Insulin Resistance Predicts Severity of Coronary Atherosclerotic Disease in Non-Diabetic Patients

 ,
,  , , , ,
, , , , 
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Definitions
2.3. Evaluation of the Complexity and the Extent of the Coronary Atherosclerosis
2.4. Assessment of Insulin Resistance
2.5. Statistical Analysis
3. Results
3.1. Patients’Characteristics
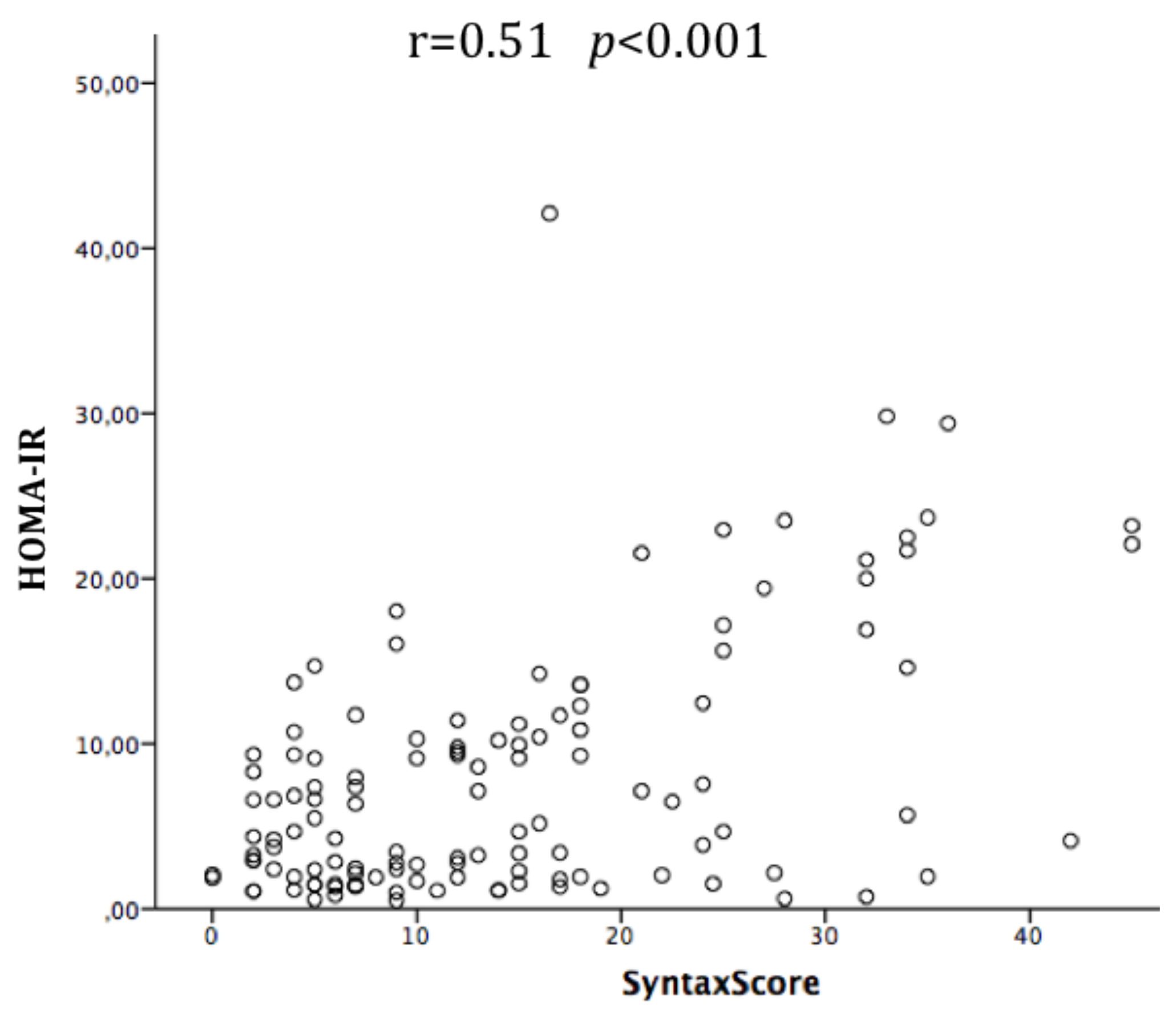
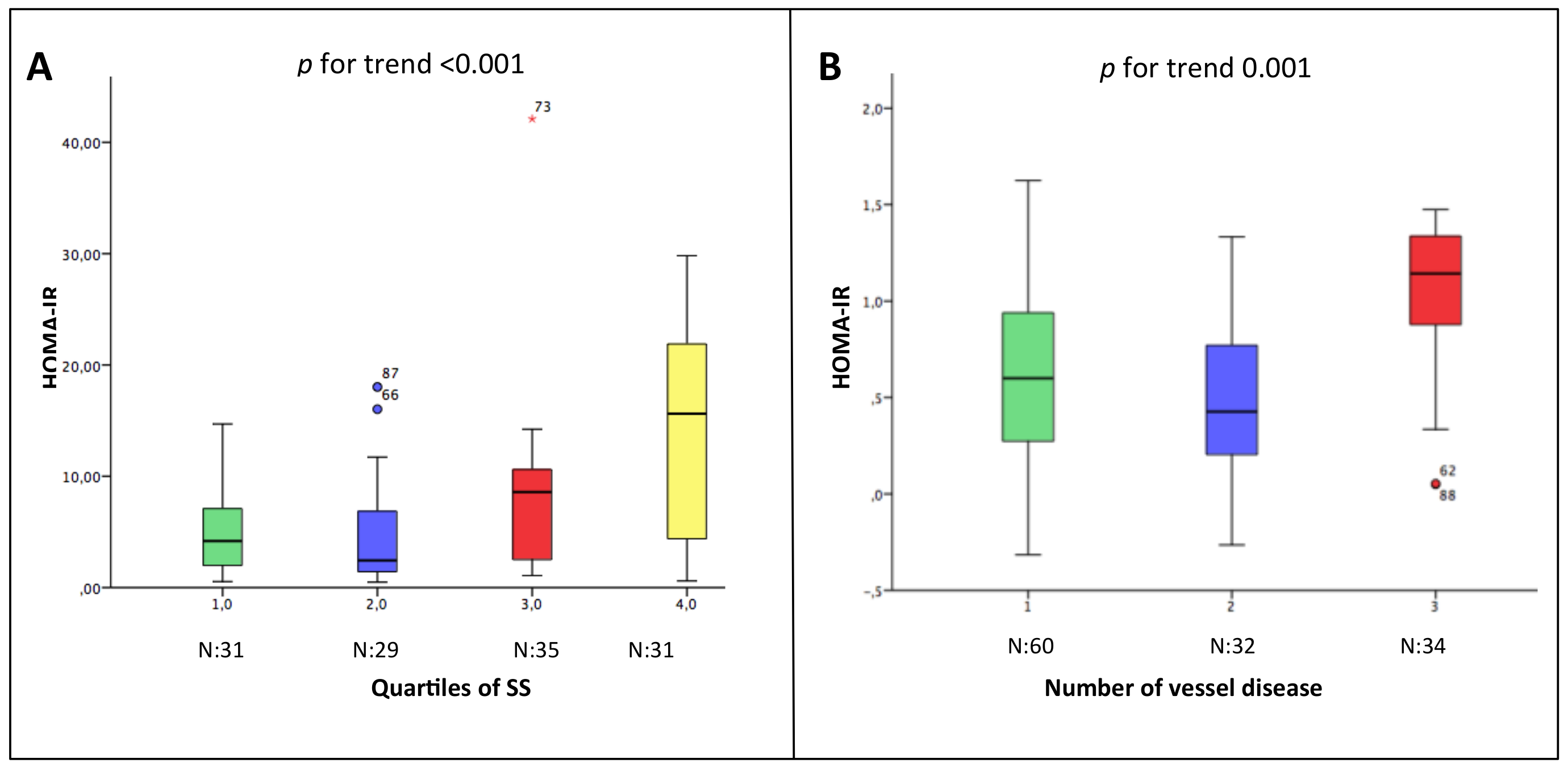
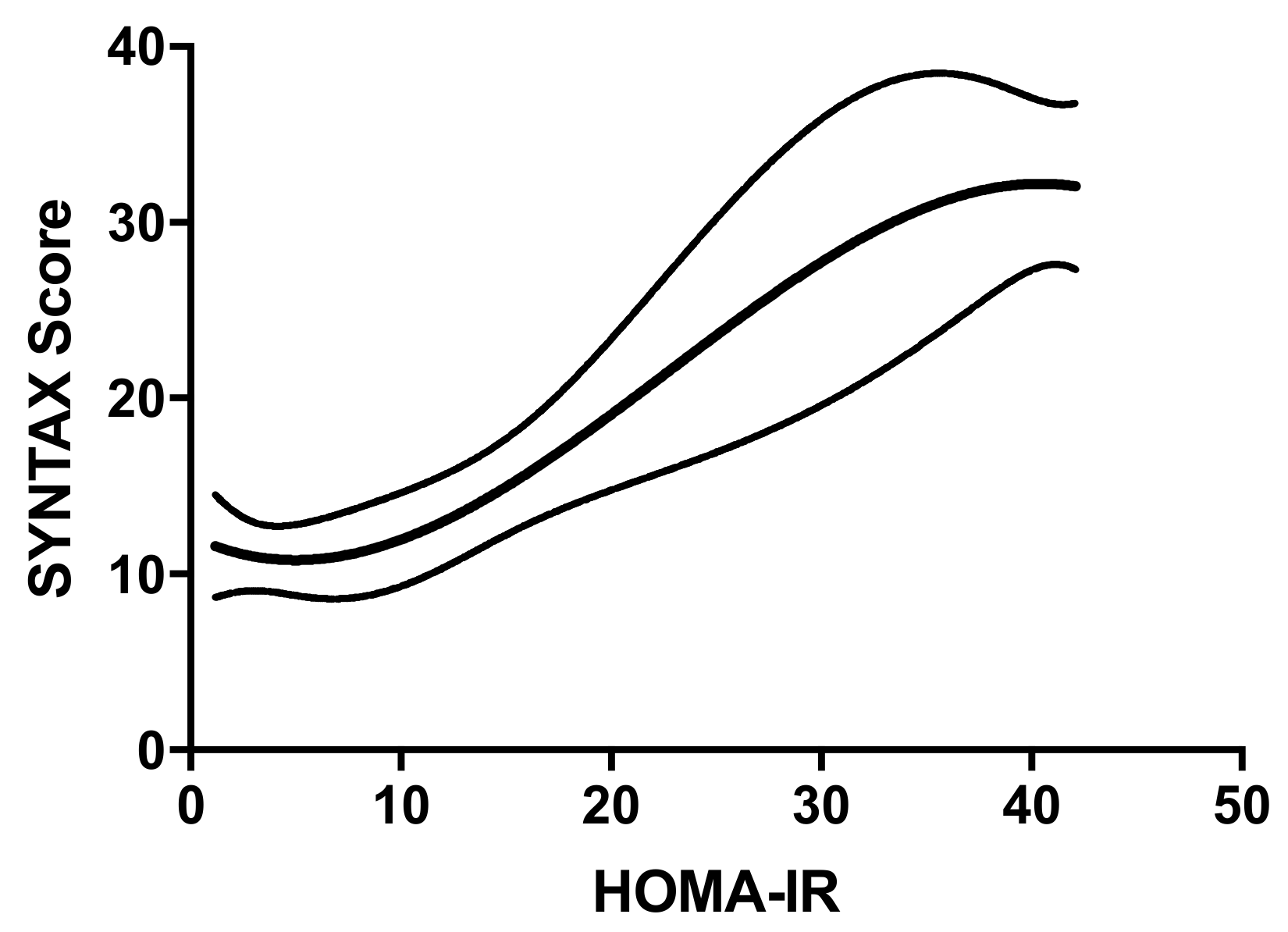
3.2. Insulin Resistance and its Relation with the Severity and the Extension of Coronary Atherosclerosis
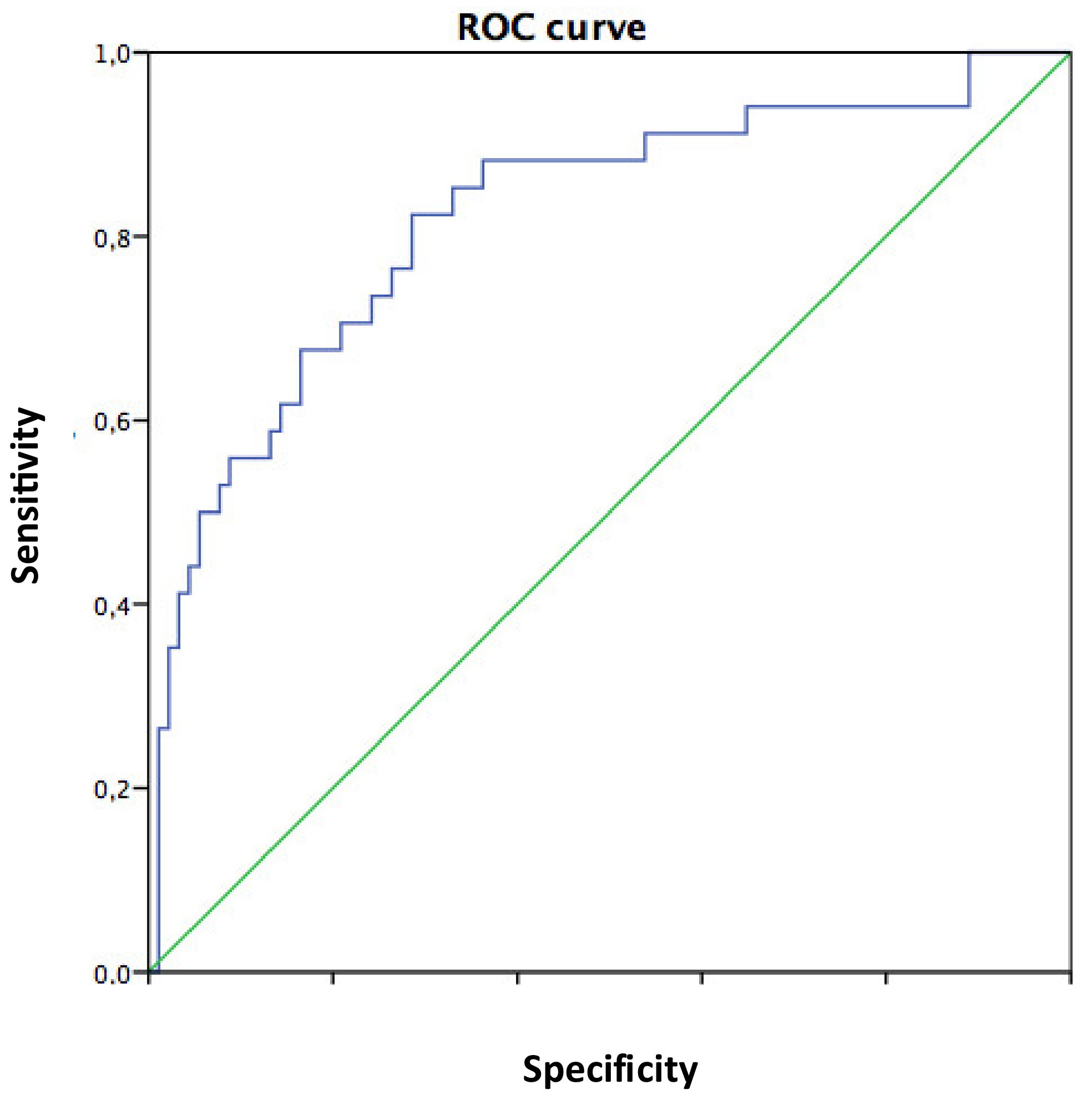
3.3. Predictors of Severity and the Extension of Coronary Atherosclerosis
4. Discussion
4.1. Main Findings
4.2. Insulin Resistance as a Risk Factor for CVD in Non-Diabetic Subjects
4.3. Insulin Resistance and Coronary Atherosclerosis
4.4. Clinical Implications
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Einarson, T.R.; Acs, A.; Ludwig, C.; Panton, U.H. Prevalence of cardiovascular disease in type 2 diabetes: A systematic literature review of scientific evidence from across the world in 2007-2017. Cardiovasc. Diabetol. 2018, 17, 83. [Google Scholar] [CrossRef] [Green Version]
- Haffner, S.M.; Stern, M.P.; Hazuda, H.P.; Mitchell, B.D.; Patterson, J.K. Cardiovascular risk factors in confirmed prediabetic individuals. Does the clock for coronary heart disease start ticking before the onset of clinical diabetes? JAMA 1990, 263, 2893–2898. [Google Scholar] [CrossRef] [PubMed]
- Harris, M.I.; Klein, R.; Welborn, T.A.; Knuiman, M.W. Onset of NIDDM occurs at least 4-7 year before clinical diagnosis. Diabet. Care 1992, 15, 815–819. [Google Scholar] [CrossRef] [PubMed]
- Pyörälä, M.; Miettinen, H.; Laakso, M.; Pyörälä, K. Hyperinsulinemia predicts coronary heart disease risk in healthy middle-aged men: The 22-year follow-up results of the Helsinki Policemen Study. Circulation 1998, 98, 398–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [Green Version]
- Katsuki, A.; Sumida, Y.; Gabazza, E.; Murashima, S.; Furuta, M.; Araki-Sasaki, R.; Hori, Y.; Yano, Y.; Adachi, Y. Homeostasis model assessment is a reliable indicator of insulin resistance during follow-up of patients with type 2 diabetes. Diabetes Care 2001, 24, 362–365. [Google Scholar] [CrossRef] [Green Version]
- Ishizaka, N.; Ishizaka, Y.; Takahashi, E.; Unuma, T.; Tooda, E.-I.; Nagai, R.; Togo, M.; Tsukamoto, K.; Hashimoto, H.; Yamakado, M. Association between insulin resistance and carotid arteriosclerosis in subjects with normal fasting glucose and normal glucose tolerance. Arterioscler Thromb. Vasc. Biol. 2003, 23, 295–301. [Google Scholar] [CrossRef] [Green Version]
- Mossmann, M.; Wainstein, M.V.; Gonçalves, S.C.; Wainstein, R.V.; Gravina, G.L.; Sangalli, M.; Veadrigo, F.; Matte, R.; Reich, R.; Costa, F.G.; et al. HOMA-IR Is Associated With Significant Angiographic Coronary Artery Disease in Non-Diabetic. Non-Obese Individuals: A Cross-Sectional Study. Diabetol. Metab. Syndr. 2015, 7, 100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2013, 36 (Suppl. S1), S67–S74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, B.; Mancia, G.; Spiering, W.; Rosei, E.A.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; De Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology (ESC) and the European Society of Hypertension (ESH). J. Hypertens. 2018, 36, 1953–2041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Catapano, A.L.; Graham, I.; De Backer, G.; Wiklund, O.; Chapman, M.J.; Drexel, H.; Hoes, A.W.; Jennings, C.S.; Landmesser, U.; Pedersen, T.R.; et al. 2016 ESC/EAS guidelines for the management of dyslipidaemias. Eur. Heart 2016, 37, 2999–3058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sianos, G.; Morel, M.A.; Kappetein, A.P.; Morice, M.C.; Colombo, A.; Dawkins, K.; van den Brand, M.; Van Dyck, N.; Russell, M.E.; Mohr, F.W.; et al. The SYNTAX score: An angiographic tool grading the complexity of CAD. EuroInterv 2005, 1, 219–227. [Google Scholar]
- Di Gioia, G.; Scarsini, R.; Strisciuglio, T.; De Biase, C.; Zivelonghi, C.; Franco, D.; De Bruyne, B.; Ribichini, F.; Barbato, E. Correlation Between Angiographic and Physiologic Evaluation of Coronary Artery Narrowings in Patients With Aortic Valve Stenosis. Am. J. Cardiol. 2017, 120, 106–110. [Google Scholar] [CrossRef] [PubMed]
- Balkau, B.; Charles, M.A. Comment on the Provisional Report From the WHO Consultation. European Group for the Study of Insulin Resistance (EGIR) Diabet. Med. 1999, 16, 442–443. [Google Scholar]
- Bonora, E.; Formentini, G.; Calcaterra, F.; Lombardi, S.; Marini, F.; Zenari, L.; Saggiani, F.; Poli, M.; Perbellini, S.; Raffaelli, A.; et al. HOMA-estimated insulin resistance is an independent predictor of cardiovascular disease in type 2 diabetic subjects: Prospective data from the Verona Diabetes Complications Study. Diabetes Care 2002, 25, 1135–1141. [Google Scholar] [CrossRef] [Green Version]
- Rundek, T.; Gardener, H.; Xu, Q.; Goldberg, R.B.; Wright, C.B.; Boden-Albata, B.; Disla, N.; Paik, M.C.; Elkind, M.S.V.; Sacco, R.L. Insulin Resistance and Risk of Ischemic Stroke among Non-Diabetic Individuals from the Northern Manhattan Study. Arch. Neurol. 2010, 67, 1195–1200. [Google Scholar] [CrossRef]
- Åberg, D.; Åberg, N.D.; Jood, K.; Holmegaard, L.; Redfors, P.; Blomstrand, C.; Isgaard, J.; Jern, C.; Svensson, J. Homeostasis model assessment of insulin resistance and outcome of ischemic stroke in non-diabetic patients—A prospective observational study. BMC Neurol. 2019, 19, 177. [Google Scholar] [CrossRef]
- Rader, D.J. Effect of insulin resistance. dyslipidemia. and intra-abdominal adiposity on the development of cardiovascular disease and diabetes mellitus. Am. J. Med. 2007, 120(3) (Suppl. 1), S12–S18. [Google Scholar] [CrossRef]
- Morisco, C.; Lembo, G.; Trimarco, B. Insulin resistance and cardiovascular risk: New insights from molecular and cellular biology. Trends. Cardiovasc Med. 2006, 16, 183–188. [Google Scholar] [CrossRef]
- Strisciuglio, T.; De Luca, S.; Capuano, E.; Luciano, R.; Niglio, T.; Trimarco, B.; Galasso, G. Endothelial dysfunction: Its clinical value and methods of assessment. Curr. Atheroscler Rep. 2014, 16, 417. [Google Scholar] [CrossRef]
- Fiordelisi, A.; Iaccarino, G.; Morisco, C.; Coscioni, E.; Sorriento, D. NFkappaB Is a Key Player in the Crosstalk Between Inflammation and Cardiovascular Diseases. Int. J. Mol. Sci. 2019, 20, 1599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Izzo, R.; de Simone, G.; Trimarco, V.; Gerdts, E.; Giudice, R.; Vaccaro, O.; DeLuca, N.; Trimarco, B. Hypertensive target organ damage predicts incident diabetes mellitus. Eur. Heart J. 2013, 34, 3419–3426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahabala, C.; Srinivasan, M.P.; Manjrekar, P.; Unnikrishnan, B.; Ullal, A.; Kamath, P.K.; Kotekar, M.F. Correlation of severity of coronary artery disease with insulin resistance. N. Am. J. Med. Sci. 2013, 5, 611–614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Os, I.; Os, A.; Abdelnoor, M.; Larsen, A.; Birkeland, K.; Westheim, A. Insulin Sensitivity in Women With Coronary Heart Disease During Hormone Replacement Therapy. J. Womens Health 2005, 14, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Rana, J.S.; Dunning, A.; Achenbach, S. Differences in Prevalence. Extent. Severity. and Prognosis of Coronary Artery Disease Among Patients With and Without Diabetes Undergoing Coronary Computed Tomography Angiography. Diabetes Care 2012, 35, 1787–1794. [Google Scholar] [CrossRef] [Green Version]
- Colaiori, I.; Izzo, R.; Barbato, E.; Franco, D.; Di Gioia, G.; Rapacciuolo, A.; Bartunek, J.; Mancusi, C.; Losi, M.A.; Strisciuglio, T.; et al. Severity of Coronary Atherosclerosis and Risk of Diabetes Mellitus. J. Clin. Med. 2019, 8, 1069. [Google Scholar] [CrossRef] [Green Version]
- Haffner, S.M.; Lehto, S.; Rönnemaa, T.; Pyörälä, K.; Laakso, M. Mortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. N. Engl. J. Med. 1998, 339, 229–234. [Google Scholar] [CrossRef]
- Sanches, P.D.L.; De Mello, M.T.; Elias, N.; Fonseca, F.A.H.; Ganen, A.D.P.; Carnier, J.; Oyama, L.M.; Tock, L.; Tufik, S.; Dâmaso, A.R. Improvement in HOMA-IR is an independent predictor of reduced carotid intima-media thickness in obese adolescents participating in an interdisciplinary weight-loss program. Hypertens Res. 2011, 34, 232–238. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Categorical Variables | SS1 (N 31) | SS2 (N 29) | SS3 (N 35) | SS4 (N 31) | p Value (χ2 Test) |
| Males, n(%) | 21 (68) | 18 (62) | 31 (89) | 24 (77) | 0.18 |
| Smokers, n(%) | 8 (26) | 12 (41) | 17 (49) | 8 (26) | 0.11 |
| Hypertension, n(%) | 24 (77) | 15 (52) | 25 (71) | 24 (77) | 0.22 |
| Dyslipidemia, n(%) | 19 (61) | 20 (69) | 24 (69) | 26 (84) | 0.24 |
| SCAD, n(%) | 20 (65) | 11 (38) | 21 (60) | 23 (74) | 0.07 |
| SCA, n(%) | 17 (55) | 20 (69) | 18 (51) | 12 (39) | 0.06 |
| Continuous Variables | SS1(N 31) | SS2 (N 29) | SS3 (N 35) | SS4 (N 31) | p Value (ANOVA Test) |
| Age, yrs | 67 ± 9 | 65 ± 13 | 64 ± 11 | 71 ± 11 | 0.06 |
| BMI, kg/m2 | 27 ± 6 | 26.8 ± 4 | 28.5 ± 4 | 26.8 ± 3 | 0.31 |
| FPG, mg/dL | 99 ± 22 | 97 ± 13 | 105 ± 24 | 101 ± 16 | 0.33 |
| SBP, mmHg | 131 ± 16 | 131 ± 19 | 127 ± 16 | 134 ± 16 | 0.44 |
| DBP, mmHg | 72 ± 8 | 74 ± 10 | 72 ± 10 | 75 ± 11 | 0.46 |
| EF, % | 54 ± 10 | 51 ± 9 | 53 ± 9 | 54 ± 8 | 0.49 |
| eGFR EPI-CKD mL/min | 79 ± 22 | 81 ± 24 | 80 ± 21 | 71 ± 21 | 0.33 |
| SS4 | Three-Vessel Disease | |||||||
|---|---|---|---|---|---|---|---|---|
| Variables | OR | 95% CI | p | OR | 95% CI | p | ||
| Males | 0.46 | 0.08 | 2.49 | 0.37 | 0.43 | 0.09 | 2.06 | 0.29 |
| Age | 1.12 | 1.03 | 1.22 | 0.01 | 1.05 | 0.98 | 1.13 | 0.15 |
| HOMA-IR | 1.22 | 1.11 | 1.34 | < 0.01 | 1.22 | 1.09 | 1.36 | < 0.01 |
| Hypertension | 0.15 | 0.01 | 1.67 | 0.12 | 0.37 | 0.05 | 2.79 | 0.33 |
| Smoke | 2.06 | 0.35 | 12.19 | 0.43 | 0.41 | 0.08 | 2.06 | 0.28 |
| Dyslipidemia | 1.09 | 0.14 | 8.19 | 0.93 | 0.89 | 0.14 | 5.67 | 0.89 |
| BMI | 0.78 | 0.59 | 1.02 | 0.07 | 0.83 | 0.66 | 1.05 | 0.12 |
| Ca2+Antagonists | 1.77 | 0.28 | 11.05 | 0.54 | 1.71 | 0.31 | 9.46 | 0.54 |
| BB | 1.27 | 0.19 | 8.21 | 0.8 | 1.88 | 0.29 | 11.90 | 0.50 |
| Statins | 0.21 | 0.01 | 5.07 | 0.34 | 0.4 | 0.03 | 5.52 | 0.49 |
| ACEI-ARBs | 3.36 | 0.35 | 31.9 | 0.29 | 3.86 | 0.50 | 29.7 | 0.19 |
| LDL | 1.01 | 0.99 | 1.02 | 0.41 | 1 | 0.98 | 1.02 | 0.74 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Strisciuglio, T.; Izzo, R.; Barbato, E.; Di Gioia, G.; Colaiori, I.; Fiordelisi, A.; Morisco, C.; Bartunek, J.; Franco, D.; Ammirati, G.; et al. Insulin Resistance Predicts Severity of Coronary Atherosclerotic Disease in Non-Diabetic Patients. J. Clin. Med. 2020, 9, 2144. https://doi.org/10.3390/jcm9072144
Strisciuglio T, Izzo R, Barbato E, Di Gioia G, Colaiori I, Fiordelisi A, Morisco C, Bartunek J, Franco D, Ammirati G, et al. Insulin Resistance Predicts Severity of Coronary Atherosclerotic Disease in Non-Diabetic Patients. Journal of Clinical Medicine. 2020; 9(7):2144. https://doi.org/10.3390/jcm9072144
Chicago/Turabian StyleStrisciuglio, Teresa, Raffaele Izzo, Emanuele Barbato, Giuseppe Di Gioia, Iginio Colaiori, Antonella Fiordelisi, Carmine Morisco, Jozef Bartunek, Danilo Franco, Giuseppe Ammirati, and et al. 2020. "Insulin Resistance Predicts Severity of Coronary Atherosclerotic Disease in Non-Diabetic Patients" Journal of Clinical Medicine 9, no. 7: 2144. https://doi.org/10.3390/jcm9072144
APA StyleStrisciuglio, T., Izzo, R., Barbato, E., Di Gioia, G., Colaiori, I., Fiordelisi, A., Morisco, C., Bartunek, J., Franco, D., Ammirati, G., Pergola, V., Imparato, L., Trimarco, B., Esposito, G., & Rapacciuolo, A. (2020). Insulin Resistance Predicts Severity of Coronary Atherosclerotic Disease in Non-Diabetic Patients. Journal of Clinical Medicine, 9(7), 2144. https://doi.org/10.3390/jcm9072144