Intensive Motion Style Acupuncture Treatment (MSAT) Is Effective for Patients with Acute Whiplash Injury: A Randomized Controlled Trial

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design
2.2. Participants
2.2.1. Inclusion Criteria
2.2.2. Exclusion Criteria
2.3. Randomization and Allocation Concealment
2.4. Blinding
2.5. Sample Size
2.6. Interventions
2.6.1. Control Group: Integrative Korean Medicine Treatment
2.6.2. Motion Style Acupuncture Treatment Group: Integrative Korean Medicine and Trapezius Motion Style Acupuncture treatments
2.7. Outcomes
2.7.1. Primary Outcome
2.7.2. Secondary Outcomes
- Visual Analog Scale
- Neck Disability Index
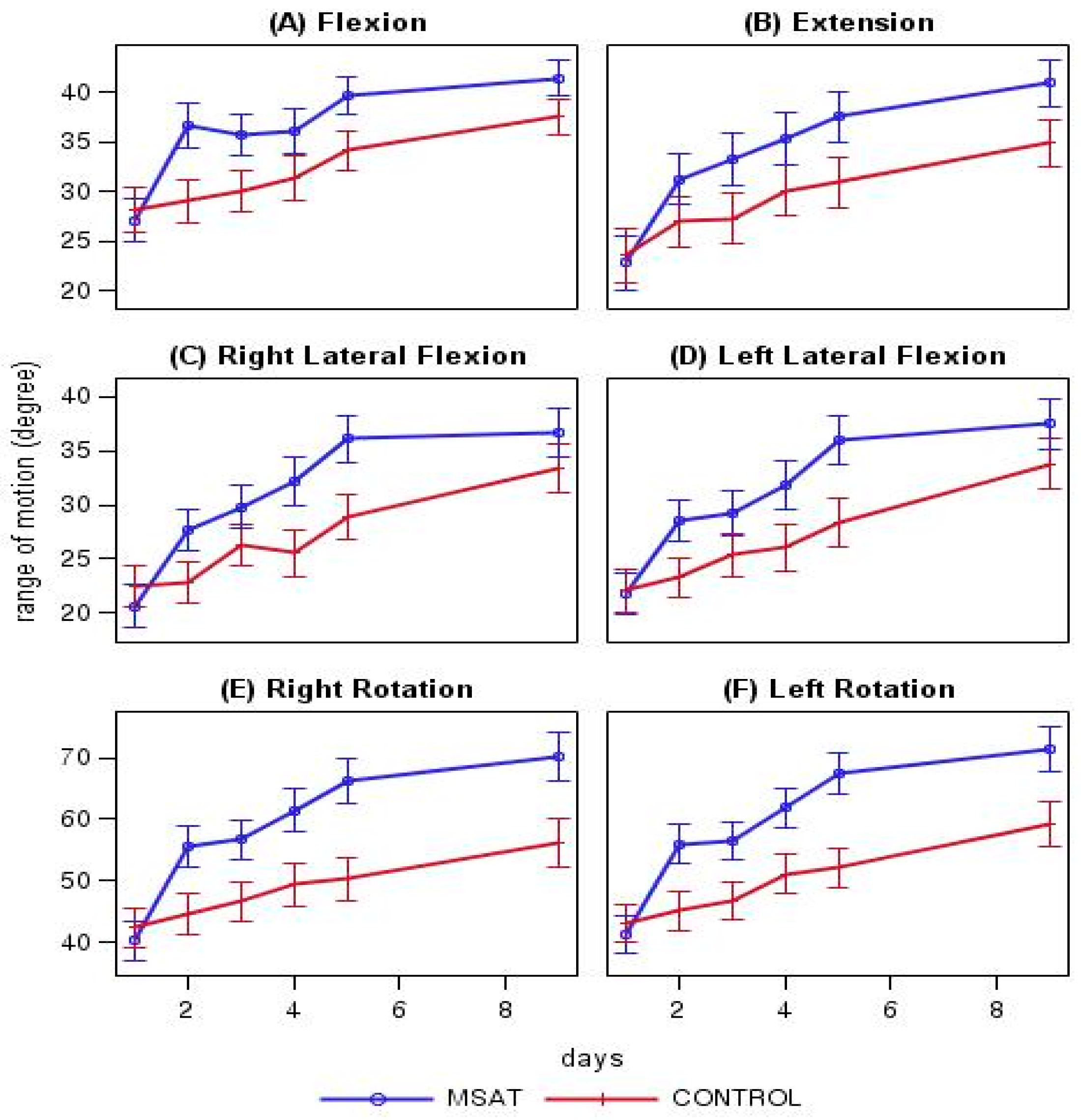
- Cervical Range of Motion
- Quality of Life
- Patient Global Impression of Change
- Adverse Events
2.8. Statistical Analysis
2.9. Data Availability
3. Results
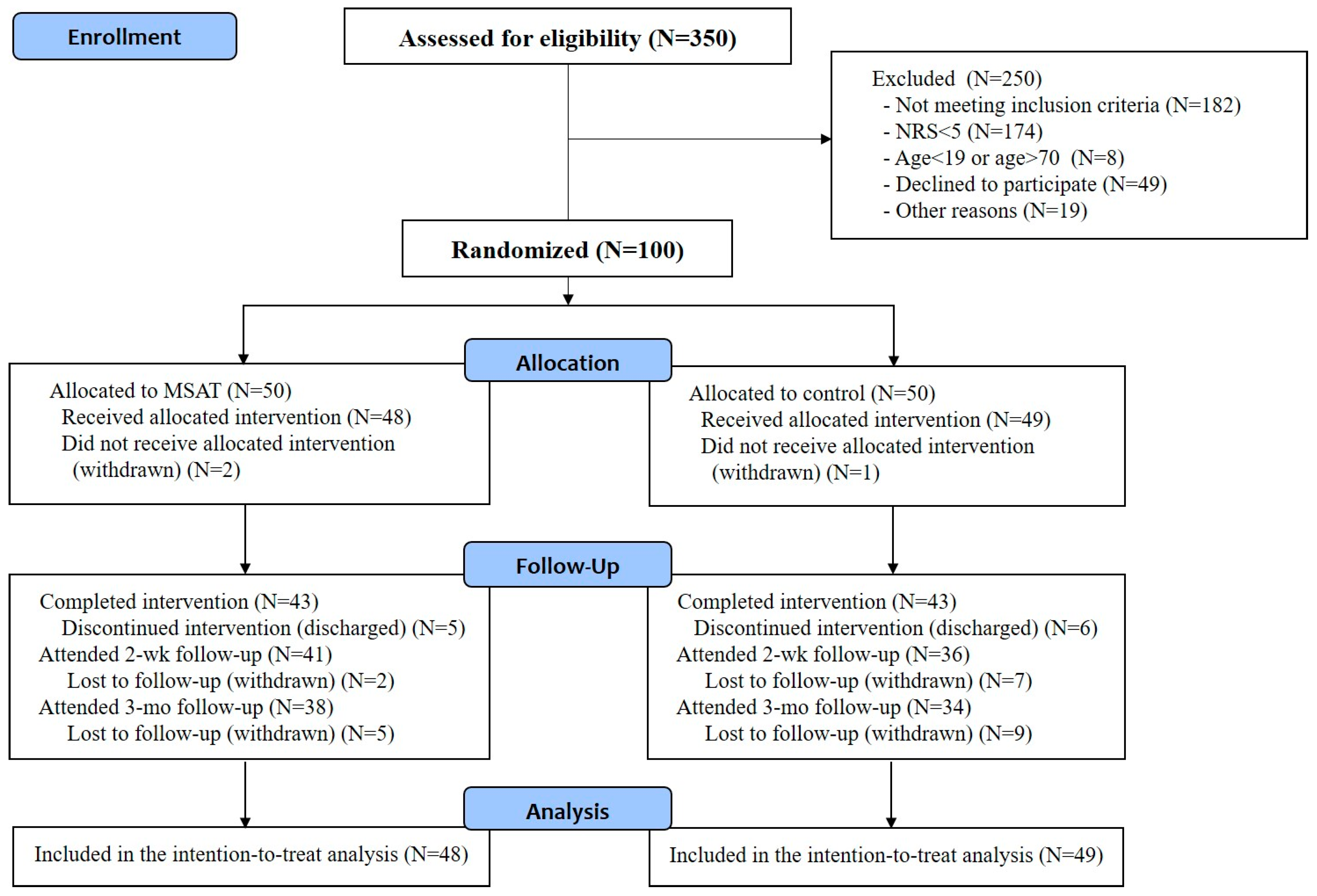
3.1. Participants
3.2. Baseline Characteristics
3.3. Outcome Comparison between the Two Groups
3.4. Outcome Changes in Each Group
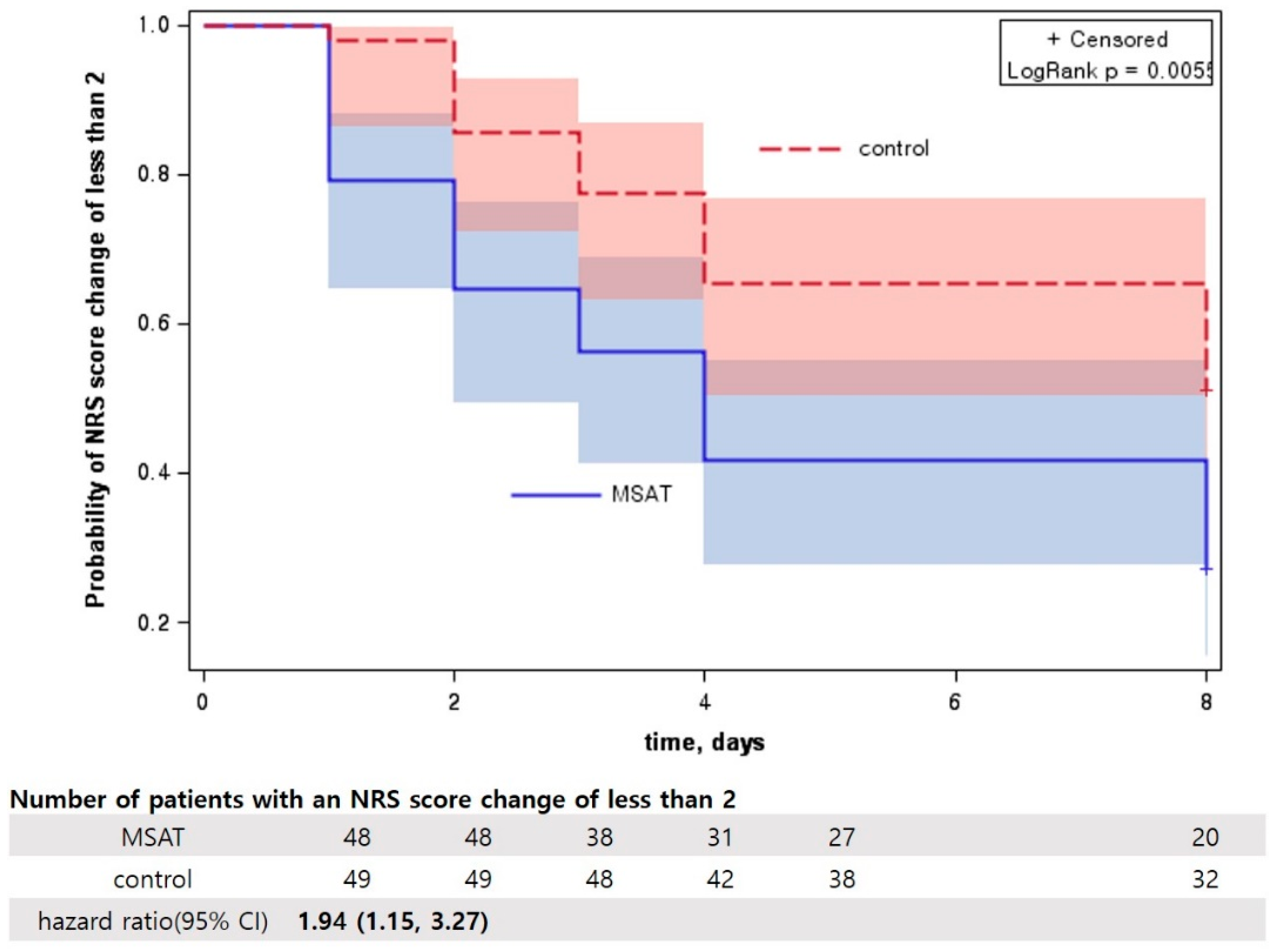
3.5. Survival Analysis of Neck Pain NRS Score Reduction
3.6. Adverse Events
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Spitzer, W.O.; Skovron, M.L.; Salmi, L.R.; Cassidy, J.D.; Duranceau, J.; Suissa, S.; Zeiss, E. Scientific monograph of the Quebec Task Force on Whiplash-Associated Disorders: Redefining “whiplash” and its management. Spine 1995, 20, 1S–73S. [Google Scholar] [PubMed]
- Cassidy, J.D.; Carroll, L.J.; Côté, P.; Lemstra, M.; Berglund, A.; Nygren, Å. Effect of eliminating compensation for pain and suffering on the outcome of insurance claims for whiplash injury. N. Engl. J. Med. 2000, 342, 1179–1186. [Google Scholar] [CrossRef] [PubMed]
- Sterling, M.; Kenardy, J. Whiplash: Evidence Base for Clinical Practice; Elsevier: Chatswood, Australia, 2011. [Google Scholar]
- Treleaven, J. Dizziness, unsteadiness, visual disturbances, and postural control: Implications for the transition to chronic symptoms after a whiplash trauma. Spine 2011, 36, S211–S217. [Google Scholar] [CrossRef]
- Guzman, J.; Hurwitz, E.L.; Carroll, L.J.; Haldeman, S.; Côté, P.; Carragee, E.J.; Peloso, P.M.; van der Velde, G.; Holm, L.W.; Hogg-Johnson, S.; et al. A new conceptual model of neck pain: Linking onset, course, and care: The Bone and Joint Decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders. J. Manip. Physiol. Ther. 2009, 32, S17–S28. [Google Scholar] [CrossRef] [PubMed]
- Hogg-Johnson, S.; van Der Velde, G.; Carroll, L.J.; Holm, L.W.; Cassidy, J.D.; Guzman, J.; Côté, P.; Haldeman, S.; Ammendolia, C.; Carragee, E.; et al. The burden and determinants of neck pain in the general population: Results of the Bone and Joint Decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders. Eur. Spine J. 2008, 17, 39–51. [Google Scholar] [CrossRef] [Green Version]
- Statistical Data Set. Accident and Casualty Costs (RAS60). Data about the Accident and Casualty Costs, Produced by Department for Transport. RAS 60003: Total Value of Prevention of Reported Accidents by Severity and Cost Element: GB 2018. Available online: https://www.gov.uk/government/statistical-data-sets/ras60-average-value-of-preventing-road-accidents (accessed on 10 January 2020).
- Rushton, A.; Wright, C.; Heneghan, N.; Eveleigh, G.; Calvert, M.; Freemantle, N. Physiotherapy rehabilitation for whiplash associated disorder II: A systematic review and meta-analysis of randomised controlled trials. BMJ. Open. 2011, 1, e000265. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.T.; Hwang, E.H.; Heo, I.; Cho, J.H.; Kim, K.W.; Ha, I.N.; Kim, M.R.; Kang, H.W.; Lee, J.H.; Shin, B.C. Clinical practice guidelines for the use of traditional Korean medicine in the treatment of patients with traffic-related injuries: An evidence-based approach. Eur. J. Integr. Med. 2018, 18, 34–41. [Google Scholar] [CrossRef]
- Health Insurance Review & Assessment Service. Available online: http://www.hira.or.kr./bbsDummy.do?pgmid=HIRAA020041000100&brdScnBltNo=4&brdBltNo=9411 (accessed on 11 January 2020).
- Korean Ministry of Health & Welfare; Press Release. “Statistics Information for Auto Insurance Fees” Will Be Released for the First Time! Available online: http://www.mohw.go.kr/front_new/al/sal0301vw.jsp?PAR_MENU_ID=04&MENU_ID=0403&CONT_SEQ=340291&page=1 (accessed on 11 January 2020).
- Cameron, I.D.; Wang, E.; Sindhusake, D. A randomized trial comparing acupuncture and simulated acupuncture for subacute and chronic whiplash. Spine 2011, 36, E1659–E1665. [Google Scholar] [CrossRef] [Green Version]
- Kwak, H.Y.; Kim, J.I.; Park, J.M.; Lee, S.H.; Yu, H.S.; Lee, J.D.; Cho, K.H.; Katai, S.; Tsukayama, H.; Kimura, T.; et al. Acupuncture for whiplash-associated disorder: A randomized, waiting-list controlled, pilot trial. Eur. J. Integr. Med. 2012, 4, e151–e158. [Google Scholar] [CrossRef]
- Tobbackx, Y.; Meeus, M.; Wauters, L.; De Vilder, P.; Roose, J.; Verhaeghe, T.; Nijs, J. Does acupuncture activate endogenous analgesia in chronic whiplash-associated disorders? A randomized crossover trial. Eur. J. Pain 2013, 17, 279–289. [Google Scholar] [CrossRef]
- Do, H.J.; Shin, Y.S.; Kim, C.E.; Song, H.S.; Shin, J.K.; Gang, B.G.; Koh, W.I.; Jeon, S.H.; Cho, Y.K.; Kim, E.S. Clinical Analysis of 2048 Musculoskeletal Patients Who Visited the Traffic Accident Clinic of a Korean Medicine Hospital. J. Korea CHUNA Man. Med. Spine Nerves 2016, 11, 11–23. [Google Scholar]
- Choi, B.; Oh, M. Two cases report of supraspinatus tendon tear treated with the daoyin exercise program combined with Korean medicine treatment. J. Haehwa Med. 2016, 25, 27–36. [Google Scholar]
- Hwang, E.H.; Kwon, Y.K.; Heo, K.H.; Cho, H.W.; Lee, H.Y.; Sung, W.Y. Comparative review of qigong and daoyin as a therapeutic exercise of traditional Korean medicine. J. Physiol. Pathol. Korean Med. 2013, 27, 594–601. [Google Scholar]
- Lee, S.H.; Lee, J.; Lee, Y.J.; Kim, M.R.; Cho, J.H.; Kim, K.W.; Ha, I.H. Effectiveness and cost-effectiveness of acupuncture with Doin therapy for chronic neck pain: A study protocol for a multicentre, randomised controlled clinical trial. BMJ. Open. 2019, 9, e026632. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.S.; Boone, W.; Kim, P.; So, C. Acute and long term benefits of motion style treatment (MST): Two case reports. Int. J. Clin. Acupunct. 2007, 16, 85. [Google Scholar]
- Chen, D. Introduction to “motion acupuncture” and target points. Zhongguo Zhen Jiu 2016, 36, 941–944. [Google Scholar] [CrossRef]
- Chen, D.; Yang, G.; Wang, F.; Qi, W. Motion acupuncture for therapeutic target. Zhongguo Zhen Jiu 2016, 36, 1177–1180. [Google Scholar] [CrossRef]
- Shin, J.S.; Ha, I.H.; Lee, J.; Choi, Y.; Kim, M.R.; Park, B.Y.; Shin, B.C.; Lee, M.S. Effects of motion style acupuncture treatment in acute low back pain patients with severe disability: A multicenter, randomized, controlled, comparative effectiveness trial. Pain 2013, 154, 1030–1037. [Google Scholar] [CrossRef] [Green Version]
- Suresh, K. An overview of randomization techniques: An unbiased assessment of outcome in clinical research. J. Human. Reprod. Sci. 2011, 4, 8–11. [Google Scholar] [CrossRef]
- Kim, J.; Shin, W. How to do random allocation (randomization). Clin. Orthop. Surg. 2014, 6, 103–109. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.H.; Cho, Y.Y.; Kim, S.; Sun, S.H. History of research on pharmacopuncture in Korea. J. Pharmacopunct. 2016, 19, 101. [Google Scholar]
- Hawker, G.A.; Mian, S.; Kendzerska, T.; French, M. Measures of adult pain: Visual analog scale for pain (vas pain), numeric rating scale for pain (nrs pain), mcgill pain questionnaire (mpq), short-form mcgill pain questionnaire (sf-mpq), chronic pain grade scale (cpgs), short form-36 bodily pain scale (sf-36 bps), and measure of intermittent and constant osteoarthritis pain (icoap). Arthritis. Care Res. (Hoboken) 2011, 63, S240–S252. [Google Scholar] [CrossRef] [PubMed]
- Solodiuk, J.C.; Scott-Sutherland, J.; Meyers, M.; Myette, B.; Shusterman, C.; Karian, V.E.; Harris, S.K.; Curley, M.A.Q. Validation of the individualized numeric rating scale (INRS): A pain assessment tool for nonverbal children with intellectual disability. Pain 2010, 150, 231–236. [Google Scholar] [CrossRef]
- De Leon, S.P.; Lara-Muñoz, C.; Feinstein, A.R.; Wells, C.K. A comparison of three rating scales for measuring subjective phenomena in clinical research: II. Use of experimentally controlled visual stimuli. Arch. Med. Res. 2004, 35, 157–162. [Google Scholar] [CrossRef]
- Song, K.J.; Choi, B.W.; Kim, S.J.; Yoon, S.J. Cross-cultural adaptation and validation of the Korean version of the neck disability index. J. Korean Orthop. Assoc. 2009, 44, 350–359. [Google Scholar] [CrossRef]
- Kim, S.H.; Ahn, J.; Ock, M.; Shin, S.; Park, J.; Luo, N.; Jo, M.W. The EQ-5D-5L valuation study in Korea. Qual. Life Res. 2016, 25, 1845–1852. [Google Scholar] [CrossRef] [PubMed]
- Dworkin, R.H.; Turk, D.C.; Farrar, J.T.; Haythornthwaite, J.A.; Jensen, M.P.; Katz, N.P.; Kerns, R.D.; Stucki, G.; Allen, R.R.; Bellamy, N.; et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain 2005, 113, 9–19. [Google Scholar] [CrossRef] [PubMed]
- Son, M.K.; Lee, Y.W.; Jung, H.Y.; Yi, S.W.; Lee, K.H.; Kim, S.U.; Jeong, J.H.; Park, J.J.; Park, J.W.; Hong, C.S. Comparison of the Naranjo and WHO-Uppsala Monitoring Centre criteria for causality assessment of adverse drug reactions. Korean J. Med. 2008, 74, 181–187. [Google Scholar]
- Chung, A.S.; Copay, A.G.; Olmscheid, N.; Campbell, D.; Walker, J.B.; Chutkan, N. Minimum clinically important difference: Current trends in the spine literature. Spine 2017, 42, 1096–1105. [Google Scholar] [CrossRef]
- Han, K.I.; Jeon, Y.T.; Sin, S.H.; Lee, J.H.; Ko, Y.S. The Retrospective Comparative Study on the Effect of Muscle Relaxation Pharmacopuncture and Chuna Manual Therapy for Neck Pain caused by Traffic Accidents. J. Korea Chuna Man. Med. Spine Nerves 2016, 11, 25–32. [Google Scholar]
- Kim, T.G.; Seo, Y.W.; Kim, Y.J.; Lee, J.R.; Choi, J.Y.; Kim, J.S.; Kim, S.Y.; Park, H.S.; Jeon, E.J.; Kim, K.O. A Comparative Study of Improvement of Neck Pain According to Hospitalization Period in Patients of Neck pain Caused by Traffic Accident. Acupuncture 2016, 33, 186–195. [Google Scholar] [CrossRef]
- Park, J.; Kim, H.J.; Kim, G.B.; Kwon, Y.S.; Lee, H.W.; Yu, J.E.; Choi, G.C. Clinical Effects of Combination of Korean Medicine Admission Treatment in Patients with Sternum Fracture after Traffic Accidents: 5 Case Series Report. J. Korea Chuna Man. Med. Spine Nerves 2019, 14, 101–111. [Google Scholar] [CrossRef]
- National Clearinghouse for Korean Medicine. Available online: http://www.nckm.or.kr/main/index.do (accessed on 23 June 2020).
- Sieben, J.M.; Vlaeyen, J.W.S.; Tuerlinckx, S.; Portegijs, P.J.M. Pain-related fear in acute low back pain: The first two weeks of a new episode. Eur. J. Pain 2002, 6, 229–237. [Google Scholar] [CrossRef]
- Turk, D.C.; Wilson, H.D. Fear of pain as a prognostic factor in chronic pain: Conceptual models, assessment, and treatment implications. Curr. Pain Headache R. 2010, 14, 88–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, J.E.; Von Korff, M.; Cherkin, D.; Saunders, K.; Lorig, K. A randomized trial of a cognitive-behavioral program for enhancing back pain self care in a primary care setting. Pain 2000, 88, 145–153. [Google Scholar] [CrossRef]
- Vlaeyen, J.W.; de Jong, J.; Geilen, M.; Heuts, P.H.; van Breukelen, G. Graded exposure in vivo in the treatment of pain-related fear: A replicated single-case experimental design in four patients with chronic low back pain. Behav. Res. Ther. 2001, 39, 151–166. [Google Scholar] [CrossRef]
- Yang, X.Y.; Shi, G.X.; Li, Q.Q.; Zhang, Z.H.; Xu, Q.; Liu, C.-Z. Characterization of deqi sensation and acupuncture effect. Evid.-Based Complement. Altern. Med. 2013, 1–7. [Google Scholar]
- Salih, N.; Bäumler, P.I.; Simang, M.; Irnich, D. Deqi sensations without cutaneous sensory input: Results of an RCT. BMC Complement. Altern. Med. 2010, 10, 81. [Google Scholar] [CrossRef] [Green Version]
- Filshie, J.; White, A.; Cummings, M. Medical Acupuncture: A Western Scientific Approach, 2nd ed.; Elsevier Ltd.: London, UK, 2016. [Google Scholar]
- Lin, R.; Zhu, N.; Liu, J.; Li, X.; Wang, Y.; Zhang, J.; Xi, C. Acupuncture-movement therapy for acute lumbar sprain: A randomized controlled clinical trial. J. Tradit. Chin. Med. 2016, 36, 19–25. [Google Scholar] [CrossRef] [Green Version]
- Luo, B.H.; Han, J.X. Cervical spondylosis treated by acupuncture at Ligou (LR 5) combined with movement therapy. J. Tradit. Chin. Med. 2010, 30, 113–117. [Google Scholar] [CrossRef] [Green Version]
- Loudon, K.; Treweek, S.; Sullivan, F.; Donnan, P.; Thorpe, K.E.; Zwarenstein, M. The PRECIS-2 tool: Designing trials that are fit for purpose. BMJ 2015, 350, h2147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lombard, C.; Treweek, S.; Maclure, M.; Zwarenstein, M. Why we will remain pragmatists: Four problems with the impractical mechanistic framework and a better solution. J. Clin. Epidemiol. 2009, 62, e485–e488. [Google Scholar]
- Rothwell, P.M. External validity of randomised controlled trials:”to whom do the results of this trial apply?”. Lancet 2005, 365, 82–93. [Google Scholar] [CrossRef]
- Herrmann, D.B. Validity study of head and neck flexion-extension motion comparing measurements of a pendulum goniometer and roentgenograms. J. Orthop. Sport Phys. 1990, 11, 414–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pellecchia, G.; Bohannon, R. Active lateral neck flexion range of motion measurements obtained with a modified goniometer: Reliability and estimates of normal. J. Manip. Physiol. Ther. 1998, 21, 443–447. [Google Scholar]
- Elahee, S.F.; Mao, H.-J.; Ling, Z.; Shen, X.-Y. Meridian system and mechanism of acupuncture action: A scientific evaluation. World J. Acupunct. Moxibustion 2020. [Google Scholar]
- Longhurst, J.C. Defining meridians: A modern basis of understanding. J. Acupunct. Meridian Stud. 2010, 3, 67–74. [Google Scholar] [CrossRef] [Green Version]
- Qu, J. Acupuncture mechanism, applications, and future development. Chin. Med. Cult. 2020, 3, 33. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| MSAT Group (n = 48) | Control Group (n = 49) | ||
|---|---|---|---|
| Sex, n (%) | Female | 23 (52.1) | 19 (61.2) |
| Male | 25 (47.9) | 30 (38.8) | |
| Age (years) | 41.35 ± 12.62 | 42.63 ± 12.96 | |
| Length of stay (days) | 8.73 ± 3.84 | 8.41 ± 3.91 | |
| Height (cm) | 167.9 ± 8.97 | 167.92 ± 9.6 | |
| Bodyweight (kg) | 68.73 ± 13.73 | 66.49 ± 12.12 | |
| BMI (kg/m2) | 24.21 ± 3.34 | 23.44 ± 2.97 | |
| Alcohol use, n (%) | No | 21 (43.7) | 25 (51) |
| Yes | 27 (56.3) | 24 (49) | |
| Smoking, n (%) | No | 29 (60.4) | 30 (61.2) |
| Yes | 19 (39.6) | 19 (38.8) | |
| NRS score for neck pain | 5.67 ± 1.17 | 5.44 ± 1.31 |
| Baseline | Day2 | Day5 | Discharge 1 | 90 Days f/u | |
|---|---|---|---|---|---|
| NRS score for neck pain | |||||
| MSAT | 5.67 (5.33, 6.01) | 4.80 (4.39, 5.21) | 3.55 (3.04, 4.06) | 3.30 (2.78, 3.83) | 1.41 (0.80, 2.01) |
| Control | 5.44 (5.06, 5.82) | 5.36 (4.98, 5.73) | 4.59 (4.10, 5.07) | 3.60 (2.95, 4.25) | 1.05 (0.43, 1.67) |
| Difference 2 | — | −0.76 (−1.15, −0.38) | −1.07 (−1.76, −0.37) | −0.34 (−1.19, 0.51) | 0.23 (−0.67, 1.14) |
| p-value 3 | — | 0.0002 | 0.003 | 0.427 | 0.611 |
| NRS score for arm pain | |||||
| MSAT | 2.82 (2.04, 3.60) | 2.51 (1.87, 3.15) | 2.13 (1.55, 2.71) | 1.39 (0.70, 2.09) | 0.66 (0.05, 1.27) |
| Control | 3.61 (2.91, 4.31) | 3.40 (2.72, 4.08) | 2.70 (2.03, 3.38) | 2.49 (1.76, 3.23) | 0.30 (−0.26, 0.86) |
| Difference 2 | — | −0.23 (−0.60, 0.14) | 0.01 (−0.66, 0.69) | −0.66 (−1.55, 0.22) | 0.53 (−0.23, 1.28) |
| p-value 3 | — | 0.2247 | 0.971 | 0.142 | 0.174 |
| VAS score for neck pain | |||||
| MSAT | 5.74 (5.37, 6.12) | 4.79 (4.31, 5.26) | 3.64 (3.12, 4.17) | 3.35 (2.78, 3.93) | — |
| Control | 5.53 (5.13, 5.93) | 5.31 (4.92, 5.71) | 4.58 (4.09, 5.07) | 3.56 (2.78, 4.33) | — |
| Difference 2 | — | −0.66 (−1.13, −0.20) | −0.96 (−1.65, −0.26) | −0.34 (−1.19, 0.51) | — |
| p-value 3 | — | 0.0054 | 0.007 | 0.427 | — |
| VAS score for arm pain | |||||
| MSAT | 2.80 (2.02, 3.58) | 2.49 (1.83, 3.16) | 2.15 (1.55, 2.75) | 1.46 (0.79, 2.13) | — |
| Control | 3.62 (2.91, 4.34) | 3.45 (2.76, 4.14) | 2.84 (2.17, 3.50) | 2.31 (1.54, 3.07) | — |
| Difference 2 | — | −0.24 (−0.64, 0.17) | −0.05 (−0.71, 0.62) | −0.42 (−1.32, 0.48) | — |
| p-value 3 | — | 0.2501 | 0.890 | 0.359 | — |
| NDI | |||||
| MSAT | 40.94 (36.91, 44.97) | — | 30.18 (25.87, 34.49) | 27.89 (23.10, 32.68) | 7.76 (3.90, 11.61) |
| Control | 41.57 (37.94, 45.19) | — | 32.61 (27.88, 37.33) | 29.01 (23.83, 34.19) | 4.26 (0.14, 8.37) |
| Difference 2 | — | — | −2.21 (−8.22, 3.80) | −1.47 (−8.57, 5.62) | 3.40 (−2.02, 8.83) |
| p-value 3 | — | — | 0.470 | 0.684 | 0.218 |
| ROM for flexion | |||||
| MSAT | 27.08 (24.26, 29.91) | 36.67 (34.12, 39.21) | 39.70 (37.14, 42.27) | 41.22 (38.76, 43.68) | — |
| Control | 28.16 (25.63, 30.70) | 29.08 (26.37, 31.80) | 34.34 (31.43, 37.26) | 37.75 (35.28, 40.21) | — |
| Difference 2 | — | 8.50 (5.89, 11.11) | 5.87 (2.09, 9.66) | 3.66 (−0.01, 7.33) | — |
| p-value 3 | — | <0.0001 | 0.002 | 0.050 | — |
| ROM for extension | |||||
| MSAT | 22.81 (19.24, 26.38) | 31.25 (28.14, 34.36) | 38.16 (34.92, 41.41) | 40.81 (38.30, 43.32) | — |
| Control | 23.57 (20.52, 26.62) | 26.94 (23.92, 29.95) | 30.68 (27.00, 34.37) | 35.22 (31.89, 38.55) | — |
| Difference 2 | — | 4.64 (1.40, 7.89) | 7.42 (2.42, 12.42) | 5.40 (1.11, 9.69) | — |
| p-value 3 | — | 0.0055 | 0.004 | 0.014 | — |
| ROM for right rotation | |||||
| MSAT | 40.21 (36.12, 44.29) | 55.63 (51.28, 59.97) | 66.69 (61.86, 71.51) | 70.57 (65.56, 75.59) | — |
| Control | 42.45 (38.76, 46.14) | 44.69 (40.82, 48.57) | 51.28 (46.00, 56.56) | 57.55 (51.27, 63.83) | — |
| Difference 2 | — | 12.42 (8.33, 16.52) | 16.14 (8.71, 23.57) | 13.29 (4.60, 21.98) | — |
| p-value 3 | — | <0.0001 | 0.000 | 0.003 | — |
| ROM for left rotation | |||||
| MSAT | 41.25 (37.73, 44.77) | 55.94 (51.86, 60.02) | 67.62 (63.03, 72.21) | 71.41 (66.34, 76.48) | — |
| Control | 43.16 (39.34, 46.98) | 45.10 (41.40, 48.80) | 52.58 (47.99, 57.16) | 59.87 (54.49, 65.25) | — |
| Difference 2 | — | 12.13 (8.38, 15.87) | 15.94 (9.21, 22.68) | 11.80 (4.13, 19.47) | — |
| p-value 3 | — | <0.0001 | 0.000 | 0.003 | — |
| ROM for right lateral flexion | |||||
| MSAT | 20.63 (18.14, 23.11) | 27.60 (25.27, 29.94) | 36.20 (33.14, 39.27) | 36.76 (33.27, 40.25) | — |
| Control | 22.45 (20.14, 24.76) | 22.86 (20.57, 25.15) | 28.74 (25.81, 31.67) | 33.54 (30.55, 36.54) | — |
| Difference 2 | — | 5.80 (3.50, 8.11) | 7.49 (3.15, 11.82) | 3.03 (−1.85, 7.92) | — |
| p-value 3 | — | <0.0001 | 0.001 | 0.222 | — |
| ROM for left lateral flexion | |||||
| MSAT | 21.77 (19.24, 24.30) | 28.54 (26.24, 30.84) | 36.36 (33.25, 39.46) | 37.59 (34.44, 40.75) | — |
| Control | 22.04 (19.81, 24.27) | 23.27 (21.12, 25.41) | 28.37 (25.35, 31.39) | 33.67 (30.47, 36.87) | — |
| Difference 2 | — | 5.16 (3.02, 7.30) | 7.90 (3.52, 12.28) | 3.63 (−1.08, 8.34) | — |
| p-value 3 | — | <0.0001 | 0.000 | 0.130 | — |
| EQ5D | |||||
| MSAT | 0.67 (0.63, 0.72) | — | 0.73 (0.69, 0.77) | 0.75 (0.71, 0.78) | 0.88 (0.85, 0.91) |
| Control | 0.67 (0.63, 0.72) | — | 0.73 (0.69, 0.77) | 0.74 (0.70, 0.78) | 0.88 (0.84, 0.92) |
| Difference 2 | — | — | 0.00 (−0.05, 0.05) | 0.00 (−0.04, 0.05) | 0.00 (−0.04, 0.05) |
| p-value 3 | — | — | 0.991 | 0.872 | 0.846 |
| PGIC | |||||
| MSAT | — | — | 2.72 (2.44, 3.00) | 2.38 (2.11, 2.65) | 1.49 (1.21, 1.77) |
| Control | — | — | 3.23 (2.96, 3.50) | 2.65 (2.34, 2.97) | 1.14 (0.82, 1.47) |
| Difference 2 | — | — | −0.48 (−0.87, −0.10) | −0.24 (−0.67, 0.20) | 0.36 (−0.07, 0.79) |
| p-value 3 | — | — | 0.014 | 0.284 | 0.097 |
| Day 2 | Day 5 | Discharge | 90 Days f/u | |
|---|---|---|---|---|
| NRS score for neck pain | ||||
| MSAT 1 | 0.86 (0.64, 1.09) | 2.18 (1.76, 2.60) | 2.34 (1.89, 2.79) | 4.15 (3.73, 4.57) |
| Control 1 | 0.08 (−0.15, 0.31) | 1.40 (0.98, 1.82) | 1.86 (1.41, 2.31) | 4.02 (3.59, 4.45) |
| Group*days 2 | −0.56 (−1.01, −0.10) | −1.05 (−1.57, −0.53) | −0.25 (−0.86, 0.35) | 0.10 (−0.42, 0.61) |
| p-value | 0.047 * | 0.001 * | 0.4896 | 0.755 |
| NRS score for arm pain | ||||
| MSAT 1 | 0.31 (0.07, 0.55) | 0.82 (0.28, 1.36) | 1.36 (0.83, 1.90) | 1.91 (1.33, 2.49) |
| Control 1 | 0.21 (−0.02, 0.45) | 0.52 (−0.03, 1.07) | 1.10 (0.57, 1.63) | 2.78 (2.18, 3.37) |
| Group*days 2 | −0.89 (−1.66, −0.12) | −0.81 (−1.49, −0.12) | −1.05 (−1.74, −0.36) | 0.07 (−0.49, 0.63) |
| p-value | 0.059 | 0.054 | 0.0134 * | 0.825 |
| VAS score for neck pain | ||||
| MSAT 1 | 0.96 (0.68, 1.23) | 2.03 (1.65, 2.41) | 2.32 (1.82, 2.82) | — |
| Control 1 | 0.21 (−0.06, 0.49) | 0.88 (0.50, 1.25) | 1.93 (1.43, 2.43) | — |
| Group*days 2 | −0.53 (−1.04, −0.02) | −0.94 (−1.49, −0.39) | −0.17 (−0.86, 0.51) | — |
| p-value | 0.088 | 0.005 * | 0.676 | — |
| VAS score for arm pain | ||||
| MSAT 1 | 0.30 (0.05, 0.56) | 0.65 (0.26, 1.05) | 1.33 (0.81, 1.86) | — |
| Control 1 | 0.18 (−0.08, 0.43) | 0.62 (0.23, 1.01) | 1.22 (0.70, 1.75) | — |
| Group*days 2 | −0.96 (−1.74, −0.17) | −0.86 (−1.56, −0.15) | −0.94 (−1.64, −0.24) | — |
| p-value | 0.047 * | 0.046 * | 0.029 * | — |
| NDI | ||||
| MSAT 1 | — | 5.16 (3.73, 6.59) | 6.17 (4.29, 8.04) | 16.16 (14.24, 18.07) |
| Control 1 | — | 3.66 (2.24, 5.08) | 7.57 (4.38, 10.76) | 7.57 (4.38, 10.76) |
| Group*days 2 | — | −1.72 (−3.92, 0.48) | −0.17 (−2.49, 2.14) | 1.11 (−0.60, 2.82) |
| p-value | — | 0.197 | 0.901 | 0.284 |
| ROM of flexion | ||||
| MSAT 1 | −9.58 (−11.21, −7.96) | −12.63 (−14.95, −10.31) | −14.35 (−16.74, −11.96) | — |
| Control 1 | −0.92 (−2.53, 0.69) | −6.00 (−8.29, −3.70) | −9.37 (−11.74, −7.00) | — |
| Group*days 2 | 7.59 (4.51, 10.66) | 5.55 (2.80, 8.31) | 3.90 (1.39, 6.41) | — |
| p-value | 0.000 * | 0.001 * | 0.011 * | — |
| ROM of extension | ||||
| MSAT1 | −8.44 (−10.56, −6.32) | −14.77 (−17.84, −11.69) | −18.14 (−21.29, −14.98) | — |
| Control 1 | −3.37 (−5.47, −1.27) | −7.41 (−10.44, −4.37) | −11.45 (−14.58, −8.32) | — |
| Group*days 2 | 4.31 (0.74, 7.89) | 6.60 (2.97, 10.23) | 5.93 (2.60, 9.26) | — |
| p-value | 0.048 * | 0.003 * | 0.004 * | — |
| ROM for right rotation | ||||
| MSAT 1 | −15.42 (−17.94, −12.90) | −26.07 (−29.61, −22.53) | −29.93 (−34.14, −25.73) | — |
| Control 1 | −2.24 (−4.74,0.25) | −7.85 (−11.36, −4.35) | −13.77 (−17.95, −9.58) | — |
| Group*days 2 | 10.93 (6.13,15.73) | 15.98 (10.91, 21.04) | 13.93 (8.28, 19.57) | — |
| p-value | <0.001 * | <0.001 * | <0.001 * | — |
| ROM for left rotation | ||||
| MSAT 1 | −14.69 (−16.92, −12.45) | −26.08 (−29.45, −22.70) | −30.16 (−34.10, −26.23) | — |
| Control 1 | −1.94 (−4.15, 0.27) | −8.91 (−12.25, −5.56) | −15.97 (−19.89, −12.06) | — |
| Group*days 2 | 10.84 (6.29, 15.38) | 15.26 (10.60, 19.91) | 12.28 (7.13, 17.42) | — |
| p-value | <0.001 * | <0.001 * | <0.001 * | — |
| ROM for right lateral flexion | ||||
| MSAT 1 | −6.98 (−8.44, −5.52) | −15.48 (−18.01, −12.96) | −16.06 (−18.65, −13.47) | — |
| Control 1 | −0.41 (−1.85, 1.04) | −6.38 (−8.87, −3.89) | −11.03 (−13.58, −8.47) | — |
| Group*days 2 | 4.75 (2.04, 7.45) | 7.28 (4.30, 10.26) | 3.21 (−0.01, 6.43) | — |
| p-value | 0.004 * | <0.001 * | 0.101 | — |
| ROM for left lateral flexion | ||||
| MSAT 1 | −6.77 (−8.18, −5.36) | −14.20 (−16.72, −11.69) | −15.71 (−18.28, −13.14) | — |
| Control 1 | −1.22 (−2.62, 0.17) | −6.36 (−8.84, −3.88) | −11.78 (−14.32, −9.25) | — |
| Group*days 2 | 5.28 (2.68, 7.87) | 7.57 (4.38, 10.76) | 3.66 (0.44, 6.88) | — |
| p-value | 0.001 * | <0.001 * | 0.062 | — |
| EQ-5D | ||||
| MSAT 1 | — | −0.06 (−0.09, −0.02) | −0.07 (−0.10, −0.04) | −0.20 (−0.24, −0.16) |
| Control 1 | — | −0.05 (−0.09, −0.02) | 7.57 (4.38, 10.76) | 7.57 (4.38, 10.76) |
| Group *days 2 | — | 0.00 (−0.03, 0.04) | 0.00 (−0.04, 0.04) | −0.01 (−0.04, 0.02) |
| p-value | — | 0.841 | 0.925 | 0.553 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, D.; Park, K.-S.; Lee, J.-H.; Ryu, W.-H.; Moon, H.; Park, J.; Jeon, Y.-H.; Seo, J.-Y.; Moon, Y.-J.; Namgoong, J.; et al. Intensive Motion Style Acupuncture Treatment (MSAT) Is Effective for Patients with Acute Whiplash Injury: A Randomized Controlled Trial. J. Clin. Med. 2020, 9, 2079. https://doi.org/10.3390/jcm9072079
Kim D, Park K-S, Lee J-H, Ryu W-H, Moon H, Park J, Jeon Y-H, Seo J-Y, Moon Y-J, Namgoong J, et al. Intensive Motion Style Acupuncture Treatment (MSAT) Is Effective for Patients with Acute Whiplash Injury: A Randomized Controlled Trial. Journal of Clinical Medicine. 2020; 9(7):2079. https://doi.org/10.3390/jcm9072079
Chicago/Turabian StyleKim, Doori, Kyoung-Sun Park, Jin-Ho Lee, Won-Hyung Ryu, Heeyoung Moon, Jiwon Park, Yong-Hyun Jeon, Ji-Yeon Seo, Young-Joo Moon, Jin Namgoong, and et al. 2020. "Intensive Motion Style Acupuncture Treatment (MSAT) Is Effective for Patients with Acute Whiplash Injury: A Randomized Controlled Trial" Journal of Clinical Medicine 9, no. 7: 2079. https://doi.org/10.3390/jcm9072079
APA StyleKim, D., Park, K.-S., Lee, J.-H., Ryu, W.-H., Moon, H., Park, J., Jeon, Y.-H., Seo, J.-Y., Moon, Y.-J., Namgoong, J., Shin, B.-C., & Ha, I.-H. (2020). Intensive Motion Style Acupuncture Treatment (MSAT) Is Effective for Patients with Acute Whiplash Injury: A Randomized Controlled Trial. Journal of Clinical Medicine, 9(7), 2079. https://doi.org/10.3390/jcm9072079