Chagas Disease: Detection of Trypanosoma cruzi by a New, High-Specific Real Time PCR



Abstract
:1. Introduction
2. Material and Methods
2.1. Ethical Clearance
2.2. Study Design
2.3. Demographic Overview
2.4. Clinical Assessment
2.5. Clinical Samples
3. Serologic Methods
3.1. DNA Extractions
3.2. Real-Time-Polymerase Chain Reactions (RT-PCR) (kDNA, TCZ, and 18s rRNA)
3.3. Sequencing
3.4. Newly Developed One Real-Time Polymerase Chain Reaction (NDO-RT-PCR)
3.5. Disease Classification
3.6. Statistical Analysis
- -
- Sensitivity: tp/tp + fn
- -
- Specificity: tn/tn + fp
- -
- Positive Predictive Value (PPV, precision): tp/tp + fp
- -
- Negative Predictive Value (NPV): tn/tn + fn
- -
- Accuracy (correct classification rate): tp + tn/tp + fp + tn + fn
- -
- False Negative Rate (FNR): fn/tp + fn
- -
- False Positive Rate (FPR): fp/tn + fp
- -
- Prevalence: tp + fn/tp + fp + tn + fn
4. Results
4.1. Results of the NDO-PCR
4.2. Sequenced Samples (87)
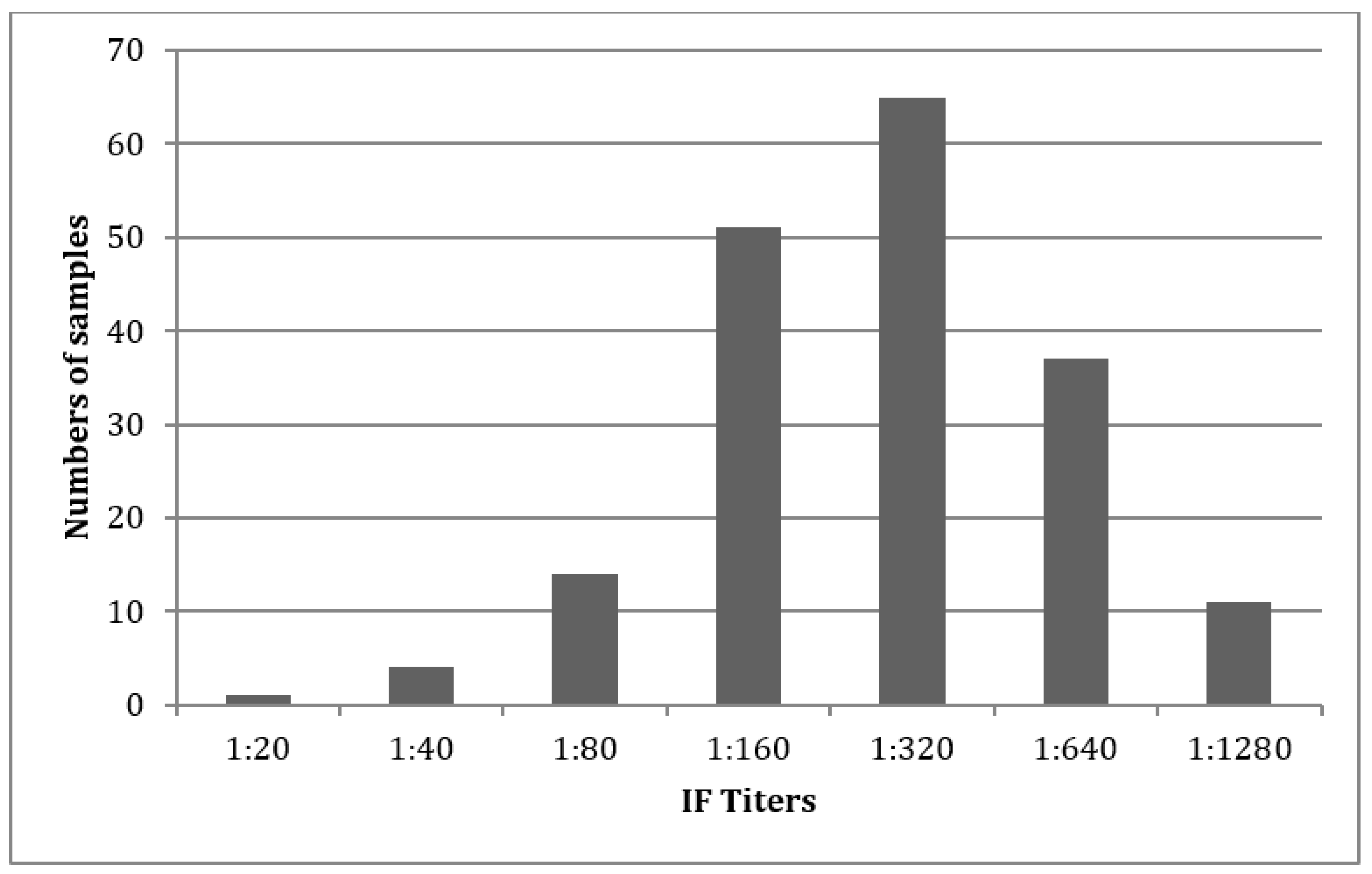
5. Serology
6. PCR Run Analysis
Analysis of the Non-Sequenced Samples (265)
7. Disease Classification Outcomes
7.1. Sequenced Samples (87)
7.2. Not Sequenced Samples (265)
7.3. Overall Analysis (352)
7.4. Chronic Cases Were Found in 70 Cases
8. Test Combinations
9. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Andrade, D.V.; Gollob, K.J.; Dutra, W.O. Acute chagas disease: New global challenges for an old neglected disease. PLoS Negl. Trop. Dis. 2014, 8, 3010. [Google Scholar] [CrossRef] [PubMed]
- Meymandi, S.; Hernandez, S.; Park, S.; Sanchez, D.R.; Forsyth, C. Treatment of chagas disease in the United States. Curr. Treat. Options Infect. Dis. 2018, 10, 373–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martins-Melo, F.R.; Alencar, C.H.; Ramos, A.N., Jr.; Heukelbach, J. Epidemiology of mortality related to chagas’ disease in Brazil, 1999–2007. PLoS Negl. Trop. Dis. 2012, 6, 1508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gascon, J.; Bern, C.; Pinazo, M.J. Chagas disease in Spain, the united states and other non-endemic countries. Acta Trop. 2010, 115, 22–27. [Google Scholar] [CrossRef]
- Schmunis, G.A. Epidemiology of chagas disease in non-endemic countries: The role of international migration. Mem. Inst. Oswaldo Cruz 2007, 102, 75–85. [Google Scholar] [CrossRef]
- Piron, M.; Fisa, R.; Casamitjana, N.; Lopez-Chejade, P.; Puig, L.; Verges, M.; Gascon, J.; Gomez i Prat, J.; Portus, M.; Sauleda, S. Development of a real-time PCR assay for trypanosoma cruzi detection in blood samples. Acta Trop. 2007, 103, 195–200. [Google Scholar] [CrossRef]
- Health Situation in the Americas. Neglected Tropical Diseases (nid). Available online: https://www.paho.org/salud-en-las-americas-2017/?p=1244 (accessed on 12 May 2017).
- Reithinger, R.; Tarleton, R.L.; Urbina, J.A.; Kitron, U.; Gurtler, R.E. Eliminating chagas disease: Challenges and a roadmap. BMJ 2009, 338, 1283. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Content Source: Global Health, Division of Parasitic Diseases. Available online: https://www.cdc.gov/parasites/chagas/prevent.html (accessed on 6 March 2019).
- World Health Organization (WHO). Chagas Disease (American Trypanosomiasis). 2020. Available online: https://www.who.int/health-topics/chagas-disease#tab=tab_1 (accessed on 8 May 2020).
- Pecoul, B.; Batista, C.; Stobbaerts, E.; Ribeiro, I.; Vilasanjuan, R.; Gascon, J.; Pinazo, M.J.; Moriana, S.; Gold, S.; Pereiro, A.; et al. The benefit trial: Where do we go from here? PLoS Negl. Trop. Dis. 2016, 10, 0004343. [Google Scholar] [CrossRef]
- Volta, B.J.; Russomando, G.; Bustos, P.L.; Scollo, K.; De Rissio, A.M.; Sanchez, Z.; Cardoni, R.L.; Bua, J. Diagnosis of congenital Trypanosoma cruzi infection: A serologic test using shed acute phase antigen (SAPA) in mother-child binomial samples. Acta Trop. 2015, 147, 31–37. [Google Scholar] [CrossRef]
- Duarte, L.F.F.O.; Rincon, G.; Gonzales, C.I. Comparison of seven diagnostic tests to detect Trypanosoma cruzi infection in patients in chronic phase of chagas disease. Colomb. Med. 2014, 45, 61–66. [Google Scholar] [CrossRef]
- WHO. Consultation on International Biological Reference Preparations for Chagas Diagnostic Tests. Available online: https://www.who.int/bloodproducts/ref_materials/WHO_Report_1st_Chagas_BRP_consultation_7-2007_final.pdf?ua=1 (accessed on 6 March 2019).
- Qvarnstrom, Y.; Schijman, A.G.; Veron, V.; Aznar, C.; Steurer, F.; da Silva, A.J. Sensitive and specific detection of trypanosoma cruzi DNA in clinical specimens using a multi-target real-time PCR approach. PLoS Negl. Trop. Dis. 2012, 6, 1689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seiringer, P.; Pritsch, M.; Flores-Chavez, M.; Marchisio, E.; Helfrich, K.; Mengele, C.; Hohnerlein, S.; Bretzel, G.; Loscher, T.; Hoelscher, M.; et al. Comparison of four PCR methods for efficient detection of Trypanosoma cruzi in routine diagnostics. Diagn. Microbiol. Infect. Dis. 2017, 88, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Balouz, V.; Aguero, F.; Buscaglia, C.A. Chagas disease diagnostic applications: Present knowledge and future steps. Adv. Parasitol. 2017, 97, 1–45. [Google Scholar] [PubMed] [Green Version]
- Bermejo, D.A.; Jackson, S.W.; Gorosito-Serran, M.; Acosta-Rodriguez, E.V.; Amezcua-Vesely, M.C.; Sather, B.D.; Singh, A.K.; Khim, S.; Mucci, J.; Liggitt, D.; et al. Trypanosoma cruzi trans-sialidase initiates a program independent of the transcription factors rorgammat and ahr that leads to il-17 production by activated b cells. Nat. Immunol. 2013, 14, 514–522. [Google Scholar] [CrossRef] [PubMed]
- Alonso-Padilla, J.; Rodriguez, A. High throughput screening for anti-Trypanosoma cruzi drug discovery. PLoS Negl. Trop. Dis. 2014, 8, 3259. [Google Scholar] [CrossRef] [PubMed]
- Schijman, A.G.; Bisio, M.; Orellana, L.; Sued, M.; Duffy, T.; Mejia Jaramillo, A.M.; Cura, C.; Auter, F.; Veron, V.; Qvarnstrom, Y.; et al. International study to evaluate PCR methods for detection of Trypanosoma cruzi DNA in blood samples from chagas disease patients. PLoS Negl. Trop. Dis. 2011, 5, 931. [Google Scholar] [CrossRef]
- Ramirez, J.C.; Cura, C.I.; da Cruz Moreira, O.; Lages-Silva, E.; Juiz, N.; Velazquez, E.; Ramirez, J.D.; Alberti, A.; Pavia, P.; Flores-Chavez, M.D.; et al. Analytical validation of quantitative real-time PCR methods for quantification of Trypanosoma cruzi DNA in blood samples from chagas disease patients. J. Mol. Diagn. 2015, 17, 605–615. [Google Scholar] [CrossRef]
- De Winne, K.; Buscher, P.; Luquetti, A.O.; Tavares, S.B.; Oliveira, R.A.; Solari, A.; Zulantay, I.; Apt, W.; Diosque, P.; Monje Rumi, M.; et al. The Trypanosoma cruzi satellite DNA oligoc-test and trypanosoma cruzi kinetoplast DNA oligoc-test for diagnosis of chagas disease: A multi-cohort comparative evaluation study. PLoS Negl. Trop. Dis. 2014, 8, 2633. [Google Scholar] [CrossRef]
- Arroyave, E.; Londono, A.F.; Quintero, J.C.; Agudelo-Florez, P.; Arboleda, M.; Diaz, F.J.; Rodas, J.D. Etiology and epidemiological characterization of non-malarial febrile syndrome in three municipalities of Uraba (Antioquia), Colombia. Biomed. Rev. Inst. Nac. Salud 2013, 33, 99–107. [Google Scholar]
- Blonshine, S.; Fallon, K.D.; Lehman, C.M.; Sittig, S. Procedures for the Collection of Diagnostic Specimens by Venipuncture: Approved Standard-Fourth Edition. Available online: https://clsi.org/media/1370/gp43a4_sample.pdf (accessed on 12 May 2017).
- Flores-Chavez, M.D.; Sambri, V.; Schottstedt, V.; Higuera-Escalante, F.A.; Roessler, D.; Chaves, M.; Laengin, T.; Martinez, A.; Fleischer, B. Evaluation of the elecsys chagas assay for detection of Trypanosoma cruzi-specific antibodies in a multicenter study in Europe and Latin America. J. Clin. Microbiol. 2018, 56. [Google Scholar] [CrossRef] [Green Version]
- Available online: http://blast.ncbi.nlm.gob//Blast.cgi (accessed on 12 May 2017).
- Kann, S.; Hansen, J. Oligunukleotide und Deren Verwendung. DE 10 2015 111 267.1 19 January 2017. [Google Scholar]
- Available online: http://www.phpmyadmin.net/home_page/ (accessed on 12 May 2017).
- Brisse, S.; Barnabe, C.; Banuls, A.L.; Sidibe, I.; Noel, S.; Tibayrenc, M. A phylogenetic analysis of the Trypanosoma cruzi genome project cl brener reference strain by multilocus enzyme electrophoresis and multiprimer random amplified polymorphic DNA fingerprinting. Mol. Biochem. Parasitol. 1998, 92, 253–263. [Google Scholar] [CrossRef]
- El-Sayed, N.M.; Myler, P.J.; Bartholomeu, D.C.; Nilsson, D.; Aggarwal, G.; Tran, A.N.; Ghedin, E.; Worthey, E.A.; Delcher, A.L.; Blandin, G.; et al. The genome sequence of Trypanosoma cruzi, etiologic agent of chagas disease. Science 2005, 309, 409–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, S.C. Establishment of clones of Trypanosoma cruzi and their characterization in vitro and in vivo. Bull. World Health Organ. 1982, 60, 101–107. [Google Scholar] [PubMed]
- Brisse, S.; Dujardin, J.C.; Tibayrenc, M. Identification of six Trypanosoma cruzi lineages by sequence-characterised amplified region markers. Mol. Biochem. Parasitol. 2000, 111, 95–105. [Google Scholar] [CrossRef]
- Callejas-Hernandez, F.; Rastrojo, A.; Poveda, C.; Girones, N.; Fresno, M. Genomic assemblies of newly sequenced Trypanosoma cruzi strains reveal new genomic expansion and greater complexity. Sci. Rep. 2018, 8, 14631. [Google Scholar] [CrossRef]
- Cariola, J.; Prado, R.; Agosin, M.; Christen, R. Susceptibility of the hamster and peromyscus to experimental Trypanosoma cruzi infection (tulahuen strain). Bol. Inf. Parasit. Chil. 1950, 5, 44–45. [Google Scholar]
- Araujo-Lima, C.F.; Peres, R.B.; Silva, P.B.; Batista, M.M.; Aiub, C.A.F.; Felzenszwalb, I.; Soeiro, M.N.C. Repurposing strategy of atorvastatin against Trypanosoma cruzi: In vitro monotherapy and combined therapy with benznidazole exhibit synergistic trypanocidal activity. Antimicrob. Agents Chemother. 2018, 62. [Google Scholar] [CrossRef] [Green Version]
- Simoes-Silva, M.R.; Nefertiti, A.S.; De Araujo, J.S.; Batista, M.M.; Da Silva, P.B.; Bahia, M.T.; Menna-Barreto, R.S.; Pavao, B.P.; Green, J.; Farahat, A.A.; et al. Phenotypic screening in vitro of novel aromatic amidines against Trypanosoma cruzi. Antimicrob. Agents Chemother. 2016, 60, 4701–4707. [Google Scholar] [CrossRef] [Green Version]
- Carlier, Y.; Truyens, C. Congenital chagas disease as an ecological model of interactions between Trypanosoma cruzi parasites, pregnant women, placenta and fetuses. Acta Trop. 2015, 151, 103–115. [Google Scholar] [CrossRef]
- Tarleton, R.L.; Gurtler, R.E.; Urbina, J.A.; Ramsey, J.; Viotti, R. Chagas disease and the London declaration on neglected tropical diseases. PLoS Negl. Trop. Dis. 2014, 8, 3219. [Google Scholar] [CrossRef] [Green Version]
- Bermudez, J.; Davies, C.; Simonazzi, A.; Real, J.P.; Palma, S. Current drug therapy and pharmaceutical challenges for chagas disease. Acta Trop. 2016, 156, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Guhl, F.; Ramirez, J.D. Retrospective molecular integrated epidemiology of chagas disease in Colombia. Infect. Genet. Evol. 2013, 20, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, C.; Cucunuba, Z.; Florez, C.; Olivera, M.; Valencia, C.; Zambrano, P.; Leon, C.; Ramirez, J.D. Molecular diagnosis of chagas disease in Colombia: Parasitic loads and discrete typing units in patients from acute and chronic phases. PLoS Negl. Trop. Dis. 2016, 10, 0004997. [Google Scholar]
- Zingales, B.; Andrade, S.G.; Briones, M.R.; Campbell, D.A.; Chiari, E.; Fernandes, O.; Guhl, F.; Lages-Silva, E.; Macedo, A.M.; Machado, C.R.; et al. A new consensus for Trypanosoma cruzi intraspecific nomenclature: Second revision meeting recommends tci to tcvi. Mem. Inst. Oswaldo Cruz 2009, 104, 1051–1054. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, J.D.; Tapia-Calle, G.; Guhl, F. Genetic structure of Trypanosoma cruzi in Colombia revealed by a high-throughput nuclear multilocus sequence typing (nmlst) approach. BMC Genet. 2013, 14, 96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mejia-Jaramillo, A.M.; Agudelo-Uribe, L.A.; Dib, J.C.; Ortiz, S.; Solari, A.; Triana-Chavez, O. Genotyping of Trypanosoma cruzi in a hyper-endemic area of colombia reveals an overlap among domestic and sylvatic cycles of chagas disease. Parasites Vectors 2014, 7, 108. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Variable | Sequenced Samples (n = 87) | Unsequenced Samples (n = 265) | All Samples (n = 352) |
|---|---|---|---|
| Age | |||
| N (%) | 86 (98.85) | 265 (100) | 351 (99.72) |
| Mean | 23.92 | 18.95 | 20.17 |
| Median | 16 | 12 | 14 |
| Gender (%) | |||
| Female | 49 (56.32) | 133 (50.19) | 182 (51.70) |
| Male | 38 (43.68) | 132 (49.81) | 170 (48.30) |
| Region (%) | |||
| Wiwas | 69 (79.31) | 265 (100) | 334 (94.89) |
| Wintukwa | 18 (20.69) | 0 (0) | 18 (5.11) |
| Ashintukwa | 9 (10.34) | 22 (8.3) | 31 (8.81) |
| Marocaso | 16 (18.39) | 69 (26.04) | 85 (24.15) |
| Siminke | 19 (21.84) | 69 (26.04) | 88 (25.00) |
| Tezumake | 21 (24.14) | 105 (39.62) | 126 (35.80) |
| Savannah Crespo | 4 (4.60) | 0 (0) | 4 (1.14) |
| Arwamake | 17 (19.54) | 0 (0) | 17 (4.83) |
| Timaka | 1 (1.15) | 0 (0) | 1 (0.28) |
| Serology (At Least 2 Tests Positive) | 87 Sequenced Samples * | 265 Non-Sequenced Samples * | 352 All Samples * |
|---|---|---|---|
| Positive result | 71 | 112 | 183 |
| Negative result | 16 | 153 | 169 |
| Sensitivity (%) | 96.92 | ||
| Specificity (%) | 59.09 | ||
| PPV (%) | 87.50 | ||
| NPV (%) | 86.67 | ||
| FNR (%) | 3.08 | ||
| FPR (%) | 40.91 | ||
| Accuracy (%) | 87.36 |
| 87 Sequenced Samples (Total Number of Test Runs: 261) | PCRs | |||
|---|---|---|---|---|
| kDNA | 18S rRNA | TCZ | NDO | |
| True positive | 174 | 3 | 40 | 180 |
| False positive | 51 | 0 | 0 | 0 |
| False negative | 21 | 192 | 155 | 15 |
| True negative | 15 | 66 | 66 | 66 |
| Sensitivity (%) | 89.23 | 1.53 | 20.51 | 92.31 |
| Specificity (%) | 22.73 | 100 | 100 | 100 |
| PPV (%) | 77.33 | 100 | 100 | 100 |
| NPV (%) | 41.67 | 25.58 | 29.86 | 81.48 |
| FNR (%) | 10.77 | 98.46 | 79.49 | 7.69 |
| FPR (%) | 77.27 | 0 | 0 | 0 |
| Accuracy (%) | 72.41 | 26.44 | 40.61 | 94.25 |
| 352 Samples (87 Sequenced, 265 not Sequenced), (total Number of Test Runs: 1056) | PCRs | |||
|---|---|---|---|---|
| kDNA | 18S rRNA | TCZ | NDO | |
| True positive | 198 | 3 | 57 | 208 |
| False positive | 134 | 1 | 4 | 0 |
| False negative | 27 | 222 | 168 | 17 |
| True negative | 697 | 830 | 827 | 831 |
| Sensitivity (%) | 88.00 | 1.33 | 25.33 | 92.44 |
| Specificity (%) | 83.87 | 99.88 | 99.52 | 100 |
| PPV (%) | 59.64 | 75.00 | 93.44 | 100 |
| NPV (%) | 96.27 | 78.90 | 83.12 | 98.00 |
| FNR (%) | 12.00 | 98.67 | 74.67 | 7.56 |
| FPR (%) | 16.13 | 0.12 | 0.48 | 0 |
| Accuracy (%) | 84.75 | 78.88 | 83.71 | 98.39 |
| Methods | No. of Positive Results | No. of True Positive Results | No. of False Positive Results | Missed Chronic T. cruzi Infections | Missed Acute T. cruzi Infections |
|---|---|---|---|---|---|
| 2 ST only | 71 | 62 | 9 | 1 | n.a. |
| 1 ST + kDNA-PCR * | 72 | 63 | 9 | 0 | 2 |
| 1 ST + 18S rRNA-PCR * | 2 | 2 | 0 | 61 | 2 |
| 1 ST + TCZ-PCR * | 21 | 21 | 0 | 42 | 2 |
| 1 ST + NDO-PCR * | 62 | 62 | 0 | 1 | 2 |
| 2 ST + kDNA-PCR * | 71 | 62 | 9 | 1 | 2 |
| 2 ST + 18S rRNA-PCR * | 2 | 2 | 0 | 61 | 2 |
| 2 ST + TCZ-PCR * | 21 | 21 | 0 | 42 | 2 |
| 2 ST + NDO-PCR * | 61 | 61 | 0 | 2 | 2 |
| 0 ST + kDNA-PCR * | 13 | 0 | 13 | n.a. | 2 |
| 0 ST + 18S rRNA-PCR * | 0 | 0 | 0 | n.a. | 2 |
| 0 ST + TCZ-PCR * | 1 | 1 | 0 | n.a. | 1 |
| 0 ST + NDO-PCR * | 2 | 2 | 0 | n.a. | 0 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kann, S.; Kunz, M.; Hansen, J.; Sievertsen, J.; Crespo, J.J.; Loperena, A.; Arriens, S.; Dandekar, T. Chagas Disease: Detection of Trypanosoma cruzi by a New, High-Specific Real Time PCR. J. Clin. Med. 2020, 9, 1517. https://doi.org/10.3390/jcm9051517
Kann S, Kunz M, Hansen J, Sievertsen J, Crespo JJ, Loperena A, Arriens S, Dandekar T. Chagas Disease: Detection of Trypanosoma cruzi by a New, High-Specific Real Time PCR. Journal of Clinical Medicine. 2020; 9(5):1517. https://doi.org/10.3390/jcm9051517
Chicago/Turabian StyleKann, Simone, Meik Kunz, Jessica Hansen, Jürgen Sievertsen, Jose J. Crespo, Aristides Loperena, Sandra Arriens, and Thomas Dandekar. 2020. "Chagas Disease: Detection of Trypanosoma cruzi by a New, High-Specific Real Time PCR" Journal of Clinical Medicine 9, no. 5: 1517. https://doi.org/10.3390/jcm9051517
APA StyleKann, S., Kunz, M., Hansen, J., Sievertsen, J., Crespo, J. J., Loperena, A., Arriens, S., & Dandekar, T. (2020). Chagas Disease: Detection of Trypanosoma cruzi by a New, High-Specific Real Time PCR. Journal of Clinical Medicine, 9(5), 1517. https://doi.org/10.3390/jcm9051517