Contemporary Speech and Oral Language Care for Deaf and Hard-of-Hearing Children Using Hearing Devices


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Contemporary Rehabilitation Approaches and Techniques
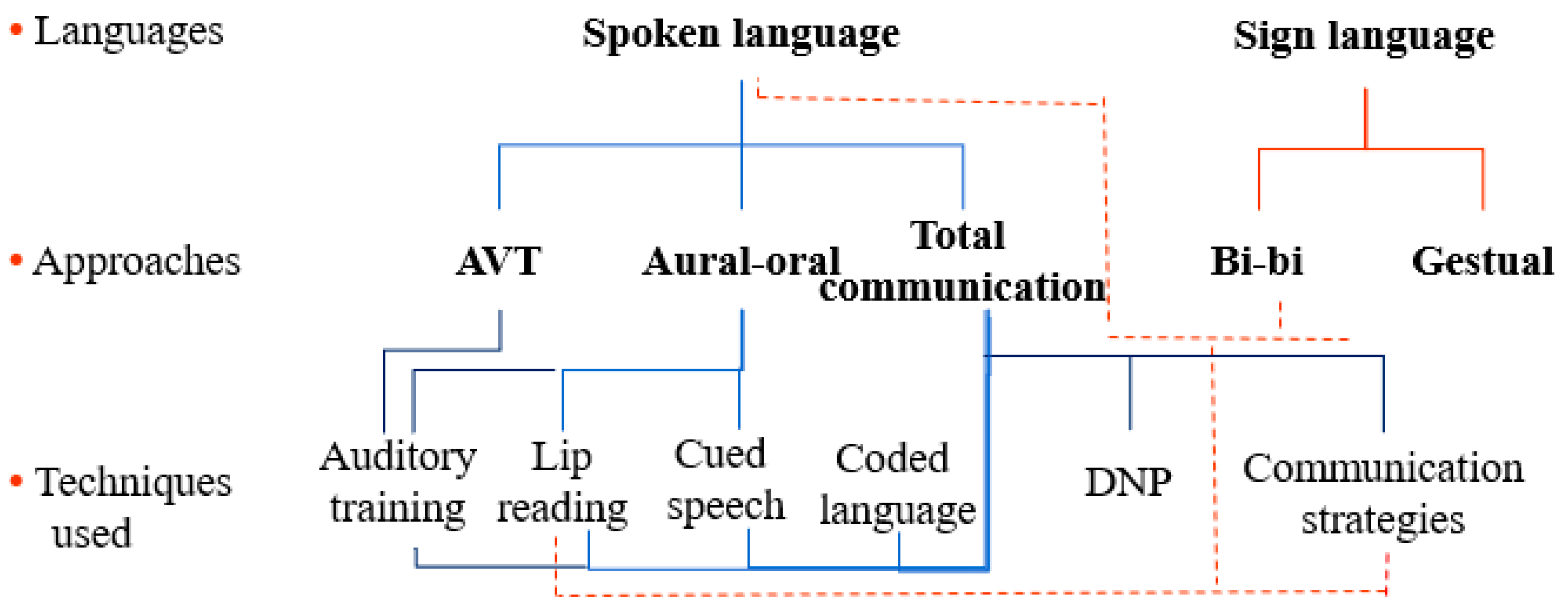
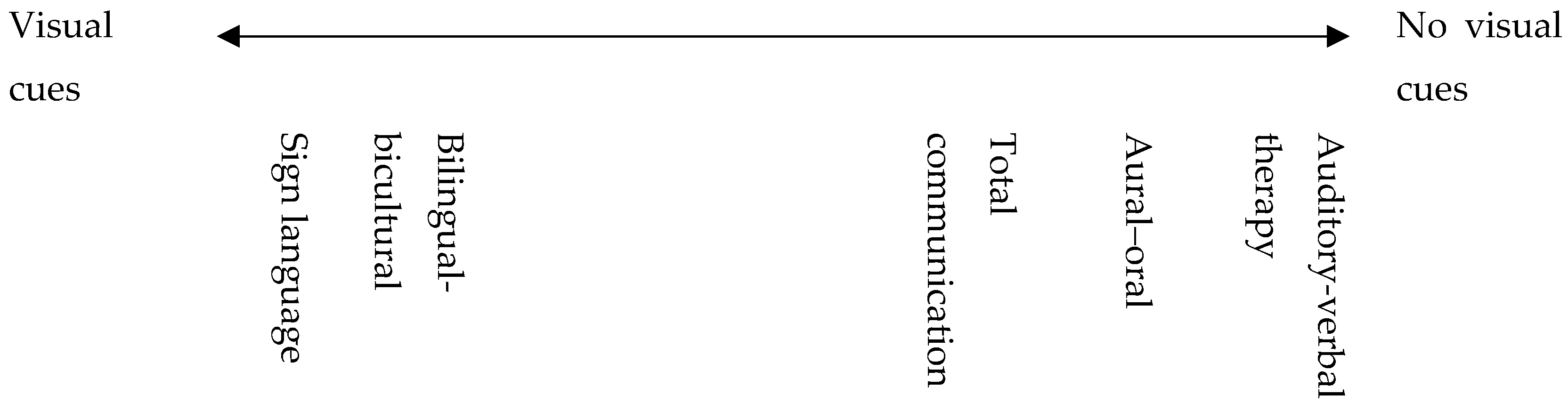
2.1. Approaches
2.1.1. Auditory-Verbal Therapy (AVT)
2.1.2. Aural–Oral Communication
2.1.3. Total Communication (TC)
2.1.4. Bilingual-Bicultural (Bi-Bi)
2.1.5. Sign Language
2.2. Techniques
2.2.1. Auditory Training
2.2.2. Lip-Reading
2.2.3. Cued Speech
2.2.4. Coded Language
2.2.5. Speech’s Natural Dynamic (Dynamique Naturelle De La Parole; DNP)
2.2.6. Other Communication Techniques
“… the communication between hearing families and their implanted deaf children evolves along a bipolar continuum whose two ends are oral communication alone vs a visual-gestural mode of communication alone [28]. In our population indeed, some families use the oral alone (but very often including some mimogestuality), others not using “official” sign language create conventional “house” or “family” signs [28], still others offer their child a spoken and signed linguistic environment (in our case, a “more or less signed”), others trained to cued speech use it more or less systematically, and more or less fluidly [29]. Oral language is thus the primary language used in all families (as found in hearing families of deaf children, [30]), but the target language offered by these families is very variable, and in fact, not so clear cut that it appears …”
2.3. Evidence of Efficacy
3. Clinical Rehabilitation Care of the Deaf and Hard-of-Hearing Child
3.1. Children Using Hearing Aids
3.2. Children Using Cochlear Implants
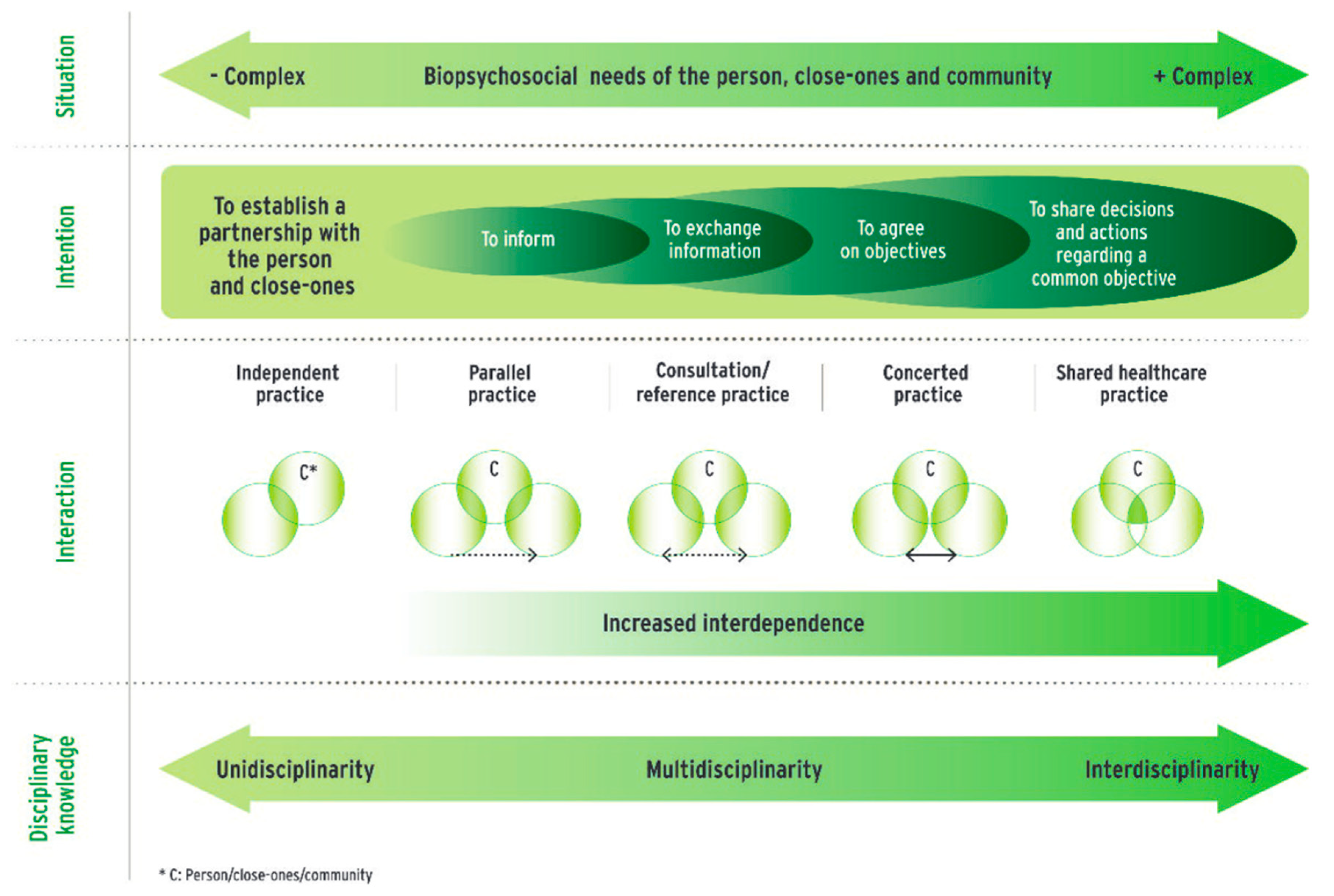
3.3. Interprofessional Collaboration
3.4. Variant Rehabilitation Care Models
- -
- The modalities of support for the child: in structure, the sessions are carried out in individual and/or small groups. Indeed, since services are most often specialized in early support, the children taken in may have similar needs, and peer group work is encouraged. The groups can be led by the speech therapist alone or with another professional (e.g., psychologist, psychomotor therapist, etc.). In the liberal exercise, work is most often carried out on an individual basis.
- -
- The type of follow-up of the child and his family: in a structure, multidisciplinary medical, para-medical and educational support is provided. Physician, paediatric nurse, psychologist, speech therapist, psychomotor therapist, specialized teacher, specialized educator, early childhood educator, sign language educator, cued speech coder and social worker are all professions that generally compose these teams. The technical platform may differ according to the institutions. At the end of an evaluation period, a personalized child project is carried out in collaboration with the entire team and the family. Depending on the identified needs of the child and his family, individual or small group rehabilitation sessions are offered: discovery of the sound environment, awakening and development, socialization, speech therapy, psychomotricity, educational workshops. In private practice, the professional sometimes carries the therapeutic project alone. If other liberal professionals follow the child, he can link with them, but collaboration is more complex. Moreover, early diagnosis implies that the speech therapist can welcome deaf babies from 3 to 4 months of age into his private practice. This change from the more traditional private practice work and require the speech and language therapist to be trained in early education [47].
4. Prospects for the Future
Author Contributions
Funding
Conflicts of Interest
References
- Cardon, G.; Campbell, J.; Sharma, A. Plasticity in the Developing Auditory Cortex: Evidence from Children with Sensorineural Hearing Loss and Auditory Neuropathy Spectrum Disorder. J. Am. Acad. Audiol. 2012, 23, 396–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang-Roth, R. Hearing impairment and language delay in infants: Diagnostics and genetics. GMS Curr. Top. Otorhinolaryngol. Head Neck Surg. 2014, 13, 1–31. [Google Scholar]
- Sarant, J.Z.; Holt, C.M.; Dowell, R.C.; Rickards, F.W.; Blamey, P.J. Spoken Language Development in Oral Preschool Children With Permanent Childhood Deafness. J. Deaf Stud. Deaf Educ. 2009, 14, 205–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jalilevand, N.; Ebrahimipour, M.; Zarandi, M.M.; Kamali, M.; Fayazi, L. Comparison of Verbal and Non-Verbal Communication Between Deaf Children with no Cochlear Implantation and Deaf Children 12–24 Months After Cochlear Implantation. Func. Disabil. J. 2018, 1, 1–7. [Google Scholar] [CrossRef]
- Hadjikakou, K.; Petridou, L.; Stylianou, C. The academic and social inclusion of oral deaf and hard-of-hearing children in Cyprus secondary general education: investigating the perspectives of the stakeholders. Eur. J. Special Needs Educ. 2008, 23, 17–29. [Google Scholar] [CrossRef]
- Marschark, M.; Shaver, D.M.; Nagle, K.N.; Newman, L.A. Predicting the Academic Achievement of Deaf and Hard-of-Hearing Students From Individual, Household, Communication, and Educational Factors. Except Child. 2015, 81, 350–369. [Google Scholar] [CrossRef] [Green Version]
- Engel-Yeger, B.; Hamed-Daher, S. Comparing participation in out of school activities between children with visual impairments, children with hearing impairments and typical peers. Res. Dev. Disabil. 2013, 34, 3124–3132. [Google Scholar] [CrossRef]
- Perkins-Dock, R.E.; Battle, T.R.; Edgerton, J.M.; McNeill, J.N. A Survey of Barriers to Employment for Individuals Who Are Deaf. ADARA 2015, 49, 66–85. [Google Scholar]
- Sharma, A.; Campbell, J.; Cardon, G. Developmental and cross-modal plasticity in deafness: Evidence from the P1 and N1 event related potentials in cochlear implanted children. Int. J. Psychophysiol. 2015, 95, 135–144. [Google Scholar] [CrossRef] [Green Version]
- Papsin, B.C.; Gordon, K.A. Cochlear Implants for Children with Severe-to-Profound Hearing Loss. Engl. J. Med. 2007, 357, 2380–2387. [Google Scholar] [CrossRef] [Green Version]
- Ching, T.Y.C.; Crowe, K.; Martin, V.; Day, J.; Mahler, N.; Youn, S.; Street, L.; Cook, C.; Orsini, J. Language development and everyday functioning of children with hearing loss assessed at 3 years of age. Int. J. Speech Lang Pathol. 2010, 12, 124–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruben, R.J. Language development in the pediatric cochlear implant patient. Laryngoscope Investig. Otolaryngol. 2018, 3, 209–213. [Google Scholar] [CrossRef] [PubMed]
- Punch, R.; Hyde, M. Social Participation of Children and Adolescents With Cochlear Implants: A Qualitative Analysis of Parent, Teacher, and Child Interviews. J. Deaf Stud. Deaf Educ. 2011, 16, 474–493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
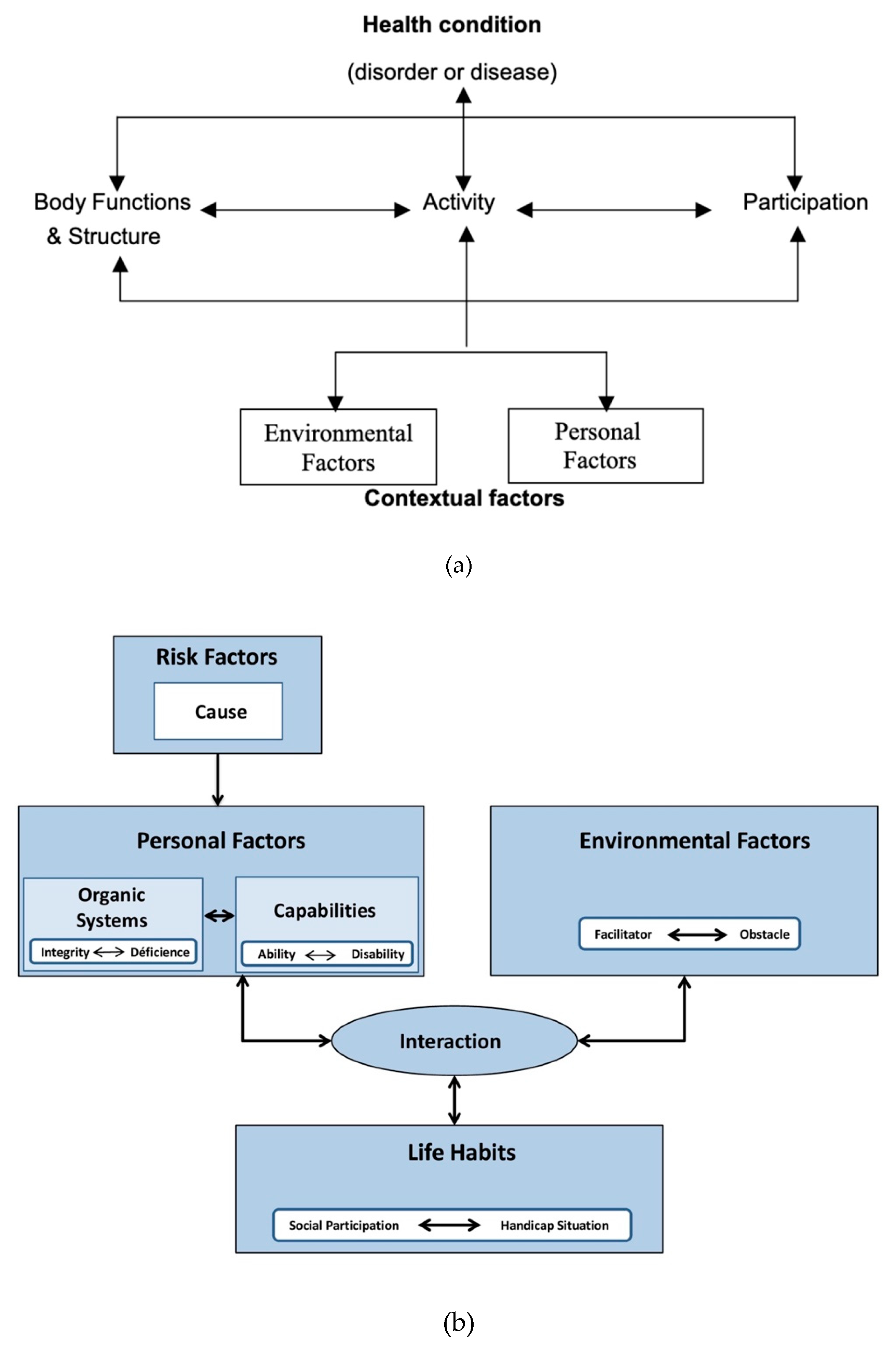
- World Health Organization. International Classification of Functioning, Disability, and Health; World Health Organization: Organization, 2001. [Google Scholar]
- Fougeyrollas, P. La funambule, le fil et la toile. Transformations réciproques du sens du handicap. Presses de l’Université Laval. 2010. (In French) [Google Scholar]
- Li, Y.; Bain, L.; Steinberg, A.G. Parental decision making and the choice of communication modality for the child who is deaf. Arch. Pediatr. Adolesc. Med. 2003, 157, 162–168. [Google Scholar] [CrossRef] [Green Version]
- Eleweke, C.J.; Rodda, M. Factors contributing to parents’ selection of a communication mode to use with their deaf children. Am. Ann. Deaf. 2000, 145, 375–383. [Google Scholar] [CrossRef]
- Mitchell, R.E.; Karchmer, M.A. Chasing the mythical ten percent: Parental hearing status of deaf and hard of hearing students in the United States. Sign Lang. Stud. 2004, 4, 138–163. [Google Scholar] [CrossRef]
- Gravel, J.S.; O’Gara, J. Communication Options for Children with Hearing Loss. Ment. Retard. Dev. Disabil. Res. Rev. 2003, 9, 243–251. [Google Scholar] [CrossRef] [Green Version]
- AG Bell Academy. AG Bell Academy LSLS Certification Handbook. 2017. Available online: https://agbellacademy.org/wp-content/uploads/2018/10/Certification-Handbook-1.pdf (accessed on 26 December 2019).
- Fortnum, H.M.; Marshall, D.H. Hearing-impaired children in the UK: Education setting and communication approach. Deafness Educ. Int. 2002, 4, 123–141. [Google Scholar] [CrossRef]
- Rayes, H.; Al-Malky, G.; Vickers, D. Systematic Review of Auditory Training in Pediatric Cochlear Implant Recipients. J. Speech Lang. Hear Res. 2019, 62, 1574–1593. [Google Scholar] [CrossRef] [Green Version]
- Sweetow, R.W.; Sabes, J.H. The need for and development of an adaptive listening and communication enchancement (LACETM) program. JAAA 2006, 17, 538–558. [Google Scholar] [CrossRef]
- Attina, V.; Beautemps, D.; Cathiard, M.A.; Odisio, M. A pilot study of temporal organization in Cued Speech production of French syllables: Rules for a Cued Speech synthesizer. Speech Commun. 2004, 44, 197–214. [Google Scholar] [CrossRef]
- National Cued Speech Association. Definition of Cued Speech. 2019. Available online: http://www.cuedspeech.org/cued-speech-definition (accessed on 26 December 2019).
- Dunoyer de Ségonzac, M. Pour que vibre la dynamique naturelle de la parole. 1991 Editions E. Robert. Lyon. (In French)
- Berland, A.; Cochard, N.; Calmels, M.-N.; Deguine, O.; Guidetti, M. Le développement du langage et de la communication chez le jeune enfant sourd: Trajectoires développementales avant et après implantation cochléaire. ANAE 2015, 138, 1–12. (In French) [Google Scholar]
- Lepot-Froment, C. Chapitre 7. L’acquisition d’une langue des signes: Données empiriques et questions apparentées. In L’acquisition du Langage; Kail, M., Ed.; Presses Universitaires de France Psychologie et sciences de la pensée: Paris, France, 2000; pp. 193–229. (In French) [Google Scholar]
- Bardin, S.; Racine, E. Nina, fête son anniversaire! Participation à la création d’un livre numérique codé en L.P.C. destiné aux enfants sourds de cycle 1 et à leurs parents. Master’s Thesis, Ecole d’orthophonie de Nancy, Nancy, France, 2010. (In French). [Google Scholar]
- Tomblin, J.B.; Barker, B.A.; Spencer, L.J.; Zhang, X.; Gantz, B.J. The effect of age at cochlear implant initial stimulation on expressive language growth in infants and toddlers. J. Speech Lang. Hear. Res. 2005, 48, 853–867. [Google Scholar] [CrossRef] [Green Version]
- Demers, D.; Bergeron, F. Effectiveness of Rehabilitation Approaches Proposed to Children with Severe-to-Profound Prelinguistic Deafness on the Development of Auditory, Speech, and Language Skills: A Systematic Review. J. Speech Lang. Hear. Res. 2019, 62, 4196–4230. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, E.M.; Hamel, C.; Stevens, A.; Pratt, M.; Moher, D.; Doucet, S.P.; Na, E. Sign Language and Spoken Language for Children with Hearing Loss: A Systematic Review. Pediatrics 2016, 137, 1–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaipa, R.; Danser, M.L. Efficacy of Auditory-Verbal Therapy in Children with Hearing Impairment: A Systematic Review from 1993 to 2015. Int. J. Pediatr. Otorhinolaryngol. 2016, 86, 124–134. [Google Scholar] [CrossRef] [PubMed]
- Brennan-Jones, C.G.; White, J.; Rush, R.W.; La, J. Auditory-verbal therapy for promoting spoken language development in children with permanent hearing impairments. Cochrane Database Syst. Rev. 2014, 3. [Google Scholar] [CrossRef] [Green Version]
- Joint Committee on Infant Hearing (JCIH). Year 2019 Position Statement: Principles and Guidelines for Early Hearing Detection and Intervention Programs. JEHDI 2019, 4, 2–37. [Google Scholar]
- Brouns, A.; Refaie, E.L.; Pryce, H. Auditory training and adult rehabilitation: A critical review of the evidence. Glob. J. Health Sci. 2011, 3, 49–63. [Google Scholar] [CrossRef]
- Kyle, F.E.; Harris, M. Concurrent correlates and predictors of reading and spelling achievement in deaf and hearing school children. J. Deaf Stud. Deaf Educ. 2006, 11, 273–288. [Google Scholar] [CrossRef] [Green Version]
- Kyle, F.E.; Harris, M. Predictors of reading development in deaf children: A 3-year longitudinal study. J. Exp. Child Psychol. 2010, 107, 229–243. [Google Scholar] [CrossRef] [PubMed]
- Kyle, F.E.; Campbell, R.; MacSweeney, M. The relative contributions of speechreading and vocabulary to deaf and hearing children’s reading ability. Res. Dev. Disabil. 2016, 48, 13–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, M.; Terlektsi, E.; Kyle, F.E. Concurrent and Longitudinal Predictors of Reading for Deaf and Hearing Children in Primary School. J. Deaf Stud. Deaf Educ. 2017, 22, 233–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- LaSasso, C.; Crain, K.; Leybaert, J. Rhyme generation in deaf students: The effect of exposure to cued speech. J. Deaf Stud. Deaf Educ. 2003, 8, 250–270. [Google Scholar] [CrossRef] [PubMed]
- Leybaert, J.; Colin, C. Le rôle des informations visuelles dans le développement du langage de l’enfant sourd muni d’un implant cochléaire. Enfance 2007, 59, 245–253. [Google Scholar] [CrossRef] [Green Version]
- Bouton, S.; Bertoncini, J.; Serniclaes, W.; Colé, P. Reading and reading-related skills in children using cochlear implants: Prospects for the influence of cued speech. J. Deaf Stud. Deaf Educ. 2011, 16, 458–473. [Google Scholar] [CrossRef]
- Colin, S.; Ecalle, J.; Truy, E.; Lina-Granade, G.; Magnan, A. Effect of age at cochlear implantation and at exposure to Cued Speech on literacy skills in deaf children. Res. Dev. Disabil. 2017, 71, 61–69. [Google Scholar] [CrossRef]
- Bergeron, F.; Berland, A.; Fitzpatrick, E.; Vincent, C.; Giasson, A.; Cloutier, D.; Tremblay, G.; Hotton, M.; Leung Kam, K.; Puel, J.L.; et al. An Ecological Approach to Assess Auditory Perception. Can. Acoust. 2016, 44(3), 216–217. [Google Scholar]
- Careau, E.; Brière, N.; Houle, N.; Dumont, S.; Maziade, J.; Paré, L.; Desaulniers, M.; Museux, A.-C. Continuum of Interprofessional CollaborativePractice in Health and Social Care—Guide; RCPI: Dublin, Ireland, 2014; rev 2018. (In French) [Google Scholar]
- Toffin, C.; Alis-Salamanca, V. Le bébé sourd, sa famille et l’orthophoniste. Contraste 2014, 39, 239–263. (In French) [Google Scholar] [CrossRef]
- Marschark, M.; Antia, S.; Knoors, H. Co-Enrollment in Deaf Education; Oxford university Press: Oxford, UK, 2019. [Google Scholar]
- Haute Autorité de la Santé—HAS. Surdité de l’enfant: Accompagnement des familles et suivi de l’enfant de 0 à 6 ans. 2009. Available online: http://www.has-sante.fr/portail/upload/docs/application/pdf/2010-03/surdite_de_lenfant_-_0_a_6_ans_-_recommandations.pdf (accessed on 26 December 2019).
- Wavreille, F.; Hébrard, N.; Hyman, C.; Laurent, K.; Tombel, V. Les troubles expressifs sont-ils spécifiques à une pathologie? Cas de la dysphasie et de la surdité. Entretiens d’Orthophonie 2012, 160–178. (In French) [Google Scholar]
- Fédération Nationale des Etudiants en Orthophonie—FNEO. Synthèse de l’installation des néo-diplômés. 2019. Available online: http://www.fneo.fr/wp-content/uploads/2019/11/Synthèse-installation-2019 (accessed on 26 December 2019).
- Fédération Nationale des Orthophonistes—FNO. Les orthophonistes: Données statistiques. 2019. Available online: https://www.fno.fr/wp-content/uploads/2019/01/Drees-2019.pdf (accessed on 26 December 2019).
- UNIFAF. Enquête emploi, Secteur des activités sanitaires, sociales et médico-sociales privé à but non-lucratif. 2017. Available online: https://enquete-emploi.unifaf.fr/files/2018-03/1522164696_20180322-unifaf-enqueteemploi17.pdf?43a2b5c466 (accessed on 26 December 2019).
- Ministère de l’Education Nationale, Circulaire de rentrée 2019 -École inclusive. 2019. Available online: http://cache.media.education.gouv.fr/file/Actualites/03/3/Circulaire-de-rentree-2019-ecole-inlusive_1136033.pdf (accessed on 26 December 2019).
- Centre national de ressources handicaps rares à composantes (CNRHR). Les enfants sourds qui présentent des déficiences associées à leur surdité. Available online: https://www.cnrlaplane.fr/enfants-sourds-deficiences-associees (accessed on 26 December 2019).
- Clavier, N. L’enquête scolarité de Génération Cochlée. Connaissances surdités. 2012, 39, 19–22. (In French) [Google Scholar]
- Sorkin, D.L.; Zwolan, T.A. Trends in educational services for children with cochlear implants. Int. Cong. 2004, 1273, 417–421. [Google Scholar] [CrossRef]
- Sanchez, J.; Medina, V.; Senpéré, M.; Bounot, A. Suivi longitudinal sur 10 ans d’enfants sourds pré-linguaux implantés et appareillés. Premier rapport Global à 5 ans. 2006. (In French) [Google Scholar]
- Giezen, M. Speech and sign perception in deaf children with cochlear implants (English summary of thesis in Dutch). Sign Lang. Linguist. 2011, 14, 277–283. [Google Scholar] [CrossRef]
- Flory, D. Nouvelles technologies et grande iconicité en Langue des signes: l’exemple d’un site éducatif et pédagogique inclusif. La nouvelle revue de l’adaptation et de la scolarisation 2019, 2, 119–133. (In French) [Google Scholar] [CrossRef]



© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bergeron, F.; Berland, A.; Demers, D.; Gobeil, S. Contemporary Speech and Oral Language Care for Deaf and Hard-of-Hearing Children Using Hearing Devices. J. Clin. Med. 2020, 9, 378. https://doi.org/10.3390/jcm9020378
Bergeron F, Berland A, Demers D, Gobeil S. Contemporary Speech and Oral Language Care for Deaf and Hard-of-Hearing Children Using Hearing Devices. Journal of Clinical Medicine. 2020; 9(2):378. https://doi.org/10.3390/jcm9020378
Chicago/Turabian StyleBergeron, François, Aurore Berland, Dominique Demers, and Suzie Gobeil. 2020. "Contemporary Speech and Oral Language Care for Deaf and Hard-of-Hearing Children Using Hearing Devices" Journal of Clinical Medicine 9, no. 2: 378. https://doi.org/10.3390/jcm9020378
APA StyleBergeron, F., Berland, A., Demers, D., & Gobeil, S. (2020). Contemporary Speech and Oral Language Care for Deaf and Hard-of-Hearing Children Using Hearing Devices. Journal of Clinical Medicine, 9(2), 378. https://doi.org/10.3390/jcm9020378