1. Introduction
In 2018, an estimated 1.3 million new cases of prostate cancer and 359,000 associated deaths occurred worldwide, making it the second most frequent cancer and fifth leading cause of cancer death in men [
1]. Androgen deprivation therapy (ADT) is used to improve prognosis, and its efficacy in combination with standard radiation therapy up to 70 Gy has been confirmed by several randomized controlled trials (RCTs) [
2,
3]. However, in modern radiotherapy, wherein higher doses of ≥74 Gy can be delivered, there is little evidence to support the role of additional ADT [
3,
4]. Furthermore, as ADT causes several untoward effects such as diabetes and cardiovascular toxicity, physicians should employ meticulous caution while treating fragile patients [
5,
6], including the elderly, to prevent other-cause mortality (OCM), i.e., death due to causes other than prostate cancer [
5,
6]. Recently, the outcomes of prostate cancer treatment have improved, and a nearly 100% prostate cancer-specific relative survival rate has been achieved [
3,
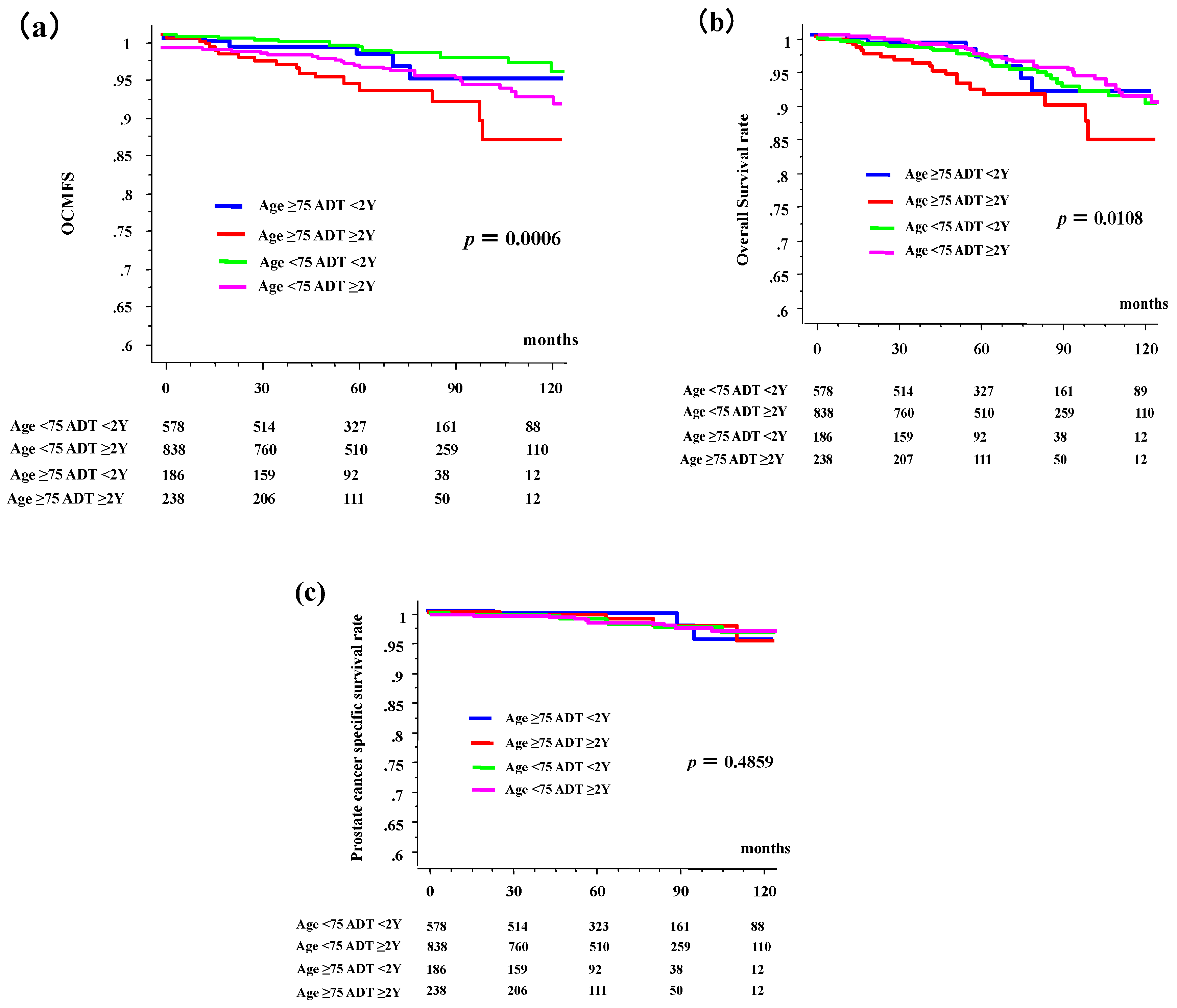
7]; therefore, the simultaneous importance of OCM has increased. Previously, we unexpectedly found that long-term ADT ≥ 2 years increases the risk of OCM in patients aged ≥75 years in a study on 1125 patients with localized prostate cancer treated with modern high-dose RT including low-dose-rate brachytherapy [
8]. The 10-year OCM-free survival (OCMFS) rates in patients aged ≥75 years were 86.8% and 60.7% in the <2- and ≥2-year ADT groups, respectively, whereas they were 90.0% and 86.8% (
p < 0.0001) in their younger counterparts. Furthermore, overall survival (OS) was also poorest in elderly patients who received ADT for ≥2 years [
8]. This unexpected previous finding prompted us to conducted a confirmation study using different databases open for public use that included >1800 patients with clinically localized prostate cancer treated with RT including high does rate brachytherapy (HDR) [
9]. Therefore, this study aimed to examine the influence of long-term ADT, according to age, on survival after radiotherapy.
4. Discussion
We present evidence that ADT does not always improve survival outcomes after RT for patients with localized prostate cancer. In fact, long-term ADT for ≥2 years has a negative effect on OCM and OS, especially in elderly patients aged ≥75 years [
8], which was reported in a previous cohort and confirmed in this study. The strength of this study is that large cohorts were used, including >1000 patients, in both a previous experimental arm [
8] and this confirmation arm.
Generally, ADT has been recognized as an important intervention in the management of prostate cancer. Huggins and Hodges [
11,
12] initialized a successful ADT strategy in the early 1940s in which castration arrested the growth of prostate cancer cells and suppressed serum prostate phosphatases in metastatic prostate cancer cells. Several RCTs confirmed that simultaneous RT with ADT is a useful treatment for high-risk prostate cancer with RT doses of up to 70 Gy [
2,
3,
4]. Modern technical advancement in RT enabled us to increase the irradiation dose to the target area without administering unnecessary higher doses to the surrounding normal tissue, which improved the outcome of localized prostate cancer RT; modern high-dose RT (e.g., IMRT and BT) combined with ADT is recognized as the standard treatment for locally advanced and/or intermediate- to high-risk disease [
3,
4]. However, there is little evidence to support these combinations of higher-dose RT ≥ 74 Gy and/or BT. Furthermore, the optimum duration of ADT with higher-dose RT is yet to be determined [
3,
4,
13].
It is often said that most men with prostate cancer will die with the disease rather than of the disease because the prostate cancer-specific survival rate has improved [
1,
3,
7,
8]. Our data confirmed this tenet, because most men died of causes other than prostate cancer, and long-term ADT ≥2 years worsened not only OCM but also OS. Several adverse effects of ADT have been reported: 5 weight gain, decreased muscle mass and increased insulin resistance, decreased bone mineral density, decreased libido and sexual dysfunction, hot flashes, gynecomastia, reduced testicle size, anemia, fatigue, diabetes, cardiovascular events (myocardial infarction [MI] and sudden cardiac death) [
14,
15], cerebrovascular diseases [
15], kidney injury [
16], dementia [
17], and thromboembolic events [
18,
19]. Abdollah et al., in their study including 137,524 patients with non-metastatic prostate cancer treated between 1995 and 2009, reported that treatment with medical ADT may increase the risk of OCM [
6]. Morgans et al. cited the importance of age because they speculated that the risk of incident diabetes mellitus (DM) or cardiovascular disease in men exposed to long-term ADT for ≥2 years increases with age at diagnosis, especially in those ≥75 years [
20]. In contrast, most studies, including a meta-analysis of RCTs, reported that ADT is not related to greater cardiovascular mortality [
3,
5].
Several studies describe the negative effects of ADT after RT [
21,
22,
23]. Beyer et al. found a poorer 10-year OS rate that decreased from 44% in hormone-naïve patients receiving low dose rate BT (LDR-BT) to 20% in patients receiving ADT and under treatment with LDR-BT, with the leading causes of death being cardiovascular death and prostate and other cancers [
21]. This finding was confirmed by other studies. Nanda reported that neoadjuvant ADT is significantly associated with an increased risk of all-cause mortality among men with a history of coronary artery disease (CAD), CAD-induced chronic heart failure, or MI who are treated with LDR-BT but not among men with no comorbidity or a single CAD risk factor [
22]. Pickles et al. also confirmed increased cardiovascular death rates after LDR-BT in intermediate-risk patients treated with ADT [
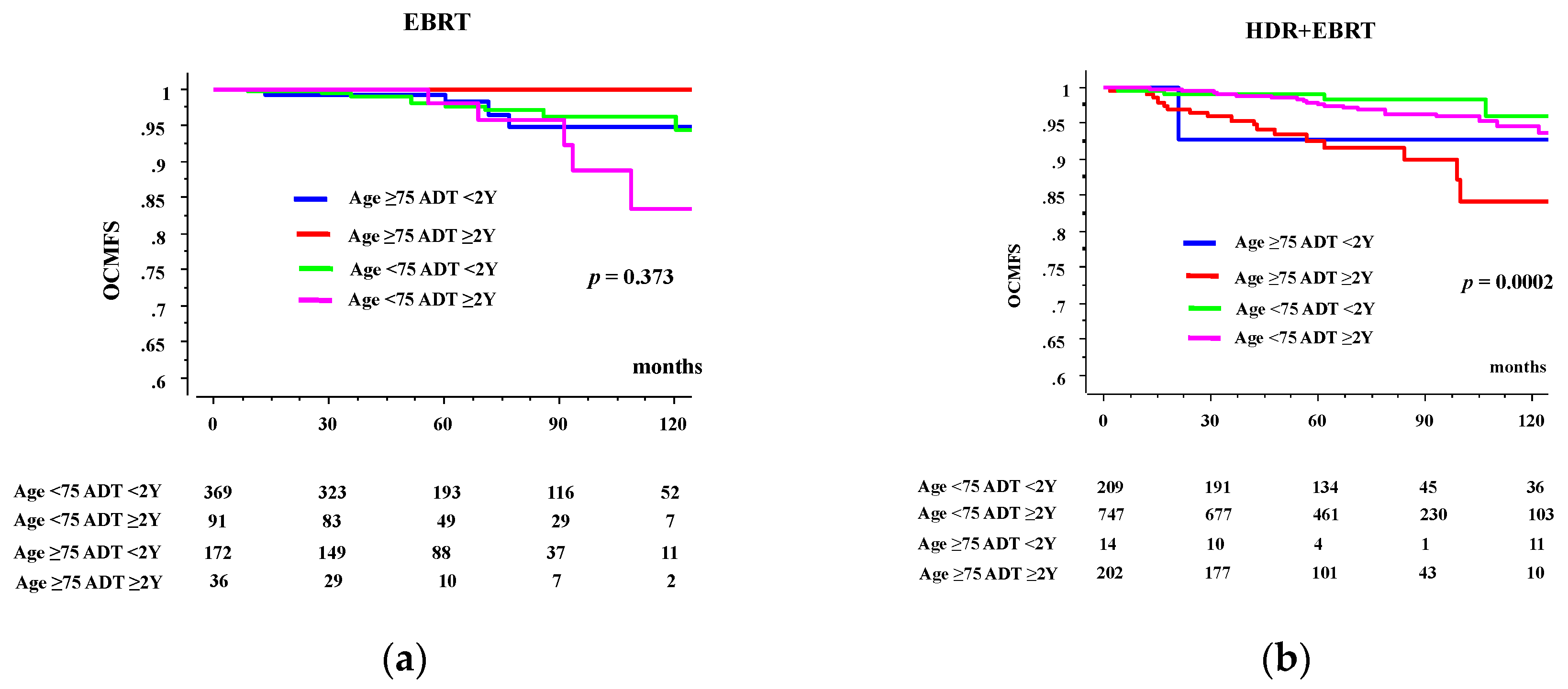
23]. Our findings are in line with these results. Especially, in comparison between EBRT and brachytherapy, we found that negative effect of long-term ADT was only found in HDR-BT group, and the strength of this study is that we examined the effect of ADT on OCM in patients treated with modern RT with a high biologically effective dose, focusing on age.
In this decade, only few patients with localized prostate cancer died of prostate cancer. Therefore, we consider this an important finding not only for radiation oncologists but also for general healthcare practitioners. Whether this is a simple association or a cause–effect relationship is unknown. At least, our data raise a question to longer-term ADT use in elderly patients without evidence, which should be performed with meticulous care.
This study remains several limitations. The primary limitation of this study is its retrospective design and inherent selection bias associated with treatment being as rendered. A longer follow-up with a larger number of homogenous patients is needed before establishing concrete conclusions. Further, a comorbidity analysis was lacking, including geriatric assessment (i.e., Geriatric 8 Score proposed by SIOP), and this is important because DM and cardiovascular diseases are confirmed important factors influencing OCM [
8,
14,
15,
20,
22]. Additionally, the lack of serum testosterone measurements could be a concern since many older men will have a prolonged recovery time after 2 years of ADT. Therefore, this study could not examine the role of preventive measures or targeted intervention. Finally, the reason for OCM could not be specified; it is not always the cardiovascular system and is mainly other cancers. The hypothesis explains the mechanism of unexpected OCM is required to mitigate toxicity.
In conclusion, long-term ADT for ≥2 years is correlated with a risk of mortality due to causes other than prostate cancer, in patients with localized prostate cancer aged ≥75 years.

 ,
, 




{kind=link}
{kind=link}