1. Introduction
Pregnancy induces hemodynamic changes in response to the increased metabolic demands of the mother and fetus [
1]. These changes lead to an overall hyperdynamic and hypervolemic cardiovascular state that begins in the first two trimesters and reaches a maximum in the third trimester, during labor and in the postpartum period. The maternal aorta, in particular, is subject to major wall stress and intimal shear forces [
2,
3]. In addition, pregnancy-induced alterations in estrogen and progesterone levels lead to significant histological changes in the microstructure of the aortic media that cause an increased susceptibility to hemodynamic stress [
4]. The aorta reaches a maximal size during the third trimester in pregnant women and stays enlarged by an average of 1 mm at 6 weeks after delivery [
5]. In women younger than 40 years, 50% of dissecting aneurysms occur during pregnancy or in the immediate postpartum period [
6]. Therefore, many authors consider pregnancy as an important risk factor for adverse aortic events [
7,
8].
However, most healthy women seem to tolerate physiological changes during gestation without any difficulty [
9], whereas women with preexisting aortic disease may actually experience aortic complications [
10]. Aortopathies in women of childbearing age have been identified as a significant cause of maternal morbidity and mortality during pregnancy [
11]. Due to earlier diagnosis and major advances in medical and surgical therapy, the number of women with genetic aortopathies who are able to undergo pregnancy is continuously rising [
12]. Among all hereditary aortopathies, Marfan syndrome constitutes the most frequent cause of adverse aortic outcome during pregnancy [
11,
13,
14]. Some authors have reported an increased risk of aortic events even during long-term follow-up after pregnancy [
15,
16], as well as of obstetric complications in pregnant women with Marfan syndrome [
17,
18]. However, most reports are casuistic, and data from larger cohorts remain scarce.
The lack of conclusive data is even more striking in aortopathy related to bicuspid aortic valve disease. With a prevalence between 0.5% and 1.39% in the general population, the bicuspid aortic valve is the most common congenital cardiovascular malformation [
19], yet the risk of pregnancy-related complications in women with bicuspid aortic valve disease has not been sufficiently elucidated [
20]. Nonetheless, some pathogenetic similarities between aortopathy in Marfan syndrome and in bicuspid aortic valve disease have led authors to suggest that there is also some increased aortic risk in pregnancy of women with bicuspid aortic valve disease [
21,
22].
However, studies comparing the outcome of pregnancy in Marfan syndrome and in bicuspid aortic valve disease are currently missing. Hence, this retrospective longitudinal, observational study aimed to explore the frequency of pregnancy-associated aortic and obstetric complications among women with Marfan syndrome and with bicuspid aortic valve disease. We provide the first analysis with a special focus on the comparison of immediate and long-term aortic outcomes of pregnancy in women with Marfan syndrome and with bicuspid aortic valve disease.
4. Discussion
Our observational study compared the immediate and long-term outcome of pregnancy between women with Marfan syndrome and with bicuspid aortic valve disease. Obstetric outcome in women with Marfan syndrome was comparable to women with bicuspid aortic valve disease. Pregnancy exhibited an increased immediate aortic risk in women with Marfan syndrome, but not in women with bicuspid aortic valve disease. On long-term follow-up, ever-pregnant women with Marfan syndrome were more likely to experience an aortic dissection or to undergo proximal aortic surgery at a younger age than those with bicuspid aortic valve disease. However, pregnancy did not relate to an increased risk of aortic dissection or aortic surgery in the long term, both in Marfan syndrome and in bicuspid aortic valve disease. In Marfan syndrome, pregnancy did not lead to an increased growth of the aorta in the long term.
Pregnancies were less frequent in Marfan syndrome than in bicuspid aortic valve disease. In fact, 29% of never-pregnant women with Marfan syndrome decided to remain childless due to disease-associated fears or a negative advice from their cardiologists. In line with previous findings [
15,
18], in our study never-pregnant women were initially diagnosed of having Marfan syndrome at a significantly younger age than ever-pregnant women. This may indicate that definitive knowledge of having Marfan syndrome may profoundly affect a woman’s family planning, as was also suggested previously [
34].
Aortic root diameters and Z-scores at baseline were comparable between ever-pregnant women with Marfan syndrome and with bicuspid aortic valve disease, and also between ever-pregnant and never-pregnant females in both diagnosis groups, respectively. Several studies corroborated the fact that there is no association between previous pregnancy and the size of the proximal aorta in women with Marfan syndrome [
15,
35,
36] or with bicuspid aortic valve disease [
22]. Diameters of the ascending segment of the aorta were larger in ever-pregnant women with bicuspid aortic valve disease than with Marfan syndrome, whereas more distal segments of the aorta were more dilated in ever-pregnant women with Marfan syndrome than with bicuspid aortic valve disease. Previous investigations confirmed that the anatomic site of major aortic pathology was distinct in both entities and showed that the maximal aortic dilatation occurred at the ascending aorta in individuals with bicuspid aortic valve disease [
37,
38]. In accordance with the literature, we found coarctation of the aorta only with bicuspid aortic valve disease but not with Marfan syndrome [
39], and identified mitral valve prolapse only with Marfan syndrome but not with bicuspid aortic valve disease [
40].
Delivery-related complications were somewhat more frequent in Marfan syndrome (37%) than in bicuspid aortic valve disease (21%), although the difference was not significant. Other studies on pregnancy in Marfan syndrome corroborated rates of obstetric complications, which were comparable to our findings [
18,
36]. Study data on the obstetric outcome of women are available for Marfan syndrome but not for bicuspid aortic valve disease.
Two women with Marfan syndrome experienced aortic dissection during a total of 62 completed pregnancies, accounting for a rate of 3% in our study. A literature review that comprised 12 studies (39 aortic dissections among 1271 pregnancies in 832 women with Marfan syndrome) yielded a similar composite risk rate of approximately 3.1% [
41]. Conversely, our study identified no aortic dissection during a total of 36 completed pregnancies in 23 ever-pregnant women with bicuspid aortic valve disease. In line with current European guidelines, our findings suggest that pregnancy in bicuspid aortic valve disease carries a low immediate risk for the maternal aorta [
1].
In the long-term follow-up, our study demonstrated a higher risk of aortic dissection in ever-pregnant with Marfan syndrome than in women with a congenital bicuspid aortic valve, who remained free of aortic dissection events. This finding reflects the higher long-term aortic risk exhibited by Marfan aortopathy than by aortopathy related to bicuspid aortic valve disease [
14,
42]. In Marfan syndrome, we observed a similar proportion of dissecting aneurysms in ever-pregnant (21%) and never-pregnant women (18%). However, findings on pregnancy-related long-term risk of aortic dissection varied across previous studies—although some studies did not find an association of aortic dissection with previous pregnancy in Marfan syndrome [
43], in some other investigations ever-pregnant women with Marfan syndrome were more likely to have experienced an aortic dissection than never-pregnant women [
16,
35]. Hypertension is a well-known risk factor of aortic dissection [
44] and was also identified as an independent predictor of aortic dissection among Marfan patients in our study. Interestingly, the use of ACEi/ARB medication was associated with aortic dissection in the long term. However, systolic blood pressure was similar in women with Marfan syndrome irrespective of ACEi/ARB medication. An insufficient blood-lowering effect and/or reduced drug compliance may thus be a possible explanation for our somewhat unexpected finding. Our finding may also reflect the more common use of ACEi/ARB medication among Marfan patients with high-risk aortic pathology.
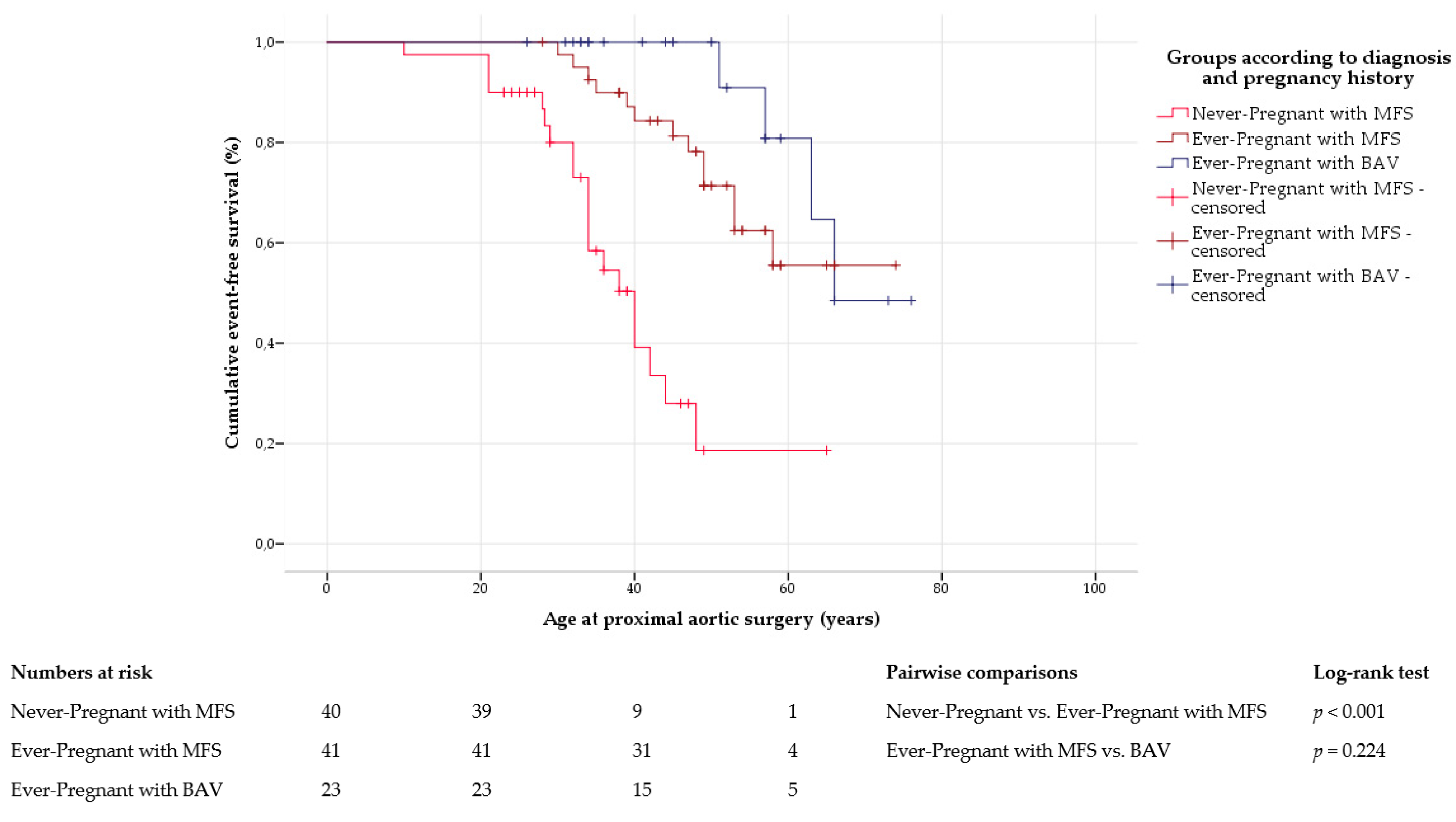
The frequency of proximal aortic surgery was comparable in ever-pregnant women with Marfan syndrome and with bicuspid aortic valve disease. However, ever-pregnant women with Marfan syndrome underwent surgery of the proximal aorta at a significantly younger age. Irrespective of pregnancy history, previous studies confirmed that aortic surgery was necessary at an earlier age in Marfan syndrome than in bicuspid aortic valve disease [
42]. In our study, proximal artic surgery was performed with similar frequency in ever-pregnant and never-pregnant women with Marfan syndrome. Although some studies suggested that pregnancy may increase the long-term risk of proximal aortic surgery in women with Marfan syndrome [
16,
35], in our study, never-pregnant women with Marfan syndrome were younger when surgery was performed. Our findings show that women with a more severe involvement of the aorta and the consecutive need for proximal aortic surgery at a young age were likely to decide against pregnancy due to the associated risks. In Marfan syndrome, growth at all aortic levels was comparable between ever-pregnant and never-pregnant women. Previous studies also detected similar long-term growth of the aortic root in both Marfan subgroups [
15,
36]. However, comparable imaging data on more distal aortic segments are missing in the current literature.
As we performed a retrospective study in a survival-only cohort, no information on fatal cardiovascular complications were available. Given the retrospective design of our study, missing or incomplete data were inevitable. The sample size of our study was limited, and statistical analyses therefore have to be considered with caution. The retrospective nature of our study also accounted for the lack of data on peripartum aortic diameters.
Large multicenter studies, ideally of prospective design, may be necessary to further elucidate and compare the immediate and long-term impact of pregnancy on the aortic outcome in women with Marfan syndrome and with bicuspid aortic valve disease.

 ,
, 



{kind=link}
{kind=link}
{kind=link}
{kind=link}