Outcomes after Complicated and Uncomplicated Mild Traumatic Brain Injury at Three-and Six-Months Post-Injury: Results from the CENTER-TBI Study

 ,
,  , , , , , ,
, , , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Participants
2.3. Instruments
2.3.1. Health-Related Quality of Life (HRQoL)
2.3.2. Functional Outcome
2.3.3. Post-Traumatic Stress, Depression, and Anxiety
2.4. Ethical Approval
2.5. Statistical Analyses
3. Results
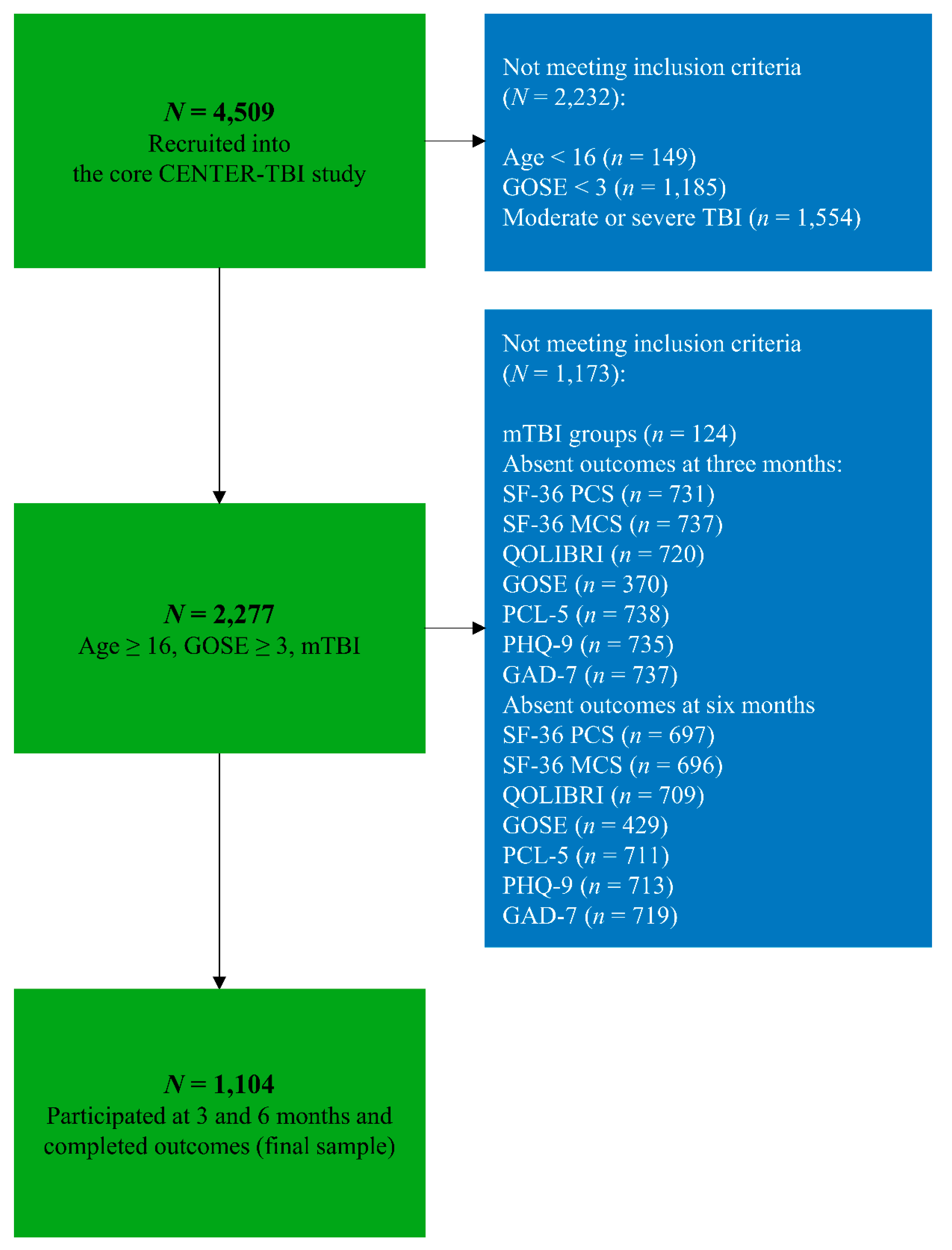
3.1. Study Sample
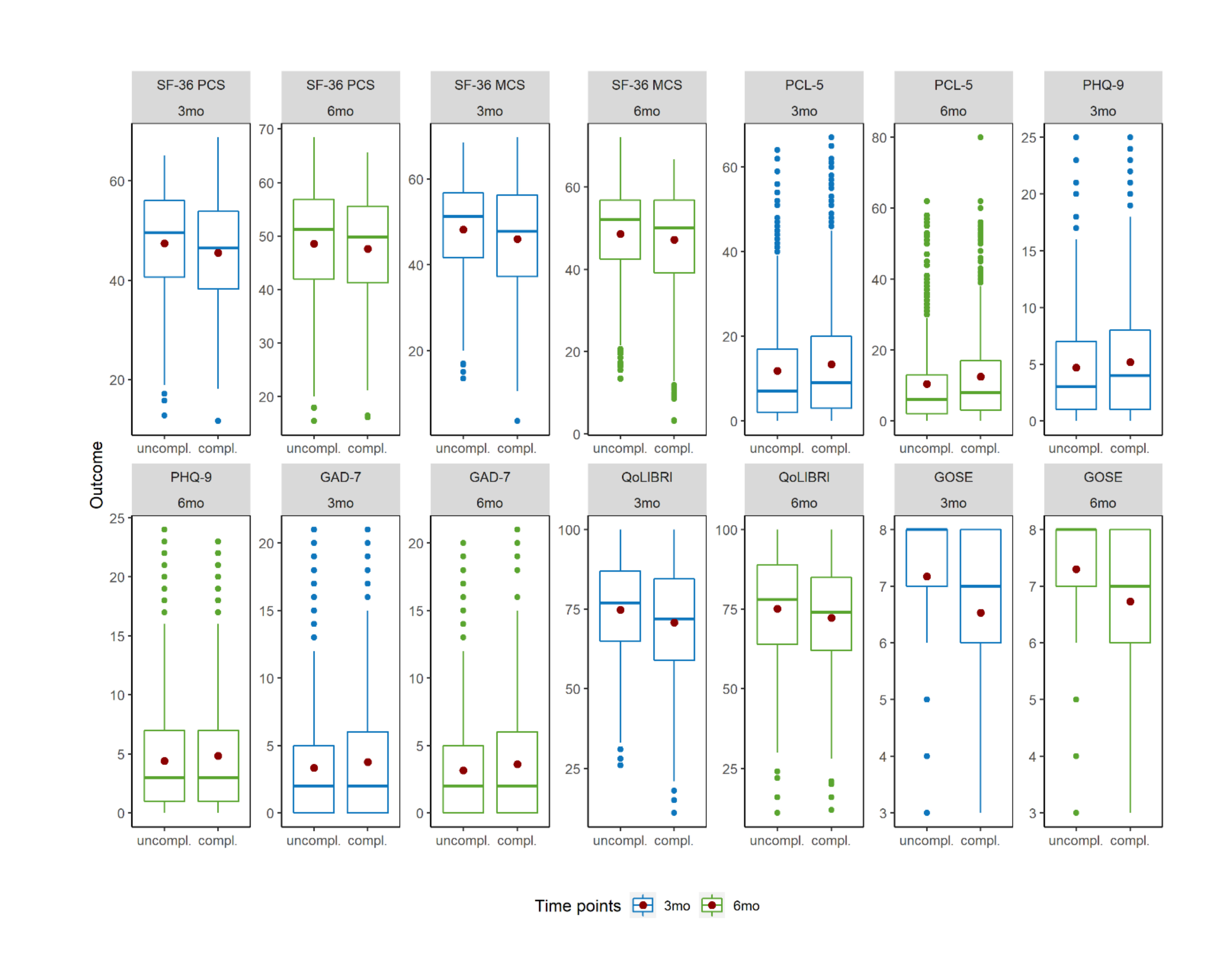
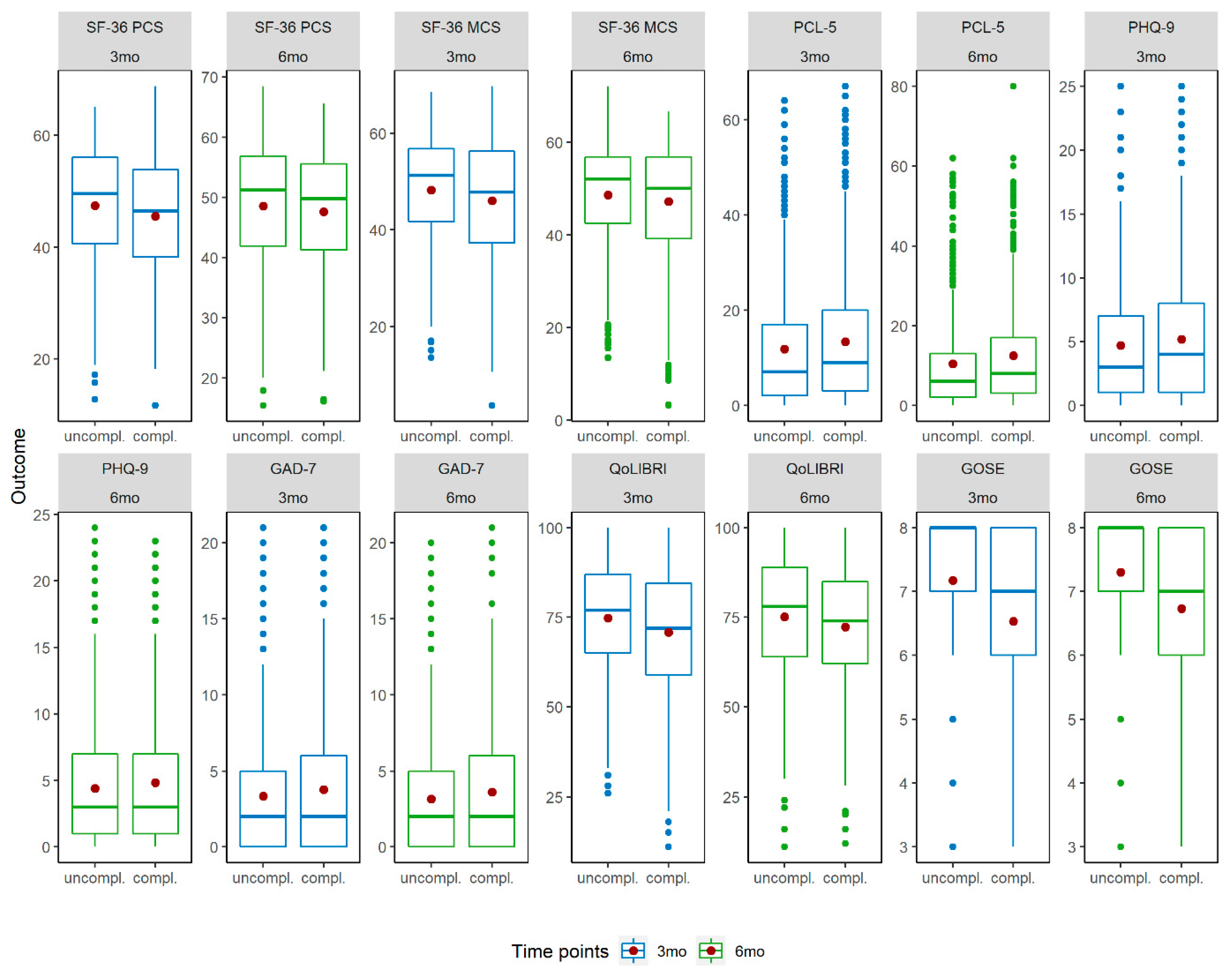
3.2. Descriptive Statistics of Outcomes
3.3. MANOVA-RM
3.4. Post-Hoc Comparisons
3.4.1. Health-Related Quality of Life
3.4.2. Functional Outcome
3.4.3. Post-Traumatic Stress, Depression, and Anxiety
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Uncomplicated mTBI (n = 569) | Complicated mTBI (n = 535) | ||||
|---|---|---|---|---|---|
| Outcome | Time Points | M | SD | M | SD |
| SF-36 PCS | 3mo | 47.41 | 10.56 | 45.56 | 10.22 |
| 6mo | 48.58 | 10.37 | 47.59 | 10.01 | |
| SF-36 MCS | 3mo | 48.24 | 10.89 | 45.98 | 12.14 |
| 6mo | 48.62 | 11.12 | 47.24 | 11.98 | |
| PCL-5 | 3mo | 11.80 | 13.00 | 13.33 | 13.86 |
| 6mo | 10.45 | 12.39 | 12.42 | 13.51 | |
| PHQ-9 | 3mo | 4.69 | 4.90 | 5.17 | 5.18 |
| 6mo | 4.40 | 4.92 | 4.84 | 5.10 | |
| GAD-7 | 3mo | 3.35 | 4.25 | 3.77 | 4.65 |
| 6mo | 3.15 | 4.02 | 3.61 | 4.64 | |
| QOLIBRI | 3mo | 74.77 | 16.46 | 70.79 | 17.45 |
| 6mo | 75.17 | 17.18 | 72.32 | 17.20 | |
| GOSE | 3mo | 7.17 | 1.10 | 6.53 | 1.42 |
| 6mo | 7.30 | 1.06 | 6.73 | 1.32 | |
Appendix B

References
- Maas, A.I.R.; Menon, D.K.; Adelson, P.D.; Andelic, N.; Bell, M.J.; Belli, A.; Bragge, P.; Brazinova, A.; Buki, A.; Chesnut, R.M. Traumatic brain injury: Integrated approaches to improve prevention, clinical care, and research. Lancet Neurol. 2017, 16, 987–1048. [Google Scholar] [CrossRef]
- Majdan, M.; Plancikova, D.; Brazinova, A.; Rusnak, M.; Nieboer, D.; Feigin, V.; Maas, A. Epidemiology of traumatic brain injuries in europe: A cross-sectional analysis. Lancet Public Health 2016, 1, e76–e83. [Google Scholar] [CrossRef]
- Williams, D.H.; Levin, H.S.; Eisenberg, H.M. Mild head injury classification. Neurosurgery 1990, 27, 422–428. [Google Scholar] [CrossRef] [PubMed]
- Iverson, G.L. Complicated vs uncomplicated mild traumatic brain injury: Acute neuropsychological outcome. Brain Inj. 2006, 20, 1335–1344. [Google Scholar] [CrossRef] [PubMed]
- Kashluba, S.; Hanks, R.A.; Casey, J.E.; Millis, S.R. Neuropsychologic and functional outcome after complicated mild traumatic brain injury. Arch. Phys. Med. Rehabil. 2008, 89, 904–911. [Google Scholar] [CrossRef] [PubMed]
- van der Naalt, J.; van Zomeren, A.H.; Sluiter, W.J.; Minderhoud, J.M. One year outcome in mild to moderate head injury: The predictive value of acute injury characteristics related to complaints and return to work. J. Neurol. Neurosurg. Psychiatry 1999, 66, 207–213. [Google Scholar] [CrossRef]
- Iverson, G.L.; Lange, R.T.; Waljas, M.; Liimatainen, S.; Dastidar, P.; Hartikainen, K.M.; Soimakallio, S.; Ohman, J. Outcome from complicated versus uncomplicated mild traumatic brain injury. Rehabil. Res. Pract. 2012, 2012, 415740. [Google Scholar] [CrossRef]
- Lee, H.; Wintermark, M.; Gean, A.D.; Ghajar, J.; Manley, G.T.; Mukherjee, P. Focal lesions in acute mild traumatic brain injury and neurocognitive outcome: Ct versus 3t mri. J. Neurotrauma 2008, 25, 1049–1056. [Google Scholar] [CrossRef]
- Panenka, W.J.; Lange, R.T.; Bouix, S.; Shewchuk, J.R.; Heran, M.K.; Brubacher, J.R.; Eckbo, R.; Shenton, M.E.; Iverson, G.L. Neuropsychological outcome and diffusion tensor imaging in complicated versus uncomplicated mild traumatic brain injury. PLoS ONE 2015, 10, e0122746. [Google Scholar] [CrossRef]
- van der Naalt, J.; Hew, J.M.; van Zomeren, A.H.; Sluiter, W.J.; Minderhoud, J.M. Computed tomography and magnetic resonance imaging in mild to moderate head injury: Early and late imaging related to outcome. Ann. Neurol. 1999, 46, 70–78. [Google Scholar] [CrossRef]
- Dikmen, S.; Machamer, J.; Temkin, N. Mild traumatic brain injury: Longitudinal study of cognition, functional status, and post-traumatic symptoms. J. Neurotrauma 2017, 34, 1524–1530. [Google Scholar] [CrossRef] [PubMed]
- Veeramuthu, V.; Narayanan, V.; Ramli, N.; Hernowo, A.; Waran, V.; Bondi, M.W.; Delano-Wood, L.; Ganesan, D. Neuropsychological outcomes in patients with complicated versus uncomplicated mild traumatic brain injury: 6-month follow-up. World Neurosurg. 2017, 97, 416–423. [Google Scholar] [CrossRef] [PubMed]
- McMahon, P.; Hricik, A.; Yue, J.K.; Puccio, A.M.; Inoue, T.; Lingsma, H.F.; Beers, S.R.; Gordon, W.A.; Valadka, A.B.; Manley, G.T.; et al. Symptomatology and functional outcome in mild traumatic brain injury: Results from the prospective track-tbi study. J. Neurotrauma 2014, 31, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Karr, J.E.; Iverson, G.L.; Berghem, K.; Kotilainen, A.K.; Terry, D.P.; Luoto, T.M. Complicated mild traumatic brain injury in older adults: Post-concussion symptoms and functional outcome at one week post injury. Brain Inj. 2020, 34, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Voormolen, D.C.; Haagsma, J.A.; Polinder, S.; Maas, A.I.R.; Steyerberg, E.W.; Vuleković, P.; Sewalt, C.A.; Gravesteijn, B.Y.; Covic, A.; Andelic, N.; et al. Post-concussion symptoms in complicated vs. Uncomplicated mild traumatic brain injury patients at three and six months post-injury: Results from the center-tbi study. J. Clin. Med. 2019, 8, 1921. [Google Scholar] [CrossRef]
- Polinder, S.; Haagsma, J.A.; van Klaveren, D.; Steyerberg, E.W.; van Beeck, E.F. Health-related quality of life after tbi: A systematic review of study design, instruments, measurement properties, and outcome. Popul. Health Metr. 2015, 13, 4. [Google Scholar] [CrossRef]
- von Steinbuechel, N.; Richter, S.; Morawetz, C.; Riemsma, R. Assessment of subjective health and health-related quality of life in persons with acquired or degenerative brain injury. Curr. Opin. Neurol. 2005, 18, 681–691. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Feeny, D.H.; Patrick, D.L. Measuring health-related quality of life. Ann. Intern. Med. 1993, 118, 622–629. [Google Scholar] [CrossRef]
- von Steinbuechel, N.; Petersen, C.; Bullinger, M.; Group, Q. Assessment of health-related quality of life in persons after traumatic brain injury—Development of the qolibri, a specific measure. Acta Neurochir. Suppl. 2005, 93, 43–49. [Google Scholar]
- Maestas, K.L.; Sander, A.M.; Clark, A.N.; van Veldhoven, L.M.; Struchen, M.A.; Sherer, M.; Hannay, H.J. Preinjury coping, emotional functioning, and quality of life following uncomplicated and complicated mild traumatic brain injury. J. Head Trauma Rehabil. 2014, 29, 407–417. [Google Scholar] [CrossRef]
- Ewing-Cobbs, L.; Prasad, M.; Fletcher, J.M.; Levin, H.S.; Miner, M.E.; Eisenberg, H.M. Attention after pediatric traumatic brain injury: A multidimensional assessment. Child. Neuropsychol. 1998, 4, 35–48. [Google Scholar] [CrossRef]
- Nelson, L.D.; Ranson, J.; Ferguson, A.R.; Giacino, J.; Okonkwo, D.O.; Valadka, A.; Manley, G.; McCrea, M. Validating multidimensional outcome assessment using the tbi common data elements: An analysis of the track-tbi pilot sample. J. Neurotrauma 2017, 34, 3158–3172. [Google Scholar] [CrossRef] [PubMed]
- Maas, A.I.; Menon, D.K.; Steyerberg, E.W.; Citerio, G.; Lecky, F.; Manley, G.T.; Hill, S.; Legrand, V.; Sorgner, A.; Participants, C.-T.; et al. Collaborative european neurotrauma effectiveness research in traumatic brain injury (center-tbi): A prospective longitudinal observational study. Neurosurgery 2015, 76, 67–80. [Google Scholar] [CrossRef] [PubMed]
- Steyerberg, E.; Wiegers, E.; Sewalt, C.; Buki, A.; Citerio, G.; Keyser, V.; Ercole, A.; Kunzmann, K.; Lanyon, L.; Lecky, F.; et al. Case-mix, care pathways, and outcomes in patients with traumatic brain injury in center-tbi: A european prospective, multicentre, longitudinal, cohort study. Lancet Neurol. 2019, 18, 923–934. [Google Scholar] [CrossRef]
- Abouleish, A.E.; Leib, M.L.; Cohen, N.H. Asa provides examples to each asa physical status class. ASA Newsl. 2015, 79, 38–49. [Google Scholar]
- Ware, J.E., Jr.; Sherbourne, C.D. The mos 36-item short-form health survey (sf-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef]
- Ware, J.E. User’s Manual for the Sf-36v2 Health Survey; Quality Metric: Lincoln, UK, 2007. [Google Scholar]
- von Steinbuchel, N.; Wilson, L.; Gibbons, H.; Hawthorne, G.; Hofer, S.; Schmidt, S.; Bullinger, M.; Maas, A.; Neugebauer, E.; Powell, J.; et al. Quality of life after brain injury (qolibri): Scale validity and correlates of quality of life. J. Neurotrauma 2010, 27, 1157–1165. [Google Scholar] [CrossRef]
- Wilson, L.; Marsden-Loftus, I.; Koskinen, S.; Bakx, W.; Bullinger, M.; Formisano, R.; Maas, A.; Neugebauer, E.; Powell, J.; Sarajuuri, J. Interpreting quality of life after brain injury scores: Cross-walk with the short form-36. J. Neurotrauma 2017, 34, 59–65. [Google Scholar] [CrossRef]
- Jennett, B.; Snoek, J.; Bond, M.R.; Brooks, N. Disability after severe head injury: Observations on the use of the glasgow outcome scale. J. Neurol. Neurosurg. Psychiatry 1981, 44, 285–293. [Google Scholar] [CrossRef]
- Wilson, J.T.; Pettigrew, L.E.; Teasdale, G.M. Structured interviews for the glasgow outcome scale and the extended glasgow outcome scale: Guidelines for their use. J. Neurotrauma 1998, 15, 573–585. [Google Scholar] [CrossRef]
- Jackson, C. Multi-state models for panel data: The msm package for R. J. Stat. Softw. 2011, 38, 28. [Google Scholar] [CrossRef]
- Blanchard, E.B.; Jones-Alexander, J.; Buckley, T.C.; Forneris, C.A. Psychometric properties of the ptsd checklist (pcl). Behav. Res. Ther. 1996, 34, 669–673. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; (dsm-5); American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Stein, M.B.; Jain, S.; Giacino, J.T.; Levin, H.; Dikmen, S.; Nelson, L.D.; Vassar, M.J.; Okonkwo, D.O.; Diaz-Arrastia, R.; Robertson, C.S.; et al. Risk of posttraumatic stress disorder and major depression in civilian patients after mild traumatic brain injury: A track-tbi study. JAMA Psychiatry 2019, 76, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The phq-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; (dsm-iv); American Psychiatric Association: Washington, DC, USA, 1994. [Google Scholar]
- Kroenke, K.; Spitzer, R.L. The phq-9: A new depression diagnostic and severity measure. Psychiatr. Ann. 2002, 32, 509–515. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Lowe, B. A brief measure for assessing generalized anxiety disorder: The gad-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef]
- Friedrich, S.; Konietschke, F.; Pauly, M. Manova.Rm: Resampling-Based Analysis of Multivariate Data and Repeated Measures Designs (Version R Package Version 0.4.1.). 2020. Available online: http://github.com/smn74/MANOVA.RM (accessed on 8 April 2020).
- Friedrich, S.; Konietschke, F.; Pauly, M. Resampling-based analysis of multivariate data and repeated measures designs with the r package manova.Rm. R J. 2019, 11, 380–400. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019. [Google Scholar]
- Shinn, E.; Pate, A.; Pinto, F.; Chendrasekhar, A. Long-term outcomes after mild traumatic brain injury. J. Am. Coll. Surg. 2014, 219, e144–e145. [Google Scholar] [CrossRef]
- Ponsford, J.; Nguyen, S.; Downing, M.; Bosch, M.; McKenzie, J.E.; Turner, S.; Chau, M.; Mortimer, D.; Gruen, R.L.; Knott, J. Factors associated with persistent post-concussion symptoms following mild traumatic brain injury in adults. J. Rehabil. Med. 2019, 51, 32–39. [Google Scholar] [CrossRef]
- Yuh, E.L.; Mukherjee, P.; Lingsma, H.F.; Yue, J.K.; Ferguson, A.R.; Gordon, W.A.; Valadka, A.B.; Schnyer, D.M.; Okonkwo, D.O.; Maas, A.I.; et al. Magnetic resonance imaging improves 3-month outcome prediction in mild traumatic brain injury. Ann. Neurol. 2013, 73, 224–235. [Google Scholar] [CrossRef]
- Corrigan, J.; Harrison-Felix, C.; Bogner, J.; Dijkers, M.; Terrill, M.; Whiteneck, G. Systematic bias in traumatic brain injury outcome studies because of loss to follow-up. Arch. Phys. Med. Rehabil. 2003, 84, 153–160. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, J.; Hibbard, M.R.; Brown, M.; Jaffe, M.; Sliwinski, M.; Vandergoot, D.; Weiss, M.J. The effect of employment on quality of life and community integration after traumatic brain injury. J. Head Trauma Rehabil. 1998, 13, 68–79. [Google Scholar] [CrossRef] [PubMed]


| Study Sample | Uncomplicated | Complicated | p-Value | |
|---|---|---|---|---|
| N | 1104 | 569 (51.5%) | 535 (48.5%) | |
| Care paths | <0.01 | |||
| ER | 338 (30.6%) | 286 (50.3%) | 52 (9.7%) | |
| Admission | 525 (47.6%) | 236 (41.5%) | 289 (54.0%) | |
| ICU | 241 (21.8%) | 47 (8.3%) | 194 (36.3%) | |
| Demographic characteristics | ||||
| Gender (male) | 700 (63.4%) | 352 (61.9%) | 348 (65.0%) | 0.272 |
| Age1 (years) | 54 [37.3–67] | 51 [35–65] | 58 [40–68] | <0.01 |
| Socio-economic characteristics | ||||
| Education1 (years) | 14 [12–17] | 14 [12–17] | 14 [11–17] | 0.054 |
| Employment status before injury | ||||
| Working 2 | 593 (53.7%) | 331 (58.2%) | 262 (49.0%) | <0.01 |
| Pre-injury health status and medical history | ||||
| Pre-injury ASA-PS classification | 0.175 | |||
| A patient with mild systemic disease | 377 (34.1%) | 181 (31.8%) | 196 (36.6%) | |
| A patient with severe systemic disease | 106 (9.6%) | 60 (10.5%) | 46 (8.6%) | |
| Previous TBI | 129 (11.7%) | 84 (14.8%) | 45 (8.4%) | <0.01 |
| Cause of injury | ||||
| Injury Mechanism | 0.409 | |||
| Road traffic accident | 429 (38.9%) | 222 (39.0%) | 207 (38.7%) | |
| Incidental fall | 517 (46.8%) | 265 (46.6%) | 252 (47.2%) | |
| Other non-intentional | 60 (5.4%) | 36 (6.3%) | 24 (4.5%) | |
| Violence/assault | 38 (3.4%) | 19 (3.3%) | 19 (3.6%) | |
| Act of mass violence | 1 (0.1%) | - | 1 (0.2%) | |
| Suicide attempt | 7 (0.6%) | 2 (0.4%) | 5 (0.9%) | |
| Other | 36 (3.3%) | 20 (3.5%) | 16 (3.0%) | |
| Unknown | 16 (1.4) | 5 (0.9%) | 11 (2.1%) | |
| Clinical presentation | ||||
| GCS baseline1 | 15 [15–15] | 15 [15–15] | 15 [14,15] | <0.01 |
| 13 | 65 (5.9%) | 9 (1.6%) | 56 (10.5%) | |
| 14 | 155 (14.0%) | 53 (9.3%) | 102 (19.1%) | |
| 15 | 884 (80.1%) | 507 (89.1%) | 377 (70.5%) | |
| CT characteristics | ||||
| Computed Tomography | ||||
| Any intracranial injury on first CT | 535 (48.5%) | 0 (0.0%) | 535 (100%) | <0.01 |
| Outcome | Time Points | Uncomplicated mTBI (n = 569) | Complicated mTBI (n = 535) |
|---|---|---|---|
| SF-36 PCS | 3mo | 24% | 29% |
| 6mo | 21% | 22% | |
| SF-36 MCS | 3mo | 22% | 30% |
| 6mo | 21% | 28% | |
| PCL-5 | 3mo | 10% | 10% |
| 6mo | 8% | 10% | |
| PHQ-9 | 3mo | 16% | 19% |
| 6mo | 16% | 16% | |
| GAD-7 | 3mo | 11% | 13% |
| 6mo | 8% | 11% | |
| QOLIBRI | 3mo | 19% | 26% |
| 6mo | 19% | 21% | |
| GOSE | 3mo | 23% | 41% |
| 6mo | 16% | 35% |
| Analysis | Dependent Variable(s) | Independent Variable | (M)ATS | df1 | df2 | p |
|---|---|---|---|---|---|---|
| MANOVA RM | Multiple outcomes * | mTBI | 197.538 | - | - | <0.001 |
| Time points | 34.708 | - | - | <0.001 | ||
| mTBI: Time points | 2.932 | - | - | 0.158 | ||
| ANOVA RM | SF-36 PCS | mTBI | 5.897 | 1 | 1365.422 | 0.015 |
| Time points | 61.133 | 1 | - | <0.001 | ||
| mTBI: Time points | 4.361 | 1 | - | 0.037 | ||
| SF-36 MCS | mTBI | 7.879 | 1 | 1399.985 | 0.005 | |
| Time points | 10.502 | 1 | - | 0.001 | ||
| mTBI: Time points | 3.058 | 1 | - | 0.080 | ||
| PCL-5 | mTBI | 5.481 | 1 | 1366.071 | 0.019 | |
| Time points | 16.902 | 1 | - | <0.001 | ||
| mTBI: Time points | 0.653 | 1 | - | 0.448 | ||
| PHQ-9 | mTBI | 2.632 | 1 | 1386.136 | 0.114 | |
| Time points | 9.075 | 1 | - | 0.005 | ||
| mTBI: Time points | 0.032 | 1 | - | 0.848 | ||
| GAD-7 | mTBI | 3.216 | 1 | 1425.187 | 0.073 | |
| Time points | 3.137 | 1 | - | 0.077 | ||
| mTBI: Time points | 0.026 | 1 | - | 0.872 | ||
| QOLIBRI | mTBI | 12.25 | 1 | 1337.174 | <0.001 | |
| Time points | 8.588 | 1 | - | 0.003 | ||
| mTBI: Time points | 2.980 | 1 | - | 0.084 | ||
| GOSE | mTBI | 80.944 | 1 | 1444.067 | <0.001 | |
| Time points | 26.15 | 1 | - | <0.001 | ||
| mTBI: Time points | 1.057 | 1 | - | 0.304 |
| Outcome | mTBI | Time Points | Interaction |
|---|---|---|---|
| SF-36 PCS | -- | ++ | -- |
| SF-36 MCS | ++ | ++ | -- |
| PCL-5 | -- | ++ | -- |
| PHQ-9 | -- | ++ | -- |
| GAD-7 | -- | -- | -- |
| QOLIBRI | ++ | ++ | -- |
| GOSE | ++ | ++ | -- |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Voormolen, D.C.; Zeldovich, M.; Haagsma, J.A.; Polinder, S.; Friedrich, S.; Maas, A.I.R.; Wilson, L.; Steyerberg, E.W.; Covic, A.; Andelic, N.; et al. Outcomes after Complicated and Uncomplicated Mild Traumatic Brain Injury at Three-and Six-Months Post-Injury: Results from the CENTER-TBI Study. J. Clin. Med. 2020, 9, 1525. https://doi.org/10.3390/jcm9051525
Voormolen DC, Zeldovich M, Haagsma JA, Polinder S, Friedrich S, Maas AIR, Wilson L, Steyerberg EW, Covic A, Andelic N, et al. Outcomes after Complicated and Uncomplicated Mild Traumatic Brain Injury at Three-and Six-Months Post-Injury: Results from the CENTER-TBI Study. Journal of Clinical Medicine. 2020; 9(5):1525. https://doi.org/10.3390/jcm9051525
Chicago/Turabian StyleVoormolen, Daphne C., Marina Zeldovich, Juanita A. Haagsma, Suzanne Polinder, Sarah Friedrich, Andrew I. R. Maas, Lindsay Wilson, Ewout W. Steyerberg, Amra Covic, Nada Andelic, and et al. 2020. "Outcomes after Complicated and Uncomplicated Mild Traumatic Brain Injury at Three-and Six-Months Post-Injury: Results from the CENTER-TBI Study" Journal of Clinical Medicine 9, no. 5: 1525. https://doi.org/10.3390/jcm9051525
APA StyleVoormolen, D. C., Zeldovich, M., Haagsma, J. A., Polinder, S., Friedrich, S., Maas, A. I. R., Wilson, L., Steyerberg, E. W., Covic, A., Andelic, N., Plass, A. M., Wu, Y.-J., Asendorf, T., von Steinbüechel, N., & Participants Investigators, C.-T. (2020). Outcomes after Complicated and Uncomplicated Mild Traumatic Brain Injury at Three-and Six-Months Post-Injury: Results from the CENTER-TBI Study. Journal of Clinical Medicine, 9(5), 1525. https://doi.org/10.3390/jcm9051525