Different Pulp Dressing Materials for the Pulpotomy of Primary Teeth: A Systematic Review of the Literature



 ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
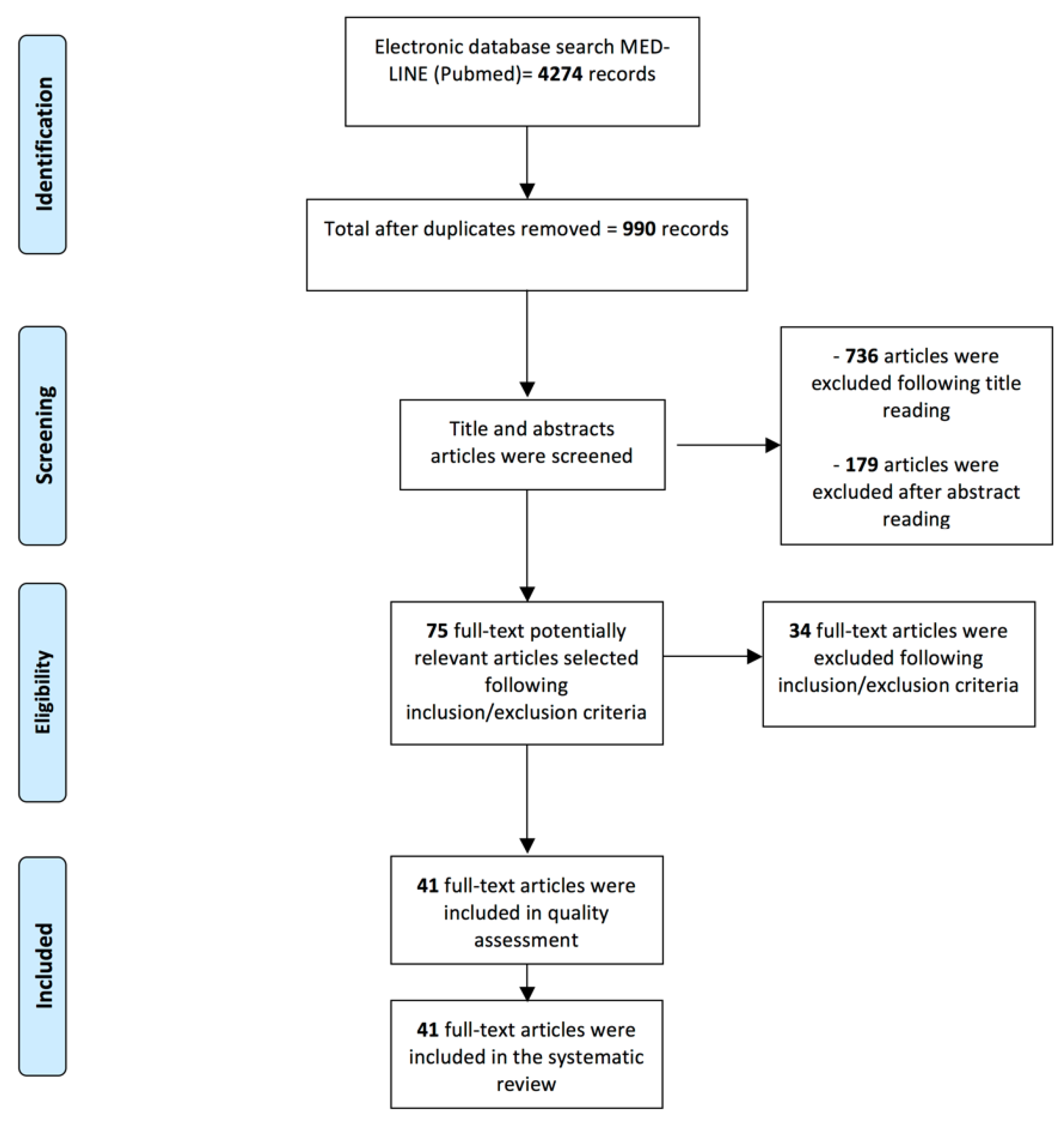
2.1. Search Strategy
2.2. Study Selection
2.2.1. Inclusion Criteria
- -
- Human in vivo studies written in English published in peer-reviewed journals;
- -
- Comparative clinical articles reporting on different materials applied in pulpotomy of primary teeth;
- -
- Definitive restorations of the primary teeth;
- -
- Clinical and/or radiographical follow-up of at least 12 months;
- -
- Random allocation of the samples.
2.2.2. Exclusion Criteria
- -
- In vitro studies on human and animals;
- -
- Systematic reviews, case series, case studies, retrospective studies;
- -
- Follow-up < 12 months;
- -
- Clinical studies without random allocation of the samples;
- -
- Non-comparative papers, namely reporting on only one material used in pulpotomy procedures;
- -
- Papers evaluating other clinical procedures that involved the pulp, such as direct capping, indirect capping, endodontic treatment.
2.3. Data Collection
2.4. Assessment of Heterogeneity
- Pulpotomy procedure
- Materials management
- Expertise of the clinician
- Restoration materials
- Outcome variables
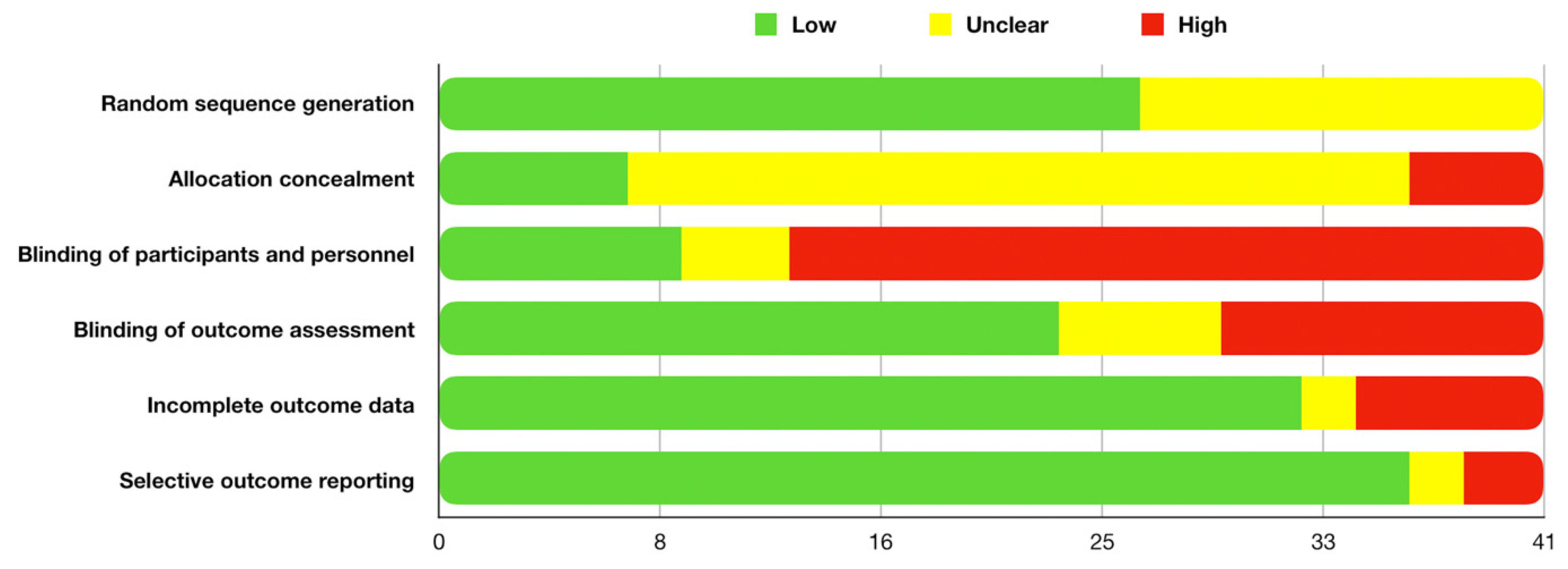
2.5. Quality Assessment
3. Results
3.1. Search and Selection
3.2. Assessment of Heterogeneity
3.3. Quality Assessment
3.4. Outcomes
3.4.1. MTA
3.4.2. Biodentine
3.4.3. Ferric Sulphate
3.4.4. Formocresol
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- US Department of Health and Human Services, National Institute of Dental and Craniofacial Research, National Institutes of Health. Oral Health in America: A Report of the Surgeon General; U.S. Department of Health and Human Services, National Institute of Dental and Craniofacial Research, National Institutes of Health: Rockville, MD, USA, 2000. Available online: https://www.nidcr.niih.gov/sites/default/files/2017-10/hck1ocv.%40www.surgeon.fullrpt.pdf (accessed on 2 December 2019).
- Smaïl-Faugeron, V.; Glenny, A.M.; Courson, F.; Durieux, P.; Muller-Bolla, M.; Fron Chabouis, H. Pulp treatment for extensive decay in primary teeth. Cochrane Database Syst. Rev. 2018, 5, CD003220. [Google Scholar]
- GBD 2016 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259. [Google Scholar] [CrossRef]
- Stringhini Junior, E.; Dos Santos, M.G.C.; Oliveira, L.B.; Mercadé, M. MTA and biodentine for primary teeth pulpotomy: A systematic review and meta-analysis of clinical trials. Clin. Oral Investig. 2019, 23, 1967–1976. [Google Scholar] [CrossRef] [PubMed]
- Bhujel, N.; Duggal, M.S.; Saini, P.; Day, P.F. The effect of premature extraction of primary teeth on the subsequent need for orthodontic treatment. Eur. Arch. Paediatr. Dent. 2016, 17, 423–434. [Google Scholar] [CrossRef]
- American Academy on Pediatric Dentistry; American Academy of Pediatrics. Policy on early childhood caries (ECC): Classifications, consequences, and preventive strategies. Pediatr. Dent. 2008, 30, 40–43. [Google Scholar]
- Dhar, V.; Marghalani, A.A.; Crystal, Y.O.; Kumar, A.; Ritwik, P.; Tulunoglu, O.; Graham, L. Use of vital pulp therapies in primary teeth with deep caries lesions. Pediatr. Dent. 2017, 39, E146–E159. [Google Scholar]
- American Academy on Pediatric Dentistry. Pulp Therapy for Primary and Immature Permanent Teeth. Pediatr. Dent. 2017, 39, 325–333. [Google Scholar]
- Brizuela, C.; Ormeño, A.; Cabrera, C.; Cabezas, R.; Silva, C.I.; Ramírez, V.; Mercade, M. Direct pulp capping with calcium hydroxide, mineral trioxide aggregate, and biodentine in permanent young teeth with caries: A randomized clinical trial. J. Endod. 2017, 43, 1776–1780. [Google Scholar] [CrossRef]
- Li, Z.; Cao, L.; Fan, M.; Xu, Q. Direct pulp capping with calcium hydroxide or mineral trioxide aggregate: A meta-analysis. J. Endod. 2015, 41, 1412–1417. [Google Scholar] [CrossRef]
- Smaïl-Faugeron, V.; Porot, A.; Muller-Bolla, M.; Courson, F. Indirect pulp capping versus pulpotomy for treating deep carious lesions approaching the pulp in primary teeth: A systematic review. Eur. J. Paediatr. Dent. 2016, 17, 107–112. [Google Scholar]
- Omar, S. MTA, formocresol, and ferric sulfate have significantly better clinical and radiographic outcomes than calcium hydroxide and laser therapies in primary molar pulpotomies after 18-24 months. J. Evid. Based Dent. Pract. 2015, 15, 58–60. [Google Scholar] [CrossRef] [PubMed]
- Stringhini Junior, E.; Vitcel, M.E.; Oliveira, L.B. Evidence of pulpotomy in primary teeth comparing MTA, calcium hydroxide, ferric sulphate, and electrosurgery with formocresol. Eur. Arch. Paediatr. Dent. 2015, 16, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Asgary, S.; Shirvani, A.; Fazlyab, M. MTA and ferric sulfate in pulpotomy outcomes of primary molars: A systematic review and meta-analysis. J. Clin. Pediatr. Dent. 2014, 39, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Parirokh, M.; Torabinejad, M.; Dummer, P.M.H. Mineral trioxide aggregate and other bioactive endodontic cements: An updated overview - part I: Vital pulp therapy. Int. Endod. J. 2018, 51, 177–205. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0; The Cochrane Collaboration: 2011. Available online: http://training.cochrane.org/handbook/archive/v5.1/ (accessed on 24 October 2019).
- Kathal, S.; Gupta, S.; Bhayya, D.P.; Rao, A.; Roy, A.P.; Sabhlok, A. A comparative evaluation of clinical and radiographic success rate of pulpotomy in primary molars using antioxidant mix and mineral trioxide aggregate: An in vivo 1-year follow-up study. J. Indian Soc. Pedod. Prev. Dent. 2017, 35, 327–331. [Google Scholar] [CrossRef]
- Alsanouni, M.; Bawazir, O.A. A randomized clinical trial of neomta plus in primary molar pulpotomies. Pediatr. Dent. 2019, 41, 107–111. [Google Scholar]
- Pratima, B.; Chandan, G.D.; Nidhi, T.; Nitish, I.; Sankriti, M.; Nagaveni, S.; Shweta, S. Postoperative assessment of diode laser zinc oxide eugenol and mineral trioxide aggregate pulpotomy procedures in children: A comparative clinical study. J. Indian Soc. Pedod. Prev. Dent. 2018, 36, 308–314. [Google Scholar] [CrossRef]
- Kang, C.M.; Kim, S.H.; Shin, Y.; Lee, H.S.; Lee, J.H.; Kim, G.T.; Song, J.S. A randomized controlled trial of ProRoot MTA, OrthoMTA and RetroMTA for pulpotomy in primary molars. Oral. Dis. 2015, 21, 785–791. [Google Scholar] [CrossRef]
- Akcay, M.; Sari, S. The effect of sodium hypochlorite application on the success of calcium hydroxide and mineral trioxide aggregate pulpotomies in primary teeth. Pediatr. Dent. 2014, 36, 316–321. [Google Scholar]
- Fernández, C.C.; Martínez, S.S.; Jimeno, F.G.; Lorente Rodríguez, A.I.; Mercadé, M. Clinical and radiographic outcomes of the use of four dressing materials in pulpotomized primary molars: A randomized clinical trial with 2-year follow-up. Int. J. Paediatr. Dent. 2013, 23, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Zhou, Q.; Qin, M. Mineral trioxide aggregate versus calcium hydroxide for pulpotomy in primary molars. Chin. J. Dent. Res. 2011, 14, 121–125. [Google Scholar]
- Holan, G.; Eidelman, E.; Fuks, A.B. Long-term evaluation of pulpotomy in primary molars using mineral trioxide aggregate or formocresol. Pediatr. Dent. 2005, 27, 129–136. [Google Scholar] [PubMed]
- Nematollahi, H.; Noorollahian, H.; Bagherian, A.; Yarbakht, M.; Nematollahi, S. Mineral trioxide aggregate partial pulpotomy versus formocresol pulpotomy: A randomized, split-mouth, controlled clinical trial with 24 months follow-up. Pediatr. Dent. 2018, 40, 184–189. [Google Scholar] [PubMed]
- Musale, P.K.; Soni, A.S. Clinical pulpotomy trial of copaifera langsdorffii oil resin versus formocresol and white mineral trioxide aggregate in primary teeth. Pediatr. Dent. 2016, 38, 5–12. [Google Scholar] [PubMed]
- Atasever, G.; Keceli, T.I.; Uysal, S.; Gungor, H.C.; Olmez, S. Primary molar pulpotomies with different hemorrhage control agents and base materials: A randomized clinical trial. Niger J. Clin. Pract. 2019, 22, 305–312. [Google Scholar] [PubMed]
- Huth, K.C.; Paschos, E.; Hajek-Al-Khatar, N.; Hollweck, R.; Crispin, A.; Hickel, R.; Folwaczny, M. Effectiveness of 4 pulpotomy techniques--randomized controlled trial. J. Dent. Res. 2005, 84, 1144–1148. [Google Scholar] [CrossRef]
- Nguyen, T.D.; Judd, P.L.; Barrett, E.J.; Sidhu, N.; Casas, M.J. Comparison of ferric sulfate combined mineral trioxide aggregate pulpotomy and zinc oxide eugenol pulpectomy of primary maxillary incisors: An 18-month randomized, controlled trial. Pediatr. Dent. 2017, 39, 34–38. [Google Scholar]
- Saltzman, B.; Sigal, M.; Clokie, C.; Rukavina, J.; Titley, K.; Kulkarni, G.V. Assessment of a novel alternative to conventional formocresol-zinc oxide eugenol pulpotomy for the treatment of pulpally involved human primary teeth: Diode laser-mineral trioxide aggregate pulpotomy. Int. J. Paediatr. Dent. 2005, 15, 437–447. [Google Scholar] [CrossRef]
- Grewal, N.; Salhan, R.; Kaur, N.; Patel, H.B. Comparative evaluation of calcium silicate-based dentin substitute (Biodentine®) and calcium hydroxide (pulpdent) in the formation of reactive dentin bridge in regenerative pulpotomy of vital primary teeth: Triple blind, randomized clinical trial. Contemp. Clin. Dent. 2016, 7, 457–463. [Google Scholar] [CrossRef]
- Hugar, S.M.; Kukreja, P.; Hugar, S.S.; Gokhale, N.; Assudani, H. Comparative evaluation of clinical and radiographic success of formocresol, propolis, turmeric gel, and calcium hydroxide on pulpotomized primary molars: A preliminary study. Int. J. Clin. Pediatr. Dent. 2017, 10, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Kalra, M.; Garg, N.; Rallan, M.; Pathivada, L.; Yeluri, R. Comparative evaluation of fresh aloe barbadensis plant extract and mineral trioxide aggregate as pulpotomy agents in primary molars: A 12-month follow-up study. Contemp. Clin. Dent. 2017, 8, 106–111. [Google Scholar]
- Uloopi, K.S.; Vinay, C.; Ratnaditya, A.; Gopal, A.S.; Mrudula, K.J.; Rao, R.C. Clinical evaluation of low level diode laser application for primary teeth pulpotomy. J. Clin. Diagn Res. 2016, 10, ZC67–ZC70. [Google Scholar] [CrossRef] [PubMed]
- Yildiz, E.; Tosun, G. Evaluation of formocresol, calcium hydroxide, ferric sulfate, and MTA primary molar pulpotomies. Eur. J. Dent. 2014, 8, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Ansari, G.; Morovati, S.P.; Asgary, S. Evaluation of four pulpotomy techniques in primary molars: A randomized controlled trial. Iran Endod. J. 2018, 13, 7–12. [Google Scholar] [PubMed]
- Gupta, G.; Rana, V.; Srivastava, N.; Chandna, P. Laser pulpotomy-an effective alternative to conventional techniques: A 12 months clinicoradiographic study. Int. J. Clin. Pediatr. Dent. 2015, 8, 18–21. [Google Scholar] [PubMed]
- Cantekin, K.; Gümüş, H. Success rates of ankaferd blood stopper and ferric sulfate as pulpotomy agents in primary molars. Int. Sch. Res. Notices 2014, 2014, 819605. [Google Scholar] [CrossRef]
- Trairatvorakul, C.; Koothiratrakarn, A. Calcium hydroxide partial pulpotomy is an alternative to formocresol pulpotomy based on a 3-year randomized trial. Int. J. Paediatr. Dent 2012, 22, 382–389. [Google Scholar] [CrossRef]
- Zurn, D.; Seale, N.S. Light-cured calcium hydroxide vs. formocresol in human primary molar pulpotomies: A randomized controlled trial. Pediatr. Dent 2008, 30, 34–41. [Google Scholar]
- Percinoto, C.; de Castro, A.M.; Pinto, L.M. Clinical and radiographic evaluation of pulpotomies employing calcium hydroxide and trioxide mineral aggregate. Gen Dent 2006, 54, 258–261. [Google Scholar]
- Ghoniem, N.; Vaidyanathan, V.; Zealand, C.M.; Sushynski, J.M.; Mettlach, S.M.; Botero, T.M.; Majewski, R.F.; Boynton, J.R.; Hu, J.C. Mineral trioxide aggregate and diluted formocresol pulpotomy: Prospective and retrospective study outcomes. J. Mich. Dent. Assoc. 2018, 100, 40–65. [Google Scholar]
- Biedma Perea, M.; Solano Mendoza, B.; Garcia-Godoy, F.; Mendoza Mendoza, A.; Iglesias-Linares, A. Clinical and radiographic evaluation of white MTA versus formocresol pulpotomy: A 48-month follow-up study. Am. J. Dent. 2017, 30, 131–136. [Google Scholar] [PubMed]
- Airen, P.; Shigli, A.; Airen, B. Comparative evaluation of formocresol and mineral trioxide aggregate in pulpotomized primary molars--2 year follow up. J. Clin. Pediatr. Dent. 2012, 37, 143–147. [Google Scholar] [CrossRef] [PubMed]
- Frenkel, G.; Kaufman, A.; Ashkenazi, M. Clinical and radiographic outcomes of pulpotomized primary molars treated with white or gray mineral trioxide aggregate and ferric sulfate--long-term follow-up. J. Clin. Pediatr. Dent. 2012, 37, 137–141. [Google Scholar] [CrossRef] [PubMed]
- Cardoso-Silva, C.; Barbería, E.; Maroto, M.; García-Godoy, F. Clinical study of Mineral Trioxide Aggregate in primary molars. Comparison between Grey and White MTA--a long term follow-up (84 months). J. Dent. 2011, 39, 187–193. [Google Scholar] [CrossRef]
- Ibricevic, H.; Al-Jame, Q. Ferric sulphate and formocresol in pulpotomy of primary molars: Long term follow-up study. Eur. J. Paediatr. Dent. 2003, 4, 28–32. [Google Scholar] [PubMed]
- Godhi, B.; Tyagi, R. Success rate of MTA pulpotomy on vital pulp of primary molars: A 3-year observational study. Int. J. Clin. Pediatr. Dent. 2016, 9, 222–227. [Google Scholar] [CrossRef]
- Hugar, S.M.; Deshpande, S.D. Comparative investigation of clinical/radiographical signs of mineral trioxide aggregate and formocresol on pulpotomized primary molars. Contemp. Clin. Dent. 2010, 1, 146–151. [Google Scholar] [CrossRef]
- Ibricevic, H.; Al-Jame, Q. Ferric sulfate as pulpotomy agent in primary teeth: Twenty month clinical follow-up. J. Clin. Pediatr. Dent. 2000, 24, 269–272. [Google Scholar] [CrossRef]
- Çelik, B.N.; Mutluay, M.S.; Arıkan, V.; Sarı, Ş. The evaluation of MTA and Biodentine as a pulpotomy materials for carious exposures in primary teeth. Clin. Oral Investig. 2019, 23, 661–666. [Google Scholar] [CrossRef]
- Malekafzali, B.; Shekarchi, F.; Asgary, S. Treatment outcomes of pulpotomy in primary molars using two endodontic biomaterials. A 2-year randomised clinical trial. Eur. J. Paediatr. Dent. 2011, 12, 189–193. [Google Scholar] [PubMed]
- Sakai, V.T.; Moretti, A.B.; Oliveira, T.M.; Fornetti, A.P.; Santos, C.F.; Machado, M.A.; Abdo, R.C. Pulpotomy of human primary molars with MTA and Portland cement: A randomised controlled trial. Br. Dent. J. 2009, 207, 128–129. [Google Scholar] [CrossRef] [PubMed]
- Farsi, N.; Alamoudi, N.; Balto, K.; Mushayt, A. Success of mineral trioxide aggregate in pulpotomized primary molars. J. Clin. Pediatr. Dent. 2005, 29, 307–311. [Google Scholar] [CrossRef]
- Carti, O.; Oznurhan, F. Evaluation and comparison of mineral trioxide aggregate and biodentine in primary tooth pulpotomy: Clinical and radiographic study. Niger J. Clin. Pract. 2017, 20, 1604–1609. [Google Scholar] [PubMed]
- Guven, Y.; Aksakal, S.D.; Avcu, N.; Unsal, G.; Tuna, E.B.; Aktoren, O. Success rates of pulpotomies in primary molars using calcium silicate-based materials: A randomized control trial. Biomed. Res. Int. 2017, 2017, 4059703. [Google Scholar] [CrossRef] [PubMed]
- Bani, M.; Aktaş, N.; Çınar, Ç.; Odabaş, M.E. The clinical and radiographic success of primary molar pulpotomy using Biodentine™ and mineral trioxide aggregate: A 24-month randomized clinical trial. Pediatr. Dent. 2017, 39, 284–288. [Google Scholar]
- Juneja, P.; Kulkarni, S. Clinical and radiographic comparison of biodentine, mineral trioxide aggregate and formocresol as pulpotomy agents in primary molars. Eur. Arch. Paediatr. Dent. 2017, 18, 271–278. [Google Scholar] [CrossRef]
- Togaru, H.; Muppa, R.; Srinivas, N.; Naveen, K.; Reddy, V.K.; Rebecca, V.C. Clinical and radiographic evaluation of success of two commercially available pulpotomy agents in primary teeth: An in vivo study. J. Contemp. Dent. Pract. 2016, 17, 557–563. [Google Scholar]
- Rajasekharan, S.; Martens, L.C.; Vandenbulcke, J.; Jacquet, W.; Bottenberg, P.; Cauwels, R.G. Efficacy of three different pulpotomy agents in primary molars: A randomized control trial. Int. Endod. J. 2017, 50, 215–228. [Google Scholar] [CrossRef]
- Cuadros-Fernández, C.; Lorente Rodríguez, A.I.; Sáez-Martínez, S.; García-Binimelis, J.; About, I.; Mercadé, M. Short-term treatment outcome of pulpotomies in primary molars using mineral trioxide aggregate and Biodentine: A randomized clinical trial. Clin. Oral Investig. 2016, 20, 1639–1645. [Google Scholar] [CrossRef]
- Silva, L.L.C.E.; Cosme-Silva, L.; Sakai, V.T.; Lopes, C.S.; Silveira, A.P.P.D.; Moretti Neto, R.T.; Gomes-Filho, J.E.; Oliveira, T.M.; Moretti, A.B.D.S. Comparison between calcium hydroxide mixtures and mineral trioxide aggregate in primary teeth pulpotomy: A randomized controlled trial. J. Appl. Oral Sci. 2019, 27, e20180030. [Google Scholar] [CrossRef] [PubMed]
- Junqueira, M.A.; Cunha, N.N.O.; Caixeta, F.F.; Marques, N.C.T.; Oliveira, T.M.; Moretti, A.B.D.S.; Cosme-Silva, L.; Sakai, V.T. Clinical, radiographic and histological evaluation of primary teeth pulpotomy using MTA and ferric sulfate. Braz. Dent. J. 2018, 29, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Jamali, Z.; Alavi, V.; Najafpour, E.; Aminabadi, N.A.; Shirazi, S. Randomized controlled trial of pulpotomy in primary molars using MTA and formocresol compared to 3Mixtatin: A novel biomaterial. J. Clin. Pediatr. Dent. 2018, 42, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Yildirim, C.; Basak, F.; Akgun, O.M.; Polat, G.G.; Altun, C. Clinical and radiographic evaluation of the effectiveness of formocresol, mineral trioxide aggregate, portland cement, and enamel matrix derivative in primary teeth pulpotomies: A two year follow-up. J. Clin. Pediatr. Dent. 2016, 40, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Olatosi, O.O.; Sote, E.O.; Orenuga, O.O. Effect of mineral trioxide aggregate and formocresol pulpotomy on vital primary teeth: A clinical and radiographic study. Niger J. Clin. Pract. 2015, 18, 292–296. [Google Scholar] [CrossRef] [PubMed]
- Celik, B.; Ataç, A.S.; Cehreli, Z.C.; Uysal, S. A randomized trial of mineral trioxide aggregate cements in primary tooth pulpotomies. J. Dent. Child (Chic) 2013, 80, 126–132. [Google Scholar]
- Oliveira, T.M.; Moretti, A.B.; Sakai, V.T.; Lourenço Neto, N.; Santos, C.F.; Machado, M.A.; Abdo, R.C. Clinical, radiographic and histologic analysis of the effects of pulp capping materials used in pulpotomies of human primary teeth. Eur. Arch. Paediatr. Dent 2013, 14, 65–71. [Google Scholar] [CrossRef]
- Sushynski, J.M.; Zealand, C.M.; Botero, T.M.; Boynton, J.R.; Majewski, R.F.; Shelburne, C.E.; Hu, J.C. Comparison of gray mineral trioxide aggregate and diluted formocresol in pulpotomized primary molars: A 6- to 24-month observation. Pediatr. Dent 2012, 34, 120–128. [Google Scholar]
- Erdem, A.P.; Guven, Y.; Balli, B.; Ilhan, B.; Sepet, E.; Ulukapi, I.; Aktoren, O. Success rates of mineral trioxide aggregate, ferric sulfate, and formocresol pulpotomies: A 24-month study. Pediatr. Dent. 2011, 33, 165–170. [Google Scholar]
- Ansari, G.; Ranjpour, M. Mineral trioxide aggregate and formocresol pulpotomy of primary teeth: A 2-year follow-up. Int. Endod. J. 2010, 43, 413–418. [Google Scholar] [CrossRef]
- Doyle, T.L.; Casas, M.J.; Kenny, D.J.; Judd, P.L. Mineral trioxide aggregate produces superior outcomes in vital primary molar pulpotomy. Pediatr. Dent. 2010, 32, 41–47. [Google Scholar] [PubMed]
- Moretti, A.B.; Sakai, V.T.; Oliveira, T.M.; Fornetti, A.P.; Santos, C.F.; Machado, M.A.; Abdo, R.C. The effectiveness of mineral trioxide aggregate, calcium hydroxide and formocresol for pulpotomies in primary teeth. Int. Endod. J. 2008, 41, 547–555. [Google Scholar] [CrossRef] [PubMed]
- Noorollahian, H. Comparison of mineral trioxide aggregate and formocresol as pulp medicaments for pulpotomies in primary molars. Br. Dent. J. 2008, 204, E20. [Google Scholar] [CrossRef] [PubMed]
- Agamy, H.A.; Bakry, N.S.; Mounir, M.M.; Avery, D.R. Comparison of mineral trioxide aggregate and formocresol as pulp-capping agents in pulpotomized primary teeth. Pediatr. Dent. 2004, 26, 302–309. [Google Scholar]
- Eidelman, E.; Holan, G.; Fuks, A.B. Mineral trioxide aggregate vs. formocresol in pulpotomized primary molars: A preliminary report. Pediatr. Dent. 2001, 23, 15–18. [Google Scholar]
- Mettlach, S.E.; Zealand, C.M.; Botero, T.M.; Boynton, J.R.; Majewski, R.F.; Hu, J.C. Comparison of mineral trioxide aggregate and diluted formocresol in pulpotomized human primary molars: 42-month follow-up and survival analysis. Pediatr. Dent. 2013, 35, E87–E94. [Google Scholar]
- Durmus, B.; Tanboga, I. In vivo evaluation of the treatment outcome of pulpotomy in primary molars using diode laser, formocresol, and ferric sulphate. Photomed. Laser Surg. 2014, 32, 289–295. [Google Scholar] [CrossRef]
- Havale, R.; Anegundi, R.T.; Indushekar, K.; Sudha, P. Clinical and radiographic evaluation of pulpotomies in primary molars with formocresol, glutaraldehyde and ferric sulphate. Oral Health Dent. Manag. 2013, 12, 24–31. [Google Scholar]
- Huth, K.C.; Hajek-Al-Khatar, N.; Wolf, P.; Ilie, N.; Hickel, R.; Paschos, E. Long-term effectiveness of four pulpotomy techniques: 3-year randomised controlled trial. Clin. Oral Investig. 2012, 16, 1243–1250. [Google Scholar] [CrossRef]
- Markovic, D.; Zivojinovic, V.; Vucetic, M. Evaluation of three pulpotomy medicaments in primary teeth. Eur. J. Paediatr. Dent. 2005, 6, 133–138. [Google Scholar]
- Ozmen, B.; Bayrak, S. Comparative evaluation of ankaferd blood stopper, ferric sulfate, and formocresol as pulpotomy agent in primary teeth: A clinical study. Niger J. Clin. Pract. 2017, 20, 832–838. [Google Scholar] [CrossRef] [PubMed]
- Farsi, D.J.; El-Khodary, H.M.; Farsi, N.M.; El Ashiry, E.A.; Yagmoor, M.A.; Alzain, S.M. Sodium hypochlorite versus formocresol and ferric sulfate pulpotomies in primary molars: 18-month follow-up. Pediatr. Dent. 2015, 37, 535–540. [Google Scholar] [PubMed]
- Jayam, C.; Mitra, M.; Mishra, J.; Bhattacharya, B.; Jana, B. Evaluation and comparison of white mineral trioxide aggregate and formocresol medicaments in primary tooth pulpotomy: Clinical and radiographic study. J. Indian Soc. Pedod. Prev. Dent. 2014, 32, 13–18. [Google Scholar] [CrossRef]
- Srinivasan, D.; Jayanthi, M. Comparative evaluation of formocresol and mineral trioxide aggregate as pulpotomy agents in deciduous teeth. Indian J. Dent. Res. 2011, 22, 385–390. [Google Scholar] [CrossRef] [PubMed]
- El Meligy, O.A.E.S.; Alamoudi, N.M.; Allazzam, S.M.; El-Housseiny, A.A.M. BiodentineTM versus formocresol pulpotomy technique in primary molars: A 12-month randomized controlled clinical trial. BMC Oral Health 2019, 19, 3. [Google Scholar] [CrossRef] [PubMed]
- Sunitha, B.; Puppala, R.; Kethineni, B.K.; Mallela, M.; Peddi, R.; Tarasingh, P. Clinical and radiographic evaluation of four different pulpotomy agents in primary molars: A longitudinal study. Int. J. Clin. Pediatr. Dent. 2017, 10, 240–244. [Google Scholar]
- Fernandes, A.P.; Lourenço Neto, N.; Teixeira Marques, N.C.; Silveira Moretti, A.B.; Sakai, V.T.; Cruvinel Silva, T.; Andrade Moreira Machado, M.A.; Marchini Oliveira, T. Clinical and radiographic outcomes of the use of Low-Level Laser Therapy in vital pulp of primary teeth. Int. J. Paediatr. Dent. 2015, 25, 144–150. [Google Scholar] [CrossRef]
- Subramaniam, P.; Konde, S.; Mathew, S.; Sugnani, S. Mineral trioxide aggregate as pulp capping agent for primary teeth pulpotomy: 2 year follow up study. J. Clin. Pediatr. Dent. 2009, 33, 311–314. [Google Scholar] [CrossRef]
- Sonmez, D.; Sari, S.; Cetinbaş, T. A Comparison of four pulpotomy techniques in primary molars: A long-term follow-up. J. Endod. 2008, 34, 950–955. [Google Scholar] [CrossRef]
- Fuks, A.B.; Holan, G.; Davis, J.M.; Eidelman, E. Ferric sulfate versus dilute formocresol in pulpotomized primary molars: Long-term follow up. Pediatr. Dent. 1997, 19, 327–330. [Google Scholar]
- International Agency for Research on Cancer. Pres Release no. 153. 15 June. Available online: www.iarc.fr/ENG/Press_Releases/archives/ pr153a.html (accessed on 16 March 2020).
- Coll, J.A.; Seale, N.S.; Vargas, K.; Marghalani, A.A.; Al Shamali, S.; Graham, L. Primary tooth vital pulp therapy: A systematic review and meta-analysis. Pediatr. Dent. 2017, 39, 16–123. [Google Scholar] [PubMed]
- Lin, P.Y.; Chen, H.S.; Wang, Y.H.; Tu, Y.K. Primary molar pulpotomy: A systematic review and network meta-analysis. J. Dent. 2014, 42, 1060–1077. [Google Scholar] [CrossRef] [PubMed]
- Gandolfi, M.G.; Spagnuolo, G.; Siboni, F.; Procino, A.; Rivieccio, V.; Pelliccioni, G.A.; Prati, C.; Rengo, S. Calcium silicate/calcium phosphate biphasic cements for vital pulp therapy: Chemical-physical properties and human pulp cells response. Clin. Oral. Investig. 2015, 19, 2075–2089. [Google Scholar] [CrossRef] [PubMed]
- Gopalakrishnan, V.; Anthonappa, R.; Ekambaram, M.; King, N.M. Qualitative assessment of published studies on pulpotomy medicaments for primary molar teeth. J. Investig. Clin. Dent. 2019, 10, e12389. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author, Year | Reason of Exclusion |
|---|---|
| Kathal et al. 2017 [18] | The studied material did not present clinical evidence among scientific literature. |
| Alsanouni et al. 2019 [19] | Authors compared the same pulpotomy dressing material. |
| Pratima et al. 2018 [20] | Pulpotomy was performed by diode laser prior to MTA. |
| Kang et al. 2015 [21] | Authors compared the same pulpotomy dressing material. |
| Akcay et al. 2014 [22] | Sodium hypochlorite was applied prior to MTA and might act as a variable. |
| Fernández et al. 2013 [23] | Internal root resorption was not considered as a failure. |
| Liu et al. 2011 [24] | Calcium hydroxide paste was mixed with other agents and the obtained material did not present clinical evidence among scientific literature. |
| Holan et al. 2005 [25] | Internal root resorption was not considered as a failure. |
| Nematollahi 2018 [26] | Authors performed partial pulpotomy that is poorly reproducible and standardizable. |
| Musale et al. 2016 [27] | The studied material did not present clinical evidence among scientific literature. |
| Atasever et al. 2019 [28] | Sodium hypochlorite was used during pulpotomy procedure and might act as a variable. |
| Huth et al. 2005 [29] | The paper reported on the same sample size of Huth et al. 2012. |
| Nguyen et al. 2017 [30] | Pulpotomy was compared with root canal therapy. |
| Saltzman et al. 2005 [31] | Pulpotomy procedures were different between the evaluated groups. |
| Grewal et al. 2016 [32] | The success of the materials was evaluated on dentin thickness without reproducibility and standardization. |
| Hugar et al. 2017 [33] | Incomplete data reported. |
| Kalra et al. 2017 [34] | The studied material did not present clinical evidence among scientific literature. |
| Uloopi et al. 2016 [35] | Pulpotomy procedures were different between the evaluated groups. |
| Yildiz et al. 2014 [36] | No random allocation of the sample size. |
| Ansari et al. 2018 [37] | Absence of rubber dam. |
| Gupta et al. 2015 [38] | Pulpotomy procedures were performed by laser or electrosurgery. |
| Cantekin et al. 2014 [39] | Authors compared the same pulpotomy dressing material. |
| Trairatvorakul et al. 2012 [40] | Authors performed partial pulpotomy that is poorly reproducible and standardizable. |
| Zurn et al. 2008 [41] | Pulpotomy was obtained by light-cured calcium hydroxide. |
| Percinoto et al. 2006 [42] | Corticosteroid/antibiotic solution was applied as therapeutic dressing and might act as a variable. |
| Ghoniem et al. 2018 [43] | No random allocation of the sample size. |
| Biedm-Perea et al. 2017 [44] | Retrospective study and no random allocation of the sample size. |
| Airen et al. 2012 [45] | Retrospective study and no random allocation of the sample size. |
| Frenkel et al. 2012 [46] | No random allocation of the sample size. |
| Cardoso Silva et al. 2011 [47] | No random allocation of the sample size. |
| Ibricevic et al. 2003 [48] | Retrospective study. |
| Godhi et al. 2011 [49] | No random allocation of the sample size. |
| Hugar et al. 2010 [50] | No random allocation of the sample size. |
| Ibricevic et al. 2000 [51] | No random allocation of the sample size. |
| Random Sequence Generation | Allocation Concealment | Blinding of Participants and Personnel | Blinding of Outcome Assessment | Incomplete Outcome Data | Selective Outcome Reporting | |
|---|---|---|---|---|---|---|
| Çelik et al. 2019 [52] | Low | Unclear | High | Low | Low | Low |
| Malekafzali et al. 2011 [53] | Unclear | High | High | Low | Unclear | Unclear |
| Sakai et al. 2009 [54] | Low | High | High | Low | High | High |
| Farsi et al. 2005 [55] | Low | Unclear | Unclear | Unclear | High | High |
| Carti et al. 2017 [56] | Low | High | High | Unclear | Low | Low |
| Guven et al. 2017 [57] | Low | High | Low | Low | Low | Low |
| Bani et al. 2017 [58] | Low | Unclear | Unclear | High | Low | Low |
| Juneja et al. 2017 [59] | Low | Unclear | Unclear | Low | Low | Low |
| Togaru et al. 2016 [60] | Unclear | High | High | High | Low | Low |
| Rajasekharan et al. 2017 [61] | Low | Low | Low | Low | Low | Low |
| Cuadros-Fernández et al. 2016 [62] | Low | Unclear | High | High | Low | Low |
| Silva et al. 2019 [63] | Low | Low | Low | Low | Low | Low |
| Junqueira et al. 2018 [64] | Low | Unclear | High | Low | High | Low |
| Jamali et al. 2018 [65] | Low | Unclear | Low | Low | High | Low |
| Yildirim et al. 2016 [66] | Unclear | Unclear | High | High | Low | Low |
| Olatosi et al. 2015 [67] | Unclear | Unclear | High | High | Low | Low |
| Celik et al. 2013 [68] | Low | Low | Low | Low | Low | Low |
| Oliveira et al. 2013 [69] | Low | Unclear | High | Low | Low | Low |
| Sushynski et al. 2012 [70] | Unclear | Unclear | High | Low | Low | Low |
| Erdem et al. 2011 [71] | Unclear | Unclear | Low | High | Low | Low |
| Ansari et al. 2010 [72] | Unclear | Unclear | High | Unclear | Low | Low |
| Doyle et al. 2010 [73] | Low | Low | Unclear | Low | Unclear | Low |
| Moretti et al. 2008 [74] | Low | Unclear | High | Low | Low | Low |
| Noorollahian 2008 [75] | Low | Unclear | High | Low | High | Low |
| Agamy et al. 2004 [76] | Unclear | Unclear | High | Low | Low | Low |
| Eidelman et al. 2001 [77] | Low | Unclear | High | High | High | Low |
| Mettlach et al. 2013 [78] | Low | Unclear | High | Low | High | Low |
| Durmus et al. 2014 [79] | Unclear | Unclear | High | Low | Low | Low |
| Havale et al. 2013 [80] | Unclear | Unclear | High | Unclear | Low | Low |
| Huth et al. 2012 [81] | Low | Low | Low | Low | Low | Low |
| Markovic et al. 2005 [82] | Unclear | Unclear | High | Unclear | Low | Low |
| Ozmen et al. 2017 [83] | Low | Unclear | High | High | Low | Low |
| Farsi et al. 2015 [84] | Low | Low | Low | Low | Low | Low |
| Jayam et al. 2014 [85] | Unclear | Unclear | High | High | Low | Low |
| Srinivasan et al. 2011 [86] | Unclear | Unclear | High | Low | Low | Low |
| El Meligy et al. 2019 [87] | Low | Low | Low | Low | Low | Low |
| Sunitha et al. 2017 [88] | Unclear | Unclear | High | High | Low | Low |
| Fernandes et al. 2015 [89] | Low | Unclear | High | Low | Low | High |
| Subramaniam et al. 2009 [90] | Low | Unclear | High | High | Low | Low |
| Sonmez et al. 2008 [91] | Unclear | Unclear | High | High | Low | Low |
| Fuks et al. 1997 [92] | Low | Unclear | High | Unclear | Low | Unclear |
| Material | Groups Distribution | Type of Definitive Restorations | Follow-up | Evaluated Outcomes | Reported Outcomes | Conclusions | |||
|---|---|---|---|---|---|---|---|---|---|
| Clinical | Radiographical | Clinical | Radiographical | ||||||
| Çelik et al. 2019 [52] | MTA* vs. BD° | MTA group (n = 24) BD group (n = 20) | IRM and SCC | 12, 18 and 24 months. | Absence of spontaneous pain and/ or sensitivity to palpation/percussion; absence of fistula, swelling, and/or abnormal mobility. | Absence of radiolucencies at the inter-radicular and/or periapical regions, absence of pulp canal obliteration (fully obliterated canals); absence of internal or external (pathologic) resorption that was not compatible with a normal exfoliation process. | MTA = 100% success rate at 12, 18 and 24 months. BD = 89.4% success rate at 12, 18 and 24 months. | MTA = 100% success rate at 12, 18 and 24 months. BD = 89.4% success rate at 12, 18 and 24 months. | MTA and BD showed similar success rates without any statistically significant difference. |
| Malekafzali et al. 2011 [53] | MTA* vs. CEM§ | MTA group (n = 40) CEM group (n = 40) | SCC or amalgam depending on the cavity size | 12 and 24 months | Swelling/abscess, sinus tract, spontaneous pain, and or pathological mobility. | Furcation radiolucency, periapical bone destruction, internal root resorption, and pathological external root resorption. | MTA = 100% success rate at 12, 18 and 24 months. CEM = 100% success rate at 12, 18 and 24 months. | One and three cases of pathologic external root resorption were observed in CEM and MTA groups at 12-month follow-up, respectively, without significant difference. In the last follow-up (24 months) MTA and CEM achieved 100% radiographic success. | The study demonstrated favorable treatment outcomes of CEM/MTA pulpotomy in human primary molar teeth. CEM as a new endodontic cement is a promising biomaterial. |
| Sakai et al. 2009 [54] | Grey MTA** vs. PC# | MTA group (n = 15) PC group (n = 15) | IRM and GIC | 12, 18 and 24 months | Absence of spontaneous pain, mobility, swelling, fistula, or smell. | Absence of internal root resorption or furcation radiolucency. | 100% of the available teeth were clinically and radiographically successful during all the follow-ups. | 100% of the available teeth were clinically and radiographically successful during all the follow-ups | The present data suggested that PC might serve as an effective and less expensive MTA substitute in primary molar pulpotomies. |
| Farsi et al. 2005 [55] | MTA vs. FC (both not specified) | MTA group (n = 60) FC group (n = 60) | IRM was placed prior to restoration with SCC. | 12, 18 and 24 months | Absence of pain; swelling; sinus tract; mobility; or pain on percussion. | Absence of internal root resorption; furcation radiolucency; periapical radiolucency; or widening of the periodontal ligament space. | After 24 months, the FC group showed only one case reported pain. On the other hand, 100% of teeth treated with MTA were considered clinically successful. | At the end of the study, the FC group showed five cases with pulp pathosis (13.2%). MTA showed 100% of radiographical success. | MTA might be considered as a valid alternative to FC. |
| Carti et al. 2017 [56] | MTA (not specified) vs. BD° | MTA group (n = 25) BD group (n = 25) | - MTA group: GIC and SCC cemented with GIC. - BD group: the cavity was filled with BD and then restored by using a SCC cemented with GIC. | 12 months | Absence of palpation–percussion sensitivity, spontaneous pain, hot–cold sensitivity, presence of fistula-swelling, pathologic mobility. | Absence of internal–external resorption, periapical/interradicular bone destruction, disintegration of the lamina dura, enlargement of the periodontal space, and radiological calcific metamorphosis. | There was no statistically significant difference between clinical success rates over time. In both groups one tooth was extracted due to fistula formation at month 12. | The success rates were 80% and 60% for MTA and BD groups, respectively. There were no statistically significant differences between the groups. | Both MTA and BD could be used as pulpotomy agents, but more long-term studies with larger sample sizes are required. |
| Guvenet al. 2017 [57] | MTA-P*** vs. PR-MTA* vs. BD° vs. FS (not specified) | MTA-P group (n = 29) PR-MTA group (n = 29) BD group (n = 29) FS group (n = 29) | - MTA groups: GIC was placed over the MTA. - BD group: permanent restoration was performed on the same session with GIC. - FS group: a ZOE base, then GIC | 12 and 24 months | Absence of swelling, pain, fistula, or pathologic mobility. | Absence of evidence of internal or external resorption or periradicular radiolucency. | 24-month: no clinical failure was observed among groups. Total success rates of the BD, MTA-P, PR-MTA and FS groups were 82.75%, 86.2%, 93.1% and 75.86%, respectively. No statistically significant differences in total success rates were observed over time. | Overall, seven teeth demonstrated radiographic failure at 24 months. | This study found no statistically significant differences among pulpotomy techniques; however, calcium-silicate-based materials appeared to be clinically more appropriate than FS. |
| Bani et al. 2017 [58] | MTA* vs. BD° | MTA group (n = 32) BD group (n = 32) | GIC and SCC | 12, 18 and 24 months | Absence of tenderness to percussion, swelling, pain, fistula, or pathologic mobility. | Absence of internal or external resorption; furcal or periradicular radiolucency; widening of periodontal ligament spaces. | The 24-month follow-up evaluations revealed that the clinical success rates were 96.8% for both BD and MTA groups. | The radiographic success rates at 24 months were 93.6% for BD and 87.1% for MTA. | BD and MTA did not differ significantly in combined clinical and radiographic success after 24 months. However, BD showed slightly better radiographical results after two years of follow-up. |
| Juneja et al. 2017 [59] | MTA* vs. BD° vs. FC (not specified) | MTA group (n = 17) BD group (n = 17) FC group (n = 17) | All teeth were immediately restored with IRM and GIC, then were restored with pre-formed metal crowns. | 12 and 18 months | Absence of pain, tenderness to percussion/palpation, swelling, intraoral/extraoral sinus, pathologic mobility. | Absence of internal or external resorption; furcal or periradicular radiolucency. | 100% of available teeth for MTA and BD groups were clinically successful, and 73.3% of the FC group. There were statistically significant differences between FC and MTA and BD at 12 and 18 months, respectively. | Radiographic success rate for the FC group at 18 months follow up was 73.3% for FC, 100% for MTA and 86.6% for BD group. There were statistically significant differences between FC and MTA at 12 and 18 months. | MTA and BD showed more favorable results than FC. |
| Togaru et al. 2016 [60] | MTA* vs. BD° | MTA group (n = 45) BD group (n = 45) | Permanent restoration with GIC followed by SCC | 12 months | Absence of pain, tenderness on percussion, swelling and/or fistula, pathologic tooth mobility. | Absence of radiolucency in furcation/periapical area, internal or external root resorption, and widening of periodontal space. | 12 months: MTA and BD provided 95.5% of success rate. | 12 months: MTA and BD provided 95.5% of success rate. Radiographic examination provided 1 failure in both MTA and BD groups. No statistical differences were detected. | Pulpotomy treatment using BD and MTA had similar success rates in primary teeth. |
| Rajasekharanet al. 2017 [61] | MTA* vs. BD° vs. TP## | MTA group (n = 29) BD group (n = 25) TP group (n = 27) | GIC and SCC | 12 and 18 months | Absence of pain, tenderness on percussion, swelling and/or fistula, pathologic tooth mobility, chewing sensitivity, gingival inflammation, periodontal pocket formation, sinus tract present, premature tooth loss due to pathology. | Absence of radiolucency in furcation/periapical area, internal or external root resorption, and widening of periodontal space, variation radiodensity. | Clinical success was 95.24%, 100% and 95.65% in the BD, MTA and TP groups, respectively. | Radiographic success was 94.4%, 90.9% and 82.4% in the BD, MTA and TP groups, respectively | After 18-month follow-up, there was no significant difference between BD in comparison with MTA or TP. |
| Cuadros-Fernández C et al. 2016 [62] | MTA* vs. BD° | MTA group (n = 43) BD group (n = 41) | IRM and SCC. | 12 months | Absence of pain, swelling or gingival inflammation, fistulation, or pathologic mobility. | Absence of evidence of internal or external resorption or periradicular radiolucency. | The clinical success rate in the MTA group after 12 months was 92% (36/39), whereas the clinical success rate in the BD group after 12 months was 97% (38/39). | MTA yielded a radiographic success of 97% (38/39). Use of BD yielded a radiographic success of 95% (37/39). | BD showed similar clinical results as MTA with comparable success rates when used for pulpotomies of primary molars. |
| Silva et al. 2019 [63] | MTA** (only gray), CH (not specified) with saline (CH+saline group) and CH with polyethylene glycol (CH+PEG group) | MTA group (n = 15) CH+saline group (n = 15) CH+PEG group (n = 15) | 1-mm-thick layer of material was used for capping, followed by another 1-mm-thick of a layer of cement-cured CH°° employed as an intermediate base for the restoration GIC | 12 months | Lack of spontaneous pain, mobility, swelling, or fistula in the treated tooth. | Lack of internal or external root resorption and furcation radiolucency were indicative of radiographic success. | Clinical analysis showed 100% treatment success using MTA, at all follow-up appointments. | Radiographic analysis showed 100% treatment success using MTA, at all follow-up appointments. At 12 months of follow-up, the CH+saline group had an increased incidence of radiographic failure compared with the MTA group. | The association of CH with PEG provided better results than that of CH + saline as a capping material for pulpotomy of primary teeth. However, both associations demonstrated clinical and radiographic results inferior to those of MTA. |
| Junqueira et al. 2018 [64] | MTA** vs. FS§§ | MTA (n = 15) FS (n = 16) | IRM was placed prior to the restoration with GIC | 12 and 18 months | Absence of spontaneous pain, mobility, swelling or fistula. | Absence of internal root resorption, inter-radicular radiolucency and periapical lesion were absent. Hard tissue barrier formation and stenosis were considered as radiographic successes; tooth discoloration was not considered as a failure. | In both groups, 100% of the available teeth were clinically successful during all the follow-up appointments. | The radiographic success rate for both groups was 100% at 12 months. At the end of the 18-month follow-up period, one tooth from FS group presented a radiographic failure (inter-radicular radiolucency), but it was not statistically different from MTA group. | Based on this study, both MTA and 15.5% FS are effective for pulpotomies of primary teeth. Although MTA is considered the first choice material, FS may be a suitable alternative when treatment cost is an issue. |
| Jamali et al. 2018 [65] | 3Mixtatin vs. FC°°° vs. MTA** | 3Mixtatin group (n = 50) FC group (n = 50) MTA group (n = 50) | IRM and amalgam | 12 and 24 months | Absence of sinus tract, tenderness to palpation and percussion, spontaneous pain or pain of long duration, swelling, pain of other sources mimicking irreversible pulpitis such as a gingival problem, food impaction, etc. | Absence of external or internal root resorption, inter-radicular radiolucency and periapical lesion. | The overall success rate was 78.9% for FC, 90.5% for 3Mixtatin and 88.1% for MTA group. There was no significant difference in overall success rate among the groups after 24-month follow-up. | The overall success rate was 78.9% for FC, 90.5% for 3Mixtatin and 88.1% for MTA group. There was no significant difference in overall success rate among the groups after 24-month follow-up. | The present study showed that 3Mixtatin can be utilized as a pulp capping material in pulpotomy of primary teeth owing to its successful clinical and radiographic outcomes after 24 months of follow-up period. |
| Yildirim et al. 2016 [66] | FC°°° vs. MTA* vs. PC# vs. EMP | FC group (n = 35) MTA group (n = 35) PC group (n = 35) EMP group (n = 35) | GIC and SCC | 12 and 24 months | Absence of spontaneous pain, swelling, fistula | Absence of radiolucency of the periapical or furcation, and pathological external root resorption, internal root resorption | 24 months: FC = 96.9%, MTA = 100%, PC = 93.3%, EMD = 90.6%. | 24 months: FC = 96.9%, MTA = 100%, PC = 93.3%, EMD = 90.6%. | This study demonstrated that MTA had better long-term clinical success rates than FC, PS and EMP, respectively. |
| Olatosi et al. 2015 [67] | FC§§§ vs. White MTA* | MTA group (n = 25) FC group (n = 25) | SSC | 12 months | Absence of symptoms of pain, tenderness to percussion, swelling or sinus tract, pathologic tooth mobility. | Absence of periodontal ligament widened, furcation or periapical radiolucency, active/progressing internal root resorption, pathologic external root resorption. | The clinical success rate at 12 months was 100% and 81% for MTA and FC, respectively. The difference was statistically significant. | The radiographic success rates for MTA and FC were 96% and 81%, respectively. There was no statistically significant difference between the two agents. | MTA showed clinical and radiographic success as a dressing material following pulpotomy procedure in primary teeth, and it has a promising potential to become a replacement for FC in primary molars. |
| Celik et al. 2013 [68] | MTA*(P-MTA) vs. MTA** (A-MTA) vs. CH (not specified) | P-MTA group (n = 46) A-MTA group (n = 45) CH group (n = 48) | GIC and amalgam | 12, 18 and 24 months | Absence of spontaneous pain, sensitivity to palpation/percussion, fistula, swelling, abnormal mobility. | Absence of radiolucencies at the inter-radicular and/or periapical regions, pulp canal obliteration (fully obliterated canals), internal or external resorption. | Comparisons using the log-rank test showed that the clinical survival probabilities of P-MTA and A-MTA were similar and significantly greater than that of the CH group, respectively. | The 24-month cumulative radiographic survival probabilities of the P-MTA, A-MTA, and CH groups were 0.974, 0.908, and 0.446, respectively. Most radiographic failures were associated with internal resorption, which was observed in 23 teeth in the CH group, compared to none in the P-MTA and three in the A-MTA groups. | Based on the results of this study, P-MTA and A-MTA showed high clinical and radiographic success rates as pulpotomy agents in primary molars. CH showed considerably less clinical and radiographic success than the MTA cements. |
| Oliveira et al. 2013 [69] | CH† vs. MTA** vs. PC# | CH group (n = 15) MTA group (n = 15) PC group (n = 15). | IRM and GIC | 12 and 24 months | Absence of spontaneous pain, mobility, swelling and fistula. | Absence of internal root resorption and furcation radiolucency. | Clinically, the MTA and PC groups showed 100 % success rates at 12 and 24 months. | Radiographically, the MTA and PC groups showed 100 % success rates at 12 and 24 months. | MTA and PC might serve as effective materials for pulpotomies of primary teeth as compared to CH. Although results are encouraging, further studies and longer follow-up assessments are needed in order to determine the safe clinical indication of Portland cement. |
| Sushynski et al. 2012 [70] | Gray MTA* vs. DFC | MTA group (n = 119) DFC group (n = 133) | IRM and SSC | 24 months | Absence of mobility, percussion or chewing sensitivity, gingival inflammation, pathology, periodontal pocket formation, spontaneous pain, sinus tract presence, premature tooth loss due to pathology. | Absence of internal root resorption (nonperforated/perforated); external root resorption; dentin bridge formation; pulp canal obliteration/calcific metamorphosis; furcal/periradicular radiolucencies, widening of the periodontal ligament space; periapical bone destruction; physiological root resorption. | All teeth in the MTA group were judged to be clinically successful (100%), whereas 1% of teeth in the DFC group were judged to have failed from 6 to 24 months (success ~99%). The differences between groups were not significant at all follow-up points. | At the 24-month follow-up 62/65 (~95%) molars of the MTA group were radiographically successful, while only 50/66 (~76%) molars of the DFC group demonstrated radiographic success. | MTA demonstrated significantly better radiographic outcomes vs. the DFC. However, both pulpal agents, presented comparable clinical outcomes after two years of follow-up. |
| Erdem et al. 2011 [71] | MTA* vs. FS§§ vs. DFC vs. ZOE | MTA group (n = 32) FS group (n = 32) FC group (n = 32) ZOE group (n = 32) | amalgam | 12 and 24 months | Absence of spontaneous pain or after percussion, mobility, swelling. | Absence of internal root resorption and furcation and/or periapical bone destruction. | 12 months success: 100% for MTA, FC and FS., and 92% for ZOE. 24 months success: 96% MTA, 88% FS, 88% FC and ZOE 68%. | 12 months success: 100% for MTA, FC and FS., and 92% for ZOE. 24 months success: 96% MTA, 88% FS, 88% FC and ZOE 68%. | ZOE, as the only pulpotomy medicament, had a significantly lower success rate than MTA. No significant differences were observed, among the 3 experimental materials (MTA, FC and FS) at two years follow-up. |
| Ansari et al. 2010 [72] | MTA* vs. DFC | MTA group (n = 20) FC group (n = 20) | SSC | 12 and 24 months | Absence of pain, presence of gingival swelling and sinus tract. | Absence of internal resorption, radiographic signs of pathosis (periapical radiolucency). | The number of teeth judged as failed was six in the FC-treated group with only one failed case in the MTA-treated group | Overall radiographic success at 24th month was observed in > 95% of MTA group and 90% of FC group | Pulpotomy of primary teeth performed with MTA demonstrated comparable results of FC-treated teeth. |
| Doyle et al. 2010 [73] | MTA* vs. FS§§ vs. Eugenol-free FS§§ vs. FS/MTA | FS group (n = 58) MTA group (n = 57) Eugenol-free FS group (n = 78) FS/MTA group (n = 77) | IRM and SSC | 12, 24 and 36 months | Absence of SCC perforation, mobility, percussion sensitivity, palpation sensitivity, soft tissue pathology. | Absence of widening of the periodontal ligament space, furcal/periradicular radiolucencies, pulp canal obliteration, internal or external root resorption. | Eugenol-free FS molars demonstrated significantly lower survival rates than MTA ones, over 6 to 38 months. | MTA molars demonstrated significantly fewer radiographical changes than FS ones. Eugenol-free FS showed significantly more radiographical changes than MTA or FS/MTA. | MTA showed statistically significant better performances than FS and Eugenol-free FS |
| Moretti et al. 2008 [74] | MTA** vs. CH°° vs. DFC | MTA group (n = 15) CH group (n = 15) DFC group (n = 15) | IRM and GIC | 12, 18 and 24 months | Absence of spontaneous pain, mobility, swelling, fistula and smell. | Absence of internal root resorption, inter-radicular bone destruction and furcation radiolucency. | Both groups showed100% of clinical success during all the follow-up appointments. The CH group demonstrated 64% of success. | Both groups showed 100% radiographical success during all the follow-up appointments. The CH group demonstrated 64% success; in the same group, internal resorption was a frequent radiographic finding. | MTA was superior to CH and equally effective to DFC as a pulpotomy agent in primary molars. |
| Noorollahian 2008 [75] | MTA* vs. DFC | MTA group (n = 30) DFC group (n = 30) | SSC | 12 and 24 months | Absence of pain symptoms, tenderness to percussion, swelling, fistulation or pathologic mobility. | Absence of radicular radiolucency, internal or external root resorption, periodontal ligament space widening. | After 24 months 100% of DFC and MTA teeth were clinically successful. | After 24 months 100% of DFC teeth were radiographically successful. The radiographic follow-up evaluation revealed one failure (furcation involvement) in 18 molars treated with MTA after 24 months. | MTA could be used as a safe pulpotomy agent in cariously exposed primary molars and might be used as alternative to FC. |
| Agamy et al. 2004 [76] | Gray MTA (G-MTA) vs. White MTA (W-MTA) vs. FC (all not specified) | G-MTA group (n = 24) W-MTA group (n = 24) FC group (n = 24) | IRM and SSC | 12 months | Absence of pain symptoms; tenderness to percussion; swelling; fistulation; pathologic mobility. | Absence of internal or external root resorption; periodontal ligament space widening. | At the 12-month evaluation, 100% of G-MTA teeth were clinically successful, while in the W-MTA group 3/18 showed clinical failure as well as two teeth in FC group. | At the 12-month evaluation, 100% of G-MTA teeth were radiographically successful, while in the W-MTA group 3/18 showed radiographical failure as well as two teeth in FC group. | In conclusion, G-MTA was superior to both W-MTA and FC as a pulp dressing agent for pulpotomized primary molars. |
| Eidelman et al. 2001 [77] | MTA vs. FC (both not specified) | MTA group (n = 30) FC group (n = 30) | SSC | 30 months | Absence of pain; swelling; sinus tract. | Absence of internal root resorption; furcation radiolucency; periapical bone destruction. | MTA and FC showed 100% of clinical success. The follow-up evaluations revealed only one failure (internal resorption detected at 17-month postoperative evaluation) in a molar treated with FC. | MTA showed 100% of radiographical success. The evaluation of FC group, revealed only one failure (internal resorption). Pulp canal obliteration was observed in 9 of 32 (28%) evaluated molars. This finding was detected in 2/15 teeth treated with FC (13%) and in 7/17 treated with MTA (41%). | MTA showed promising clinical and radiographic success as a dressing material in the pulpotomy procedure of primary teeth. |
| Mettlach et al. 2013 [78] | Gray MTA* vs. DFC | MTA group (n = 119) FC group (n = 133) | IRM and SSC | 12, 18, 24, 30, 36, 42 months | Authors stated that clinical success was scored based on modified scales adopted by Zurn and Seale. | Absence of pathologic nonperforated and perforated internal root resorption; external root resorption; inter-radicular or periapical bone destruction. | One tooth in the MTA group was judged to be a clinical failure (99% of success), and four teeth in the DFC group were judged to have failed (99% of success). There was no significant difference found between groups. | MTA group yielded a 95% of radiographical success, whereas DFC group showed 79%. This difference was found to be significant. | Gray MTA performed statistically better than DFC. |
| Durmus et al. 2014 [79] | DL vs. DFC vs. FS§§ | DL group (n = 40) FC group (n = 40) FS group (n = 40) | GI and SCC | 12 months | Absence of spontaneous pain, percussion/palpation, abscess, swelling, fistula, pathologic mobility. | Absence of periapical radiolucency, widened periodontal ligament space, pathologic internal/external root resorption, pathological changes of the alveolar bone in the furcation area. | After 12 months, a clinical success rate of 100%, 92.5% and 97% was observed in DL, FS and FC group, respectively. No statistically significant differences were detected between groups. | After 12 months, a radiographic success rate of 75%, 79% and 87% was observed in DL, FS and FC group, respectively. No statistically significant differences were detected between groups. | Pulpotomy performed with FS and FC provided comparable results. Although DL pulpotomy seemed to offer promising clinical success, it yielded low radiographic success rate. |
| Havale et al. 2013 [80] | FC### vs. GA vs. FS§§ | FC group (n = 30) GA group (n = 30) FS (n = 30) | SSC | 12 months | Absence of pain, tenderness, swelling, fistula formation, pathologic mobility. | Absence of widening of the periodontal ligament space, internal root resorption, external root resorption, pathological interradicular radiolucency, calcification of canal. | Clinical success was 96.7% for FS, 86.7% for FC and 100% for GA | Radiological success rates in FC, GA, and FS groups were 56.7%, 83.3% and 63.3%, respectively. | Although GA seemed the most efficient, FS and FC did not show statistically significant differences. |
| Huth et al. 2012 [81] | DFC vs., Er:YAG vs. CH†† vs. FS§§ | FC group (n = 50) Er:YAG group (n = 50) CH group (n = 50) FS group (n = 50) | IRM and GI and SSC or composite resin restoration | 12, 18, 24 and 36 months | Absence of spontaneous pain, tenderness to percussion, fistula, soft tissue swelling, pathological tooth mobility. | Absence of periapical or furcal radiolucency, pathologic external or distinct internal root resorption, widened periodontal ligament space. | After 36 months clinical success rates were: 92% for FC, 89% for Er:YAG, 75% for CH and 97% for FS. | Overall success after 36 months were: 72% for FC, 73% for Er:YAG, 46% for CH and 76% for FS. | After 36 months, CH was the least effective pulpotomy material, and FS was the most effective; however, FS did not show significant differences with FC. The Er:YAG laser showed comparable outcomes to FC. |
| Markovic et al. 2005 [82] | FS§§ vs. CH (not specified) vs. FC††† | FC group (n = 33) CH group (n = 34) FS group (n = 37) | GIC and amalgam | 12 and 18 months | Absence of spontaneous pain, abnormal mobility, tenderness to percussion, fistula. | Absence of pathological changes of the alveolar bone in the apical and/or furcation area (visible periapical or inter-radicular radiolucency), integrity of lamina dura, pathological internal resorption, external root resorption. | The clinical success rate at 18 months for the FC and FS groups was 90.9% and 89.2% respectively. CH group showed an overall lower clinical success of 82.3%, although differences were not statistically significant. | RX success: FC 84.4%, CH 76.5%, and FS 81.1%. The differences between groups were not significant. | FS pulpotomy provided favorable clinical and radiographic success rates, comparable to FC pulpotomy. CH showed the worse performance among groups. |
| Ozmen et al. 2017 [83] | DFC vs. ABS vs. FS**** | DFC group (n = 15) ABS group (n = 15) FS group (n = 15) | amalgam (in case of Class I cavities) or SCC (in case of Class II cavities) | 24 months | Absence of spontaneous or severe pain, pathological mobility, swelling, sinus tract, tenderness to percussion, palpation. | Absence of furcal or periapical radiolucency, widened periodontal ligament spaces, internal or external root resorption, loss of lamina dura. | At the end of 24 months, the clinical success rates for ABS, DFC and FS were 87%, 87% and 100%, respectively. | RX success: DFC 80%, ABS 87%, FS 87%. | Comparable success was achieved using ABS, FC and FS as pulpotomy agents of deciduous teeth. |
| Farsi et al. 2015 [84] | NaOCl vs. DFC vs. FS (not specified) | NaOCl group (n = 27) DFC group (n = 27) FS group (n = 27) | ZOE and SCC cemented with GIC. | 12 and 18 months | Absence of pain, swelling, sinus tract, mobility, pain on percussion. | Absence of internal root resorption, furcation radiolucency, periapical radiolucency, widening of the periodontal ligament space. | 18 months: the clinical success rates were NaOCl 83.3%, FC 96%, FS 87%, respectively. | 18 months: rx success rates were NaOCl 91.7%, FC 100%, FS 91.3%, respectively. | Comparable results were obtained using NaOCl, DFC and FS as pulpotomy agents for primary molars. |
| Jayam et al. 2014 [85] | white MTA** vs. FC°°°° | MTA group (n = 50) FC group (n = 50) | SCC and/or GI and amalgam. | 24 months | Absence of history of pain, tenderness to palpation/percussion, pathological mobility, intra- or extra-oral swelling, intra- or extra-oral sinus. | Absence of integrity of lamina, radiolucencies in the apical or bifurcation areas of tooth, pathological internal or external root resorption. | MTA success rate was 100% in comparison to 90.48% success in FC group. | MTA success rate was 100% in comparison to 90.48% success in FC group. | MTA provided promising results as pulpotomy dressing material. |
| Srinivasan et al. 2011 [86] | MTA** vs. DFC | MTA group (n = 50) DFC group (n = 50) | SSC | 12 months | Absence of spontaneous pain, draining fistula, swelling or abscess, mobility, premature exfoliation, | Absence of abnormal root resorption, internal root resorption, furcation involvement, periapical bone destruction. | After 12 months, DFC clinical success rate was 91.3%. In the MTA group, no clinical signs and symptoms were noted; thus, the clinical success was 100%. | Radiographic success rates were 78.26% and 95.74%, in DFC and MTA group, respectively. | MTA seemed to be clinically and radiographically superior to FC. |
| El Meligy et al. 2019 [87] | DFC vs. BD° | DFC group (n = 50) BD group (n = 50) | SSC | 12 months | Absence of pain, swelling, tenderness to percussion, fistula, abnormal tooth mobility. | Absence of periodontal ligament space, periapical and furcation pathosis, internal resorption. | 100% clinical success rates for both groups. | The BD group had a radiographic success rate of 100% at 12-month follow-up, while the DFC group had a success rate of 98.1% at 12 months. | BD and DFC pulpotomy techniques demonstrated favorable clinical and radiographic results in primary teeth, after a 12-month follow-up without any significant differences. |
| Sunitha et al. 2017 [88] | FC (not specified) vs. MTA* vs. EMP vs. PT | FC group (n = 50) MTA group (n = 50) EMP group (n = 50) PT group (n = 50) | SSC | 12, 18 and 24 months | Absence of pain, swelling or abscess, sinus tract opening, mobility, pain on percussion. | Absence of pathological root resorption, widening of periodontal space, bifurcation radiolucency, and periapical radiolucency. | Clinical evaluation: FC 94%; PT 94%; MTA 100%; EMP 83%. | Rx success: FC 88%; PT 83%; MTA 94%; EMP 72%. | MTA was demonstrated to be a valid alternative to FC in pulpotomy procedures. PT and EMP were also proven to be promising agents. |
| Fernandes et al. 2015 [89] | CH (not specified) vs. DFC vs. LLLT vs. LLLT+ CH | CH group (n = 15) DFC group (n = 15) LLLT group (n = 15) LLLT+ CH group (n = 15) | IRM and GIC | 12, and 18 months | Absence of spontaneous pain, mobility, swelling, fistula. | Absence of internal or external root resorption and furcation radiolucency. | All the groups were clinically successful over the follow-up period. | At 18 months follow-up, the radiographic success rate for the DFC group was 100%, 66.7% for CH group, 73.3% for LLLT group, and 75% for LLLT + CH group. | DFC provided the best results over the follow-up period. However, LLLT might be considered as an adjuvant alternative for vital pulp therapy on human primary teeth. |
| Subramaniam et al. 2009 [90] | MTA* vs. FC°°°° | MTA group (n = 20) FC group (n = 20) | SSC | 24 months | Absence of pain, tenderness to percussion, gingival abscess, sinus/fistula, pathologic mobility. | Absence of internal root resorption, external root resorption, periapical/furcal radiolucency. | At the 12th month of evaluation a success rate of 95% and 85% was seen in the MTA and FC groups, respectively. | At the 12th month of evaluation a success rate of 95% and 85% was seen in the MTA and FC groups, respectively. | MTA provided highly promising results as pulpotomy agent. |
| Sonmez et al. 2008 [91] | DFC vs. FS (not specified) vs. CH (vs. MTA* | MTA group (n = 15) CH group (n = 15) DFC group (n = 15) FS group (n = 15) | amalgam (FS, DFC and CH groups) IRM and amalgam; (MTA group) | 24 months | Absence of symptoms of pain, tenderness to percussion, swelling, fistulization, pathological mobility. | Absence of periradicular or interradicular radiolucency, internal or external root resorption, periodontal ligament space widening. | The success rates of CH (46.1%) and MTA (66.6%) were lower than FC (76.9%) and FS (73.3 %), although not statistically significant. | The success rates of CH (46.1%) and MTA (66.6%) were lower than FC (76.9%) and FS (73.3%), although not statistically significant. | CH appeared to clinically be less appropriate than FC, FS and MTA as pulpotomy dressing material. |
| Fuks et al. 1997 [92] | FC§§ and DFS | DFC group (n = 38) FS group (n = 58) | IRM and SSC | 12-35 months (mean 20.5 months) | Absence of pain, swelling, sinus tract. | Absence of internal root resorption, furcation radiolucency, periapical bone destruction. | Total success rates of pulpotomies with FS and DFC were 92.7% and 83.8%, respectively. | Total success rates of pulpotomies with FS and DFC were 92.7% and 83.8%, respectively. | FS and DFC provided similar results. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bossù, M.; Iaculli, F.; Di Giorgio, G.; Salucci, A.; Polimeni, A.; Di Carlo, S. Different Pulp Dressing Materials for the Pulpotomy of Primary Teeth: A Systematic Review of the Literature. J. Clin. Med. 2020, 9, 838. https://doi.org/10.3390/jcm9030838
Bossù M, Iaculli F, Di Giorgio G, Salucci A, Polimeni A, Di Carlo S. Different Pulp Dressing Materials for the Pulpotomy of Primary Teeth: A Systematic Review of the Literature. Journal of Clinical Medicine. 2020; 9(3):838. https://doi.org/10.3390/jcm9030838
Chicago/Turabian StyleBossù, Maurizio, Flavia Iaculli, Gianni Di Giorgio, Alessandro Salucci, Antonella Polimeni, and Stefano Di Carlo. 2020. "Different Pulp Dressing Materials for the Pulpotomy of Primary Teeth: A Systematic Review of the Literature" Journal of Clinical Medicine 9, no. 3: 838. https://doi.org/10.3390/jcm9030838
APA StyleBossù, M., Iaculli, F., Di Giorgio, G., Salucci, A., Polimeni, A., & Di Carlo, S. (2020). Different Pulp Dressing Materials for the Pulpotomy of Primary Teeth: A Systematic Review of the Literature. Journal of Clinical Medicine, 9(3), 838. https://doi.org/10.3390/jcm9030838