Virtual Reality Aggression Prevention Therapy (VRAPT) versus Waiting List Control for Forensic Psychiatric Inpatients: A Multicenter Randomized Controlled Trial

 , , , , and
, , , , and
Abstract
:1. Introduction
- decreases both self-reported and staff-reported aggressive behavior;
- reduces determinants of aggressive behavior, including anger, impulsivity, and hostility.
2. Methods
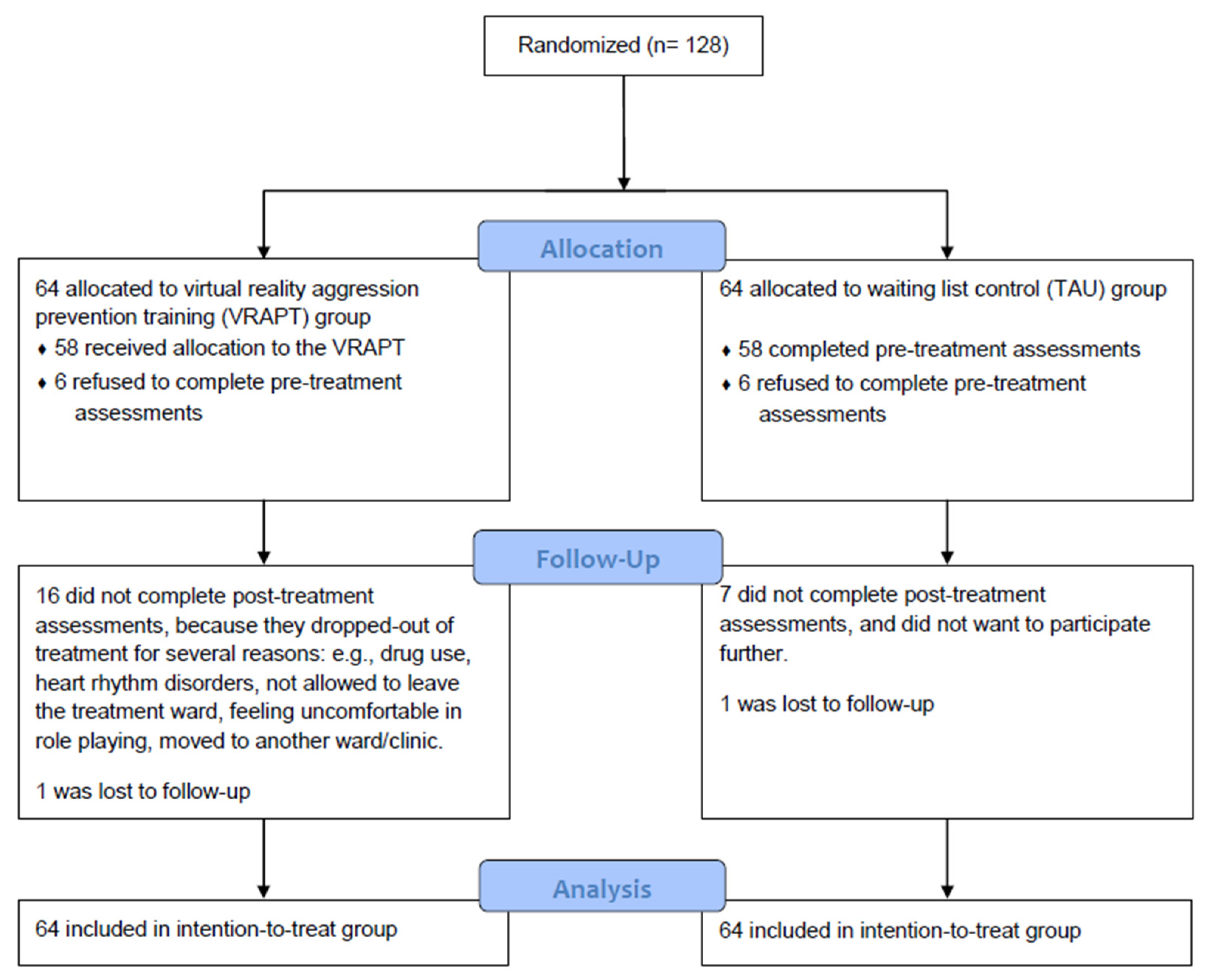
2.1. Study Design and Participants
2.2. Randomization and Masking
2.3. Procedures
2.4. Intervention
2.5. Outcomes
2.5.1. Primary Outcome—Aggression
Social Dysfunction and Aggression Scale (SDAS)—Completed by Staff Members
Aggression Questionnaire (AVL)—Completed by Participants
2.5.2. Secondary Outcomes
2.5.3. Other Measures
2.6. Statistical Analyses
3. Results
4. Discussion
4.1. Strengths and Limitations
4.2. Implications and Future Research
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Broderick, C.; Azizian, A.; Kornbluh, R.; Warburton, K. Prevalence of physical violence in a forensic psychiatric hospital system during 2011–2013: Patient assaults, staff assaults, and repeatedly violent patients. CNS Spectr. 2015. [Google Scholar] [CrossRef]
- Verstegen, N.; de Vogel, V.; de Vries Robbé, M.; Helmerhorst, M. Inpatient violence in a Dutch forensic psychiatric hospital. J. Forensic Pract. 2017, 19, 102–114. [Google Scholar] [CrossRef]
- Novaco, R.W.; Taylor, J.L. Behaviour Research and Therapy Reduction of assaultive behavior following anger treatment of forensic hospital patients with intellectual disabilities. Behav. Res. Ther. 2015, 65, 52–59. [Google Scholar] [CrossRef]
- Papadopoulos, C.; Ross, J.; Stewart, D.; Dack, C.; James, K.; Bowers, L. The antecedents of violence and aggression within psychiatric in-patient settings. Acta Psychiatr. Scand. 2012, 125, 425–439. [Google Scholar] [CrossRef] [PubMed]
- Ross, J.; Quayle, E.; Newman, E.; Tansey, L. The impact of psychological therapies on violent behaviour in clinical and forensic settings: A systematic review. Aggress. Violent Behav. 2013, 18, 761–773. [Google Scholar] [CrossRef]
- Brännström, L.; Kaunitz, C.; Andershed, A.K.; South, S.; Smedslund, G. Aggression replacement training (ART) for reducing antisocial behavior in adolescents and adults: A systematic review. Aggress. Violent Behav. 2016, 17, 30–41. [Google Scholar] [CrossRef] [Green Version]
- Papalia, N.; Spivak, B.; Daffern, M.; Ogloff, J.R.P. A meta-analytic review of the efficacy of psychological treatments for violent offenders in correctional and forensic mental health settings. Clin. Psychol. Sci. Pract. 2019, 26, 1–28. [Google Scholar] [CrossRef]
- Tuente, S.K.; Bogaerts, S.; Van Ijzendoorn, S.; Veling, W. Effect of virtual reality aggression prevention training for forensic psychiatric patients (VRAPT): Study protocol of a multi-center RCT. BMC Psychiatry 2018, 18, 1–9. [Google Scholar]
- Crick, N.R.; Dodge, K.A. A Review and Reformulation of Social Information-Processing Mechanisms in Children’s Social Adjustment. Psychol. Bull. 1994, 115, 74–101. [Google Scholar] [CrossRef]
- Oostermeijer, S.; Nieuwenhuijzen, M.; van de Ven, P.M.; Popma, A.; Jansen, L.M.C. Social information processing problems related to reactive and proactive aggression of adolescents in residential treatment. Pers. Individ. Differ. 2016, 90, 54–60. [Google Scholar] [CrossRef]
- Kobes, M.H.B.M.; Nijman, H.H.L.I.; Bulten, E.B.H. Assessing aggressive behavior in forensic psychiatric patients: Validity and clinical utility of combining two instruments. Arch. Psychiatr. Nurs. 2012, 26, 487–494. [Google Scholar] [CrossRef] [PubMed]
- Wistedt, B.; Rasmussen, A.; Pederson, L.; Malm, U.; Traskman-Bendz, L.; Wakelin, J.; Bech, P. The development of an observer scale for measuring social dysfunction and aggression. Pharmacopsychiatry 1990, 23, 249–252. [Google Scholar] [CrossRef] [PubMed]
- Bousardt, A.; Hoogendoorn, A.W.; Noorthoorn, E.O.; Hummelen, J.W.; Nijman, H.L. Predicting inpatient aggression by self-reported impulsivity in forensic psychiatric patients. Crim. Behav. Ment. Health 2016, 26, 161–173. [Google Scholar] [CrossRef] [PubMed]
- Meesters, C.; Muris, P.; Bosma, H.; Schouten, E.; Beuving, S. Psychometric evaluation of the Dutch version of the Aggression Questionnaire. Behav. Res. Ther. 1996, 34, 839–843. [Google Scholar] [CrossRef]
- Buss, A.H.; Perry, M. The Aggression Questionnaire. J. Pers. Soc. Psychol. 1992, 63, 452–459. [Google Scholar] [CrossRef] [PubMed]
- Patton, J.H.; Stanford, M.S.; Barratt, E.S. Factor Structure of the Barratt impulsiveness scale. J. Clin. Psychol. 1995, 51, 768–774. [Google Scholar] [CrossRef]
- Lange, A.; Hoogendoorn, M.; Wiederspahn, A.; de Beurs, E. BDHI-Dutch: Buss-Durkee Hostility Inventory; Handleiding, Verantwoording en Normering van de Nederlandse Buss-Durkee Agressie Vragenlijst (Manual and Norms of the Dutch Adaptation of the BUss-Durkee Hostility Inventory); Swets & Zeitlinger: Lisse, The Netherlands, 1995. [Google Scholar]
- Hornsveld, R.H.J.; Muris, P.; Kraaimaat, F.W. The Novaco Anger Scale—Provocation Inventory (1994 Version) in Dutch Forensic Psychiatric Patients. Psychol. Assess. 2011, 23, 937–944. [Google Scholar] [CrossRef]
- Hovens, J.E.; Lievaart, M.; Rodenburg, J.J. STAXI-2: Vragenlijst over Boosheid; Hogrefe: Amsterdam, The Netherlands, 2014. [Google Scholar]
- Domburgh, L.; Popma, A. Reactive and Proactive Questionnaire [Dutch Translation]; PI Research: Duivendrecht, The Netherlands, 2003. [Google Scholar]
- Smeijers, D.; Rinck, M.; Bulten, E.; van den Heuvel, T.; Verkes, R.J. Generalized hostile interpretation bias regarding facial expressions: Characteristic of pathological aggressive behavior. Aggress. Behav. 2017, 43, 386–397. [Google Scholar] [CrossRef]
- Bernstein, D.P.; Stein, J.A.; Newcomb, M.D.; Walker, E.; Pogge, D.; Ahluvalia, T.; Stokes, J.; Handelsman, L.; Medrano, M.; Desmond, D.; et al. Development and validation of a brief screening version of the Childhood Trauma Questionnaire. Child Abus. Negl. 2003, 27, 169–190. [Google Scholar] [CrossRef]
- Schubert, T.; Friedmann, F.; Regenbrecht, H. The Experience of Presence: Factor Analytic Insights. Presence 2001, 10, 266–281. [Google Scholar] [CrossRef]
- Faraone, S.V. Interpreting estimates of treatment effects: Implications for managed care. Pharm. Ther. 2008, 33, 700. [Google Scholar]
- Cullen, A.E.; Clarke, A.Y.; Kuipers, E.; Hodgins, S.; Dean, K.; Fahy, T. A Multisite Randomized Trial of a Cognitive Skills Program for Male Mentally Disordered Offenders: Violence and Antisocial Behavior Outcomes. J. Consult. Clin. Psychol. 2012, 80, 1114. [Google Scholar] [CrossRef] [PubMed]
- Tarrier, N.; Dolan, M.; Doyle, M.; Dunn, G.; Shaw, J.; Blackburn, R. Exploratory randomised control trial of schema modal therapy in the personality disorder service at Ashworth Hospital. In Ministry of Justice Research; GORS: London, UK, 2010; Volume 5, p. 10. [Google Scholar]
- Wilson, C.; Gandolfi, S.; Dudley, A.; Thomas, B.; Tapp, J.; Moore, E.; Service, G.; Unit, N.T.; Hospital, B. Evaluation of anger management groups in a high-security hospital. Crim. Behav. Ment. Health 2013, 371, 356–371. [Google Scholar] [CrossRef] [PubMed]
- Lardén, M.; Nordén, E.; Forsman, M.; Långström, N. Effectiveness of aggression replacement training in reducing criminal recidivism among convicted adult offenders. Crim. Behav. Ment. Health 2018, 28, 476–491. [Google Scholar] [CrossRef] [PubMed]
- Jolliffe, D.; Farrington, D.P. A systematic review of the national and international evidence on the effectiveness of interventions with violent offenders. In Ministry of Justice Research; GORS: London, UK, 2007; Volume 16, p. 7. [Google Scholar]
- Lemerise, E.; Arsenio, W.F. An integrated model of emotion processes and cognition in social information processing. Child Dev. 2000, 71, 107–118. [Google Scholar] [CrossRef]
- Sansone, R.A.; Leung, J.S.; Wiederman, M.W. Having been bullied in childhood: Relationship to aggressive behaviour in adulthood. Int. J. Soc. Psychiatry 2012, 8, 824–826. [Google Scholar] [CrossRef] [PubMed]
- Sarchiapone, M.; Carli, V.; Cuomo, C.; Marchetti, M.; Roy, A. Association between childhood trauma and aggression in male prisoners. Psychiatry Res. 2009, 165, 187–192. [Google Scholar] [CrossRef]
- Veling, W.; Counotte, J.; Os, J. Van; Van Der Gaag, M. Childhood trauma, psychosis liability and social stress reactivity: A virtual reality study. Psychol. Med. 2016, 46, 3339–3348. [Google Scholar] [CrossRef]
- Broome, M.R.; Johns, L.C.; Valli, I.; Woolley, J.B.; Tabraham, P.; Brett, C.; Valmaggia, L.; Peters, E.; Garety, P.A.; McGuire, P.K. Delusion formation and reasoning biases in those at clinical high risk for psychosis. Br. J. Psychiatry 2007, 191, S38–S42. [Google Scholar] [CrossRef]
- Kip, H.; Bouman, Y.H.A.; Kelders, S.M.; van Gemert-Pijnen, L.J.E.W.C. eHealth in treatment of Offenders in Forensic mental Health: A Review of the current State. Front. Psychiatry 2018, 9, 42. [Google Scholar] [CrossRef]
- Bernstein, D.P.; Arntz, A.; De Vos, M. Schema focused therapy in forensic settings: Theoretical model and recommendations for best clinical practice. Int. J. Forensic Ment. Health 2012, 6, 169–183. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| VRAPT Group (n = 64) | Waiting List (n = 64) | ||||||
|---|---|---|---|---|---|---|---|
| M (SD) or n % | M (SD) or n % | p | |||||
| Age, in years | 39.4 | (10.6) | 38.0 | (10.0) | t (126) = 0.80 | 0.43 | |
| Dutch origin | 47 | 73% | 51 | 80% | X2(1) = 0.70 | 0.40 | |
| Highest completed education level | X2(5) = 4.28 | 0.51 | |||||
| None | 4 | 6% | 6 | 9% | |||
| Lower education | 45 | 70% | 36 | 56% | |||
| Intermediate education | 7 | 11% | 7 | 11% | |||
| Tertiary education | 2 | 3% | 2 | 3% | |||
| Lower special education | 5 | 8% | 12 | 19% | |||
| Missing | 1 | 2% | 1 | 2% | |||
| DSM-5 diagnosis * | |||||||
| Schizophrenia | 12 | 19% | 14 | 22% | |||
| Schizoaffective disorder | 0 | 0% | 2 | 3% | |||
| Delusional Disorder | 0 | 0% | 2 | 3% | |||
| Psychotic disorder Not Otherwise Specified (NOS) | 6 | 10% | 4 | 6% | |||
| Paranoid personality disorder | 0 | 0% | 1 | 2% | |||
| Antisocial personality disorder | 22 | 35% | 26 | 41% | |||
| Borderline personality disorder | 13 | 21% | 3 | 5% | |||
| Narcissistic personality disorder | 4 | 6% | 3 | 5% | |||
| Dependent personality disorder | 1 | 2% | 1 | 2% | |||
| Personality disorder NOS | 25 | 40% | 27 | 43% | |||
| Autism spectrum disorder | 5 | 8% | 12 | 19% | |||
| Attention-deficit/hyperactivity disorder | 11 | 17% | 8 | 13% | |||
| Pedophilia | 4 | 6% | 4 | 6% | |||
| Other paraphilias | 3 | 5% | 2 | 3% | |||
| First-offender | 4 | 6% | 5 | 8% | X2(1) = 0.12 | 0.73 | |
| Age at first conviction, in years | 18.9 | (5.2) | 18.9 | (6.6) | t (116) = 0.02 | 0.99 | |
| Type of first offense (n = 119) * | |||||||
| (Attempted) homicide | 4 | 6% | 3 | 5% | |||
| Sexual offense | 4 | 6% | 1 | 2% | |||
| Violent offense | 26 | 41% | 26 | 41% | |||
| Property offense | 28 | 44% | 29 | 45% | |||
| Arson | 2 | 3% | 3 | 5% | |||
| Other | 11 | 17% | 10 | 16% | |||
| Age at index offense, in years | 31.3 | (9.8) | 29.5 | (9.2) | t (126) = 1.10 | 0.27 | |
| Type of index offense * | |||||||
| (Attempted) homicide | 31 | 49% | 23 | 36% | |||
| Sexual offense | 16 | 25% | 20 | 31% | |||
| Violent offense | 37 | 59% | 37 | 58% | |||
| Property offense | 17 | 27% | 18 | 28% | |||
| Arson | 4 | 6% | 3 | 5% | |||
| Damage of index offense * | |||||||
| No injury | 10 | 16% | 6 | 9% | |||
| Physical injury | 34 | 53% | 40 | 63% | |||
| Deadly injury | 11 | 17% | 8 | 13% | |||
| Material damage | 15 | 23% | 15 | 23% | |||
| Psychological neglect | 5 | 8% | 7 | 11% | |||
| Missing | 5 | 8% | 4 | 6% | |||
| Childhood trauma (CTQ-SF) | (N = 55) | (N = 57) | |||||
| Childhood trauma total | 53.8 | (20.8) | 53.5 | (20.7) | U = 1502 | 0.95 | |
| Emotional Abuse | 11.4 | (5.6) | 11.0 | (5.6) | U = 1508.5 | 0.55 | |
| Emotional Neglect | 13.0 | (5.4) | 13.4 | (6.1) | U = 1584.5 | 0.79 | |
| Psychical Abuse | 11.2 | (6.6) | 9.9 | (6.2) | U = 1376.5 | 0.32 | |
| Psychical Neglect | 10.8 | (3.4) | 11.0 | (2.7) | U = 1787.5 | 0.26 | |
| Sexual Abuse | 7.9 | (5.4) | 8.6 | (5.8) | U = 1681 | 0.45 | |
| VRAPT | Waiting List Control | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Follow-up | Pre | Post | Follow-up | ||||||||
| Instrument | M | SD | M | SD | M | SD | M | SD | M | SD | M | SD | |
| Staff-rated | n = 64 | n = 63 | n = 62 | n = 64 | n = 64 | n = 62 | |||||||
| Peak aggression (primary outcome) | SDAS | 6.9 | 6.4 | 6.9 | 6.7 | 6.9 | 6.7 | 6.2 | 6.9 | 6.6 | 7.0 | 6.2 | 6.6 |
| General aggression | SDAS | 4.0 | 4.5 | 4.3 | 5.0 | 4.1 | 5.1 | 3.6 | 5.0 | 3.8 | 4.7 | 3.6 | 4.5 |
| Aggression | n = 58 | n = 43 | n = 42 | n = 58 | n = 51 | n = 50 | |||||||
| Aggression—total (primary outcome) | AVL | 81.0 | 18.0 | 73.5 | 19.1 | 70.8 | 18.1 | 83.1 | 19.1 | 76.7 | 20.8 | 69.7 | 21.2 |
| Physical aggression | AVL | 27.6 | 8.6 | 24.0 | 8.8 | 22.0 | 8.5 | 28.0 | 8.3 | 24.2 | 9.0 | 21.5 | 8.7 |
| Verbal aggression | AVL | 14.9 | 3.0 | 14.1 | 3.2 | 13.9 | 2.9 | 14.9 | 2.9 | 14.3 | 3.2 | 13.3 | 3.6 |
| Anger | AVL | 18.1 | 5.1 | 16.3 | 5.0 | 15.7 | 5.1 | 18.3 | 5.5 | 17.5 | 5.6 | 16.4 | 5.8 |
| Hostility | AVL | 20.6 | 5.9 | 19.0 | 6.1 | 19.2 | 6.4 | 21.9 | 7.0 | 20.7 | 7.4 | 18.5 | 7.1 |
| Reactive and proactive aggression—total | RPQ | 18.8 | 9.4 | 11.5 | 10.1 | 10.0 | 11.4 | 18.9 | 9.5 | 12.5 | 10.7 | 11.8 | 10.7 |
| Proactive aggression | RPQ | 7.6 | 5.6 | 4.4 | 5.3 | 3.7 | 6.0 | 7.8 | 5.4 | 5.3 | 6.3 | 4.8 | 5.9 |
| Reactive aggression | RPQ | 11.3 | 4.6 | 7.1 | 5.6 | 6.3 | 5.9 | 11.2 | 5.1 | 7.3 | 5.2 | 7.0 | 5.5 |
| Aggression and hostility—total | BDHI_D | 20.0 | 6.2 | 17.2 | 6.8 | 18.0 | 7.2 | 19.3 | 6.8 | 19.9 | 7.4 | 18.0 | 7.6 |
| Direct aggression | BDHI_D | 10.1 | 3.9 | 7.9 | 4.4 | 8.4 | 4.5 | 9.3 | 3.9 | 8.9 | 4.0 | 8.5 | 4.1 |
| Indirect aggression | BDHI_D | 8.0 | 4.2 | 6.7 | 4.4 | 7.1 | 4.5 | 8.0 | 4.4 | 8.7 | 5.0 | 7.2 | 5.1 |
| Social desirability | BDHI_D | 2.0 | 1.3 | 2.5 | 1.4 | 2.5 | 1.3 | 2.0 | 1.3 | 2.3 | 1.4 | 2.2 | 1.3 |
| Anger | |||||||||||||
| State anger | STAXI-2 | 18.1 | 6.6 | 17.0 | 5.0 | 18.2 | 7.3 | 17.8 | 5.6 | 17.8 | 6.3 | 16.7 | 3.9 |
| Trait anger | STAXI-2 | 18.0 | 5.2 | 16.4 | 4.9 | 16.5 | 6.0 | 17.5 | 5.5 | 17.2 | 6.3 | 15.8 | 5.6 |
| Anger expression—Out | STAXI-2 | 17.0 | 4.6 | 15.5 | 3.8 | 15.7 | 4.4 | 16.0 | 4.6 | 16.0 | 4.5 | 15.7 | 4.7 |
| Anger expression—In | STAXI-2 | 17.1 | 3.6 | 17.0 | 4.3 | 17.1 | 4.1 | 16.9 | 3.7 | 16.8 | 3.6 | 15.8 | 3.9 |
| Anger control—Out | STAXI-2 | 21.2 | 5.1 | 23.1 | 5.5 | 22.8 | 5.3 | 21.0 | 5.3 | 20.9 | 5.0 | 21.5 | 5.2 |
| Anger control—In | STAXI-2 | 22.0 | 4.9 | 23.6 | 5.5 | 23.9 | 5.5 | 22.5 | 5.7 | 22.3 | 5.2 | 22.6 | 5.7 |
| Anger expression index | STAXI-2 | 38.6 | 12.8 | 33.7 | 13.8 | 34.4 | 15.2 | 37.4 | 13.9 | 37.6 | 12.7 | 35.4 | 13.6 |
| Anger | NAS-PI | 86.9 | 15.8 | 80.9 | 16.1 | 80.1 | 17.8 | 86.9 | 15.9 | 84.0 | 16.7 | 79.8 | 17.7 |
| Other | |||||||||||||
| Provocation | NAS-PI | 51.4 | 11.8 | 48.3 | 14.0 | 50.0 | 15.9 | 51.0 | 13.2 | 49.7 | 14.0 | 48.2 | 13.6 |
| Impulsivity—total | BIS-11 | 63.5 | 11.5 | 59.1 | 11.2 | 59.9 | 11.8 | 62.9 | 12.1 | 62.9 | 10.7 | 59.5 | 12.6 |
| Motor | BIS-11 | 22.8 | 4.3 | 20.9 | 3.8 | 21.2 | 4.3 | 22.1 | 4.8 | 21.6 | 4.5 | 20.4 | 5.2 |
| Cognition | BIS-11 | 15.7 | 3.6 | 14.9 | 4.1 | 15.1 | 3.6 | 15.9 | 4.4 | 16.1 | 3.8 | 15.4 | 4.4 |
| Non-planning | BIS-11 | 25.0 | 5.6 | 23.3 | 5.3 | 23.6 | 5.3 | 24.8 | 5.3 | 25.1 | 5.1 | 23.9 | 5.2 |
| Hostile interpretation bias | HIBT | 133.6 | 76.7 | 123.7 | 63.9 | 131.9 | 70.8 | 143.6 | 75.1 | 145.0 | 75.7 | 132.9 | 69.6 |
| Pre-Post | Pre-Follow-up | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| b | t | df | p | 95% CI | Effect size | b | t | df | p | 95% CI | Effect size | ||||
| Instrument | |||||||||||||||
| Staff-rated | |||||||||||||||
| Peak aggression (primary outcome) | SDAS | 0.15 | 0.27 | 127.3 | 0.79 | −0.98 | 1.29 | 0.05 | −0.01 | −0.02 | 125.1 | 0.98 | −0.60 | 0.59 | 0 |
| General aggression | SDAS | −0.08 | −0.17 | 127.5 | 0.87 | −0.97 | 0.82 | 0.03 | −0.08 | −0.30 | 125.9 | 0.76 | −0.58 | 0.43 | 0.05 |
| Aggression | |||||||||||||||
| Aggression—total (primary outcome) | AVL | 0.18 | 0.06 | 99.8 | 0.95 | −5.63 | 5.99 | 0.02 | −1.70 | −1.10 | 98.9 | 0.27 | −4.77 | 1.37 | 0.19 |
| Physical aggression | AVL | −0.77 | −0.55 | 103.1 | 0.58 | −3.55 | 2.01 | 0.11 | −0.63 | −0.80 | 104.0 | 0.42 | −2.18 | 0.92 | 0.15 |
| Verbal aggression | AVL | 0.05 | 0.10 | 101.7 | 0.92 | −0.99 | 1.10 | 0.01 | −0.35 | −1.23 | 102.2 | 0.22 | −0.92 | 0.22 | 0.26 |
| Anger | AVL | 0.52 | 0.67 | 100.8 | 0.51 | −1.03 | 2.08 | 0.12 | 0.13 | 0.34 | 98.9 | 0.73 | −0.63 | 0.89 | 0.07 |
| Hostility | AVL | 0.50 | 0.42 | 99.6 | 0.67 | −1.85 | 2.85 | 0.12 | −0.86 | −1.57 | 97.7 | 0.12 | −1.94 | 0.23 | 0.28 |
| Reactive and proactive aggression—total | RPQ | −0.23 | −0.12 | 102.7 | 0.90 | −3.96 | 3.50 | 0.37 | 0.40 | 0.42 | 102.2 | 0.68 | −1.49 | 2.28 | 0.05 |
| Proactive aggression | RPQ | −0.12 | −0.12 | 100.3 | 0.91 | −2.15 | 1.92 | 0.09 | 0.14 | 0.28 | 99.9 | 0.78 | −0.85 | 1.14 | 0 |
| Reactive aggression | RPQ | −0.08 | −0.08 | 105.3 | 0.93 | −2.02 | 1.86 | 0.03 | 0.30 | 0.59 | 104.5 | 0.56 | −0.70 | 1.30 | 0.12 |
| Aggression and hostility—total | BDHI_D | 2.74 | 2.38 | 99.8 | 0.02 * | 0.45 | 5.02 | 0.44 | 0.12 | 0.22 | 96.2 | 0.83 | −0.97 | 1.20 | 0.02 |
| Direct aggression | BDHI_D | 1.17 | 2.05 | 99.0 | 0.04 * | 0.04 | 2.31 | 0.38 | 0.30 | 1.04 | 97.5 | 0.30 | −0.27 | 0.87 | 0.18 |
| Indirect aggression | BDHI_D | 1.66 | 1.94 | 102.5 | 0.06 | −0.04 | 3.36 | 0.32 | −0.08 | −0.21 | 96.2 | 0.83 | −0.82 | 0.66 | 0.08 |
| Social desirability | BDHI_D | −0.09 | −0.34 | 102.8 | 0.74 | −0.61 | 0.43 | 0 | −0.11 | −0.83 | 99.5 | 0.41 | −0.36 | 0.15 | 0.12 |
| Anger | |||||||||||||||
| State anger | STAXI-2 | 1.13 | 0.81 | 98.0 | 0.42 | −1.64 | 3.90 | 0.16 | −0.59 | −0.78 | 104.1 | 0.44 | −2.09 | 0.91 | 0.10 |
| Trait anger | STAXI-2 | 0.99 | 1.26 | 101.2 | 0.21 | −0.56 | 2.54 | 0.25 | −0.26 | −0.63 | 99.5 | 0.53 | −1.09 | 0.56 | 0.14 |
| Anger expression—Out | STAXI-2 | 1.32 | 1.76 | 101.5 | 0.08 | −0.17 | 2.81 | 0.33 | 0.36 | 0.95 | 98.3 | 0.34 | −0.39 | 1.10 | 0.18 |
| Anger expression—In | STAXI-2 | −0.11 | −0.17 | 101.8 | 0.86 | −1.37 | 1.15 | 0.03 | −0.54 | −1.54 | 100.5 | 0.13 | −1.23 | 0.15 | 0.28 |
| Anger control—Out | STAXI-2 | −1.76 | −2.40 | 96.7 | 0.02 * | −3.22 | −0.30 | 0.48 | −0.40 | −0.91 | 94.8 | 0.36 | −1.26 | 0.47 | 0.16 |
| Anger control—In | STAXI-2 | −1.38 | −1.46 | 102.8 | 0.15 | −3.26 | 0.50 | 0.25 | −0.67 | −1.40 | 100.3 | 0.16 | −1.61 | 0.28 | 0.23 |
| Anger expression index | STAXI-2 | 4.41 | 2.21 | 98.1 | 0.03 * | 0.45 | 8.36 | 0.46 | 0.84 | 0.80 | 94.4 | 0.42 | −1.23 | 2.90 | 0.17 |
| Anger | NAS-PI | 1.21 | 0.53 | 98.9 | 0.60 | −3.33 | 5.75 | 0.07 | −1.11 | −0.95 | 97.1 | 0.34 | −3.44 | 1.21 | 0.23 |
| Other | |||||||||||||||
| Provocation | NAS-PI | 1.85 | 1.06 | 98.3 | 0.29 | −1.60 | 5.31 | 0.23 | −0.88 | −0.99 | 96.1 | 0.33 | −2.65 | 0.89 | 0.20 |
| Impulsivity—total | BIS-11 | 3.43 | 1.77 | 100.4 | 0.08 | −0.41 | 7.27 | 0.30 | −0.23 | −0.26 | 97.3 | 0.80 | −2.02 | 1.55 | 0.08 |
| Motor | BIS-11 | 1.11 | 1.34 | 99.1 | 0.18 | −0.53 | 2.76 | 0.21 | −0.20 | −0.49 | 98.1 | 0.63 | −1.03 | 0.62 | 0.15 |
| Cognition | BIS-11 | 0.73 | 0.96 | 103.0 | 0.34 | −0.77 | 2.23 | 0.14 | 0.02 | 0.05 | 99.3 | 0.96 | −0.66 | 0.69 | 0.01 |
| Non-planning | BIS-11 | 1.59 | 2.07 | 99.3 | 0.04 * | 0.06 | 3.12 | 0.39 | 0.08 | 0.20 | 97.6 | 0.84 | −0.68 | 0.83 | 0.03 |
| Hostile interpretation bias | HIBT | 10.93 | 0.93 | 76.3 | 0.36 | −12.57 | 34.43 | 0.18 | −5.99 | −0.88 | 73.2 | 0.38 | −19.62 | 7.64 | 0.27 |
| Question | Answers | n (%) |
|---|---|---|
| Did you work on your learning goals? | Yes | 26 (68.4%) |
| No, or not really | 7 (18.4%) | |
| Don’t know | 5 (13.2%) | |
| Do you notice a difference in your daily life? | Yes | 19 (50%) |
| A little | 3 (7.9%) | |
| No, or not really | 16 (42.1%) | |
| Is this therapy an addition to other therapies? | Yes | 29 (76.3%) |
| No, or not really | 4 (10.5%) | |
| Not for me personally, but for other patients | 5 (13.2%) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klein Tuente, S.; Bogaerts, S.; Bulten, E.; Keulen-de Vos, M.; Vos, M.; Bokern, H.; IJzendoorn, S.v.; Geraets, C.N.W.; Veling, W. Virtual Reality Aggression Prevention Therapy (VRAPT) versus Waiting List Control for Forensic Psychiatric Inpatients: A Multicenter Randomized Controlled Trial. J. Clin. Med. 2020, 9, 2258. https://doi.org/10.3390/jcm9072258
Klein Tuente S, Bogaerts S, Bulten E, Keulen-de Vos M, Vos M, Bokern H, IJzendoorn Sv, Geraets CNW, Veling W. Virtual Reality Aggression Prevention Therapy (VRAPT) versus Waiting List Control for Forensic Psychiatric Inpatients: A Multicenter Randomized Controlled Trial. Journal of Clinical Medicine. 2020; 9(7):2258. https://doi.org/10.3390/jcm9072258
Chicago/Turabian StyleKlein Tuente, Stéphanie, Stefan Bogaerts, Erik Bulten, Marije Keulen-de Vos, Maarten Vos, Hein Bokern, Sarah van IJzendoorn, Chris N. W. Geraets, and Wim Veling. 2020. "Virtual Reality Aggression Prevention Therapy (VRAPT) versus Waiting List Control for Forensic Psychiatric Inpatients: A Multicenter Randomized Controlled Trial" Journal of Clinical Medicine 9, no. 7: 2258. https://doi.org/10.3390/jcm9072258