1. Introduction
Prediabetes is an intermediate state in which blood glucose levels are higher than normal but not yet high enough to lead to a diagnosis of type 2 diabetes. Prediabetes has no specific signs or symptoms, but individuals with prediabetes have a higher risk of developing diabetes and microvascular complications [
1]. The American Diabetes Association defined prediabetes based on any of three distinct entities: impaired fasting glucose (IFG), defined as fasting plasma glucose (FPG) levels of 100–125 mg/dL; impaired glucose tolerance (IGT), defined as 2 h plasma glucose levels of 140–199 mg/dL after an oral glucose tolerance test (OGTT); or glycosylated hemoglobin (HbA1c) level of 5.7%–6.4% [
2]. FPG is usually related to basal insulin secretion by the pancreatic β cells and glucose production in the liver, while glucose levels during the OGTT depend on postprandial insulin secretion and subsequent glucose uptake in target cells which are primarily skeletal muscle cells [
3]. Therefore, the diagnostic value of IFG and IGT reflect different pathophysiologies of glucose metabolism, thus implicating different risk factors for developing type 2 diabetes.
However, most epidemiologic surveys and population screenings for DM or prediabetes are based on FPG. In Korea, FPG and HbA1c are recommended as a screening guideline for prediabetes, according to the Korean Centers for Disease Control and Prevention [
4]. Although FPG is relatively simple and inexpensive compared with OGTT, IGT remains undetected in many subjects when only FPG is measured, which may eventually lead to underestimates in the prevalence of prediabetes [
5]. In addition, the clinical characteristics of prediabetes cannot be determined by FPG alone.
Prediabetes can be prevented, and the risk of diabetes can be decreased if lifestyle intervention or pharmacological treatment is implemented before the development of diabetes [
6,
7,
8,
9]. Conversely, undiagnosed, and thus untreated, prediabetes causes substantial public health problems. Nevertheless, little attention has been paid to early detection, which is critical to reduce the long-term healthcare burden. Moreover, the prevalence of prediabetes varies in Korea, China and Japan, countries which share a similar lifestyle [
10,
11,
12], suggesting the existence of ethnic variations for the epidemiological and pathophysiological characteristics of prediabetes. In this study, we compared the prevalence of isolated IFG (I-IFG), isolated IGT (I-IGT) and combined IFG and IGT (C-IFG/IGT) in subjects with prediabetes identified according to plasma glucose levels after an OGTT and HbA1c levels. We also examined the anthropometric and biochemical parameters of the subjects, in order to explore whether the parameters are associated with FPG, 2 h post-challenge plasma glucose (2h-PPG) during OGTT and hemoglobin A1c (HbA1c).
2. Subjects and Methods
2.1. Data Collection
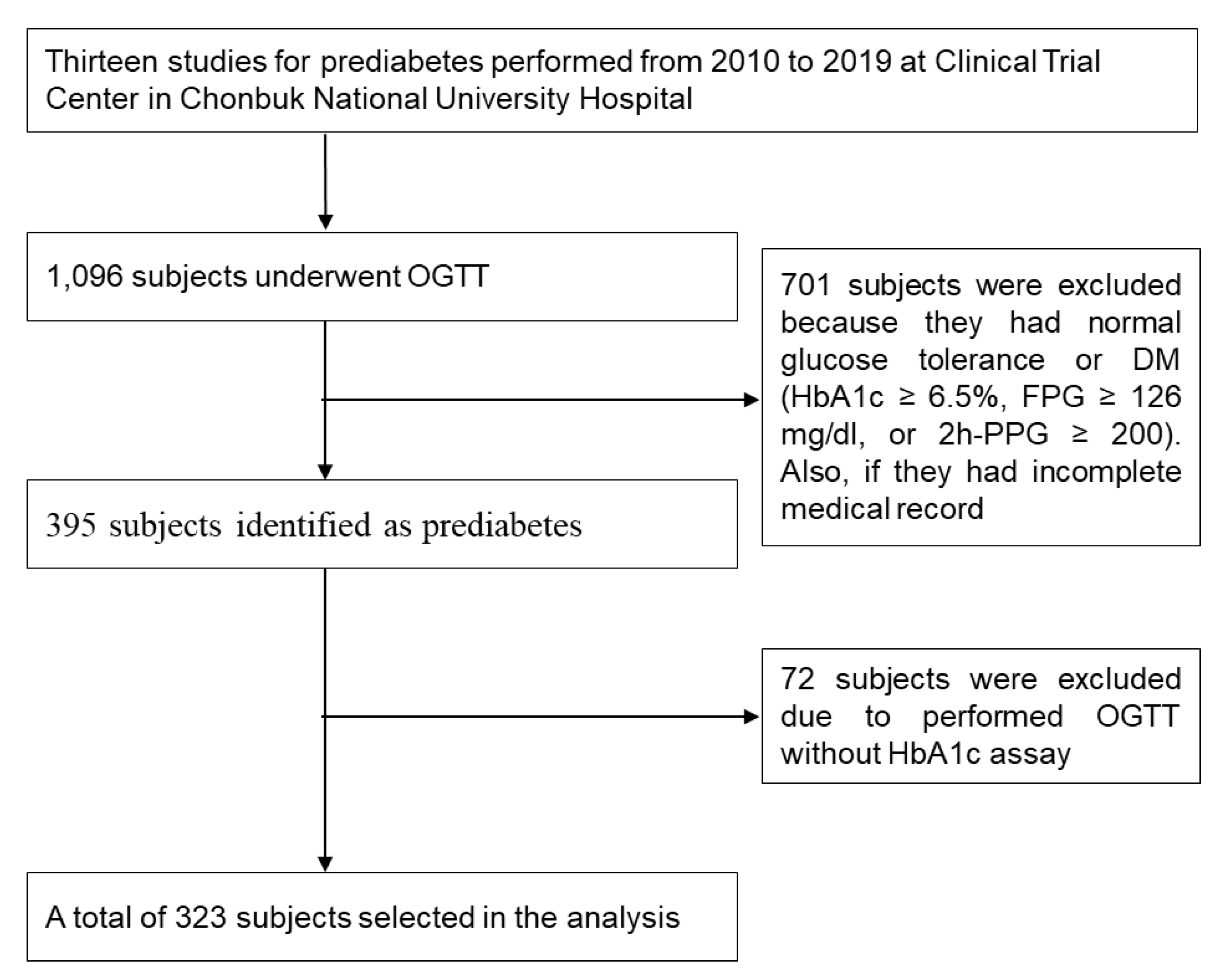
We retrospectively reviewed the medical records of participants who had undergone an OGTT for evaluation of prediabetes between 2010 and 2019, at the Clinical Trial Center in Chonbuk National University Hospital. A total of 13 studies for prediabetes were conducted at the Clinical Trial Center in Chonbuk National University Hospital. The selection of the participants for this analysis is shown in
Figure 1. All study examinations were performed according to standard operating procedures by specifically trained and certified medical technical assistants. Data selection criteria were the following: (1) prediabetes according to the OGTT and (2) absence of DM defined as HbA1c ≥ 6.5%, FPG ≥ 126 mg/dL or 2h-PPG ≥ 200 mg/dL. Exclusion criteria were the following: (1) normal glucose tolerance or HbA1c < 5.7% and (2) OGTT without HbA1c assay.
The subjects in the 13 studies had the following features in common: (1) undiagnosed DM or prediabetes, (2) no history of cardiovascular diseases, (3) not taking glucose-lowering agent or insulin therapy, (4) no lipid metabolism disorders, (5) no acute or chronic inflammatory disease, (6) no abnormal hepatic liver function or renal disease (acute/chronic renal failure or nephrotic syndrome) and (7) not currently pregnant or breastfeeding. All subjects gave written informed consent for laboratory analyses, clinical examinations and the use of data records for research purposes.
The information obtained on the demographic and clinical variables were the following: age, sex, height, weight, waist and hip circumference, current smoker, current drinker, alcohol consumption, systolic blood pressure (SBP), diastolic blood pressure (DBP) and pulse. Body mass index (BMI) was defined as weight (kg) divided by height (m2). Data from the subjects’ biochemical variables that were collected included plasma glucose (0, 30, 60, 90 and 120 min) levels, HbA1c, fasting insulin (FI), C-peptide, total cholesterol, triglyceride (TG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), apolipoprotein A1 (ApoA1), apolipoprotein B (ApoB), high-sensitivity C-reactive protein (hs-CRP), gamma glutamyl transpeptidase (γ-GT), aspartate transaminase (AST), alanine transaminase (ALT) and total bilirubin. The study protocol was approved by the Institutional Review Board of Chonbuk National University (2019-12-003).
2.2. Definitions
Prediabetes was defined by the ADA criteria on the basis of the glucose level in the 75 g OGTT or HbA1c value [
2]. Subjects with prediabetes were divided into four subtypes: (1) NGT with HbA1c 5.7%–6.4%; (2) I-IFG; (3) I-IGT; and (4) C-IFG/IGT. Individuals with a BMI less than 23.0 were classified as not overweight/obese. Those with a BMI greater than or equal to 23.0 but less than 25.0 were classified as overweight, and those with a BMI greater than or equal to 25.0 were classified as obese. Waist and hip circumference were recorded to the nearest cm, and waist–hip ratio (WHR) was defined as a ratio of waist circumference (WC) to hip circumference (HC). Central obesity was defined as WHR ≥ 0.90 for men and 0.85 for women. Hypertension was defined as having an SBP of ≥ 130 mmHg or DBP of ≥ 85 mmHg. Subjects who smoked at least 1 cigarette daily for 1 year or more were defined as current smokers.
2.3. Assays and Calculations
A 75 g OGTT was measured by using a standardized protocol. In brief, after an overnight fast, subjects consumed a 75 g glucose solution, and the plasma glucose level was measured at 0, 30, 60, 90 and 120 min. Glucose parameters were evaluated with incremental area under the curve (iAUC), plasma glucose absolute maximum concentrations (C
max) and time of maximum concentrations (T
max). The iAUC (which ignored values below the fasting value) was calculated geometrically, using the trapezoidal rule for plasma glucose for each subject [
13]. Plasma glucose levels were measured by using the glucose oxidase method, and HbA1c levels were detected by using an automated glycosylated hemoglobin analyzer (ADAMS
TM A1c HA-8180, ARKRAY Factory, Shiga, Japan). Insulin resistance (IR) and pancreatic β-cell function were estimated by a homeostasis model assessment, using the following formula [
14]: HOMA-IR = [fasting glucose (mg/dL) × fasting insulin (μU/mL)/405] and HOMA-β (%) = [360 × fasting insulin (μU/mL)]/[fasting glucose (mg/dL) − 63]. Insulin sensitivity was estimated by a quantitative insulin sensitivity check index (QUICKI), using the following formula [
15]: QUICKI = 1/[log(fasting insulin (μU/mL)) + log(fasting glucose (mg/dL))]. Insulin and C-peptide concentration were measured using a Cobas e601 module (Hitachi High-Technologies, Tokyo, Japan). hs-CRP, γ-GT, AST, ALT and total bilirubin concentrations were measured by using an ADVIA
® 2400 chemistry system (Siemens, Bayern, Germany). Lipid parameters (total cholesterol, HDL-C, LDL-C, triglyceride, ApoA1 and ApoB) were measured by using a Hitachi 7600-110
® analyzer (Hitachi High-Technologies, Tokyo, Japan). All of the biochemical variable analyses were performed in a centralized laboratory setup.
2.4. Statistical Analysis
Data were analyzed by using the statistical software SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). One-way analysis of variance (ANOVA) was performed to compare the clinical and biochemical variables of subjects from the four subtypes. Post hoc analysis was performed, using the Bonferroni method. The Chi-square test was used for the comparison of categorical variables. Data were expressed as mean ± standard deviation (SD) or number (percent). Natural logarithmic transformation was applied to variables with no normal distribution. Respective relationships of FPG, 2h-PPG or HbA1c concentration with various markers were subjected to univariate regression. Independent variables significantly associated with FPG, 2h-PPG or HbA1c concentration in univariate analysis (p < 0.05) and potentially confounding parameters were included as independent covariables in multivariate analysis by multiple regression analysis. The relationship of relevant factor to prediabetes subtypes was assessed by binary logistic regression analysis. Odds ratios were estimated, and their confidence interval (CI) was considered to be 95%. Statistical significance was set at p < 0.05.
4. Discussion
In this study, the most common subtype of prediabetes in the southwestern region of Korea was C-IFG/IGT (44.0%) for men and I-IGT (42.1%) for women. I-IGT and C-IFG/IGT accounted for 70.9% of all prediabetes subjects, suggesting that screening with a fasting glucose level, without an OGTT, may underestimate the incidence of prediabetes. The higher distribution of subjects with C-IFG/IGT in this study is not similar to the distributions reported by studies performed in other Asian countries [
12,
16]. For example, I-IFG subtype is higher than other subtypes in Japan [
17], whereas, in China, I-IGT subtype is the highest [
18]. It is not clear whether this discrepancy reflects ethnic differences between studies, or whether this result was due to a small sample size. Given that the incidence of IGT is closely related to an unhealthy diet and physical inactivity [
19], the higher percentage of subjects with C-IFG/IGT and I-IGT seems to be related to the Westernized lifestyle in Korea. Indeed, 78% of the study subjects were classified as either overweight or obese (as measured by BMI), and 68% of the subjects had central obesity (as measured by WHR). The progression rate from C-IFG/IGT to diabetes was reported to be 2–3 times higher than that from I-IFG or I-IGT to diabetes [
20,
21,
22]. Therefore, relatively higher proportions of the isolated and combined forms of IGT in prediabetes subjects may increase their future risk of type 2 diabetes, which is a well-established risk for life-threatening cardio-metabolic diseases. Therefore, prompt intervention is required to delay or prevent its progression to diabetes, especially for subjects with C-IFG/IGT.
There were sex and age differences in the proportions of subjects with prediabetes in the present study. I-IFG was higher than I-IGT in men, while I-IGT was more common in women. This is not surprising, because the fasting glucose level is positively correlated with alcohol consumption, and post-load glucose levels are predominantly affected by muscle mass. To support this notion, Roh et al. [
23] reported that higher-than-average alcohol consumption was associated with a higher odd of IFG in Korean men compared with those with lower alcohol consumption. Smaller skeletal muscle mass with larger visceral fat mass in women seems to be related to the higher glucose levels after glucose loading. The rate of prediabetes increased with age from 10.5% in those aged 20–39 years to 27.3% in those aged 40–49 years. Those aged 50–59 years had the highest rate of prediabetes at 41.5%, and prediabetes decreased in subjects aged above 60 years. Interestingly, the proportions of subjects with C-IFG/IGT was higher than the other subtypes in all age groups, except age above 60 years. Therefore, rates of prediabetes in easily identifiable groups, such as patients in their 50 s, are noticeably higher and suggest that targeted screening and an appropriate healthcare policy might be desirable.
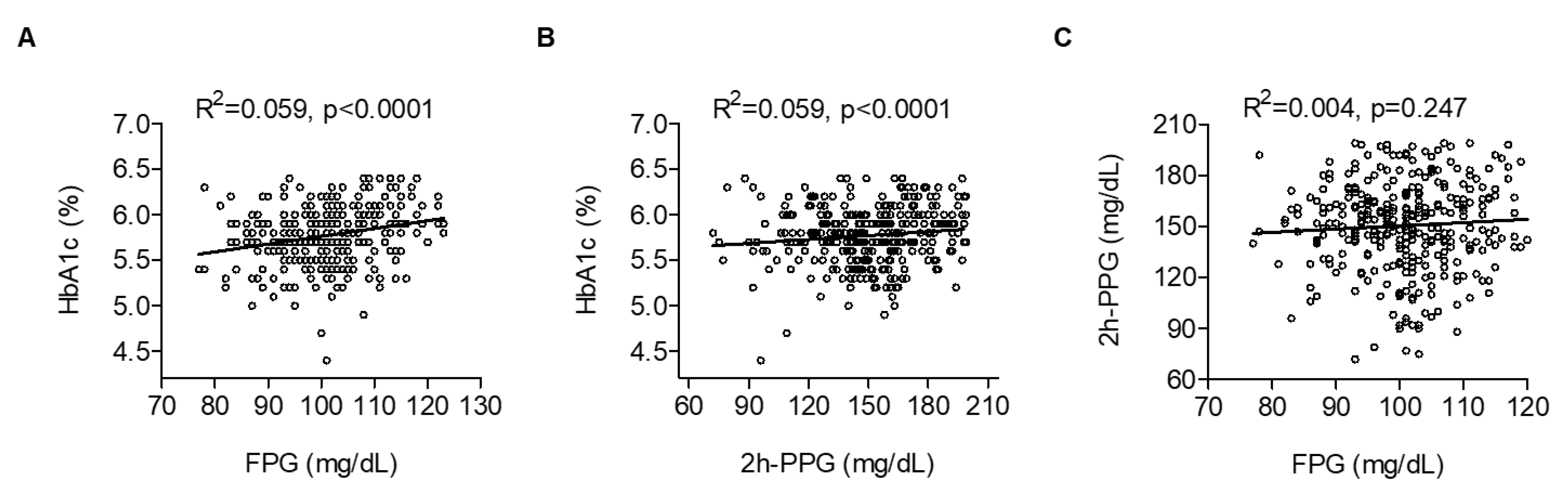
In this study, we investigated the relationship among FPG, 2h-PPG and HbA1c as a function of glucose intolerance in subjects. We found a strong correlation between HbA1c and either FPG or 2h-PPG, but only a small correlation between FPG and 2h-PPG. These results are in accordance with previous studies that demonstrated a moderate-to-strong correlation between HbA1c and FPG, as well as 2h-PPG [
24,
25]. However, in contrast to this study, Van’t Riet and colleagues reported that only 39% of subjects with prediabetes and HbA1c values in the range of 5.7%–6.4% were diagnosed with prediabetes based on the results of a 75 g OGTT [
26]. Possible mechanisms for this discrepancy may be differences in race, genetic trait, sex composition, age and socioeconomic status between subjects in different studies. Considering that HbA1c simply represents an average blood sugar level over the previous three months, it is clear that, when tested alone, HbA1c can misclassify some subjects to either the normal or the diabetes group. The weak correlation of FPG with 2h-PPG observed in this study may imply that fasting and post-load glucose levels reflect different metabolic processes, especially in the prediabetic range of glucose tolerance. More specifically, FPG reflects hepatic insulin resistance with basal insulin secretion, whereas the 2h-PPG level predominantly depends on muscular glucose uptake and postprandial insulin secretion [
3].
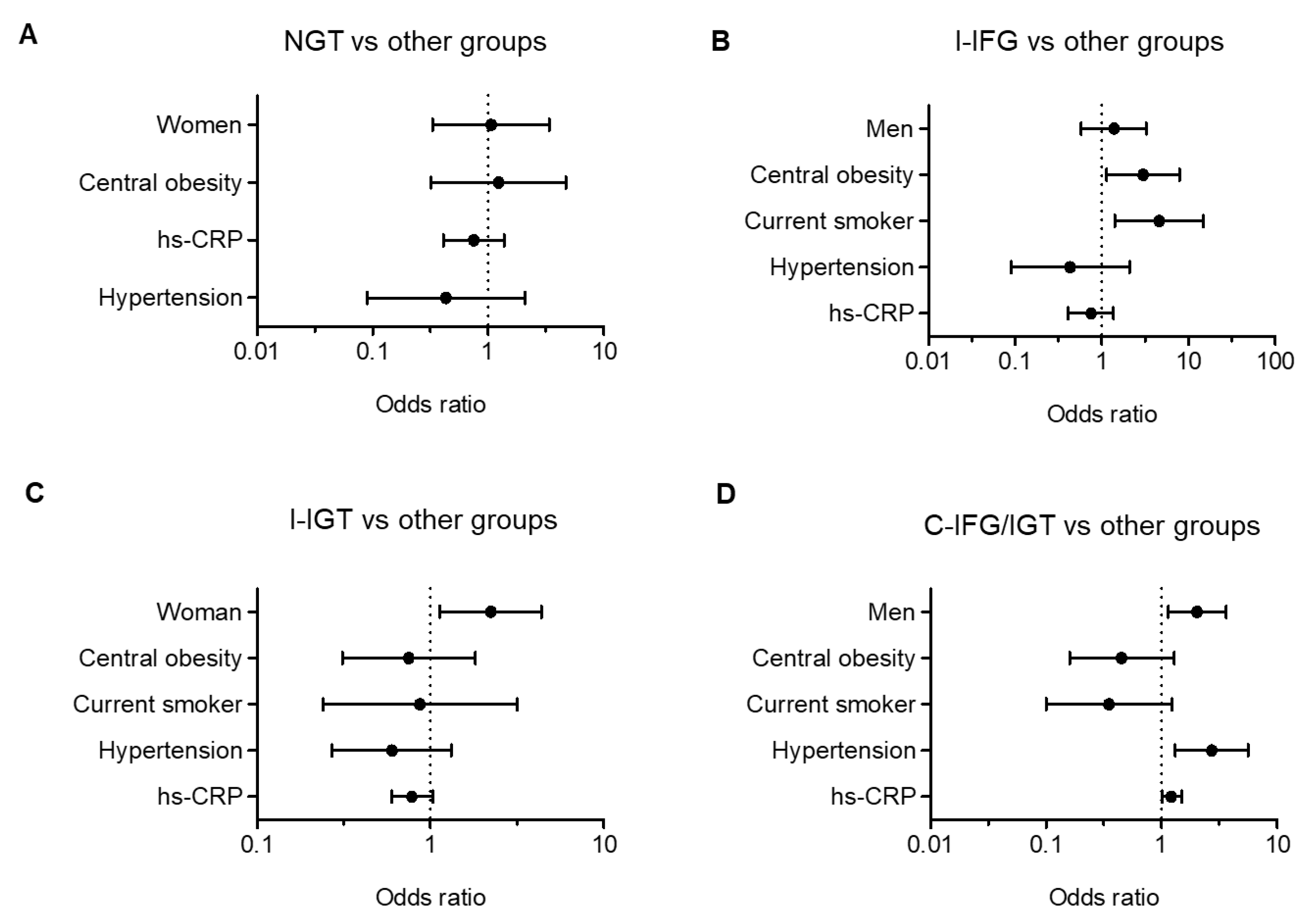
Based on multiple regression analysis after adjusting age and sex, we confirmed that the WHR, a surrogate marker for central obesity, is an independent risk factor for FPG and 2h-PPG levels, but not for the HbA1c level. Although the subjects in the present study had a much lower BMI than Western people, Koreans have a similar rate of diabetes prevalence as residents of Western countries. One possible explanation is that Korean people have less muscle and more visceral fat than Western people. Visceral fat is a main source of inflammatory cytokines and metabolites, which result in hepatic and systemic insulin resistance. Therefore, WHR is a useful marker to predict I-IFG and I-IGT. Additionally, smoking was associated with the odds of having I-IFG. Subjects who were current smokers were 4–5 times more likely to have I-IFG compared with subjects in other groups. These results may be due to the higher proportion of men in the I-IFG groups. Similar to these results, longitudinal studies have reported that cigarette smoking is an independent risk factor for type 2 diabetes [
27,
28].
Another interesting finding of the present study is that subjects in the NGT subtype had normal levels of biochemical and clinical parameters. The results indicated that about 8.4% of study subjects who had elevated HbA1c values exhibited normal glucose levels during OGTT. In 2010, the American Diabetes Association (ADA) proposed the use of HbA1c for the diagnosis of prediabetes and recommended cut-off values of between 5.7% and 6.4% [
2]. However, several studies published since the 2010 ADA statement have questioned the value of HbA1c for the diagnosis of prediabetes [
24,
25,
26]. HbA1c has several advantages for the assessment of glucose metabolism that may favor its use for diagnostic purposes, but there are patient-dependent and independent factors, some of which are not well defined [
29]. Therefore, HbA1c alone without OGTT may miss the diagnoses of prediabetes and diabetes.
There are several limitations in this study. First, it may have a potential selection bias. Selection bias occurs when recruiters selectively enroll subjects into a trial based on protocol. However, the data analyzed in this study are based on simple randomized clinical trials. Given that simple randomization is the simplest and most effective method to prevent selection bias [
30], we believe that, even if there is a selection bias, it may be minimal. Second, the sample size used in this study was relatively small compared to other studies conducted elsewhere, and the smaller size may cause biased results. Therefore, caution should be exercised in interpreting the results as an indication of the presence of prediabetes. Despite these limitations, this is the first study to identify characteristics and associated risk factors of prediabetes subtypes in Korean subjects with prediabetes. We believe that the findings described in this study extend the present knowledge of the epidemiological and pathophysiological characteristics of prediabetes subtypes in the Korean population.







{kind=link}
{kind=link}
{kind=link}