Safety and Efficacy of Embolic Protection Devices in Saphenous Vein Graft Interventions: A Propensity Score Analysis—Multicenter SVG PCI PROTECTA Study

 , , , , add
Show full author list
, , , , add
Show full author list
Abstract
:1. Introduction
2. Methods
2.1. End-Points
2.2. Statistical Analysis
3. Results
3.1. In-Hospital and Discharge Medications
3.2. Interventional Treatment and Reperfusion Strategy
3.3. 1-Year and 30-Days Outcomes in the Allcommer Population
3.4. 1-Year Outcomes of the MI Group
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Alexander, J.H.; Hafley, G.; Harrington, R.A.; Peterson, E.D.; Ferguson, T.B., Jr.; Lorenz, T.J.; Goyal, A.; Gibson, M.; Mack, M.J.; Gennevois, D.; et al. Efficacy and safety of edifoligide, an E2F transcription factor decoy, for prevention of vein graft failure following coronary artery bypass graft surgery: PREVENT IV: A randomized controlled trial. JAMA 2005, 294, 2446–2454. [Google Scholar] [PubMed] [Green Version]
- Tatoulis, J.; Buxton, B.F.; Fuller, J.A. The right internal thoracic artery: The forgotten conduit—5,766 patients and 991 angiograms. Ann. Thorac. Surg. 2011, 92, 9–15, discussion 15–17. [Google Scholar] [CrossRef] [PubMed]
- Kubiak, G.M.; Pociask, E.; Wanha, W.; Dobrolinska, M.; Gasior, P.; Smolka, G.; Ochala, A.; Gasior, Z.; Wojakowski, W.; Roleder, T. Saphenous graft atherosclerosis as assessed by optical coherence tomography data for stenotic and non-stenotic lesions from the OCTOPUS registry. Postepy W Kardiol. Interwencyjnej = Adv. Interv. Cardiol. 2018, 14, 157–166. [Google Scholar] [CrossRef] [PubMed]
- Motwani, J.G.; Topol, E.J. Aortocoronary saphenous vein graft disease: Pathogenesis, predisposition, and prevention. Circulation 1998, 97, 916–931. [Google Scholar] [CrossRef] [Green Version]
- Bryan, A.J.; Angelini, G.D. The biology of saphenous vein graft occlusion: Etiology and strategies for prevention. Curr. Opin. Cardiol. 1994, 9, 641–649. [Google Scholar] [CrossRef]
- Januszek, R.A.; Dziewierz, A.; Siudak, Z.; Rakowski, T.; Dudek, D.; Bartus, S. Predictors of periprocedural complications in patients undergoing percutaneous coronary interventions within coronary bypass grafts. Cardiol. J. 2018. [Google Scholar] [CrossRef] [Green Version]
- Mehta, S.K.; Frutkin, A.D.; Milford-Beland, S.; Klein, L.W.; Shaw, R.E.; Weintraub, W.S.; Krone, R.J.; Anderson, H.V.; Kutcher, M.A.; Marso, S.P.; et al. Utilization of distal embolic protection in saphenous vein graft interventions (an analysis of 19,546 patients in the American College of Cardiology-National Cardiovascular Data Registry). Am. J. Cardiol. 2007, 100, 1114–1118. [Google Scholar] [CrossRef]
- Desperak, P.; Hawranek, M.; Gasior, P.; Desperak, A.; Lekston, A.; Gasior, M. Long-term outcomes of patients with multivessel coronary artery disease presenting non-ST-segment elevation acute coronary syndromes. Cardiol. J. 2019, 26, 157–168. [Google Scholar] [CrossRef] [Green Version]
- Kubica, J.; Adamski, P.; Paciorek, P.; Ladny, J.R.; Kalarus, Z.; Banasiak, W.; Kochman, W.; Goracy, J.; Wozakowska-Kaplon, B.; Navarese, E.P.; et al. Treatment of patients with acute coronary syndrome: Recommendations for medical emergency teams: Focus on antiplatelet therapies. Updated experts’ standpoint. Cardiol. J. 2018, 25, 291–300. [Google Scholar] [CrossRef] [Green Version]
- Paul, T.K.; Bhatheja, S.; Panchal, H.B.; Zheng, S.; Banerjee, S.; Rao, S.V.; Guzman, L.; Beohar, N.; Zhao, D.; Mehran, R.; et al. Outcomes of Saphenous Vein Graft Intervention with and Without Embolic Protection Device: A Comprehensive Review and Meta-Analysis. Circ. Cardiovasc. Interv. 2017, 10. [Google Scholar] [CrossRef]
- Sadr-Ameli, M.; Mousavi, H.; Heidarali, M.; Maadani, M.; Ghelich, Y.; Ghadrdoost, B. Early and midterm major adverse cardiac events in patient with saphenous vein graft using direct stenting or embolic protection device stenting. Res. Cardiovasc. Med. 2014, 3, e13012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neumann, F.J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef] [PubMed]
- Windecker, S.; Kolh, P.; Alfonso, F.; Collet, J.P.; Cremer, J.; Falk, V.; Filippatos, G.; Hamm, C.; Head, S.J.; Juni, P.; et al. 2014 ESC/EACTS Guidelines on myocardial revascularization: The Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) Developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur. Heart J. 2014, 35, 2541–2619. [Google Scholar] [PubMed]
- Wanha, W.; Mielczarek, M.; Roleder, T.; Ladzinski, S.; Milewski, M.; Gilis-Malinowska, N.; Chmielecki, M.; Ciecwierz, D.; Bachorski, W.; Kunik, P.; et al. New-generation drug eluting stent vs. bare metal stent in saphenous vein graft—1 year outcomes by a propensity score ascertainment (SVG Baltic Registry). Int. J. Cardiol. 2019, 292, 56–61. [Google Scholar] [CrossRef]
- Cutlip, D.E.; Windecker, S.; Mehran, R.; Boam, A.; Cohen, D.J.; van Es, G.A.; Steg, P.G.; Morel, M.A.; Mauri, L.; Vranckx, P.; et al. Clinical end points in coronary stent trials: A case for standardized definitions. Circulation 2007, 115, 2344–2351. [Google Scholar] [CrossRef] [Green Version]
- Brennan, J.M.; Al-Hejily, W.; Dai, D.; Shaw, R.E.; Trilesskaya, M.; Rao, S.V.; Brilakis, E.S.; Anstrom, K.J.; Messenger, J.C.; Peterson, E.D.; et al. Three-year outcomes associated with embolic protection in saphenous vein graft intervention: Results in 49 325 senior patients in the Medicare-linked National Cardiovascular Data Registry CathPCI Registry. Circ. Cardiovasc. Interv. 2015, 8, e001403. [Google Scholar] [CrossRef] [Green Version]
- Dixon, S.R.; Mann, J.T.; Lauer, M.A.; Casale, P.N.; Dippel, E.J.; Strumpf, R.K.; Feldman, R.L.; Shear, W.; Resar, J.R.; Zimmer, S.D.; et al. A randomized, controlled trial of saphenous vein graft intervention with a filter-based distal embolic protection device: TRAP trial. J. Interv. Cardiol. 2005, 18, 233–241. [Google Scholar] [CrossRef]
- Iqbal, M.B.; Nadra, I.J.; Ding, L.; Fung, A.; Aymong, E.; Chan, A.W.; Hodge, S.; Della Siega, A.; Robinson, S.D.; British Columbia Cardiac Registry, I. Embolic protection device use and its association with procedural safety and long-term outcomes following saphenous vein graft intervention: An analysis from the British Columbia Cardiac registry. Catheter. Cardiovasc. Interv. 2016, 88, 73–83. [Google Scholar] [CrossRef]
- Baim, D.S.; Wahr, D.; George, B.; Leon, M.B.; Greenberg, J.; Cutlip, D.E.; Kaya, U.; Popma, J.J.; Ho, K.K.; Kuntz, R.E.; et al. Randomized trial of a distal embolic protection device during percutaneous intervention of saphenous vein aorto-coronary bypass grafts. Circulation 2002, 105, 1285–1290. [Google Scholar] [CrossRef]
- Golwala, H.; Hawkins, B.M.; Stavrakis, S.; Abu-Fadel, M.S. Embolic protection device use and outcomes in patients receiving saphenous vein graft interventions—A single-center experience. J. Invasive Cardiol. 2012, 24, 1–3. [Google Scholar]
- Lee, M.; Kong, J. Current State of the Art in Approaches to Saphenous Vein Graft Interventions. Interv. Cardiol. 2017, 12, 85–91. [Google Scholar] [CrossRef] [Green Version]
- Badhey, N.; Lichtenwalter, C.; de Lemos, J.A.; Roesle, M.; Obel, O.; Addo, T.A.; Haagen, D.; Abdel-Karim, A.R.; Saeed, B.; Bissett, J.K.; et al. Contemporary use of embolic protection devices in saphenous vein graft interventions: Insights from the stenting of saphenous vein grafts trial. Catheter. Cardiovasc. Interv. 2010, 76, 263–269. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
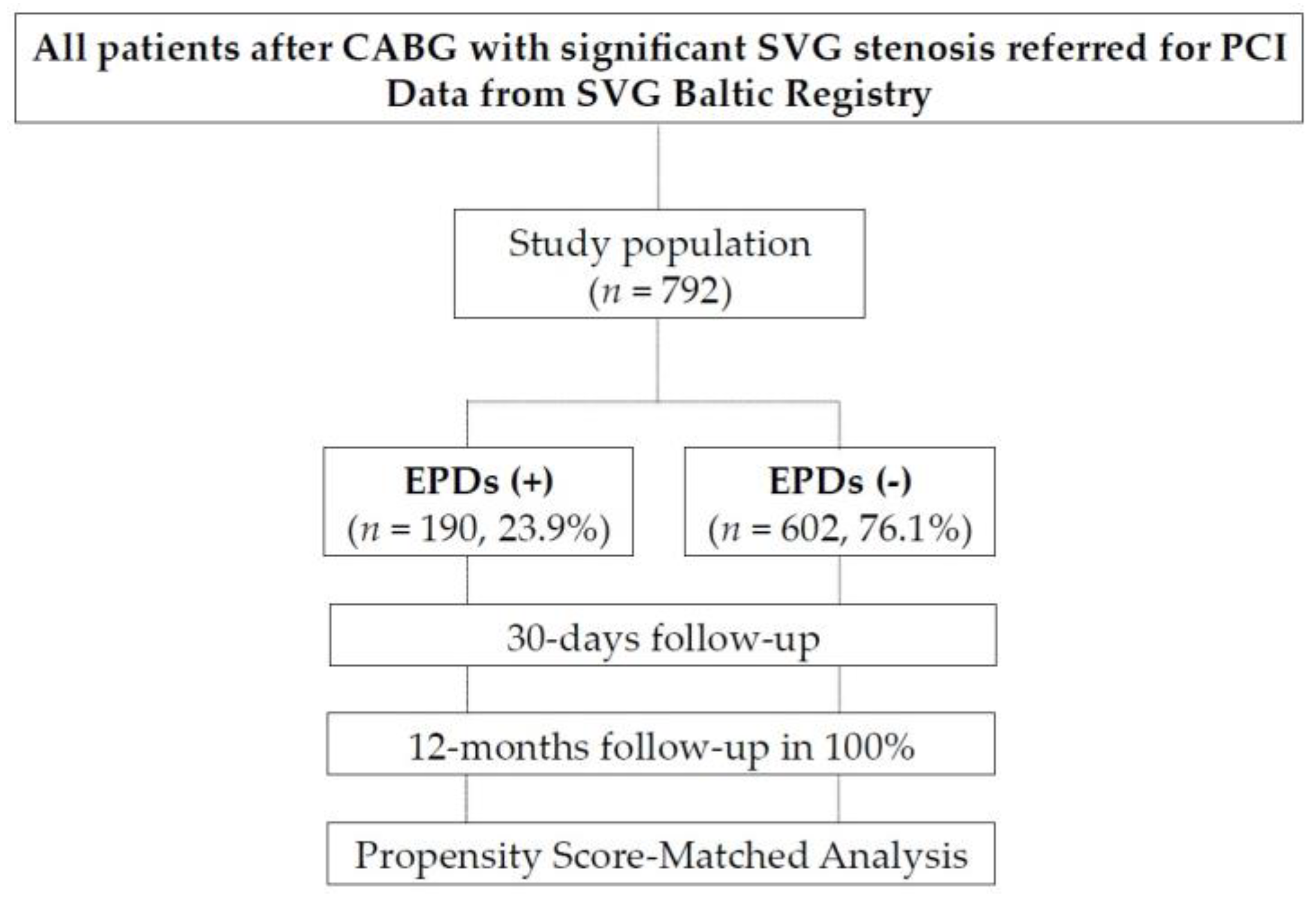
| EPDs (+) n = 190 (23.9%) | EPDs (−) n = 602 (76.1%) | p | |
|---|---|---|---|
| Demographic data | |||
| Age, median (IQR) | 70.0 (63.0–76.0) | 69.0 (62.0–75.0) | 0.124 |
| Male, n (%) | 145 (76.3) | 457(75.9) | 0.909 |
| BMI (kg/m2), median (IQR) | 29.0 (26.4–31.8) | 27.8 (25.4–30.8) | 0.111 |
| Discharge diagnosis | |||
| SA, n (%) | 61 (32.1) | 173 (28.7) | 0.375 |
| UA, n (%) | 68 (35.8) | 224 (37.2) | 0.724 |
| NSTEMI, n (%) | 50 (26.3) | 166 (27.6) | 0.734 |
| STEMI, n (%) | 11 (5.8) | 39 (6.5) | 0.865 |
| CAD history | |||
| Previous MI, n (%) | 137 (72.1) | 422 (70.1) | 0.597 |
| Previous PCI, n (%) | 93 (48.9) | 324 (53.8) | 0.241 |
| Graft age, median (IQR) | 13.8 (10.7–16.4) | 12.7(8.8–15.6) | 0.005 |
| CAD risk factors | |||
| Hypertension, n (%) | 171 (90.0) | 533 (88.5) | 0.576 |
| Dyslipidemia, n (%) | 146 (76.8) | 435 (72.3) | 0.213 |
| CKD, n (%) | 42 (22.1) | 159 (26.4) | 0.234 |
| Diabetes mellitus, n (%) | 82 (43.2) | 253 (42.0) | 0.783 |
| Current Smoking, n (%) | 54 (28.4) | 108 (17.9) | 0.002 |
| Family history of CAD, n (%) | 67 (35.3) | 156 (25.9) | 0.012 |
| Concomitant disease | |||
| Cancer, n (%) | 11 (5.8) | 26 (4.3) | 0.431 |
| COPD, n (%) | 14(7.3) | 41(6.8) | 0.792 |
| PAD, n (%) | 37 (19.5) | 123 (20.4) | 0.774 |
| Carotid artery disease, n (%) | 17 (8.9) | 81 (13.5) | 0.129 |
| Length of hospital stay, median (IQR) | 5.0 (3.0–7.0) | 4.0 (3.0–6.0) | 0.012 |
| CCS, median (IQR) | 3.0(2.0–4.0) | 3.0(2.0–4.0) | 0.939 |
| NYHA, median (IQR) | 1.0(1.0–2.0) | 1.0(1.0–2.0) | 0.097 |
| LVEF, median (IQR) | 50.0 (38.0–55.0) | 48.0 (38.0–55.0) | 0.427 |
| GRACE score >140, n (%) | 12 (15.2) | 31 (14.2) | 0.853 |
| euroSCORE II, median, (IQR) | 4.5 (3.0–9.0) | 4.6 (2.8–8.2) | 0.711 |
| EPDs (+) n = 190 (23.9%) | EPDs (−) n = 602 (76.1%) | p | |
|---|---|---|---|
| Access, n (%) | |||
| Radial | 27 (14.2) | 84 (14.0) | 0.955 |
| Femoral | 163 (85.8) | 514 (86.0) | |
| Degree of stenosis, (%), median (IQR) | 90.0 (80.0–95.0) | 90.0 (80.0–95.0) | 0.528 |
| Thrombus, n (%) | 19 (10.0) | 47 (7.8) | 0.366 |
| Restenosis in previously implanted stent, n (%) | 11 (5.8) | 59 (9.8) | 0.106 |
| Stent thrombosis in previous implanted stent, n (%) | 4 (2.1) | 5 (0.8) | 0.230 |
| PCI, n (%) | |||
| Ao-LAD | 53 (27.9) | 144 (23.9) | 0.269 |
| Ao-LCx | 85 (44.7) | 273 (45.3) | 0.883 |
| Ao-RCA | 53 (27.9) | 198 (32.9) | 0.197 |
| Ao-Y | 8 (4.2) | 30 (5.0) | 0.846 |
| Segment, n (%) | |||
| Proximal | 68 (35.8) | 179 (29.7) | 0.116 |
| Mid | 41 (21.6) | 89 (14.8) | 0.027 |
| Distal | 17 (8.9) | 148 (24.6) | <0.001 |
| Other | 66 (34.7) | 200 (33.2) | 0.700 |
| Stent, n (%) | |||
| new-DES | 112 (58.9) | 267 (44.4) | <0.001 |
| BMS | 78 (41.1) | 335 (55.6) | <0.001 |
| Predilatation, n (%) | 56 (29.5) | 172 (28.6) | 0.811 |
| Thrombectomy, n (%) | 10 (5.4) | 32 (5.6) | 0.902 |
| Total stent length (mm), median (IQR) | 20.0 (15.5–31.0) | 20.0 (15.0–29.0) | 0.083 |
| Length of stent > 28mm, n (%) | 64 (34.6) | 177 (29.6) | 0.198 |
| Average stent diameter (mm), median (IQR) | 3.5 (3.3–4.0) | 3.0 (3.0–3.5) | <0.001 |
| Stent diameter > 3.5mm, n (%) | 140 (73.7) | 284 (47.4) | <0.001 |
| Number of implanted stents, median (IQR) | 1.0 (1.0–2.0) | 1.0 (1.0–1.8) | 0.708 |
| Residual stenosis, n (%) | 5 (2.6) | 19 (3.2) | 0.813 |
| TIMI 3 post-PCI, n (%) | 187 (98.4) | 592 (98.3) | 0.938 |
| Vessel perforation, n (%) | 1 (0.5) | 1 (0.2) | 0.422 |
| Dissection, n (%) | 4 (2.1) | 7 (1.2) | 0.306 |
| No reflow during PCI, n (%) | 5 (2.6) | 8 (1.3) | 0.218 |
| Periprocedural MI, n (%) | 3 (1.6) | 12 (2.0) | 1.000 |
| IIb/IIIa inhibitors, n (%) | 25 (13.2) | 86 (14.3) | 0.721 |
| Cardiac arrest, n (%) | 1 (0.5) | 10 (1.7) | 0.475 |
| Intra-aortic balloon pump, n (%) | 0 (0) | 10 (1.7) | - |
| Acute Stent thrombosis, n (%) | 2 (1.1) | 3 (0.5) | 0.599 |
| Subacute Stent thrombosis, n (%) | 0 (0) | 0 (0) | - |
| Calcifications, n (%) | 3 (1.6) | 3 (0.5) | 0.279 |
| EPDs (+) n = 190 (23.9%) | EPDs (−) n = 602 (76.1%) | Crude Calculation | ||
|---|---|---|---|---|
| HR (95% CI) | p | |||
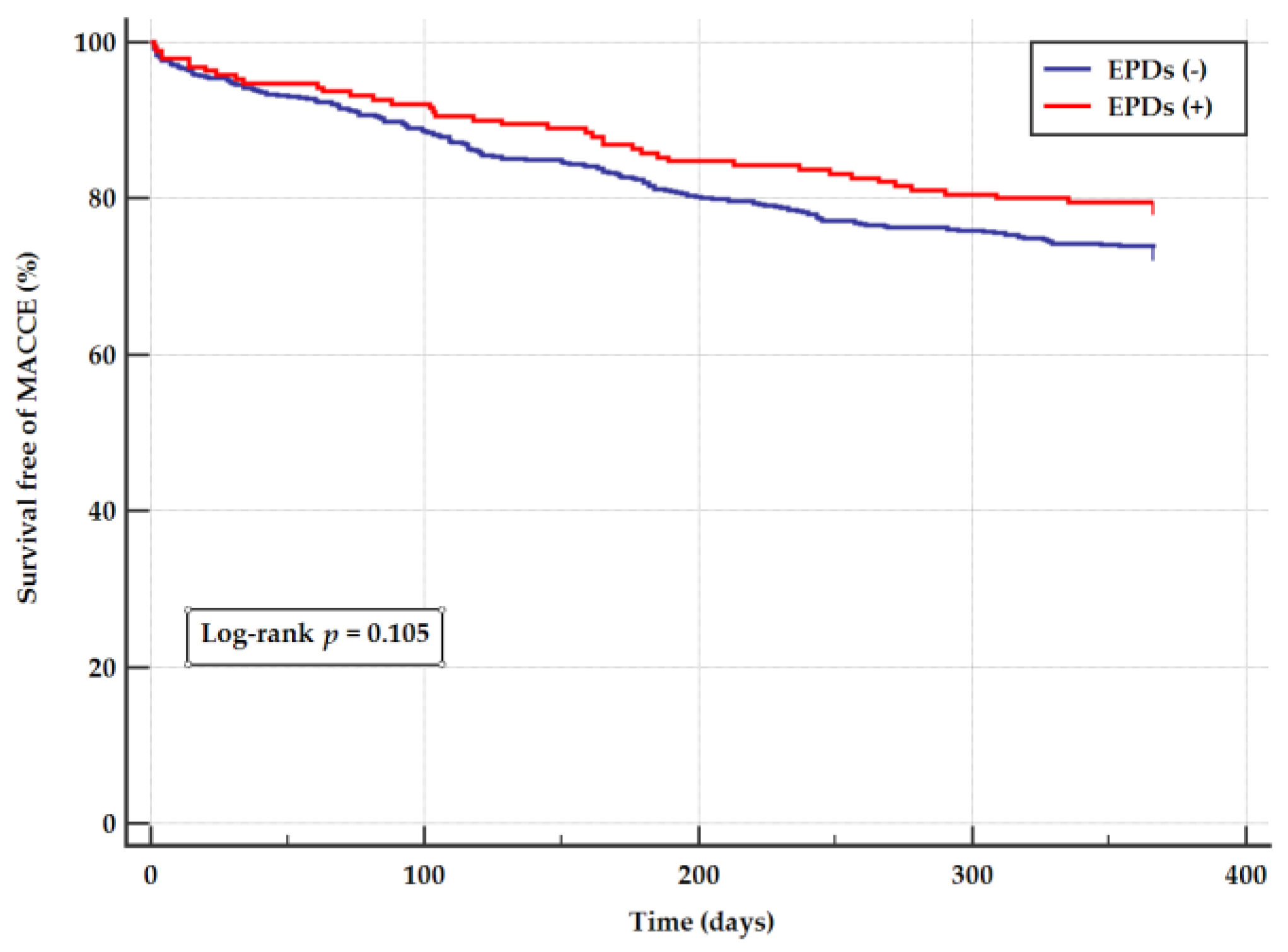
| MACCE | 39 (20.5) | 159 (26.4) | 0.75 (0.53–1.06) | 0.105 |
| Death | 8 (4.2) | 47 (7.8) | 0.53 (0.25–1.12) | 0.094 |
| MI | 14 (7.4) | 60 (10.0) | 0.73 (0.41–1.30) | 0.281 |
| Stroke | 2 (1.1) | 10 (1.7) | 0.63 (0.14–2.89) | 0.551 |
| TVR | 17 (8.9) | 74 (12.3) | 0.72 (0.43–1.22) | 0.220 |
| TLR | 13 (6.8) | 53 (8.8) | 0.78 (0.43–1.43) | 0.424 |
| EPDs (+) n = 155 | EPDs (−) n = 155 | Propensity Score | ||
|---|---|---|---|---|
| HR (95% CI) | p-Value | |||
| MACCE | 34 (21.9) | 37 (23.9) | 0.91 (0.57–1.45) | 0.681 |
| Death | 5 (3.2) | 9 (5.8) | 0.54 (0.18–1.62) | 0.271 |
| MI | 13 (8.4) | 13 (8.4) | 1.00 (0.46–2.15) | 0.994 |
| Stroke | 1 (0.6) | 1 (0.6) | 1.00 (0.06–16.0) | 0.998 |
| TVR | 16 (10.3) | 20 (12.9) | 0.80 (0.41–1.54) | 0.497 |
| TLR | 12 (7.7) | 16 (10.3) | 0.75 (0.36–1.59) | 0.451 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wańha, W.; Mielczarek, M.; Gilis-Malinowska, N.; Roleder, T.; Milewski, M.; Ładziński, S.; Ciećwierz, D.; Gąsior, P.; Pawłowski, T.; Januszek, R.; et al. Safety and Efficacy of Embolic Protection Devices in Saphenous Vein Graft Interventions: A Propensity Score Analysis—Multicenter SVG PCI PROTECTA Study. J. Clin. Med. 2020, 9, 1198. https://doi.org/10.3390/jcm9041198
Wańha W, Mielczarek M, Gilis-Malinowska N, Roleder T, Milewski M, Ładziński S, Ciećwierz D, Gąsior P, Pawłowski T, Januszek R, et al. Safety and Efficacy of Embolic Protection Devices in Saphenous Vein Graft Interventions: A Propensity Score Analysis—Multicenter SVG PCI PROTECTA Study. Journal of Clinical Medicine. 2020; 9(4):1198. https://doi.org/10.3390/jcm9041198
Chicago/Turabian StyleWańha, Wojciech, Maksymilian Mielczarek, Natasza Gilis-Malinowska, Tomasz Roleder, Marek Milewski, Szymon Ładziński, Dariusz Ciećwierz, Paweł Gąsior, Tomasz Pawłowski, Rafał Januszek, and et al. 2020. "Safety and Efficacy of Embolic Protection Devices in Saphenous Vein Graft Interventions: A Propensity Score Analysis—Multicenter SVG PCI PROTECTA Study" Journal of Clinical Medicine 9, no. 4: 1198. https://doi.org/10.3390/jcm9041198