Antithrombotic Strategies in Patients with Atrial Fibrillation Following Percutaneous Coronary Intervention: A Systemic Review and Network Meta-Analysis of Randomized Controlled Trials

 ,
,
Abstract
:1. Introduction
2. Method
2.1. Study Selection, Search Strategy and Outcome Measures
2.2. Statistical Analysis and Risk of Bias
3. Results
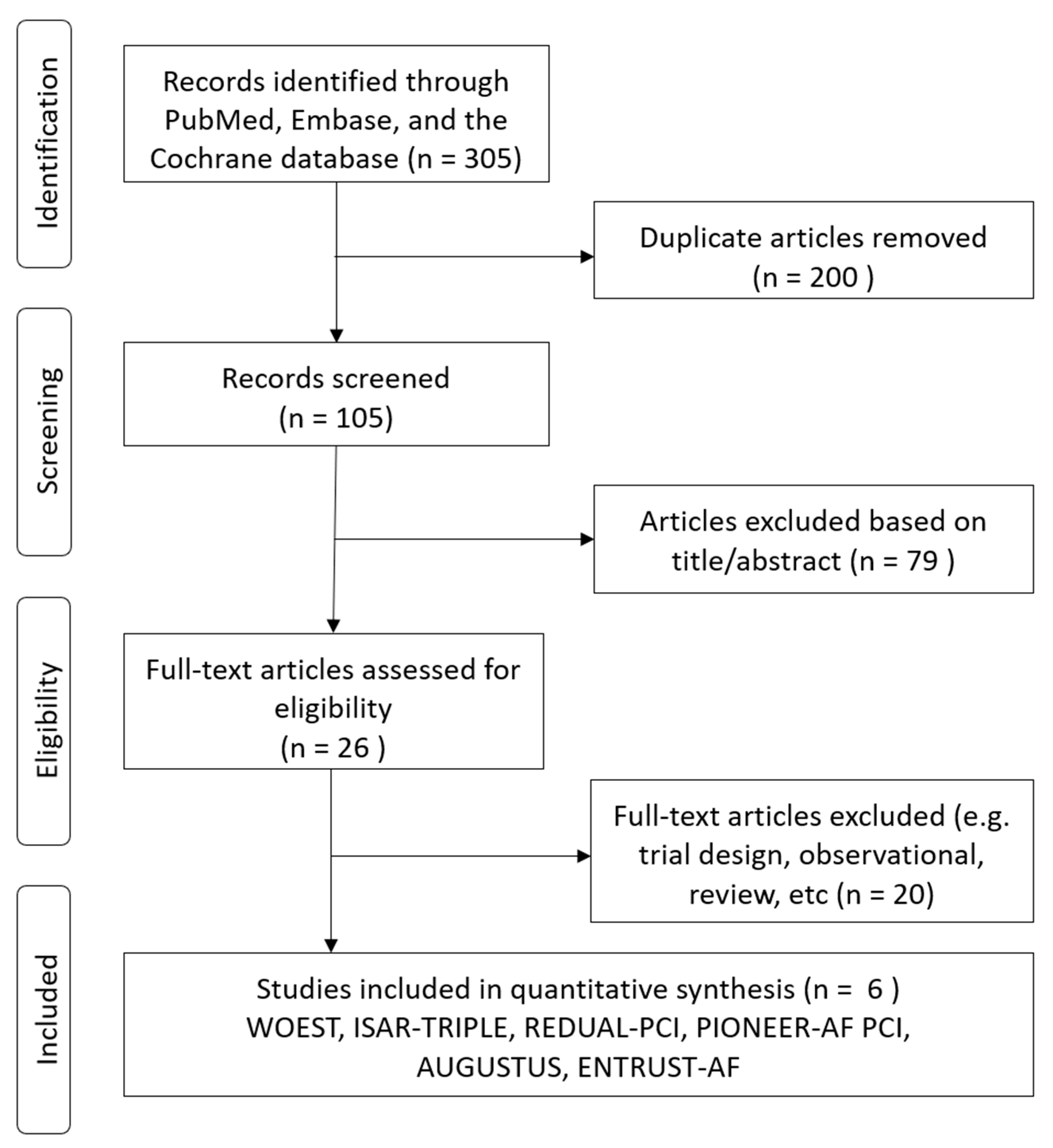
3.1. Enrollment of Studies
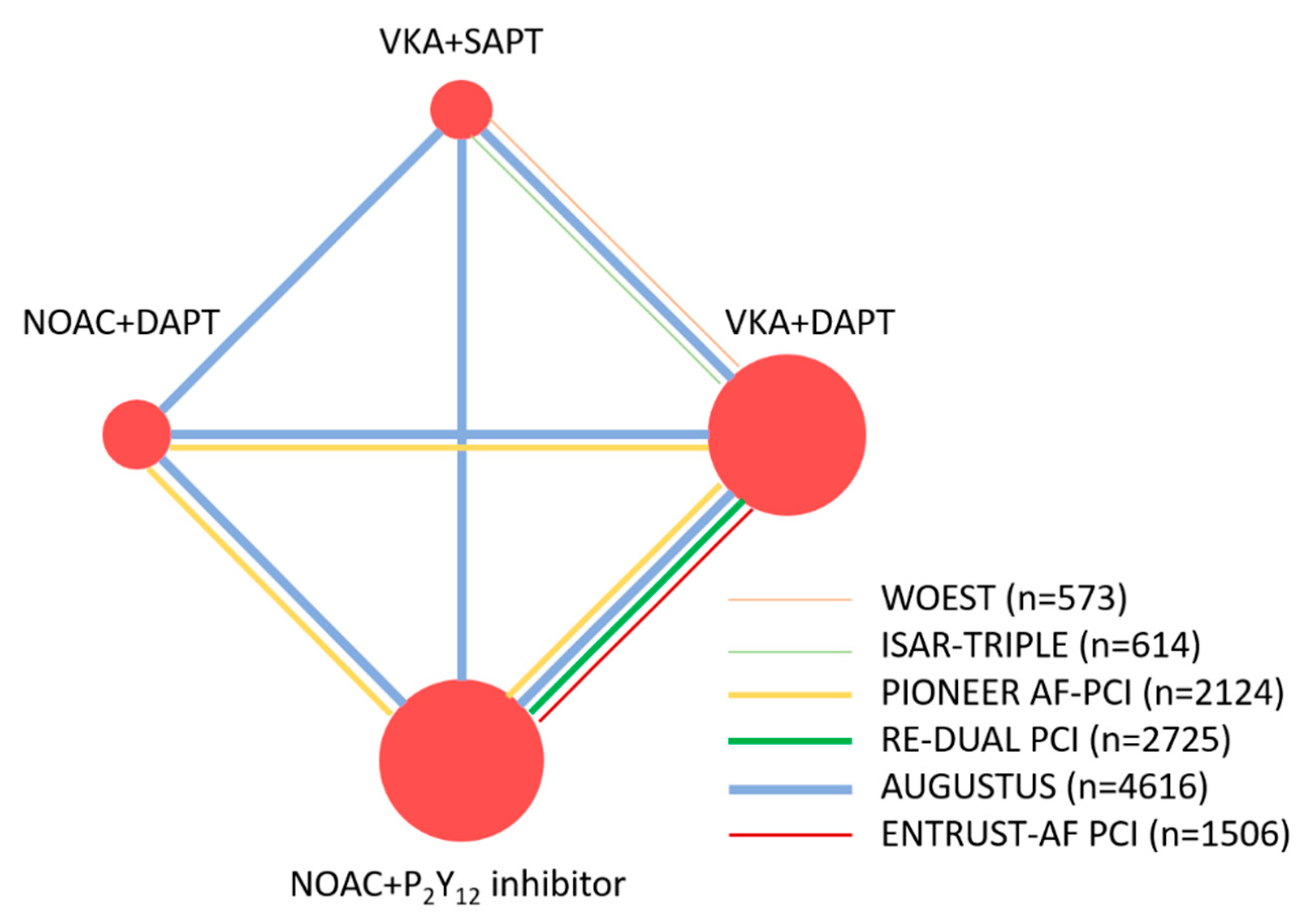
3.2. Structure of the Network Meta-Analysis
3.3. Network Meta-Analysis Safety Outcomes
3.4. Network Meta-Analysis for Efficacy Outcomes
4. Discussion
4.1. Dual Versus Triple Antithrombotic Therapy
4.2. Dual Antithrombotic Therapy with NOAC or VKA and P2Y12 Inhibitors
4.3. Previous and Present Meta-Analyses
4.4. Clinical Implication
5. Limitation
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Kralev, S.; Schneider, K.; Lang, S.; Suselbeck, T.; Borggrefe, M. Incidence and severity of coronary artery disease in patients with atrial fibrillation undergoing first-time coronary angiography. PLoS ONE 2011, 6, e24964. [Google Scholar] [CrossRef] [PubMed]
- January, C.T.; Wann, L.S.; Calkins, H.; Chen, L.Y.; Cigarroa, J.E.; Cleveland, J.C., Jr.; Ellinor, P.T.; Ezekowitz, M.D.; Field, M.E.; Furie, K.L.; et al. 2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J. Am. Coll. Cardiol. 2019, 74, 104–132. [Google Scholar] [CrossRef] [PubMed]
- Steffel, J.; Verhamme, P.; Potpara, T.S.; Albaladejo, P.; Antz, M.; Desteghe, L.; Haeusler, K.G.; Oldgren, J.; Reinecke, H.; Roldan-Schilling, V.; et al. The 2018 European Heart Rhythm Association Practical Guide on the use of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation. Eur. Heart J. 2018, 39, 1330–1393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neumann, F.J.; Sousa-Uva, M. Ten Commandments’ for the 2018 ESC/EACTS Guidelines on Myocardial Revascularization. Eur. Heart J. 2018, 39, 3759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levine, G.N.; Bates, E.R.; Blankenship, J.C.; Bailey, S.R.; Bittl, J.A.; Cercek, B.; Chambers, C.E.; Ellis, S.G.; Guyton, R.A.; Hollenberg, S.M.; et al. 2015 ACC/AHA/SCAI Focused Update on Primary Percutaneous Coronary Intervention for Patients With ST-Elevation Myocardial Infarction: An Update of the 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention and the 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Circulation 2016, 133, 1135–1147. [Google Scholar] [CrossRef] [Green Version]
- Paikin, J.S.; Wright, D.S.; Crowther, M.A.; Mehta, S.R.; Eikelboom, J.W. Triple antithrombotic therapy in patients with atrial fibrillation and coronary artery stents. Circulation 2010, 121, 2067–2070. [Google Scholar] [CrossRef]
- Holmes, D.R., Jr.; Kereiakes, D.J.; Kleiman, N.S.; Moliterno, D.J.; Patti, G.; Grines, C.L. Combining antiplatelet and anticoagulant therapies. J. Am. Coll. Cardiol. 2009, 54, 95–109. [Google Scholar] [CrossRef] [Green Version]
- Fiedler, K.A.; Maeng, M.; Mehilli, J.; Schulz-Schupke, S.; Byrne, R.A.; Sibbing, D.; Hoppmann, P.; Schneider, S.; Fusaro, M.; Ott, I.; et al. Duration of Triple Therapy in Patients Requiring Oral Anticoagulation After Drug-Eluting Stent Implantation: The ISAR-TRIPLE Trial. J. Am. Coll. Cardiol. 2015, 65, 1619–1629. [Google Scholar] [CrossRef] [Green Version]
- Dewilde, W.J.; Oirbans, T.; Verheugt, F.W.; Kelder, J.C.; De Smet, B.J.; Herrman, J.P.; Adriaenssens, T.; Vrolix, M.; Heestermans, A.A.; Vis, M.M.; et al. Use of clopidogrel with or without aspirin in patients taking oral anticoagulant therapy and undergoing percutaneous coronary intervention: An open-label, randomised, controlled trial. Lancet 2013, 381, 1107–1115. [Google Scholar] [CrossRef]
- Gibson, C.M.; Mehran, R.; Bode, C.; Halperin, J.; Verheugt, F.W.; Wildgoose, P.; Birmingham, M.; Ianus, J.; Burton, P.; van Eickels, M.; et al. Prevention of Bleeding in Patients with Atrial Fibrillation Undergoing PCI. N. Engl. J. Med. 2016, 375, 2423–2434. [Google Scholar] [CrossRef] [Green Version]
- Cannon, C.P.; Bhatt, D.L.; Oldgren, J.; Lip, G.Y.H.; Ellis, S.G.; Kimura, T.; Maeng, M.; Merkely, B.; Zeymer, U.; Gropper, S.; et al. Dual Antithrombotic Therapy with Dabigatran after PCI in Atrial Fibrillation. N. Engl. J. Med. 2017, 377, 1513–1524. [Google Scholar] [CrossRef] [PubMed]
- Lopes, R.D.; Heizer, G.; Aronson, R.; Vora, A.N.; Massaro, T.; Mehran, R.; Goodman, S.G.; Windecker, S.; Darius, H.; Li, J.; et al. Antithrombotic Therapy after Acute Coronary Syndrome or PCI in Atrial Fibrillation. N. Engl. J. Med. 2019, 380, 1509–1524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopes, R.D.; Hong, H.; Harskamp, R.E.; Bhatt, D.L.; Mehran, R.; Cannon, C.P.; Granger, C.B.; Verheugt, F.W.A.; Li, J.; Ten Berg, J.M.; et al. Safety and Efficacy of Antithrombotic Strategies in Patients With Atrial Fibrillation Undergoing Percutaneous Coronary Intervention: A Network Meta-analysis of Randomized Controlled Trials. JAMA Cardiol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Golwala, H.B.; Cannon, C.P.; Steg, P.G.; Doros, G.; Qamar, A.; Ellis, S.G.; Oldgren, J.; Ten Berg, J.M.; Kimura, T.; Hohnloser, S.H.; et al. Safety and efficacy of dual vs. triple antithrombotic therapy in patients with atrial fibrillation following percutaneous coronary intervention: A systematic review and meta-analysis of randomized clinical trials. Eur. Heart J. 2018, 39, 1726a–1735a. [Google Scholar] [CrossRef] [PubMed]
- Brunetti, N.D.; Tarantino, N.; De Gennaro, L.; Correale, M.; Santoro, F.; Di Biase, M. Direct oral anticoagulants versus standard triple therapy in atrial fibrillation and PCI: Meta-analysis. Open Heart 2018, 5, e000785. [Google Scholar] [CrossRef]
- Vranckx, P.; Valgimigli, M.; Eckardt, L.; Tijssen, J.; Lewalter, T.; Gargiulo, G.; Batushkin, V.; Campo, G.; Lysak, Z.; Vakaliuk, I.; et al. Edoxaban-based versus vitamin K antagonist-based antithrombotic regimen after successful coronary stenting in patients with atrial fibrillation (ENTRUST-AF PCI): A randomised, open-label, phase 3b trial. Lancet 2019. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA Statement. Open Med. 2009, 3, e123–e130. [Google Scholar]
- Neumann, F.J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef]
- Chen, J.; Wang, L.Y.; Deng, C.; Jiang, X.H.; Chen, T.G. The safety and efficacy of oral anticoagulants with dual versus single antiplatelet therapy in patients after percutaneous coronary intervention: A meta-analysis. Medicine (Baltim.) 2017, 96, e8015. [Google Scholar] [CrossRef]
- Zhu, W.; Guo, L.; Liu, F.; Wan, R.; Shen, Y.; Lip, G.Y.H.; Hong, K. Efficacy and safety of triple versus dual antithrombotic therapy in atrial fibrillation and ischemic heart disease: A systematic review and meta-analysis. Oncotarget 2017, 8, 81154–81166. [Google Scholar] [CrossRef] [Green Version]
- Gong, X.; Tang, S.; Li, J.; Zhang, X.; Tian, X.; Ma, S. Antithrombotic therapy strategies for atrial fibrillation patients undergoing percutaneous coronary intervention: A systematic review and network meta-analysis. PLoS ONE 2017, 12, e0186449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agarwal, N.; Jain, A.; Mahmoud, A.N.; Bishnoi, R.; Golwala, H.; Karimi, A.; Mojadidi, M.K.; Garg, J.; Gupta, T.; Patel, N.K.; et al. Safety and Efficacy of Dual Versus Triple Antithrombotic Therapy in Patients Undergoing Percutaneous Coronary Intervention. Am. J. Med. 2017, 130, 1280–1289. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.J.; Zou, C.; Liu, W.Y.; Yang, G.P. Dual versus single antiplatelet therapy for patients with long-term oral anticoagulation undergoing coronary intervention: A systematic review and meta-analysis. J. Geriatr. Cardiol. 2017, 14, 725–736. [Google Scholar] [CrossRef] [PubMed]
- Cavallari, I.; Patti, G. Meta-Analysis Comparing the Safety and Efficacy of Dual Versus Triple Antithrombotic Therapy in Patients With Atrial Fibrillation Undergoing Percutaneous Coronary Intervention. Am. J. Cardiol. 2018, 121, 718–724. [Google Scholar] [CrossRef]
- Liu, L.; Huang, J.; Zhang, X.; Tang, X. Efficacy and safety of triple therapy versus dual antiplatelet therapy in patients with atrial fibrillation undergoing coronary stenting: A meta-analysis. PLoS ONE 2018, 13, e0199232. [Google Scholar] [CrossRef] [Green Version]
- Bunmark, W.; Jinatongthai, P.; Vathesatogkit, P.; Thakkinstian, A.; Reid, C.M.; Wongcharoen, W.; Chaiyakunapruk, N.; Nathisuwan, S. Antithrombotic Regimens in Patients With Percutaneous Coronary Intervention Whom an Anticoagulant Is Indicated: A Systematic Review and Network Meta-Analysis. Front. Pharmacol. 2018, 9, 1322. [Google Scholar] [CrossRef]
- Mahmoud, A.N.; Shah, N.H.; Elgendy, I.Y.; Agarwal, N.; Elgendy, A.Y.; Mentias, A.; Barakat, A.F.; Mahtta, D.; David Anderson, R.; Bavry, A.A. Safety and efficacy of second-generation drug-eluting stents compared with bare-metal stents: An updated meta-analysis and regression of 9 randomized clinical trials. Clin. Cardiol. 2018, 41, 151–158. [Google Scholar] [CrossRef] [Green Version]
- Committee, C.S. A randomised, blinded, trial of clopidogrel versus aspirin in patients at risk of ischaemic events (CAPRIE). CAPRIE Steering Committee. Lancet 1996, 348, 1329–1339. [Google Scholar] [CrossRef]
- Gargiulo, G.; Goette, A.; Tijssen, J.; Eckardt, L.; Lewalter, T.; Vranckx, P.; Valgimigli, M. Safety and efficacy outcomes of double vs. triple antithrombotic therapy in patients with atrial fibrillation following percutaneous coronary intervention: A systematic review and meta-analysis of non-vitamin K antagonist oral anticoagulant-based randomized clinical trials. Eur. Heart J. 2019, 40, 3757–3767. [Google Scholar] [CrossRef] [Green Version]
- Mehran, R.; Rao, S.V.; Bhatt, D.L.; Gibson, C.M.; Caixeta, A.; Eikelboom, J.; Kaul, S.; Wiviott, S.D.; Menon, V.; Nikolsky, E.; et al. Standardized bleeding definitions for cardiovascular clinical trials: A consensus report from the Bleeding Academic Research Consortium. Circulation 2011, 123, 2736–2747. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Target Population | Number of Included Studies | Timespan of All Studies | Total Number of Patients | Safety Outcome (Major Bleeding) | Efficacy Outcome |
|---|---|---|---|---|---|---|
| Network Meta-Analysis of RCTs | ||||||
| Gong et al., 2017 [21] | Patients with AF undergoing PCI | 7 P, 5 R, 3 RCTs (WOEST, PIONEER -AF PCI, ROCKET AF post-hoc) | 2008 to 2016 | 13,104 | DT vs. TT Risk Ratio = 0.97 (95% CI: 0.29–3.35) | MACE: DT vs. TT Risk Ratio = 0.68 (95% CI: 0.43–0.98) |
| Bunmark et al., 2018 [26] | Patients with OAC undergoing PCI | 4 RCTs (WOEST, PIONEER-AF PCI, REDUAL-PCI), 12 P, 14 R | 2007 to 2017 | 22,179 | DT vs. TT RR = 0.68 (95% CI: 0.49–0.94) | All-cause death: DT vs. TT RR = 0.40 (95% CI: 0.17–0.93) |
| Lopes et al., 2019 [13] | Patients with AF undergoing PCI | 5 RCTs (WOEST, ISAR-TRIPLE, PIONEER AF-PCI, RE-DUAL PCI, AGUSTUS) | 2013 to 2018 | 10,026 | DT vs. TT OR = 0.49 (95% CI: 0.30–0.82) | MACE: DT vs. TT OR = 1.02 (95% CI: 0.71–1.47) All-cause death: DT vs. TT OR = 1.02 (95% CI: 0.59–1.74) Stroke: DT vs. TT OR = 0.77 (95% CI: 0.34–1.67) |
| Present study, 2020 | Patients with AF undergoing PCI | 6 RCTs (WOEST, ISAR-TRIPLE, PIONEER AF-PCI, RE-DUAL PCI, AGUSTUS, ENTRUST-AF PCI) | 2013 to 2019 | 11,532 | DT vs. TT HR = 0.53 (95% CI: 0.35–078) | MACE: DT vs. TT OR = 1.02 (95% CI: 0.72–1.42) All-cause death: DT vs. TT OR = 1.08 (95% CI: 0.72–1.60) Stroke: DT vs. TT: 0.80 (95% CI: 0.41–1.48) |
| Systemic Review and Meta-Analysis | ||||||
| Chen et al., 2017 [19] | Patients with OAC undergoing PCI | 2 RCTs (WOEST, ISAR-TRIPLE), 5 P, 5 R | 2007 to 2016 | 30,823 | TT vs. DT RR = 0.86 (95% CI: 0.74–0.99) | MACE: TT vs. DT RR = 0.82 (95% CI: 0.58–1.17) All-cause death: TT vs. DT RR = 0.90 (95% CI: 0.54–1.51) Stroke: TT vs. DT RR = 1.08 (95% CI: 0.56–2.07) |
| Zhu et al., 2017 [20] | Patients with AF and ischemic heart disease | 8 P, 9 R | 2010 to 2017 | 38,099 | TT vs. DT RR = 1.65 (95% CI: 1.23–2.21) | MACE: TT vs. DT RR = 1.14 (95% CI: 0.75–1.73, p = 0.55) All-cause death: TT vs. DT RR = 1.21 (95% CI: 0.78–1.88) TE: TT vs. DT RR: 1.55 (95% CI: 0.89–2.72; p = 0.12) |
| Agarwal et al., 2017 [22] | Patients with OAC undergoing PCI | 2 RCTs (WOEST, PIONEER-AF PCI), 6 P, 3 R | 2007 to 2016 | 7276 | TT vs. DT RR = 1.54 (95% CI: 1.20 to 1.98) | MACE: TT vs. DT RR = 1.03 (95% CI: 0.90 to 1.32) All-cause death: TT vs. DR RR = 0.98 (95% CI: 0.68 to 1.43) TE: TT vs. DR RR = 1.02 (95% CI: 0.49 to 2.10) |
| Yu et al., 2017 [23] | Patients with OAC undergoing PCI | 3 RCTs (WOEST, ISAR-TRIPLE, PIONEER AF-PCI), 5 P, 6 R | 2000 to 2016 | 32,825 | TT vs. DT OR = 1.56 (95% CI: 0.98–2.49); | MACE: TT vs. DT OR = 0.97 (95% CI: 0.68 to 1.387) All-cause death: TT vs. DT OR = 2.11 (95% CI: 1.10–4.06) SE: TT vs. DT OR = 0.43 (95% CI: 0.30–0.62) |
| Cavallari et al., 2018 [24] | Patients with AF undergoing PCI | 4 RCTs (WOEST, ISAR-TRIPLE, PIONEER AF-PCI, RE-DUAL PCI) | 2013 to 2017 | 6036 | DT vs. TT OR = 0.55 (95% CI: 0.39 to 0.78) | All-cause death: DT vs. TT OR = 0.81 (95% CI: 0.50 to 1.29) Stroke: DT vs. TT OR = 0.95 (95% CI: 0.58 to 1.57) |
| Golwala et al., 2018 [14] | Patients with AF undergoing PCI | 4 RCTs (WOEST, ISAR-TRIPLE, PIONEER AF-PCI, RE-DUAL PCI) | 2013 to 2017 | 5317 | DT vs. TT HR = 0.53 95% CI: 0.36–0.85) | MACE: DT vs. TT HR = 0.85 (95% CI: 0.48–1.29) All-cause death: DT vs TT HR = 0.85 (95% CI: 0.46–1.37) Stroke: DT vs. TT HR = 0.94 (95% CI: 0.45–1.84) |
| Brunetti et al., 2018 [15] | Patients with AF undergoing PCI | 2 RCTs (PIONEER AF-PCI, RE-DUAL PC) | 2016 to 2017 | 4849 | DT vs. TT RR = 0.59 (95% CI: 0.47–0.73) | MACE: DT vs. TT RR = 1.03 (95% CI: 0.89–1.19) |
| Liu et al., 2018 [25] | Patients with AF undergoing PCI | 5 P, 9 R | 2010 to 2016 | 11,697 | TT vs. DT OR = 1.55 (95% CI: 1.16–2.09) | MACE: TT vs. DT OR = 0.97 (95% CI: 0.87–1.07) All-cause death: TT vs. DT OR = 0.92 (95% CI: 0.83–1.03) Stroke: TT vs. DT OR = 0.74 (95% CI: 0.59–0.93) |
| Gargiulo et al., 2019 [29] | Patients with AF undergoing PCI | 4 RCTs (PIONEER AF-PCI, RE-DUAL PCI, AUGUSTUS, ENTRUST-AF PCI) | 2016 to 2019 | 10,234 | DT vs. TT RR = 0,66 (95% CI: 0.56-0.78) | MACE: DT vs. TT OR = 1.08 (95% CI: 0.95–1.23) All-cause death: DT vs. TT OR = 1.10 (95% CI: 0.91–1.34) Stroke: DT vs. TT OR = 1.00 (95% CI: 0.69–1.45) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chua, S.-K.; Chen, L.-C.; Shyu, K.-G.; Cheng, J.-J.; Hung, H.-F.; Chiu, C.-Z.; Lin, C.-M. Antithrombotic Strategies in Patients with Atrial Fibrillation Following Percutaneous Coronary Intervention: A Systemic Review and Network Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2020, 9, 1062. https://doi.org/10.3390/jcm9041062
Chua S-K, Chen L-C, Shyu K-G, Cheng J-J, Hung H-F, Chiu C-Z, Lin C-M. Antithrombotic Strategies in Patients with Atrial Fibrillation Following Percutaneous Coronary Intervention: A Systemic Review and Network Meta-Analysis of Randomized Controlled Trials. Journal of Clinical Medicine. 2020; 9(4):1062. https://doi.org/10.3390/jcm9041062
Chicago/Turabian StyleChua, Su-Kiat, Lung-Ching Chen, Kou-Gi Shyu, Jun-Jack Cheng, Huei-Fong Hung, Chiung-Zuan Chiu, and Chiu-Mei Lin. 2020. "Antithrombotic Strategies in Patients with Atrial Fibrillation Following Percutaneous Coronary Intervention: A Systemic Review and Network Meta-Analysis of Randomized Controlled Trials" Journal of Clinical Medicine 9, no. 4: 1062. https://doi.org/10.3390/jcm9041062