adults. N. Engl. J. Med. 2008, 359, 864–866. [Google Scholar] [CrossRef] [PubMed]
- Myers, G.L.; Miller, W.G.; Coresh, J.; Fleming, J.; Greenberg, N.; Greene, T.; Hostetter, T.; Levey, A.S.; Panteghini, M.; Welch, M.; et al. Recommendations for improving serum creatinine measurement: A report from the Laboratory Working Group of the National Kidney Disease Education Program. Clin. Chem. 2006, 52, 5–18. [Google Scholar] [CrossRef] [PubMed]
- Di Castelnuovo, A.; Costanzo, S.; Persichillo, M.; Olivieri, M.; De Curtis, A.; Zito, F.; Donati, M.B.; De Gaetano, G.; Iacoviello, L. Distribution of short and lifetime risks for cardiovascular disease in Italians. Eur. J. Prev. Cardiol. 2012, 19, 723–730. [Google Scholar] [CrossRef] [PubMed]
- Iacoviello, L.; De Curtis, A.; Donati, M.B.; de Gaetano, G. Biobanks for cardiovascular epidemiology and prevention. Future Cardiol. 2014, 10, 243–254. [Google Scholar] [CrossRef] [PubMed]
- Zeller, T.; Hughes, M.; Tuovinen, T.; Schillert, A.; Conrads-Frank, A.; Den Ruijter, H.; Schnabel, R.B.; Kee, F.; Salomaa, V.; Siebert, U.; et al. BiomarCaRE: Rationale and design of the European BiomarCaRE project including 300,000 participants from 13 European countries. Eur. J. Epidemiol. 2014, 29, 777–790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cirillo, M.; Bilancio, G.; Guarino, E.; Cavallo, P.; Lombardi, C.; Costanzo, S.; De Curtis, A.; Di Castelnuovo, A.; Iacoviello, L. Vitamin D Status and indices of mineral homeostasis in the population: Differences between 25-hydroxyvitamin D and 1,25-dihydroxyvitamin D. Nutrients 2019, 11, 1777. [Google Scholar] [CrossRef] [Green Version]
- Pauli, D.; Seyfarth, M.; Dibbelt, L. The Abbott Architect c8000: Analytical performance and productivity characteristics of a new analyzer applied to general chemistry testing. Clin. Lab. 2005, 51, 31–41. [Google Scholar]
- Valcour, A.; Zierold, C.; Podgorski, A.L.; Olson, G.T.; Wall, J.V.; DeLuca, H.F.; Bonelli, F. A novel, fully-automated, chemiluminescent assay for the detection of 1,25-dihydroxyvitamin D in biological samples. J. Steroid. Biochem. Mol. Biol. 2016, 164, 120–126. [Google Scholar] [CrossRef] [Green Version]
- De la Hunty, A.; Wallace, A.M.; Gibson, S.; Viljakainen, H.; Lamberg-Allardt, C.; Ashwell, M. UK Food Standards Agency Workshop Consensus Report: The choice of method for measuring 25-hydroxyvitamin D to estimate vitamin D status for the UK National Diet and Nutrition Survey. Br. J. Nutr. 2010, 104, 612–619. [Google Scholar] [CrossRef] [Green Version]
- Phinney, K.W.; Bedner, M.; Tai, S.S.; Vamathevan, V.V.; Sander, L.C.; Sharpless, K.E.; Wise, S.A.; Yen, J.H.; Schleicher, R.L.; Chaudhary-Webb, M.; et al. Development and certification of a standard reference material for vitamin D metabolites in human serum. Anal. Chem. 2012, 84, 956–962. [Google Scholar] [CrossRef] [Green Version]
- ENEA—Italian National Agency for New Technologies, Energy and Sustainable Economic Development. Italian Atlas of Solar Irradiation. Available online: www.solaritaly.enea.it (accessed on 18 March 2018).
- Engelsen, O. The relationship between ultraviolet radiation exposure and vitamin D status. Nutrients 2010, 2, 482–495. [Google Scholar] [CrossRef] [Green Version]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.; Castro, A.F., III; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Gökçe, Ç.; Gökçe, Ö.; Baydinç, C.; Īlhan, N.; Alaşehirli, E.; Özküçük, F.; Taşçi, M.; Atikeler, M.K.; Çelebi, H.; Arslan, N. Use of random urine samples to estimate total urinary calcium and phosphate excretion. Arch. Intern. Med. 1991, 151, 1587–1588. [Google Scholar] [CrossRef] [PubMed]
- John, K.A.; Cogswell, M.E.; Campbell, N.R.; Nowson, C.A.; Legetic, B.; Hennis, A.J.; Patel, S.M. Accuracy and usefulness of select methods for assessing complete collection of 24-h urine: A systematic review. J. Clin. Hypertens. 2016, 18, 456–467. [Google Scholar] [CrossRef] [Green Version]
- He, J.; Klag, M.J.; Whelton, P.K.; Chen, J.Y.; Mo, J.P.; Qian, M.C.; Coresh, J.; Mo, P.S.; He, G.Q. Agreement between overnight and 24-h urinary cation excretions in southern Chinese men. Am. J. Epidemiol. 1993, 137, 1212–1220. [Google Scholar] [CrossRef] [PubMed]
- Cirillo, M.; Stellato, D.; Panarelli, P.; Laurenzi, M.; De Santo, N.G. Cross-sectional and prospective data on urinary calcium and urinary stone disease. Kidney Int. 2003, 63, 2200–2206. [Google Scholar] [CrossRef] [Green Version]
- Ix, J.H.; Wassel, C.L.; Stevens, L.A.; Beck, G.J.; Froissart, M.; Navis, G.; Rodby, R.; Torres, V.E.; Zhang, Y.L.; Greene, T.; et al. Equations to estimate creatinine excretion rate: The CKD Epidemiology Collaboration. Clin. J. Am. Soc. Nephrol. 2011, 6, 184–191. [Google Scholar] [CrossRef] [Green Version]
- Cirillo, M.; Cavallo, P.; Bilancio, G.; Lombardi, C.; Terradura Vagnarelli, O.; Laurenzi, M. Low protein intake in the population: Low risk of kidney function decline but high risk of mortality. J. Ren. Nutr. 2018, 28, 235–244. [Google Scholar] [CrossRef]
- Charles, P. Calcium absorption and calcium bioavailability. J. Intern. Med. 1992, 231, 161–168. [Google Scholar] [CrossRef]
- Inker, L.A.; Schmid, C.H.; Tighiouart, H.; Eckfeldt, J.H.; Feldman, H.I.; Greene, T.; Kusek, J.W.; Manzi, J.; Van Lente, F.; Zhang, Y.L.; et al. Estimating glomerular filtration rate from serum creatinine and cystatin C. N. Engl. J. Med. 2012, 367, 20–29. [Google Scholar] [CrossRef] [Green Version]
- Cirillo, M.; Lombardi, C.; Luciano, M.G.; Bilancio, G.; Anastasio, P.; De Santo, N.G. Estimation of GFR: A comparison of new and established equations. Am. J. Kidney Dis. 2010, 56, 802–804. [Google Scholar] [CrossRef]
- Besarab, A.; Caro, J.F. Increased absolute calcium binding to albumin in hypoalbuminaemia. J. Clin. Pathol. 1981, 34, 1368–1374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phelps, K.R.; Lieberman, R.L. Fractional excretion and reabsorption in chronic kidney disease. Clin. Nephrol. 2012, 77, 484–490. [Google Scholar] [CrossRef]
- Mayo Clinic Laboratories. Test Catalog. Available online: https://www.mayocliniclabs.com/test-catalog/ (accessed on 20 June 2019).
- National Kidney Foundation. K/DOQI Clinical practice guidelines for chronic kidney disease: Evaluation, classification and stratification. Am. J. Kidney Dis. 2002, 39 (Suppl. S1), S1–S266. [Google Scholar]
- Musgrove, J.; Wolf, M. Regulation and effects of FGF23 in chronic kidney disease. Annu. Rev. Physiol. 2020, 82, 365–390. [Google Scholar] [CrossRef] [Green Version]
- Inker, L.A.; Grams, M.E.; Levey, A.S.; Coresh, J.; Cirillo, M.; Collins, J.F.; Gansevoort, R.T.; Gutierrez, O.M.; Hamano, T.; Heine, G.H.; et al. Relationship of estimated GFR and albuminuria to concurrent laboratory abnormalities: An individual participant data meta-analysis in a global consortium. Am. J. Kidney Dis. 2019, 73, 206–217. [Google Scholar] [CrossRef] [PubMed]
- Levin, A.; Bakris, G.L.; Molitch, M.; Smulders, M.; Tian, J.; Williams, L.A.; Andress, D.L. Prevalence of abnormal serum vitamin D, PTH, calcium, and phosphorus in patients with chronic kidney disease: Results of the study to evaluate early kidney disease. Kidney Int. 2007, 71, 31–38. [Google Scholar] [CrossRef] [Green Version]
- John, A.S.; Thomas, M.B.; Davies, C.P.; Mullan, B.; Dick, I.; Hutchison, B.; van der Schaff, A.; Prince, R.L. Determinants of intact parathyroid hormone and free 1,25-dihydroxyvitamin D levels in mild and moderate renal failure. Nephron 1992, 61, 422–427. [Google Scholar] [CrossRef]
- Ishimura, E.; Nishizawa, Y.; Inaba, M.; Matsumoto, N.; Emoto, M.; Kawagishi, T.; Shoji, S.; Okuno, S.; Kim, M.; Miki, T.; et al. Serum levels of 1,25-dihydroxyvitamin D, 24,25-dihydroxyvitamin D, and 25-hydroxyvitamin D in nondialyzed patients with chronic renal failure. Kidney Int. 1999, 55, 1019–1027. [Google Scholar] [CrossRef] [Green Version]
- Isakova, T.; Gutierrez, O.; Shah, A.; Castaldo, L.; Holmes, J.; Lee, H.; Wolf, M. Postprandial mineral metabolism and secondary hyperparathyroidism in early CKD. J. Am. Soc. Nephrol. 2008, 19, 615–623. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gubbio Study | Moli-Sani Study | |||
|---|---|---|---|---|
| Men | Women | Men | Women | |
| Number of examinees | 1555 | 1953 | 488 | 467 |
| Demographics and anthropometry | ||||
| Age, years | 49.4 ± 16.8 | 51.0 ± 16.7 | 59.7 ± 9.6 | 59.9 ± 10.1 |
| Weight, kg | 77.0 ± 11.4 | 64.8 ± 11.3 | 80.8 ± 13.2 | 69.2 ± 13.3 |
| Body mass index, kg/m2 | 26.9 ± 3.7 | 26.6 ± 4.8 | 28.6 ± 4.2 | 28.7 ± 5.5 |
| Kidney function | ||||
| Serum creatinine, mg/100 mL | 0.96 (0.89/1.03) | 0.83 (0.77/0.89) | 0.88 (0.80/0.97) | 0.72 (0.66/0.80) |
| Serum cystatin C, mg/L | n.a. | n.a. | 0.99 (0.88/1.13) | 0.98 (0.87/1.10) |
| eGFR, mL/min × 1.73 m2 | 92.2 ± 15.7 | 83.4 ± 16.5 | 84.6 ± 15.6 | 81.5 ± 16.4 |
| % eGFR 89–60 mL/min × 1.73 m2 | 39.5% | 58.8% | 52.4% | 60.4% |
| % eGFR < 60 mL/min × 1.73 m2 | 2.3% | 6.5% | 7.5% | 9.8% |
| Urinary variables | ||||
| Estimated urinary creatinine, g/24 h | 1.54 ± 0.18 | 1.00 ± 0.16 | 1.52 ± 0.18 | 1.00 ± 0.17 |
| Overnight urine Ca, mg/L | 129 (92/182) | 121 (82/172) | n.a. | n.a. |
| Overnight urine creatinine, g/L | 1.44 (1.01/1.98) | 100 (67/150) | n.a. | n.a. |
| Overnight urine Ca/creatinine ratio, mg/g | 108 ± 68 | 139 ± 82 | n.a. | n.a. |
| Morning fasting urine Ca, mg/L ^ | 110 (76/147) | 102 (69/136) | n.a. | n.a. |
| Morning fasting urine creatinine, g/L ^ | 1.61 (1.14/2.14) | 118 (77/166) | n.a. | n.a. |
| Morning fasting urine Ca/creatinine ratio, mg/g ^ | 79 ± 48 | 100 ± 57 | n.a. | n.a. |
| First-void morning urine Ca, mg/L ^ | n.a. | n.a. | 42 (21/81) | 31 (15/59) |
| First-void morning urine creatinine, g/L ^ | n.a. | n.a. | 0.68 (0.32/1.13) | 0.31 (0.17/0.65) |
| First-void morning urine Ca/creatinine ratio, mg/g ^ | n.a. | n.a. | 92 ± 60 | 126 ± 68 |
| Kidney Ca handling | ||||
| Glomerular filtered Ca load, mg/min | n.a. | n.a. | 467 ± 85 | 446 ± 87 |
| Tubular fractional Ca reabsorption,% | n.a. | n.a. | 98.8 (98.1/99.2) | 98.5 (97.8/99.0) |
| Fractional Ca excretion,% | n.a. | n.a. | 1.21 (0.80/1.90) | 1.51 (0.98/2.20) |
| CKD-MBD metabolic markers | ||||
| Serum phosphorus, mg/100 mL | n.a. | n.a. | 2.94 ± 0.56 | 3.34 ± 0.61 |
| Serum PTH, pg/mL | n.a. | n.a. | 23.5 (17.9/30.4) | 23.0 (17.1/29.5) |
| Serum 1,25(OH)2D, pg/mL | n.a. | n.a. | 38.4 ± 11.6 | 37.5 ± 10.9 |
| Serum 25(OH)D, ng/mL | n.a. | n.a. | 22.2 ± 11.9 | 21.1 ± 12.8 |
| Serum total Ca, mg/100 mL | n.a. | n.a. | 9.35 ± 0.30 | 9.27 ± 0.30 |
| Serum albumin, g/L | n.a. | n.a. | 43.5 ± 2.6 | 43.1 ± 2.5 |
| Serum ultra-filterable Ca, mg/100 mL | n.a. | n.a. | 5.52 ± 0.16 | 5.48 ± 0.18 |
| Other variables | ||||
| % with Ca supplementation | 0.8% | 0.9% | 0.6% | 1.7% |
| % with vitamin D supplementation | 0.6% | 1.2% | 0.4% | 4.9% |
| Habitual intake of milk or yogurt, mL/day | 12 (0/125) | 63 (0/125) | n.a. | n.a. |
| Ending time of evening meal, hour:min | 20:30 (20:00/21:00) | 20:50 (20:00/21:00) | n.a. | n.a. |
| Duration of the overnight urine collection, h | 8.2 ± 1.1 | 8.3 ± 1.0 | n.a. | n.a. |
| Fast duration before morning fasting urine, h | 10.1 ± 1.2 | 10.2 ± 1.1 | n.a. | n.a. |
| Duration of morning fasting urine collection, min | 63 ± 26 | 68 ± 23 | n.a. | n.a. |
| Solar irradiance, MJ/m2 per day | n.a. | n.a. | 14.3 ± 6.7 | 14.9 ± 6.8 |
| Men | Women | |||||
|---|---|---|---|---|---|---|
| eGFR mL/min × 1.73 m2 | Odds Ratio (95%CI) | eGFR mL/min × 1.73 m2 | Odds Ratio (95%CI) | |||
| ≥90 | <90 | ≥90 | <90 | |||
| Number of examinees | 195 | 293 | 139 | 328 | ||
| Hyperphosphatemia, % | 2.1% | 0.7% | 0.33 (0.06/1.81) | 5.8% | 7.6% | 1.35 (0.59/3.07) |
| High serum PTH, % | 0.0% | 2.0% | n.c. | 0.7% | 2.4% | 3.45 (0.43/27.85) |
| Low serum 1,25(OH)2D, % | 2.1% | 3.8% | 1.86 (0.58/5.94) | 0.0% | 3.7% | n.c. |
| Hypocalcemia, % | 0.5% | 1.4% | 2.69 (0.30/24.2) | 0.7% | 0.6% | 0.85 (0.08/9.41) |
| Anyone of the above, % | 4.1% | 7.2% | 1.81 (0.78/4.16) | 7.2% | 13.4% | 2.00 (0.98/4.10) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cirillo, M.; Bilancio, G.; Cavallo, P.; Giordano, F.; Iesce, G.; Costanzo, S.; De Curtis, A.; Di Castelnuovo, A.; Iacoviello, L. Reduced Kidney Function and Relative Hypocalciuria—Observational, Cross-Sectional, Population-Based Data. J. Clin. Med. 2020, 9, 4133. https://doi.org/10.3390/jcm9124133
Cirillo M, Bilancio G, Cavallo P, Giordano F, Iesce G, Costanzo S, De Curtis A, Di Castelnuovo A, Iacoviello L. Reduced Kidney Function and Relative Hypocalciuria—Observational, Cross-Sectional, Population-Based Data. Journal of Clinical Medicine. 2020; 9(12):4133. https://doi.org/10.3390/jcm9124133
Chicago/Turabian StyleCirillo, Massimo, Giancarlo Bilancio, Pierpaolo Cavallo, Francesco Giordano, Gennaro Iesce, Simona Costanzo, Amalia De Curtis, Augusto Di Castelnuovo, and Licia Iacoviello. 2020. "Reduced Kidney Function and Relative Hypocalciuria—Observational, Cross-Sectional, Population-Based Data" Journal of Clinical Medicine 9, no. 12: 4133. https://doi.org/10.3390/jcm9124133
APA StyleCirillo, M., Bilancio, G., Cavallo, P., Giordano, F., Iesce, G., Costanzo, S., De Curtis, A., Di Castelnuovo, A., & Iacoviello, L. (2020). Reduced Kidney Function and Relative Hypocalciuria—Observational, Cross-Sectional, Population-Based Data. Journal of Clinical Medicine, 9(12), 4133. https://doi.org/10.3390/jcm9124133