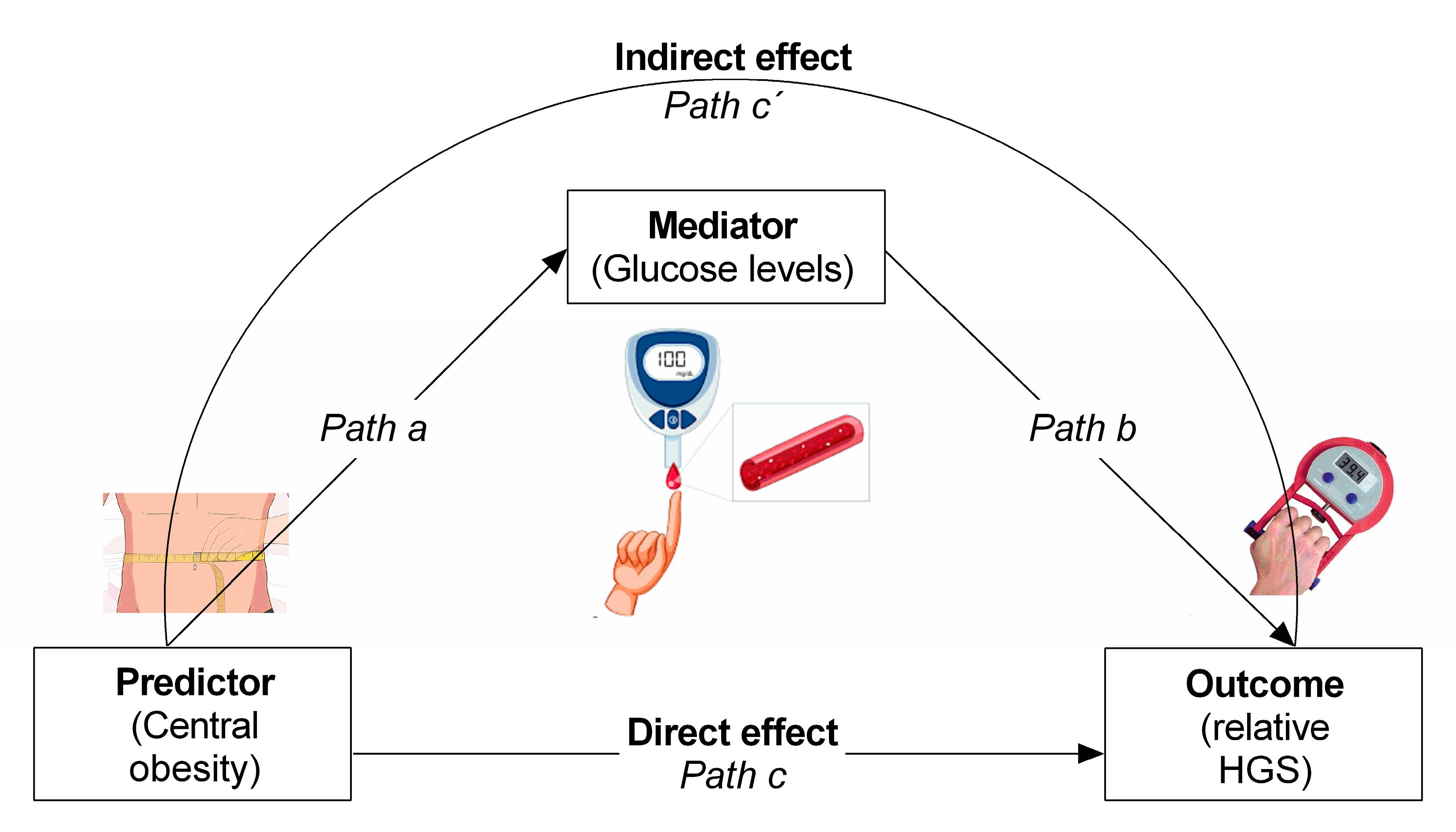
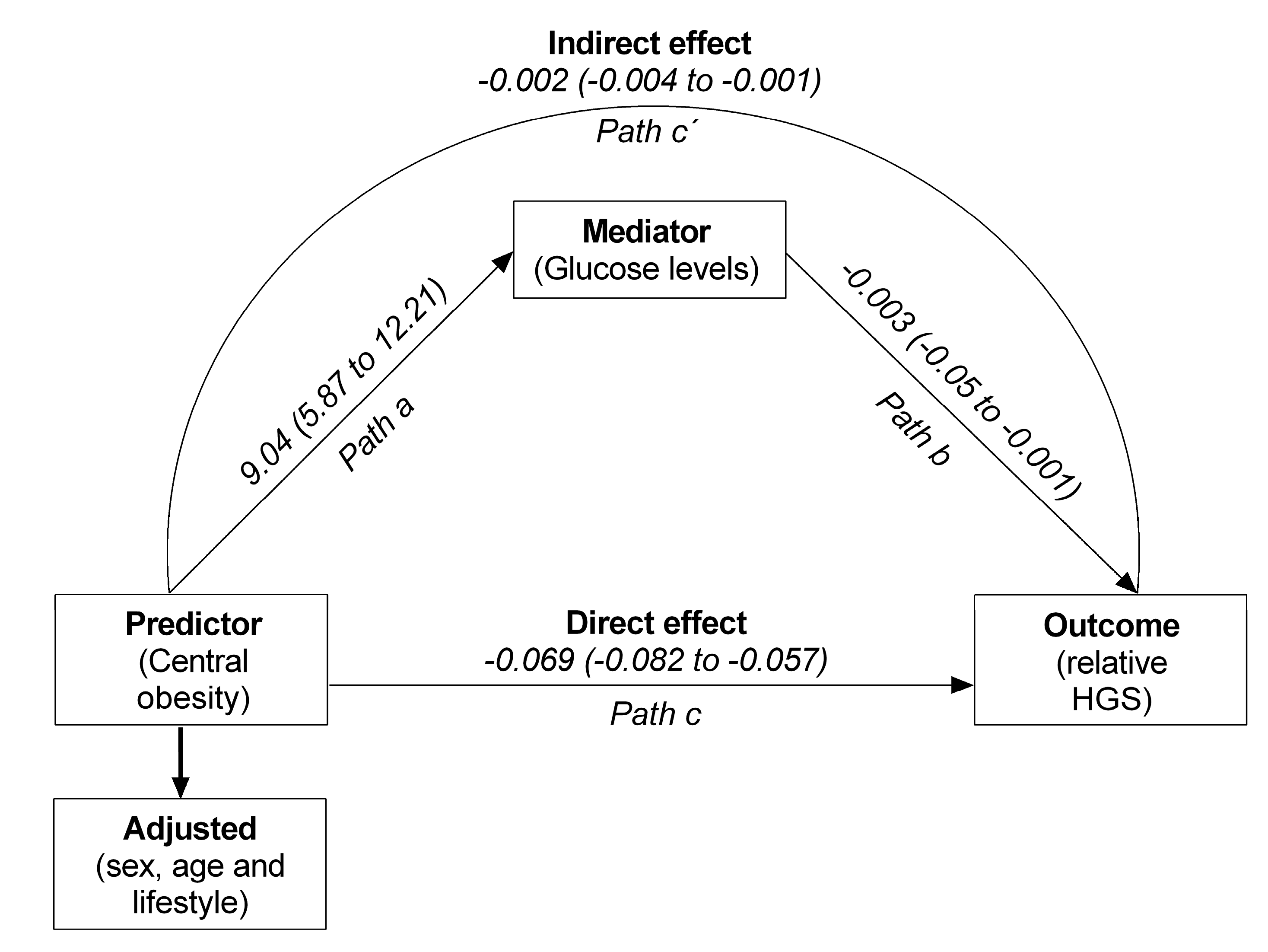
Glucose Levels as a Mediator of the Detrimental Effect of Abdominal Obesity on Relative Handgrip Strength in Older Adults

 ,
,  , , ,
, , ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sample Population
2.2. Measurements
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Newman, A.B.; Lee, J.S.; Visser, M.; Goodpaster, B.H.; Kritchevsky, S.B.A.; Tylavsky, F.; Nevitt, M.; Harris, T.B. Weight change and the conservation of lean mass in old age: The Health, Aging and Body Composition Study. Am. J. Clin. Nutr. 2005, 82, 872–878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villareal, D.T.; Apovian, C.M.; Kushner, R.F.; Klein, S. Obesity in Older Adults: Technical Review and Position Statement of the American Society for Nutrition and NAASO, The Obesity Society. Obes. Res. 2005, 13, 1849–1863. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.-C.; James, W.P.T.; Loria, C.M.; Smith, S.C. Harmonizing the Metabolic Syndrome: A Joint Interim Statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westphal, S.A. Obesity, Abdominal Obesity, and Insulin Resistance. Clin. Cornerstone 2008, 9, 23–31. [Google Scholar] [CrossRef]
- Ramírez-Vélez, R.; Perez-Sousa, M.A.; González-Ruíz, K.; Cano-Gutiérrez, C.A.; Schmidt-RioValle, J.; Correa-Rodríguez, M.; Izquierdo, M.; Romero-García, J.A.; Campos-Rodríguez, A.Y.; Triana-Reina, H.R.; et al. Obesity- and Lipid-Related Parameters in the Identification of Older Adults with a High Risk of Prediabetes According to the American Diabetes Association: An Analysis of the 2015 Health, Well-Being, and Aging Study. Nutrients 2019, 11, 2654. [Google Scholar] [CrossRef] [Green Version]
- Meisinger, C.; Döring, A.; Thorand, B.; Heier, M.; Löwel, H. Body fat distribution and risk of type 2 diabetes in the general population: Are there differences between men and women? The MONICA/KORA Augsburg cohort study. Am. J. Clin. Nutr. 2006, 84, 483–489. [Google Scholar] [CrossRef] [Green Version]
- Jura, M.; Kozak, L.P. Obesity and related consequences to ageing. Age 2016, 38. [Google Scholar] [CrossRef] [Green Version]
- De Carvalho, D.H.T.; Scholes, S.; Santos, J.L.F.; De Oliveira, C.; Alexandre, T.D.S. Does Abdominal Obesity Accelerate Muscle Strength Decline in Older Adults? Evidence From the English Longitudinal Study of Ageing. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2019, 74, 1105–1111. [Google Scholar] [CrossRef] [Green Version]
- Lee, P.G.; Halter, J.B. The Pathophysiology of Hyperglycemia in Older Adults: Clinical Considerations. Diabetes Care 2017, 40, 444–452. [Google Scholar] [CrossRef] [Green Version]
- Ohlendieck, K. Pathobiochemical Changes in Diabetic Skeletal Muscle as Revealed by Mass-Spectrometry-Based Proteomics. J. Nutr. Metab. 2012, 2012, 1–12. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Status Report on Noncommunicable Diseases; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Chamberlain, J.J.; Rhinehart, A.S.; Shaefer, C.F.; Neuman, A. Diagnosis and Management of Diabetes: Synopsis of the 2016 American Diabetes Association Standards of Medical Care in Diabetes. Ann. Intern. Med. 2016, 164, 542. [Google Scholar] [CrossRef] [PubMed]
- Cho, N.H.; Shaw, J.; Karuranga, S.; Huang, Y.; Fernandes, J.D.D.R.; Ohlrogge, A.; Malanda, B. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res. Clin. Pr. 2018, 138, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Tramunt, B.; Smati, S.; Grandgeorge, N.; Lenfant, F.; Arnal, J.-F.; Montagner, A.; Gourdy, P. Sex differences in metabolic regulation and diabetes susceptibility. Diabetology 2019, 63, 453–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bohannon, R.W. Grip Strength: An Indispensable Biomarker for Older Adults. Clin. Interv. Aging 2019, 14, 1681–1691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, W.-J.; Peng, L.-N.; Chiou, S.-T.; Chen, L.-K. Relative Handgrip Strength Is a Simple Indicator of Cardiometabolic Risk among Middle-Aged and Older People: A Nationwide Population-Based Study in Taiwan. PLoS ONE 2016, 11, e0160876. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chun, S.-W.; Kim, W.; Choi, K.H. Comparison between grip strength and grip strength divided by body weight in their relationship with metabolic syndrome and quality of life in the elderly. PLoS ONE 2019, 14, e0222040. [Google Scholar] [CrossRef]
- Peterson, M.D.; McGrath, R.; Zhang, P.; Markides, K.S.; Al Snih, S.; Wong, R. Muscle Weakness Is Associated With Diabetes in Older Mexicans: The Mexican Health and Aging Study. J. Am. Med. Dir. Assoc. 2016, 17, 933–938. [Google Scholar] [CrossRef] [Green Version]
- McGrath, R.; Vincent, B.M.; Al Snih, S.; Markides, K.S.; Peterson, M.D. The Association between Muscle Weakness and Incident Diabetes in Older Mexican Americans. J. Am. Med. Dir. Assoc. 2017, 18, 452.e7–452.e12. [Google Scholar] [CrossRef] [Green Version]
- Li, J.J.; Wittert, G.; Vincent, A.; Atlantis, E.; Shi, Z.; Appleton, S.L.; Hill, C.L.; Jenkins, A.J.; Januszewski, A.S.; Adams, R.J. Muscle grip strength predicts incident type 2 diabetes: Population-based cohort study. Metabolism 2016, 65, 883–892. [Google Scholar] [CrossRef]
- Lee, M.-R.; Jung, S.M.; Bang, H.; Kim, H.S.; Kim, Y.B. Association between muscle strength and type 2 diabetes mellitus in adults in Korea. Med. 2018, 97, e10984. [Google Scholar] [CrossRef]
- Corriere, M.; Rooparinesingh, N.; Kalyani, R.R. Epidemiology of diabetes and diabetes complications in the elderly: an emerging public health burden. Curr. Diabetes Rep. 2013, 13, 805–813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nwose, E.U.; Richards, R.S.; Bwititi, P.; Igumbor, E.O.; Oshionwu, E.J.; Okolie, K.; Onyia, I.C.; Pokhrel, A.; Gyawali, P.; Okuzor, J.N.; et al. Prediabetes and cardiovascular complications study (PACCS): international collaboration 4 years’ summary and future direction. BMC Res. Notes 2017, 10, 730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Agtmaal, M.J.; Houben, A.J.; De Wit, V.; Henry, R.M.; Schaper, N.C.; Dagnelie, P.C.; Van Der Kallen, C.J.; Koster, A.; Sep, S.J.; Kroon, A.A.; et al. Prediabetes Is Associated With Structural Brain Abnormalities: The Maastricht Study. Diabetes Care 2018, 41, 2535–2543. [Google Scholar] [CrossRef] [Green Version]
- Mizgier, M.L.; Casas, M.; Contreras-Ferrat, A.; Llanos, P.; Galgani, J.E. Potential role of skeletal muscle glucose metabolism on the regulation of insulin secretion. Obes. Rev. 2014, 15, 587–597. [Google Scholar] [CrossRef] [PubMed]
- Oberbach, A.; Bossenz, Y.; Lehmann, S.; Niebauer, J.; Adams, V.; Paschke, R.; Schön, M.R.; Blüher, M.; Punkt, K. Altered Fiber Distribution and Fiber-Specific Glycolytic and Oxidative Enzyme Activity in Skeletal Muscle of Patients with Type 2 Diabetes. Diabetes Care 2006, 29, 895–900. [Google Scholar] [CrossRef] [Green Version]
- Park, S.W.; Goodpaster, B.H.; Strotmeyer, E.S.; De Rekeneire, N.; Harris, T.B.; Schwartz, A.V.; Tylavsky, F.A.; Newman, A.B. Decreased Muscle Strength and Quality in Older Adults With Type 2 Diabetes: The Health, Aging, and Body Composition Study. Diabetes 2006, 55, 1813–1818. [Google Scholar] [CrossRef] [Green Version]
- Park, S.W.; Goodpaster, B.H.; Strotmeyer, E.S.; Kuller, L.H.; Broudeau, R.; Kammerer, C.M.; De Rekeneire, N.; Harris, T.B.; Schwartz, A.V.; Tylavsky, F.A.; et al. Accelerated Loss of Skeletal Muscle Strength in Older Adults With Type 2 Diabetes: The Health, Aging, and Body Composition Study. Diabetes Care 2007, 30, 1507–1512. [Google Scholar] [CrossRef] [Green Version]
- Giglio, B.M.; Mota, J.F.; Wall, B.T.; Pimentel, G.D. Low Handgrip Strength Is Not Associated with Type 2 Diabetes Mellitus and Hyperglycemia: a Population-Based Study. Clin. Nutr. Res. 2018, 7, 112–116. [Google Scholar] [CrossRef] [Green Version]
- Palacios-Chávez, M.; Dejo-Seminario, C.; Mayta-Tristán, P. Physical performance and muscle strength in older patients with and without diabetes from a public hospital in Lima, Peru. Endocrinol. Nutr. (Engl. Ed.) 2016, 63, 220–229. [Google Scholar] [CrossRef] [Green Version]
- Ramírez-Vélez, R.; Correa-Bautista, J.E.; Garcia-Hermoso, A.; Cano-Gutiérrez, C.A.; Izquierdo, M. Reference values for handgrip strength and their association with intrinsic capacity domains among older adults. J. Cachex—Sarcopenia Muscle 2019, 10, 278–286. [Google Scholar] [CrossRef]
- Mamtani, M.R.; Kulkarni, H.R. Predictive Performance of Anthropometric Indexes of Central Obesity for the Risk of Type 2 Diabetes. Arch. Med Res. 2005, 36, 581–589. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988. [Google Scholar]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Publications: New York, NY, USA, 2017. [Google Scholar]
- Ross, R.; Neeland, I.J.; Yamashita, S.; Shai, I.; Seidell, J.; Magni, P.; Santos, R.D.; Arsenault, B.; Cuevas, A.; Hu, F.B.; et al. Waist circumference as a vital sign in clinical practice: a Consensus Statement from the IAS and ICCR Working Group on Visceral Obesity. Nat. Rev. Endocrinol. 2020, 16, 177–189. [Google Scholar] [CrossRef] [PubMed]
- Freemantle, N.; Holmes, J.; Hockey, A.; Kumar, S. How strong is the association between abdominal obesity and the incidence of type 2 diabetes? Int. J. Clin. Pr. 2008, 62, 1391–1396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Rimm, E.B.; Stampfer, M.J.; Willett, W.C.; Hu, F.B. Comparison of abdominal adiposity and overall obesity in predicting risk of type 2 diabetes among men. Am. J. Clin. Nutr. 2005, 81, 555–563. [Google Scholar] [CrossRef] [Green Version]
- Son, Y.J.; Kim, J.; Park, H.-J.; Park, S.E.; Park, C.-Y.; Lee, W.-Y.; Oh, K.-W.; Park, S.-W.; Rhee, E.-J. Association of Waist-Height Ratio with Diabetes Risk: A 4-Year Longitudinal Retrospective Study. Endocrinol. Metab. 2016, 31, 127–133. [Google Scholar] [CrossRef] [Green Version]
- WHO. WHO Guidelines on Integrated Care for Older People (ICOPE); WHO: Geneva, Switzerland, 2019. [Google Scholar]
- Dodds, R.; Kuh, D.; Sayer, A.A.; Cooper, R. Physical activity levels across adult life and grip strength in early old age: Updating findings from a British birth cohort. Age Ageing 2013, 42, 794–798. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.X.; Yao, J.; Zirek, Y.; Reijnierse, E.M.; Maier, A.B. Muscle mass, strength, and physical performance predicting activities of daily living: A meta-analysis. J. Cachex- Sarcopenia Muscle 2019, 11, 3–25. [Google Scholar] [CrossRef] [Green Version]
- Çetinus, E.; Buyukbese, M.A.; Üzel, M.; Ekerbiçer, H.; Karaoguz, A. Hand grip strength in patients with type 2 diabetes mellitus. Diabetes Res. Clin. Pr. 2005, 70, 278–286. [Google Scholar] [CrossRef]
- Peterson, M.D.; Duchowny, K.; Meng, Q.; Wang, Y.; Chen, X.; Zhao, Y. Low Normalized Grip Strength is a Biomarker for Cardiometabolic Disease and Physical Disabilities Among U.S. and Chinese Adults. Journals Gerontol. Ser. A Boil. Sci. Med. Sci. 2017, 72, 1525–1531. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Hermoso, A.; Carrillo, H.A.; González-Ruíz, K.; Vivas, A.; Triana-Reina, H.R.; Martínez-Torres, J.; Prieto-Benavidez, D.H.; Correa-Bautista, J.E.; Ramos-Sepúlveda, J.A.; Villa-González, E.; et al. Fatness mediates the influence of muscular fitness on metabolic syndrome in Colombian collegiate students. PLoS ONE 2017, 12, e0173932. [Google Scholar] [CrossRef]
- Brand, C.; Dias, A.F.; Fochesatto, C.F.; Garcia-Hermoso, A.; Mota, J.; Gaya, A.; Gaya, A.R. The role of body fat in the relationship of cardiorespiratory fitness with cardiovascular risk factors in Brazilian children. Motriz: Revista de Educação Física 2018, 24. [Google Scholar] [CrossRef] [Green Version]
- Bailey, D.P.; Savory, L.A.; Denton, S.J.; Kerr, C.J. The Association Between Cardiorespiratory Fitness and Cardiometabolic Risk in Children is Mediated by Abdominal Adiposity: The HAPPY Study. J. Phys. Act. Heal. 2015, 12, 1148–1152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murai, J.; Nishizawa, H.; Otsuka, A.; Fukuda, S.; Tanaka, Y.; Nagao, H.; Sakai, Y.; Suzuki, M.; Yokota, S.; Tada, H.; et al. Low muscle quality in Japanese type 2 diabetic patients with visceral fat accumulation. Cardiovasc. Diabetol. 2018, 17, 112. [Google Scholar] [CrossRef] [PubMed]
- Al-Sofiani, M.E.; Ganji, S.S.; Kalyani, R.R. Body composition changes in diabetes and aging. J. Diabetes its Complicat. 2019, 33, 451–459. [Google Scholar] [CrossRef] [PubMed]
- Ryan, A.S.; Buscemi, A.; Forrester, L.; Hafer-Macko, C.E.; Ivey, F.M. Atrophy and intramuscular fat in specific muscles of the thigh: Associated weakness and hyperinsulinemia in stroke survivors. Neurorehabilit. Neural Repair 2011, 25, 865–872. [Google Scholar] [CrossRef]
- Barrett-Connor, E.; Ferrara, A. Isolated postchallenge hyperglycemia and the risk of fatal cardiovascular disease in older women and men. The Rancho Bernardo Study. Diabetes Care 1998, 21, 1236–1239. [Google Scholar] [CrossRef]
- Hong, S.; Chang, Y.; Jung, H.-S.; Yun, K.E.; Shin, H.; Ryu, S. Relative muscle mass and the risk of incident type 2 diabetes: A cohort study. PLoS ONE 2017, 12, e0188650. [Google Scholar] [CrossRef] [Green Version]
- Virtanen, K.A.; Lönnroth, P.; Parkkola, R.; Peltoniemi, P.; Asola, M.; Viljanen, T.; Tolvanen, T.; Knuuti, J.; Rönnemaa, T.; Huupponen, R.; et al. Glucose Uptake and Perfusion in Subcutaneous and Visceral Adipose Tissue during Insulin Stimulation in Nonobese and Obese Humans. J. Clin. Endocrinol. Metab. 2002, 87, 3902–3910. [Google Scholar] [CrossRef]
- Dimitriadis, G.; Mitrou, P.; Lambadiari, V.; Maratou, E.; Raptis, S.A. Insulin effects in muscle and adipose tissue. Diabetes Res. Clin. Pr. 2011, 93, S52–S59. [Google Scholar] [CrossRef]
- Shepherd, P.R.; Kahn, B.B. Glucose Transporters and Insulin Action — Implications for Insulin Resistance and Diabetes Mellitus. N. Engl. J. Med. 1999, 341, 248–257. [Google Scholar] [CrossRef]
- Eaton, S.B.; Eaton, S.B. Physical Inactivity, Obesity, and Type 2 Diabetes: An Evolutionary Perspective. Res. Q. Exerc. Sport 2017, 88, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kelley, D.E.; He, J.; Menshikova, E.V.; Ritov, V.B. Dysfunction of mitochondria in human skeletal muscle in type 2 diabetes. Diabetes 2002, 51, 2944–2950. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedersen, B.K. Muscles and their myokines. J. Exp. Boil. 2010, 214, 337–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, J.; Fan, J.; Su, Q.; Yang, Z. Cytokines and Abnormal Glucose and Lipid Metabolism. Front. Endocrinol. 2019, 10, 703. [Google Scholar] [CrossRef] [PubMed]
- Van Der Kooi, A.-L.L.F.; Snijder, M.B.; Peters, R.J.G.; Van Valkengoed, I.G.M. The Association of Handgrip Strength and Type 2 Diabetes Mellitus in Six Ethnic Groups: An Analysis of the HELIUS Study. PLoS ONE 2015, 10, e0137739. [Google Scholar] [CrossRef]
- López-Jaramillo, P.; Cohen, D.D.; Gomez-Arbelaez, D.; Bosch, J.; Dyal, L.; Yusuf, S.; Gerstein, H.C. Association of handgrip strength to cardiovascular mortality in pre-diabetic and diabetic patients: A subanalysis of the ORIGIN trial. Int. J. Cardiol. 2014, 174, 458–461. [Google Scholar] [CrossRef]
- Hamasaki, H.; Kawashima, Y.; Katsuyama, H.; Sako, A.; Goto, A.; Yanai, H. Association of handgrip strength with hospitalization, cardiovascular events, and mortality in Japanese patients with type 2 diabetes. Sci. Rep. 2017, 7, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Leenders, M.; Verdijk, L.B.; Van Der Hoeven, L.; Adam, J.J.; Van Kranenburg, J.; Nilwik, R.; Van Loon, L. Patients With Type 2 Diabetes Show a Greater Decline in Muscle Mass, Muscle Strength, and Functional Capacity With Aging. J. Am. Med. Dir. Assoc. 2013, 14, 585–592. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Full Sample (n = 1571) | Healthy (n = 331) | Abdominal Obesity (n = 1239) | p-Value |
|---|---|---|---|---|
| Age, years | 69.6 (7.3) | 70.5 (8.1) | 69.6 (7.3) | 0.052 |
| Sex, n (%) | ||||
| Females | 943 (60.0) | 108 (32.6) | 835 (67.3) | <0.001 |
| Clinical outcomes, mean (SD) | ||||
| Body mass, kg | 68.3 (11.5) | 55.2 (8.4) | 68.3 (11.5) | <0.001 |
| Height, m | 1.55 (0.08) | 1.59 (0.08) | 1.55 (0.07) | <0.001 |
| BMI, Kg/m2 | 28.9 (4.3) | 22.5 (2.7) | 28.9 (4.3) | <0.001 |
| Waist circumference, cm | 96.1 (9.1) | 79.3 (6.6) | 96.1 (9.1) | <0.001 |
| Glucose fasting, mg/dL | 100.1 (26.3) | 90.4 (18.0) | 100.1 (26.3) | <0.001 |
| Muscular strength, mean (SD) | ||||
| HGS (kg) | 21.1 (8.4) | 22.9 (8.6) | 20.6 (8.2) | <0.001 |
| Relative HGS (kg/kg body mass) | 0.32 (0.12) | 0.41 (0.13) | 0.30 (0.1) | <0.001 |
| Race/ethnic group, n (%) | ||||
| Indigenous | 79 (5.0) | 21 (6.3) | 58 (4.7) | <0.001 |
| Black “mulato” or Afro-Colombian | 125 (8.0) | 32 (9.7) | 93 (7.5) | <0.001 |
| White | 414 (26.4) | 70 (21.1) | 344 (27.7) | <0.001 |
| Others * | 753 (47.9) | 153 (46.2) | 600 (48.4) | <0.001 |
| Missing date | 200 (12.7) | 55 (16.6) | 145 (11.7) | ― |
| Socioeconomic status, n (%) | ||||
| Level I-II (low) | 1138 (72.4) | 247 (74.6) | 891 (71.9) | <0.001 |
| Level III-IV (middle) | 424 (27.0) | 83 (25.1) | 341 (27.5) | <0.001 |
| Level V-VI (high) | 9 (0.6) | 1 (0.3) | 8 (0.6) | 0.020 |
| Lifestyle outcomes, n (%) | ||||
| Smoking | 152 (9.7) | 56 (16.9) | 96 (7.7) | 0.001 |
| Alcohol intake | 203 (12.9) | 59 (17.9) | 144 (11.6) | <0.001 |
| Physical activity “proxy” | 1278 (81.3) | 261 (78.9) | 1017 (82.2) | <0.001 |
| Urbanicity, n (%) | ||||
| Urban | 1311 (83.5) | 247 (74.6) | 1064 (85.8) | <0.001 |
| Rural | 260 (16.5) | 84 (25.4) | 176 (14.2) | <0.001 |
| Variables | Model 1 | Model 2 | Model 3 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Healthy | Abdominal Obesity | d | Healthy | Abdominal Obesity | d | Healthy | Abdominal Obesity | d | |
| Glucose levels (mg/dl) | 90.5 (87.8; 93.3) | 100.0 (98.6; 101.4) | 0.38 * | 90.9 (88.1; 93.7) | 99.9 (98.5; 101.3) | 0.36 * | 90.9 (87.8; 94.0) | 100.1 (98.5; 101.5) | 0.36 * |
| Relative HSG (kg/kg) | 0.38 (0.37; 0.39) | 0.30 (0.29; 0.31) | 0.65 * | 0.38 (0.37; 0.39) | 0.31 (0.30; 0.32) | 0.63 * | 0.38 (0.37; 0.39) | 0.31 (0.30; 0.32) | 0.62 * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Sousa, M.Á.; del Pozo-Cruz, J.; Cano-Gutiérrez, C.A.; Ferrebuz, A.J.; Sandoval-Cuellar, C.; Izquierdo, M.; Hernández-Quiñonez, P.A.; Ramírez-Vélez, R. Glucose Levels as a Mediator of the Detrimental Effect of Abdominal Obesity on Relative Handgrip Strength in Older Adults. J. Clin. Med. 2020, 9, 2323. https://doi.org/10.3390/jcm9082323
Pérez-Sousa MÁ, del Pozo-Cruz J, Cano-Gutiérrez CA, Ferrebuz AJ, Sandoval-Cuellar C, Izquierdo M, Hernández-Quiñonez PA, Ramírez-Vélez R. Glucose Levels as a Mediator of the Detrimental Effect of Abdominal Obesity on Relative Handgrip Strength in Older Adults. Journal of Clinical Medicine. 2020; 9(8):2323. https://doi.org/10.3390/jcm9082323
Chicago/Turabian StylePérez-Sousa, Miguel Ángel, Jesús del Pozo-Cruz, Carlos A. Cano-Gutiérrez, Atilio J. Ferrebuz, Carolina Sandoval-Cuellar, Mikel Izquierdo, Paula A. Hernández-Quiñonez, and Robinson Ramírez-Vélez. 2020. "Glucose Levels as a Mediator of the Detrimental Effect of Abdominal Obesity on Relative Handgrip Strength in Older Adults" Journal of Clinical Medicine 9, no. 8: 2323. https://doi.org/10.3390/jcm9082323
APA StylePérez-Sousa, M. Á., del Pozo-Cruz, J., Cano-Gutiérrez, C. A., Ferrebuz, A. J., Sandoval-Cuellar, C., Izquierdo, M., Hernández-Quiñonez, P. A., & Ramírez-Vélez, R. (2020). Glucose Levels as a Mediator of the Detrimental Effect of Abdominal Obesity on Relative Handgrip Strength in Older Adults. Journal of Clinical Medicine, 9(8), 2323. https://doi.org/10.3390/jcm9082323