Associations between Depressive Symptoms and Satisfaction with Meaningful Activities in Community-Dwelling Japanese Older Adults

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
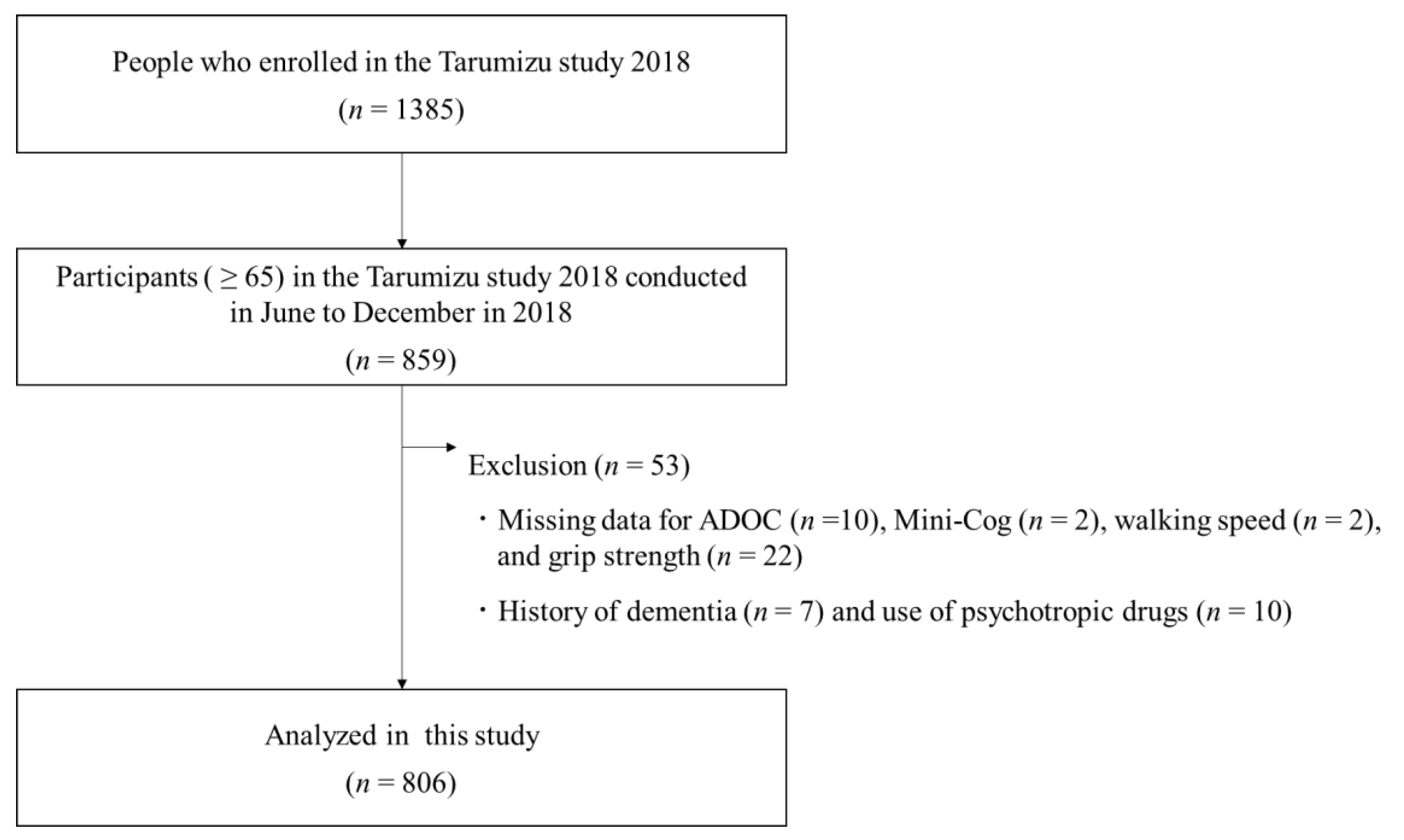
2.1. Study Population
2.2. Measures
2.2.1. Depressive Symptoms
2.2.2. Meaningful Activities
2.2.3. Covariates
2.3. Statistical Analysis
2.3.1. Association between Depressive Symptoms and Meaningful Activity Categories by Gender
2.3.2. Association between Depressive Symptoms, Satisfaction, and Performance
3. Results
3.1. Characteristics of the Participants
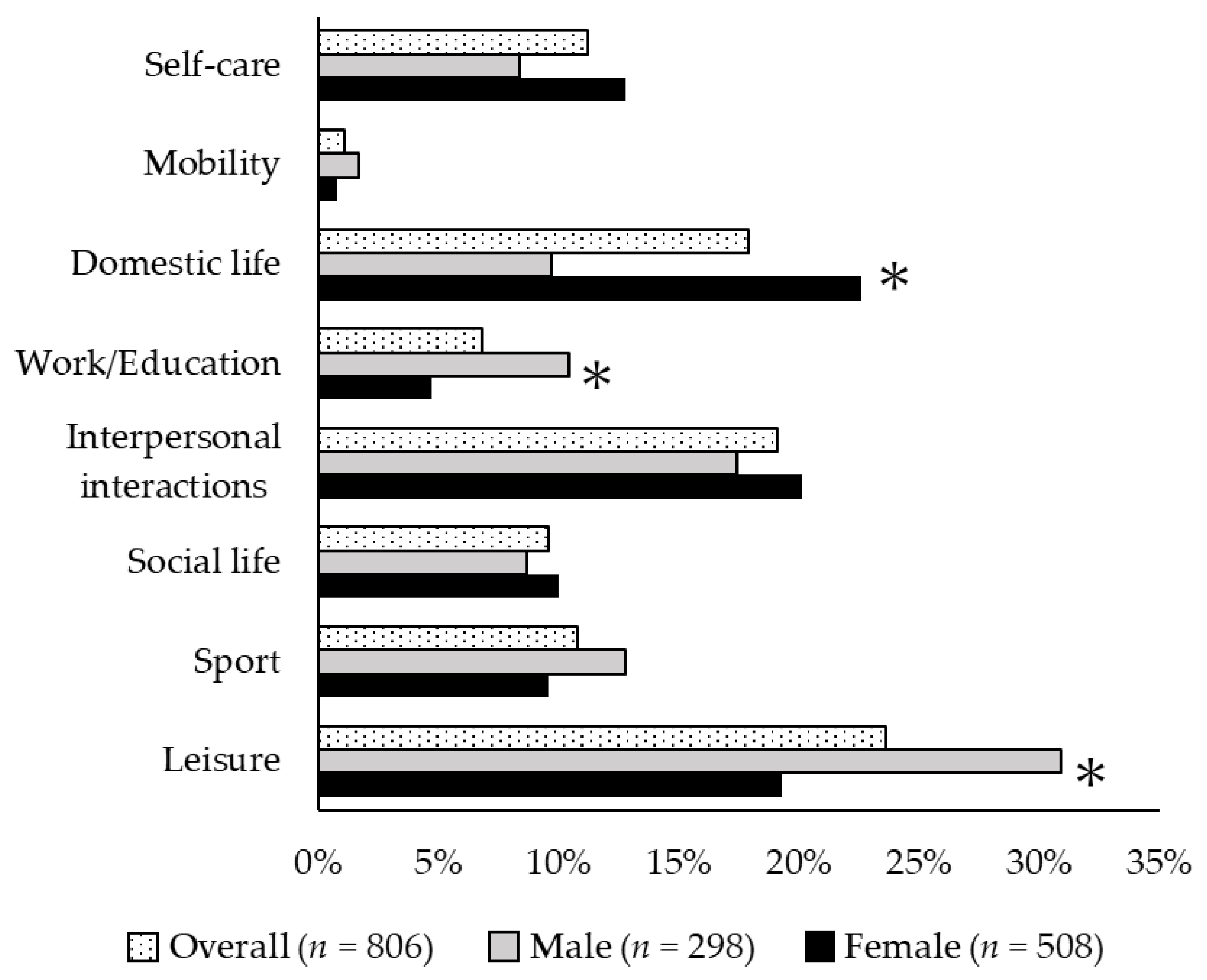
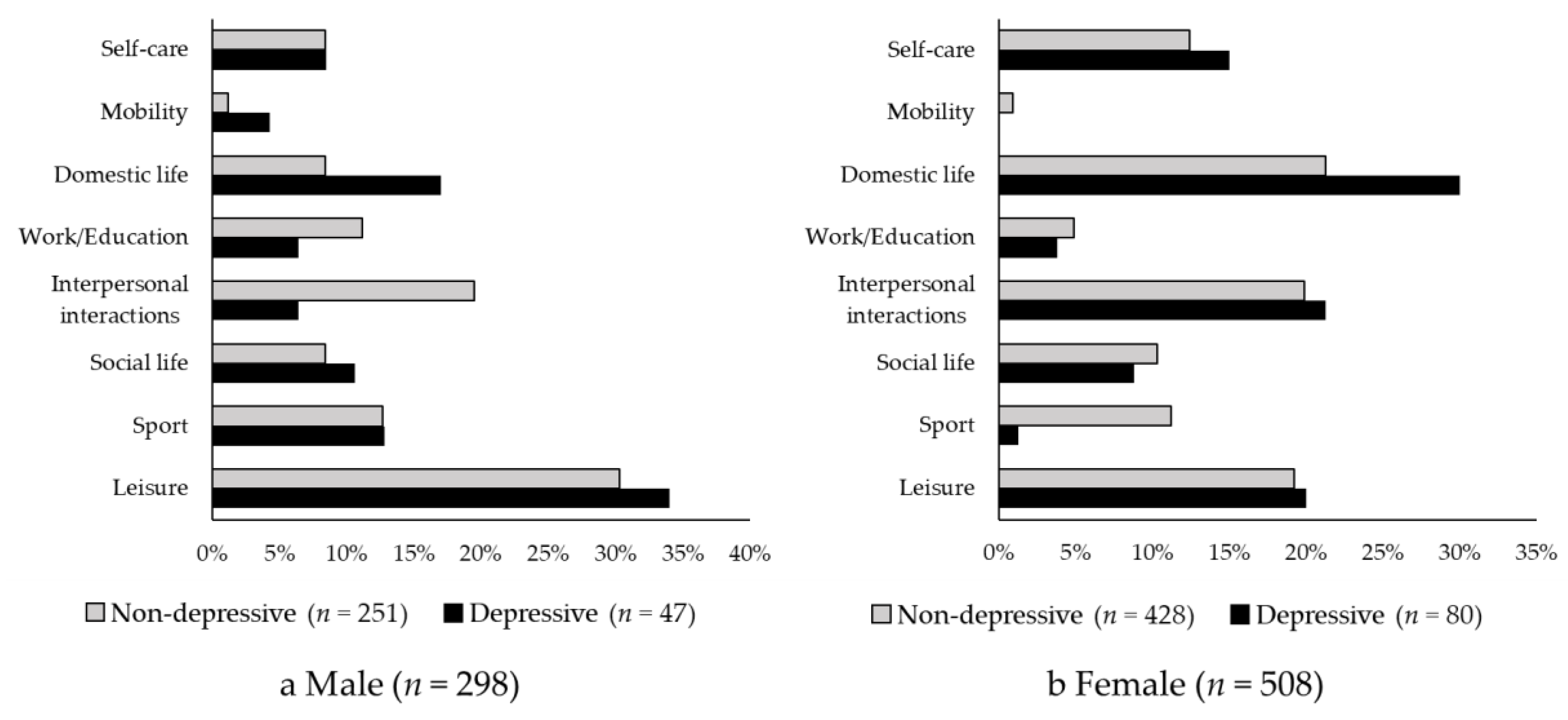
3.2. Association between Depressive Symptoms and Meaningful Activity Categories
3.3. Association between Depressive Symptoms, Satisfaction, and Performance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Laborde-Lahoz, P.; El-Gabalawy, R.; Kinley, J.; Kirwin, P.D.; Sareen, J.; Pietrzak, R.H. Subsyndromal depression among older adults in the USA: Prevalence, comorbidity, and risk for new-onset psychiatric disorders in late life. Int. J. Geriatr. Psychiatry. 2015, 30, 677–685. [Google Scholar] [CrossRef] [PubMed]
- Luppa, M.; Sikorski, C.; Luck, T.; Ehreke, L.; Konnopka, A.; Wiese, B.; Weyerer, S.; König, H.H.; Riedel-Heller, S.G. Age- and gender-specific prevalence of depression in latest-life--systematic review and meta-analysis. J. Affect. Disord. 2012, 136, 212–221. [Google Scholar] [CrossRef] [PubMed]
- Niino, N.; Ihara, K.; Suzuki, T.; Shibata, H. Prevalence of depressive symptoms among the elderly: A longitudinal study. Geriatr. Gerontol. Int. 2003, 3, 27–30. [Google Scholar] [CrossRef]
- Heser, K.; Stein, J.; Luppa, M.; Wiese, B.; Mamone, S.; Weyerer, S.; Werle, J.; König, H.H.; Hajek, A.; Scherer, M.; et al. Late-life depressive symptoms are associated with functional impairment cross-sectionally and over time: Results of the AgeMooDe study. J. Gerontol. 2018, 75, 811–820. [Google Scholar] [CrossRef] [PubMed]
- Murphy, R.A.; Hagaman, A.K.; Reinders, I.; Steeves, J.A.; Newman, A.B.; Rubin, S.M.; Satterfield, S.; Kritchevsky, S.B.; Yaffe, K.; Ayonayon, H.N.; et al. Health ABC Study. Depressive Trajectories and Risk of Disability and Mortality in Older Adults: Longitudinal Findings from the Health, Aging, and Body Composition Study. J. Gerontol. A Biol. Sci. Med. Sci. 2016, 71, 228–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braam, A.W.; Prince, M.J.; Beekman, A.T.; Delespaul, P.; Dewey, M.E.; Geerlings, S.W.; Kivelä, S.L.; Lawlor, B.A.; Magnússon, H.; Meller, I.; et al. Physical health and depressive symptoms in older Europeans. Results from EURODEP. Br. J. Psychiatry 2005, 187, 35–42. [Google Scholar] [CrossRef]
- Chachamovich, E.; Fleck, M.; Laidlaw, K.; Power, M. Impact of major depression and subsyndromal symptoms on quality of life and attitudes toward aging in an international sample of older adults. Gerontologist 2008, 48, 593–602. [Google Scholar] [CrossRef] [Green Version]
- Cuijpers, P.; Vogelzangs, N.; Twisk, J.; Kleiboer, A.; Li, J.; Penninx, B.W. Differential mortality rates in major and subthreshold depression: Meta-analysis of studies that measured both. Br. J. Psychiatry 2013, 202, 22–27. [Google Scholar] [CrossRef]
- Cuijpers, P.; Smit, F.; Oostenbrink, J.; de Graaf, R.; Ten Have, M.; Beekman, A. Economic costs of minor depression: A population-based study. Acta Psychiatr. Scand. 2007, 115, 229–236. [Google Scholar] [CrossRef]
- Jorm, A.F.; Patten, S.B.; Brugha, T.S.; Mojtabai, R. Has increased provision of treatment reduced the prevalence of common mental disorders? Review of the evidence from four countries. World Psychiatry 2017, 16, 90–99. [Google Scholar] [CrossRef] [Green Version]
- Dotson, V.M.; Hsu, F.C.; Langaee, T.Y.; McDonough, C.W.; King, A.C.; Cohen, R.A.; Newman, A.B.; Kritchevsky, S.B.; Myers, V.; Manini, T.M.; et al. Genetic Moderators of the Impact of Physical Activity on Depressive Symptoms. J. Frailty Aging 2016, 5, 6–14. [Google Scholar] [PubMed]
- Yoshida, Y.; Iwasa, H.; Kumagai, S.; Suzuki, T.; Awata, S.; Yoshida, H. Longitudinal association between habitual physical activity and depressive symptoms in older people. Psychiatry Clin. Neurosci. 2015, 69, 686–692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Opdebeeck, C.; Quinn, C.; Nelis, S.M.; Clare, L. Is cognitive lifestyle associated with depressive thoughts and self-reported depressive symptoms in later life? Eur. J. Ageing 2016, 13, 63–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jang, Y.; Chiriboga, D.A. Social activity and depressive symptoms in Korean American older adults: The conditioning role of acculturation. J. Aging Health 2011, 23, 767–781. [Google Scholar] [CrossRef] [PubMed]
- Fulbright, S.A. Rates of depression and participation in senior centre activities in community-dwelling older persons. J. Psychiatr. Ment. Health Nurs. 2010, 17, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Galli, R.; Moriguchi, E.H.; Bruscato, N.M.; Horta, R.L.; Pattussi, M.P. Active aging is associated with low prevalence of depressive symptoms among Brazilian older adults. Rev. Bras. Epidemiol. 2016, 19, 307–316. [Google Scholar] [CrossRef]
- Chen, L.J.; Stevinson, C.; Ku, P.W.; Chang, Y.K.; Chu, D.C. Relationships of leisure-time and non-leisure-time physical activity with depressive symptoms: A population-based study of Taiwanese older adults. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 28. [Google Scholar] [CrossRef] [Green Version]
- Uemura, K.; Makizako, H.; Lee, S.; Doi, T.; Tsutsumimoto, K.; Shimada, H. Behavioral protective factors of increased depressive symptoms in community-dwelling older adults: A prospective cohort study. Int. J. Geriatr. Psychiatry 2018, 33, e234–e241. [Google Scholar] [CrossRef]
- Lampinen, P.; Heikkinen, R.L.; Kauppinen, M.; Heikkinen, E. Activity as a Predictor of Mental Well-Being Among Older Adults. Aging Ment. Health 2006, 10, 454–466. [Google Scholar] [CrossRef]
- Rantanen, T.; Pynnönen, K.; Saajanaho, M.; Siltanen, S.; Karavirta, L.; Kokko, K.; Karvonen, A.; Kauppinen, M.; Rantalainen, T.; Rantakokko, M.; et al. Individualized counselling for active aging: Protocol of a single-blinded, randomized controlled trial among older people (the AGNES intervention study). BMC Geriatr. 2019, 19, 5. [Google Scholar] [CrossRef]
- Eakman, A.M.; Carlson, M.; Clark, F. Factor Structure, Reliability and Convergent Validity of the Engagement in Meaningful Activities Survey for Older Adults. OTJR 2010, 30, 111–121. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Active Ageing: A Policy Framework; WHO: Geneva, Switzerland, 2002. [Google Scholar]
- Moyers, P.A. The guide to occupational therapy practice. American Occupational Therapy Association. Am. J. Occup. Ther. 1999, 53, 247–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandez-Ballesteros, R.; Zammarron, M.D.; Ruiz, M.A. The contribution of socio-demographic and psychosocial factors to life satisfaction. Aging Soc. 2001, 21, 25–43. [Google Scholar] [CrossRef]
- Lomranz, J.; Bergman, S.; Eyal, N.; Shmotkin, D. Indoor and outdoor activities of aged women and men as related to depression and well-being. Int. J. Aging Hum. Dev. 1988, 26, 303–314. [Google Scholar] [CrossRef]
- Everard, K.M. The relationship between reasons for activity and older adult well-being. J. Appl. Gerontol. 1999, 18, 325–340. [Google Scholar] [CrossRef]
- Yesavage, J.A. Geriatric Depression Scale. Psychopharm. Bull. 1988, 24, 709–711. [Google Scholar]
- De Craen, A.J.; Heeren, T.J.; Gussekloo, J. Accuracy of the 15-item geriatric depression scale (GDS-15) in a community sample of the oldest old. Int. J. Geriatr. Psychiatry 2003, 18, 63–66. [Google Scholar] [CrossRef]
- Almeida, O.P.; Almeida, S.A. Short versions of the geriatric depression scale: A study of their validity for the diagnosis of a major depressive episode according to ICD-10 and DSM-IV. Int. J. Geriatr. Psychiatry 1999, 14, 858–865. [Google Scholar] [CrossRef]
- Tomori, K.; Uezu, S.; Kinjo, S.; Ogahara, K.; Nagatani, R.; Higashi, T. Utilization of the iPad application: Aid for Decision-making in Occupation Choice. Occup. Ther. Int. 2012, 19, 88–97. [Google Scholar] [CrossRef]
- Levack, W.; Tomori, K.; Takahashi, K.; Sherrington, A.J. Development of an English-language version of a Japanese iPad application to facilitate collaborative goal setting in rehabilitation: A Delphi study and field test. BMJ Open 2018, 8, e018908. [Google Scholar] [CrossRef]
- Tomori, K.; Saito, Y.; Nagayama, H.; Seshita, Y.; Ogahara, K.; Nagatani, R.; Higashi, T. Reliability and validity of individualized satisfaction score in aid for decision-making in occupation choice. Disabil. Rehabil. 2013, 35, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Borson, S.; Scanlan, J.; Brush, M.; Vitaliano, P.; Dokmak, A. The mini-cog: A cognitive ‘vital signs’ measure for dementia screening in multi-lingual elderly. Int. J. Geriatr. Psychiatry 2000, 15, 1021–1027. [Google Scholar] [CrossRef]
- Borson, S.; Scanlan, J.M.; Watanabe, J.; Tu, S.P.; Lessig, M. Simplifying detection of cognitive impairment: Comparison of the Mini-Cog and Mini-Mental State Examination in a multiethnic sample. J. Am. Geriatr. Soc. 2005, 53, 871–874. [Google Scholar] [CrossRef] [PubMed]
- Milian, M.; Leiherr, A.M.; Straten, G.; Mller, S.; Leyhe, T.; Eschweiler, G.W. The Mini-Cog versus the Mini-Mental State Examination and the Clock Drawing Test in daily clinical practice: Screening value in a German Memory Clinic. Int. Psychogeriatr. 2012, 24, 766–774. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.K.; Liu, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Bahyah, K.S.; Chou, M.Y.; Chen, L.Y.; Hsu, P.S.; Krairit, O.; et al. Sarcopenia in Asia: Consensus report of the Asian Working Group for Sarcopenia. J. Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Shimada, H.; Makizako, H.; Doi, T.; Yoshida, D.; Tsutsumimoto, K.; Anan, Y.; Uemura, K.; Ito, T.; Lee, S.; Park, H.; et al. Combined prevalence of frailty and mild cognitive impairment in a population of elderly Japanese people. J. Am. Med. Dir. Assoc. 2013, 14, 518–524. [Google Scholar] [CrossRef]
- Iwasa, H.; Masui, Y.; Inagaki, H.; Yoshida, Y.; Shimada, H.; Otsuka, R.; Kikuchi, K.; Nonaka, K.; Yoshida, H.; Suzuki, T. Development of the Japan Science and Technology Agency Index of Competence to Assess Functional Capacity in Older Adults: Conceptual Definitions and Preliminary Items. Gerontol. Geriatr. Med. 2015, 1. [Google Scholar] [CrossRef] [Green Version]
- Iwasa, H.; Masui, Y.; Inagaki, H.; Yoshida, Y.; Shimada, H.; Otsuka, R.; Kikuchi, K.; Nonaka, K.; Yoshida, H.; Suzuki, T. Assessing competence at a higher level among older adults: Development of the Japan Science and Technology Agency Index of Competence (JST-IC). Aging Clin. Exp. Res. 2018, 30, 383–393. [Google Scholar] [CrossRef]
- Saito, T.; Kondo, K.; Murata, C.; Jeong, S.; Suzuki, K.; Kondo, N. Gender and regional differences in going-out, social, and leisure activities among older adults. Findings from the JAGES Project. Jpn. J. Public Health 2015, 62, 596–608. [Google Scholar]
- Weller, I.; Corey, P. The impact of excluding non-leisure energy expenditure on the relation between physical activity and mortality in women. Epidemiology 1998, 9, 632–635. [Google Scholar] [CrossRef]
- Moon, J.H. Factors Affecting Activity Limitation in the Elderly: Data Processed from the Korea National Health and Nutrition Examination Survey, 2016. Osong Public Health Res. Perspect. 2019, 10, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Monma, T.; Takeda, F.; Noguchi, H.; Tamiya, N. Age and sex differences of risk factors of activity limitations in Japanese older adults. Geriatr. Gerontol. Int. 2016, 16, 670–678. [Google Scholar] [CrossRef] [PubMed]
- Polku, H.; Mikkola, T.M.; Portegijs, E.; Rantakokko, M.; Kokko, K.; Kauppinen, M.; Rantanen, T.; Viljanen, A. Life-space mobility and dimensions of depressive symptoms among community-dwelling older adults. Aging Ment. Health 2015, 19, 781–789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kandola, A.; Ashdown-Franks, G.; Hendrikse, J.; Sabiston, C.M.; Stubbs, B. Physical activity and depression: Towards understanding the antidepressant mechanisms of physical activity. Neurosci. Biobehav. Rev. 2019, 107, 525–539. [Google Scholar] [CrossRef] [PubMed]
- Glass, T.A.; De Leon, C.F.; Bassuk, S.S.; Berkman, L.F. Social engagement and depressive symptoms in late life: Longitudinal findings. J. Aging Health 2006, 18, 604–628. [Google Scholar] [CrossRef] [PubMed]
- Law, M.; Polatajko, H.; Baptiste, S.; Townsend, E. Core Concepts of Occupational Therapy; CAOT Publications ACE: Ottawa, CA, USA, 1997; pp. 29–56. [Google Scholar]
- Yoo, J.S.; Chang, S.J.; Kim, H.S. Prevalence and Predictive Factors of Depression in Community-Dwelling Older Adults in South Korea. Res. Theory Nurs. Pract. 2016, 30, 200–211. [Google Scholar] [CrossRef]
- Lue, B.H.; Chen, L.J.; Wu, S.C. Health, financial stresses, and life satisfaction affecting late-life depression among older adults: A nationwide, longitudinal survey in Taiwan. Arch. Gerontol. Geriatr. 2010, 50, S34–S38. [Google Scholar] [CrossRef]
- Strine, T.W.; Kroenke, K.; Dhingra, S.; Balluz, L.S.; Gonzalez, O.; Berry, J.T.; Mokdad, A.H. The associations between depression, health-related quality of life, social support, life satisfaction, and disability in community-dwelling US adults. J. Nerv. Ment. Dis. 2009, 197, 61–64. [Google Scholar] [CrossRef]
- Krause, N. Stressors arising in highly valued roles, meaning in life, and the physical health status of older adults. J. Gerontol. B Psychol. Sci. Soc. Sci. 2004, 59, S287–S297. [Google Scholar] [CrossRef]
- O’Connor, B.P.; Vallerand, R.J. Psychological adjustment variables as predictors of mortality among nursing home residents. Psychol. Aging 1998, 13, 368–374. [Google Scholar] [CrossRef]
- Van der Heyden, K.; Dezutter, J.; Beyers, W. Meaning in Life and depressive symptoms: A person-oriented approach in residential and community-dwelling older adults. Aging Ment. Health 2015, 19, 1063–1070. [Google Scholar] [CrossRef] [PubMed]
- Clark, F.A.; Parham, D.; Carlson, M.E.; Frank, G.; Jackson, J.; Pierce, D.; Wolfe, R.J.; Zemke, R. Occupational science: Academic innovation in the service of occupational therapy’s future. Am. J. Occup. Ther. 1991, 45, 300–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| All Participants (n = 806) | Non-Depressive Group (n = 679) | Depressive Group (n = 127) | p Value | |
|---|---|---|---|---|
| Age, mean ± SD (years) | 74.9 ± 6.3 | 74.7 ± 6.2 | 76.2 ± 6.5 | 0.010 a |
| Female, n (%) | 508(63.0) | 428 (63.0) | 80 (63.0) | 0.993 b |
| Satisfaction with Activity, Median (IQR) | 5.0 (4.0–5.0) | 5.0 (4.0–5.0) | 4.0 (3.0–5.0) | <0.001 c |
| Performance of Activity, Median (IQR) | 10.0 (8.0–10.0) | 10.0 (8.0–10.0) | 8.0 (6.0–10.0) | 0.005 c |
| Poor cognitive Status, n (%) | 168 (20.8) | 137 (20.2) | 31 (24.4) | 0.281 b |
| Poor Physical Status, n (%) | 249 (30.9) | 192 (28.3) | 57 (44.9) | <0.001 b |
| Education, Mean ± SD (years) | 11.2 ± 2.3 | 11.2 ± 2.3 | 10.8 ± 2.2 | 0.084 a |
| BMI, Mean ± SD (kg/m2) | 23.3 ± 3.4 | 23.3 ± 3.3 | 23.0 ± 3.6 | 0.286 a |
| Medications, Mean ± SD (Number) | 4.2 ± 4.6 | 4.0 ± 4.2 | 5.3 ± 6.2 | 0.022 a |
| Social Engagement, Median (IQR) | 3.0 (1.0–4.0) | 3.0 (2.0–4.0) | 2.0 (0–3.0) | <0.001 c |
| Living Alone, n (%) | 211 (26.2) | 170 (25.0) | 41 (32.3) | 0.088 b |
| Crude Model | Adjusted Model 1 | Adjusted Model 2 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p Value | OR | 95% CI | p Value | OR | 95% CI | p Value | OR | 95% CI | p Value | |
| Satisfaction with Activity | 0.60 | 0.49–0.73 | <0.001 | 0.61 | 0.49–0.75 | <0.001 | 0.62 | 0.49–0.79 | <0.001 | |||
| Performance of Activity | 0.86 | 0.78–0.93 | 0.001 | 0.89 | 0.81–0.98 | 0.019 | 0.97 | 0.88–1.08 | 0.598 | |||
| Age | 1.00 | 0.96–1.04 | 0.954 | 1.00 | 0.96–1.03 | 0.795 | 1.00 | 0.96–1.04 | 0.941 | |||
| Gender | 0.85 | 0.55–1.31 | 0.457 | 0.85 | 0.55–1.30 | 0.446 | 0.85 | 0.55–1.32 | 0.464 | |||
| Body Mass Index | 0.98 | 0.92–1.04 | 0.412 | 0.97 | 0.91–1.03 | 0.294 | 0.97 | 0.92–1.04 | 0.400 | |||
| Living Alone | 1.11 | 0.69–1.78 | 0.673 | 1.22 | 0.76–1.94 | 0.411 | 1.11 | 0.69–1.78 | 0.662 | |||
| Education | 0.97 | 0.88–1.07 | 0.557 | 0.97 | 0.88–1.06 | 0.488 | 0.97 | 0.88–1.07 | 0.530 | |||
| Medications | 1.02 | 0.98–1.06 | 0.332 | 1.03 | 0.99–1.07 | 0.200 | 1.02 | 0.98–1.06 | 0.334 | |||
| Poor Cognitive Status | 1.03 | 0.61–1.73 | 0.911 | 1.00 | 0.60–1.66 | 0.998 | 1.02 | 0.61–1.72 | 0.938 | |||
| Poor Physical Status | 1.26 | 0.78–2.04 | 0.348 | 1.21 | 0.75–1.95 | 0.442 | 1.24 | 0.77–2.02 | 0.377 | |||
| Social Engagement | 0.62 | 0.53–0.73 | <0.001 | 0.62 | 0.53–0.72 | <0.001 | 0.64 | 0.54–0.73 | <0.001 | |||
| Crude Model | Adjusted Model 1 | Adjusted Model 2 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p Value | OR | 95% CI | p Value | OR | 95% CI | p Value | |
| Men | |||||||||
| Satisfaction with Activity | 0.59 | 0.43–0.80 | 0.001 | 0.61 | 0.44–0.85 | 0.004 | 0.52 | 0.35–0.77 | 0.001 |
| Performance of Activity | 0.97 | 0.83–0.97 | 0.649 | 1.03 | 0.88–1.21 | 0.719 | 1.18 | 0.88–1.08 | 0.091 |
| Women | |||||||||
| Satisfaction with Activity | 0.60 | 0.47–0.78 | <0.001 | 0.59 | 0.44–0.78 | <0.001 | 0.67 | 0.49–0.91 | 0.009 |
| Performance of Activity | 0.80 | 0.71–0.89 | <0.001 | 0.82 | 0.73–0.92 | 0.001 | 0.87 | 0.77–0.99 | 0.041 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maruta, M.; Makizako, H.; Ikeda, Y.; Miyata, H.; Nakamura, A.; Han, G.; Shimokihara, S.; Tokuda, K.; Kubozono, T.; Ohishi, M.; et al. Associations between Depressive Symptoms and Satisfaction with Meaningful Activities in Community-Dwelling Japanese Older Adults. J. Clin. Med. 2020, 9, 795. https://doi.org/10.3390/jcm9030795
Maruta M, Makizako H, Ikeda Y, Miyata H, Nakamura A, Han G, Shimokihara S, Tokuda K, Kubozono T, Ohishi M, et al. Associations between Depressive Symptoms and Satisfaction with Meaningful Activities in Community-Dwelling Japanese Older Adults. Journal of Clinical Medicine. 2020; 9(3):795. https://doi.org/10.3390/jcm9030795
Chicago/Turabian StyleMaruta, Michio, Hyuma Makizako, Yuriko Ikeda, Hironori Miyata, Atsushi Nakamura, Gwanghee Han, Suguru Shimokihara, Keiichiro Tokuda, Takuro Kubozono, Mitsuru Ohishi, and et al. 2020. "Associations between Depressive Symptoms and Satisfaction with Meaningful Activities in Community-Dwelling Japanese Older Adults" Journal of Clinical Medicine 9, no. 3: 795. https://doi.org/10.3390/jcm9030795
APA StyleMaruta, M., Makizako, H., Ikeda, Y., Miyata, H., Nakamura, A., Han, G., Shimokihara, S., Tokuda, K., Kubozono, T., Ohishi, M., Tomori, K., & Tabira, T. (2020). Associations between Depressive Symptoms and Satisfaction with Meaningful Activities in Community-Dwelling Japanese Older Adults. Journal of Clinical Medicine, 9(3), 795. https://doi.org/10.3390/jcm9030795