Trends of Hospitalization for Acute Alcohol Intoxication in Slovenian Children and Adolescents with and without Dual Disorder. Implications for a Correct Intervention

 ,
, 
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
2.1. Data Sources and Procedures
2.2. Statistical Analysis
3. Results
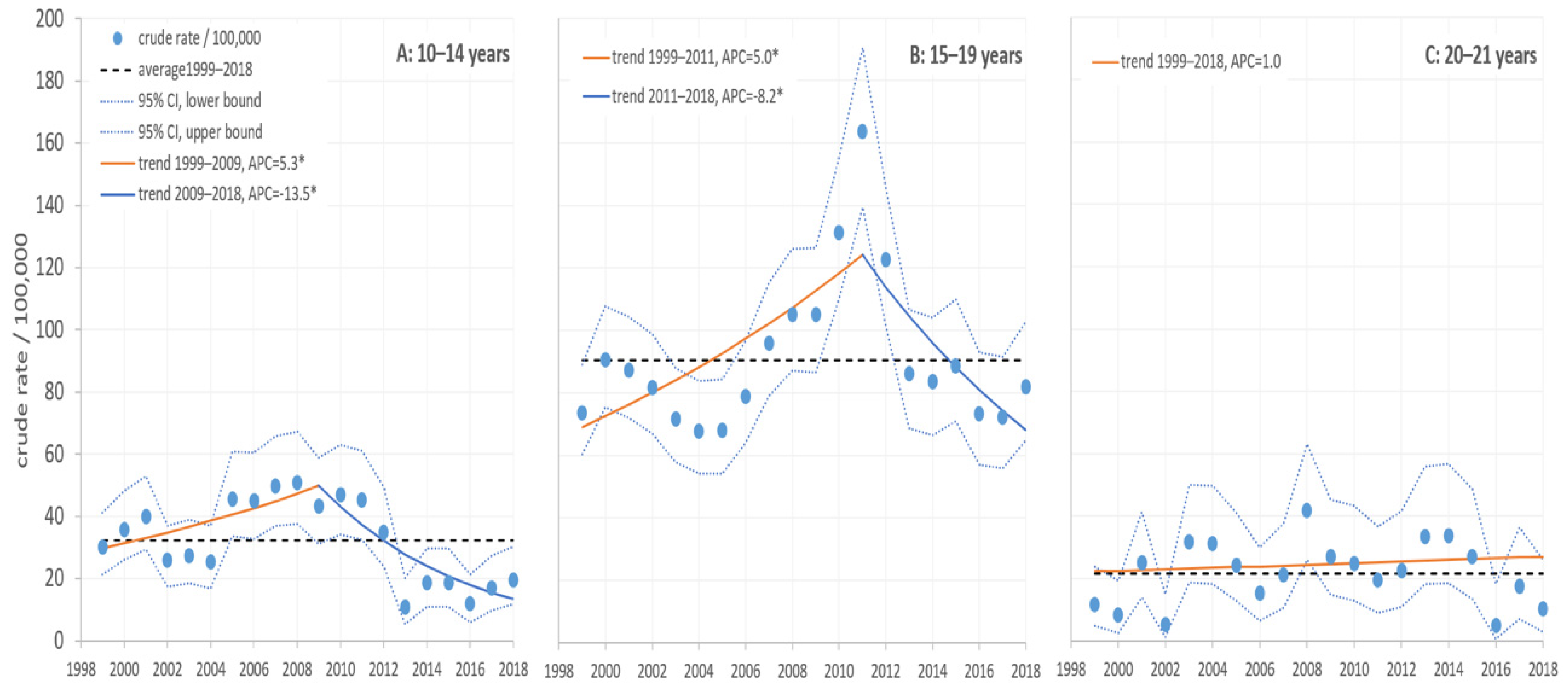
3.1. Mental and Behavioral Disorders Due to Acute Alcohol Intoxication (MBDAAI; F10.0)
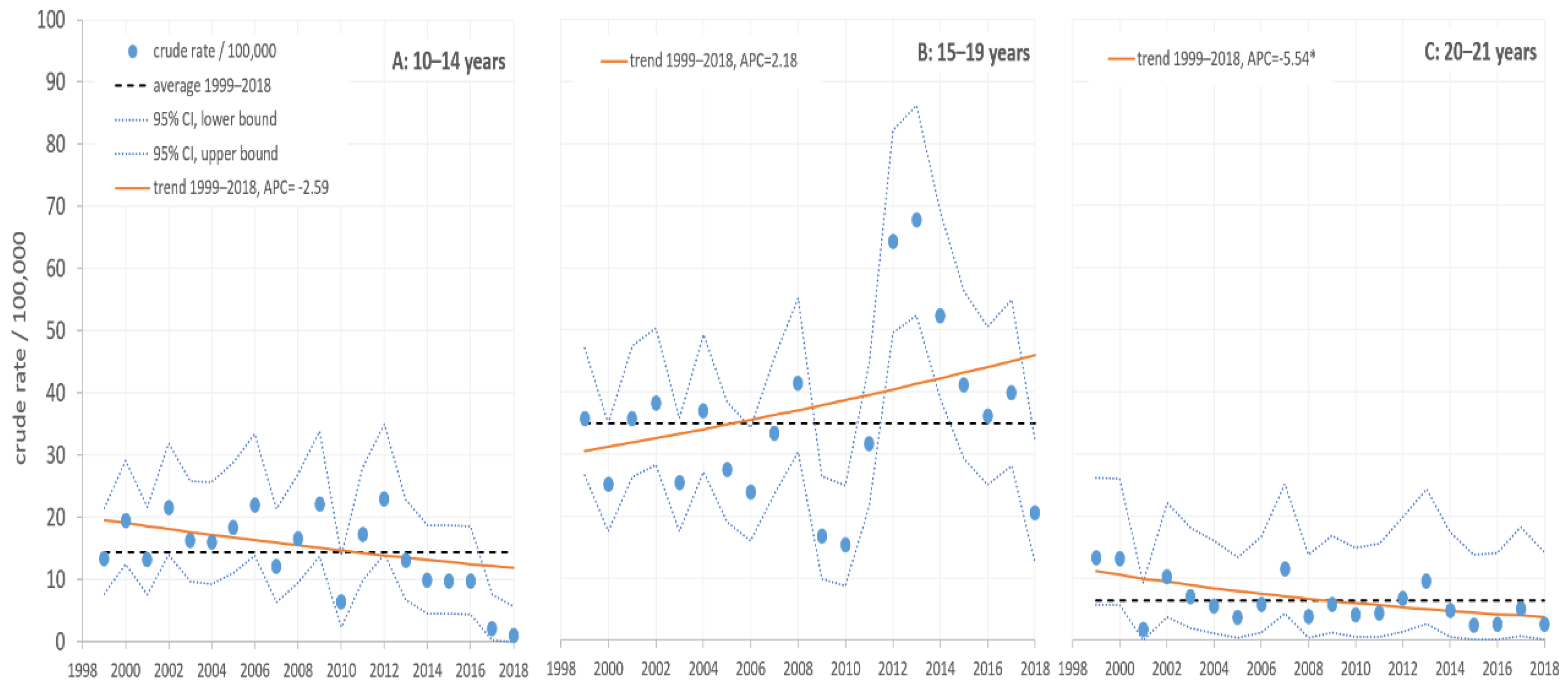
3.2. Toxic Effects of Alcohol (TEA; T51)
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Rehm, J.; Gmel, G.E., Sr.; Gmel, G.; Hasan, O.S.M.; Imtiaz, S.; Popova, S.; Probst, C.; Roerecke, M.; Room, R.; Samokhvalov, A.V.; et al. The relationship between different dimensions of alcohol use and the burden of disease-an update. Addiction 2017, 112, 968–1001. [Google Scholar] [CrossRef] [Green Version]
- WHO. International Classification of Diseases and Related Health Problems, 10th Revision; WHO: Geneva, Switzerland, 2007. [Google Scholar]
- Anderson, P.; Baumberg, B. Alcohol in Europe—Public Health Perspective: Report summary. Drugs Educ. Prev. Policy 2006, 13, 483–488. [Google Scholar] [CrossRef]
- Bagnardi, V.; Rota, M.; Botteri, E.; Tramacere, I.; Islami, F.; Fedirko, V.; Scotti, L.; Jenab, M.; Turati, F.; Pasquali, E.; et al. Alcohol consumption and site-specific cancer risk: A comprehensive dose-response meta-analysis. Br. J. Cancer 2015, 112, 580–593. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global status report on alcohol and health; WHO: Geneve, Switzerland, 2018. [Google Scholar]
- EC. WHO Regional Office for Europe. Alcohol Consumption, Harm and Policy Response Fact Sheets for 30 European Countries; WHO: Copenhagen, Denmark, 2018; p. 1079. [Google Scholar] [CrossRef] [Green Version]
- Rehm, J.; Crépault, J.-F.; Hasan, O.S.M.; Lachenmeier, D.W.; Room, R.; Sornpaisarn, B. Regulatory Policies for Alcohol, other Psychoactive Substances and Addictive Behaviours: The Role of Level of Use and Potency. A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 3749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oscar-Berman, M.; Marinković, K. Alcohol: Effects on neurobehavioral functions and the brain. Neuropsychol. Rev. 2007, 17, 239–257. [Google Scholar] [CrossRef] [PubMed]
- Ryan, S.A.; Kokotailo, P. Alcohol Use by Youth. Pediatrics 2019, 144, e20191357. [Google Scholar] [CrossRef] [Green Version]
- Steinberg, L. Cognitive and affective development in adolescence. Trends Cogn. Sci. 2005, 9, 69–74. [Google Scholar] [CrossRef]
- Casey, B.J.; Jones, R.M.; Hare, T.A. The adolescent brain. Ann. N. Y. Acad. Sci. 2008, 1124, 111–126. [Google Scholar] [CrossRef]
- Yap, M.B.H.; Cheong, T.W.K.; Zaravinos-Tsakos, F.; Lubman, D.I.; Jorm, A.F. Modifiable parenting factors associated with adolescent alcohol misuse: A systematic review and meta-analysis of longitudinal studies. Addiction 2017, 112, 1142–1162. [Google Scholar] [CrossRef]
- Xiao, L.; Bechara, A.; Gong, Q.; Huang, X.; Li, X.; Xue, G.; Wong, S.; Lu, Z.-L.; Palmer, P.; Wei, Y.; et al. Abnormal affective decision making revealed in adolescent binge drinkers using a functional magnetic resonance imaging study. Psychol. Addict. Behav. 2013, 27, 443–454. [Google Scholar] [CrossRef]
- Wells, J.E.; Horwood, L.J.; Fergusson, D.M. Drinking patterns in mid-adolescence and psychosocial outcomes in late adolescence and early adulthood. Addiction 2004, 99, 1529–1541. [Google Scholar] [CrossRef] [PubMed]
- Viner, R.M.; Taylor, B. Adult outcomes of binge drinking in adolescence: Findings from a UK national birth cohort. J. Epidemiol. Community Health 2007, 61, 902–907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Medina, K.L.; McQueeny, T.; Nagel, B.J.; Hanson, K.L.; Schweinsburg, A.D.; Tapert, S.F. Prefrontal cortex volumes in adolescents with alcohol use disorders: Unique gender effects. Alcohol. Clin. Exp. Res. 2008, 32, 386–394. [Google Scholar] [CrossRef] [PubMed]
- Morales, A.M.; Boyd, S.J.; Mackiewicz Seghete, K.L.; Johnson, A.J.; De Bellis, M.D.; Nagel, B.J. Sex Differences in the Effect of Nucleus Accumbens Volume on Adolescent Drinking: The Mediating Role of Sensation Seeking in the NCANDA Sample. J. Stud. Alcohol. Drugs 2019, 80, 594–601. [Google Scholar] [CrossRef]
- WHO. Total Alcohol per Capita Consumption (15+ Years, in Litres of Pure Alcohol). 2016. Available online: https://www.who.int/gho/alcohol/alcohol_011.png?ua=011 (accessed on 6 January 2020). [CrossRef]
- WHO. Age-Standardized Death Rates (15+) for Liver Cirrhosis per 100,000 Population. 2016. Available online: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/liver-cirrhosis-age-standardized-death-rates-(15-)-per-100-000-populatio (accessed on 6 January 2020). [CrossRef]
- Lovrecic, B.; Lovrecic, M. Epidemiološki pogled na porabo alkohola in odvisnost od alkohola v Sloveniji. Javno Zdr. 2018, 2, 51. [Google Scholar] [CrossRef]
- Kraus, L.; Guttormsson, U.; Leifman, H.; Arpa, S.; Molinaro, S.; Monshouwer, K.; Vicente, J.; Arnarsson, Á.M.; Balakireva, O.; Bye, E.K.; et al. ESPAD Report 2015: Results from the European School Survey Project on Alcohol and Other Drugs; Publications Office of the European Union: Luxembourg, 2015; Available online: http://www.espad.org/report/home (accessed on 24 June 2020).
- Inchley, J.; Currie, D.; Young, T.; Samdal, O.; Torsheim, T.; Augustson, L.; Mathison, F.; Aleman-Diaz, A.; Molcho, M.; Weber, M.; et al. Growing up Unequal. HBSC 2016 Study (2013/2014 Survey); WHO Regional Office for Europe: Copenhagen, Denmark, 2016. [Google Scholar]
- Currie, D.; Zanotti, C.; Morgan, A.; Currie, D.; de Looze, M.; Roberts, C.; Samdal, O.; Smith, O.R.F.; Barnekow, V. Social Determinants of Health and Well-Being among Young People. Health Behaviour in School-Aged Children (HBSC) Study: International Report from the 2009/2010 Survey; WHO Regional Office for Europe: Copenhagen, Denmark, 2012. [Google Scholar]
- Stolle, M.; Sack, P.-M.; Spieles, H.; Thomasius, R. Alkoholintoxikierte Kinder und Jugendliche in der Notfallversorgung Hamburger Krankenhäuser (Acute ethanol intoxication among children and adolescents in Hamburg, Germany). Bundesgesundheitsblatt-Gesundheitsforschung-Gesundheitsschutz 2010, 53, 910–916. [Google Scholar] [CrossRef]
- Bouthoorn, S.H.; van Hoof, J.J.; van der Lely, N. Adolescent alcohol intoxication in Dutch hospital centers of pediatrics: Characteristics and gender differences. Eur. J. Pediatr. 2011, 170, 1023–1030. [Google Scholar] [CrossRef]
- Bitunjac, K.; Saraga, M. Alcohol intoxication in pediatric age: Ten-year retrospective study. Croat. Med. J. 2009, 50, 151–156. [Google Scholar] [CrossRef]
- Pavarin, R.M.; Domenicali, M.; Marani, S.; Caputo, F.; Mazzoni, M. Visits of adolescents for acute alcohol intoxication to emergency departments in Northern Italy: Natives and non-natives. J. Subst. Use 2020, 25, 118–122. [Google Scholar] [CrossRef]
- Liisanantti, J.H.; Ala-Kokko, T.I.; Dunder, T.S.; Ebeling, H.E. Contributing Factors in Self-Poisoning Leading to Hospital Admission in Adolescents in Northern Finland. Subst. Use Misuse 2010, 45, 1340–1350. [Google Scholar] [CrossRef]
- Turcin, A.; Turcin, Z.; Kumperscak, H.G.; Zalsman, G.; Kores Plesnicar, B. Suicide attempts among adolescents in northeastern Slovenia: A 25 year report. Int. J. Adolesc. Med. Health 2005, 17, 259–265. [Google Scholar] [CrossRef]
- Donaldson, L. Guidance on the Consumption of Alcohol by Children and Young People. 2009. Available online: https://webarchive.nationalarchives.gov.uk/20130104153257/http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/documents/digitalasset/dh_110256.pdf (accessed on 10 June 2020).
- Slovenia Government. Restrictions on the Use of Alcohol; Act. Zakon o omejevanju porabe alkohola (ZOPA). Uradni list RS, št; 15/03 in 27/17; Slovenian Government: Ljubljana, Slovenia, 2003.
- Radobuljac, M.D.; Hudoklin, M.; Dajcman, N.P.; Kumperscak, H.G. Architecture and functioning of child and adolescent mental health services: A reply from Slovenia. Lancet Psychiatry 2017, 4, e20. [Google Scholar] [CrossRef]
- Slovenia Government. Mental Health Act. Zakon o duševnem zdravju (ZDZdr); Uradni list RS, št. 77/08, 46/15- odl. US in 44/19 odl. US; Slovenian Government: Ljubljana, Slovenia, 2018.
- Bouthoorn, S.H.; van der Ploeg, T.; van Erkel, N.E.; van der Lely, N. Alcohol intoxication among Dutch adolescents: Acute medical complications in the years 2000-2010. Clin. Pediatr. 2011, 50, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Wurdak, M.; Wolstein, J.; Kuntsche, E. Effectiveness of a drinking-motive-tailored emergency-room intervention among adolescents admitted to hospital due to acute alcohol intoxication—A randomized controlled trial. Prev. Med. Rep. 2016, 3, 83–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strandheim, A.; Holmen, T.L.; Coombes, L.; Bentzen, N. Alcohol intoxication and mental health among adolescents—A population review of 8983 young people, 13–19 years in North-Trondelag, Norway: The Young-HUNT Study. Child Adolesc. Psychiatry Ment Health 2009, 3, 18. [Google Scholar] [CrossRef] [Green Version]
- Van Hoof, J.J.; Lely, N.; Pereira, R.R.; van Dalen, W.E. Adolescent alcohol intoxication in the Dutch hospital Departments of Pediatrics. J. Stud. Alcohol. Drugs 2010, 71, 366–372. [Google Scholar] [CrossRef]
- Van Hoof, J.J.; Van Der Lely, N.; Bouthoorn, S.H.; Van Dalen, W.E.; Pereira, R.R. Adolescent alcohol intoxication in the Dutch hospital departments of pediatrics: A 2-year comparison study. J. Adolesc. Health 2011, 48, 212–214. [Google Scholar] [CrossRef] [PubMed]
- Gross, C.; Kraus, L.; Piontek, D.; Reis, O.; Zimmermann, U.S.; Group, R. Prediction of Long-Term Outcomes in Young Adults with a History of Adolescent Alcohol-Related Hospitalization. Alcohol. Alcohol. 2016, 51, 47–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gross, C.; Reis, O.; Kraus, L.; Piontek, D.; Zimmermann, U.S.; Group, R. Long-term outcomes after adolescent in-patient treatment due to alcohol intoxication: A control group study. Drug Alcohol. Depend. 2016, 162, 116–123. [Google Scholar] [CrossRef] [PubMed]
- WHO. Alcohol Consumption, Harm and Policy Responses in 30 European Countries in 2016; WHO: Copenhagen, Denmark, 2019. [Google Scholar]
- Porter, R.S. Alcohol and injury in adolescents. Pediatr. Emerg. Care 2000, 16, 316–320. [Google Scholar] [CrossRef] [PubMed]
- Windle, M. Suicidal Behaviors and Alcohol Use Among Adolescents: A Developmental Psychopathology Perspective. Alcohol. Clin. Exp. Res. 2004, 28, 29S–37S. [Google Scholar] [CrossRef] [PubMed]
- IARC. Alcohol consumption and ethyl carbamate. IARC Monogr. Eval. Carcinog. Risks Hum. 2010, 96, 1–1383. [Google Scholar] [CrossRef]
- Stockwell, T.; Zhao, J. Alcohol’s contribution to cancer is underestimated for exactly the same reason that its contribution to cardioprotection is overestimated. Addiction 2016, 112, 230–232. [Google Scholar] [CrossRef] [PubMed]
- Tapert, S.F.; Aarons, G.A.; Sedlar, G.R.; Brown, S.A. Adolescent substance use and sexual risk-taking behavior. J. Adolesc. Health 2001, 28, 181–189. [Google Scholar] [CrossRef]
- Lovrecic, M.; Lovrecic, B.; Dernovsek, M.Z.; Tavcar, R.; Maremmani, I. Unreported double frequency of heroin addicts visiting psychiatric services and addiction treatment services. Heroin Addict. Relat. Clin. Probl. 2004, 6, 27–32. [Google Scholar]
- Galanter, M. Network Terapy for Alcohol and Drug Abuse: A New Approach in Practice; Basic Books: New York, NY, USA, 1993. [Google Scholar]
- Spiessl, H.; Schon, D.; Cording, C.; Klein, H.E. Expectations and satisfaction of social-psychiatric services regarding their collaboraton with the psychiatric hospital. Neurol. Psychiatry 2000, 68, 557–563. [Google Scholar]
- Shapiro, D.S.; Maholick, L.T. A survey of unmet needs for psychiatric, psychological and social services in an urban community. Int. J. Soc. Psychiatry 1963, 9, 37–44. [Google Scholar] [CrossRef]
- Schaar, I.; Ojehagen, A. Predictors of improvement in quality of life of severely mentally ill substance abusers during 18 months of co-operation between psychiatric and social services. Soc. Psychiatry Psychiatr. Epidemiol. 2003, 38, 83–87. [Google Scholar] [CrossRef]
- Rossler, W.; Hafner, H.; Jung, E.; Loffler, W.; an der Heiden, W.; Martini, H. Need for social psychiatric services—A management model in scientific evaluation. Die Rehabil. 1988, 27, 103–111. [Google Scholar]
- Palmstierna, T.; Gadd, K.; Norman, C.; Svensson, J. Drug addicts with severe mental disorders can be helped by programs using moderate means. Good results when psychiatric, social and drug abuse services cooperate. Lakartidningen 2000, 97, 2205–2206. [Google Scholar]
- Kent, S.; Yellowlees, P. The relationship between social factors and frequent use of psychiatric services. Aust. N. Z. J. Psychiatry 1995, 29, 403–408. [Google Scholar] [CrossRef]
- Anthony, V. Psychiatric social services: Caring for the whole person. Concern Care Aging 1977, 4, 13–14. [Google Scholar] [PubMed]
- Bonder, B.R.; Hulisz, D.; Marsh, S.; Bonaguro, J. Community-Based Substance Abuse Training. Subst. Abus. 2006, 26, 27–30. [Google Scholar] [CrossRef]
- Michaud, P.-A.; Bélanger, R.; Mazur, A.; Hadjipanayis, A.; Ambresin, A.-E. How can primary care practitioners address substance use by adolescents? A position paper of the EUROPEAN academy of PAEDIATRICS. Eur. J. Pediatr. 2020. [Google Scholar] [CrossRef]
- Kulig, J.W. Tobacco, Alcohol, and Other Drugs: The Role of the Pediatrician in Prevention, Identification, and Management of Substance Abuse. Pediatrics 2005, 115, 816–821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knight, J.R.; Sherritt, L.; Shrier, L.A.; Harris, S.K.; Chang, G. Validity of the CRAFFT substance abuse screening test among adolescent clinic patients. Arch. Pediatr. Adolesc. Med. 2002, 156, 607–614. [Google Scholar] [CrossRef] [PubMed]
- Diestelkamp, S.; Arnaud, N.; Sack, P.-M.; Wartberg, L.; Daubmann, A.; Thomasius, R. Brief motivational intervention for adolescents treated in emergency departments for acute alcohol intoxication—A randomized-controlled trial. BMC Emerg. Med. 2014, 14, 13. [Google Scholar] [CrossRef]
- Lovegrove, M.T. Adolescent presentations with alcohol intoxication to the emergency department at Joondalup Health Campus in 2013. Emerg. Med. Australas. 2015, 27, 563–566. [Google Scholar] [CrossRef]


© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lovrecic, M.; Lovrecic, B.; Rok Simon, M.; Korosec, A.; Della Rocca, F.; Maremmani, A.G.I.; Maremmani, I. Trends of Hospitalization for Acute Alcohol Intoxication in Slovenian Children and Adolescents with and without Dual Disorder. Implications for a Correct Intervention. J. Clin. Med. 2020, 9, 2122. https://doi.org/10.3390/jcm9072122
Lovrecic M, Lovrecic B, Rok Simon M, Korosec A, Della Rocca F, Maremmani AGI, Maremmani I. Trends of Hospitalization for Acute Alcohol Intoxication in Slovenian Children and Adolescents with and without Dual Disorder. Implications for a Correct Intervention. Journal of Clinical Medicine. 2020; 9(7):2122. https://doi.org/10.3390/jcm9072122
Chicago/Turabian StyleLovrecic, Mercedes, Barbara Lovrecic, Mateja Rok Simon, Ales Korosec, Filippo Della Rocca, Angelo G. I. Maremmani, and Icro Maremmani. 2020. "Trends of Hospitalization for Acute Alcohol Intoxication in Slovenian Children and Adolescents with and without Dual Disorder. Implications for a Correct Intervention" Journal of Clinical Medicine 9, no. 7: 2122. https://doi.org/10.3390/jcm9072122
APA StyleLovrecic, M., Lovrecic, B., Rok Simon, M., Korosec, A., Della Rocca, F., Maremmani, A. G. I., & Maremmani, I. (2020). Trends of Hospitalization for Acute Alcohol Intoxication in Slovenian Children and Adolescents with and without Dual Disorder. Implications for a Correct Intervention. Journal of Clinical Medicine, 9(7), 2122. https://doi.org/10.3390/jcm9072122