Prediction of Function in ABCA4-Related Retinopathy Using Ensemble Machine Learning

 , , ,
, , ,
Abstract
:1. Introduction
2. Experimental Section
2.1. Subjects
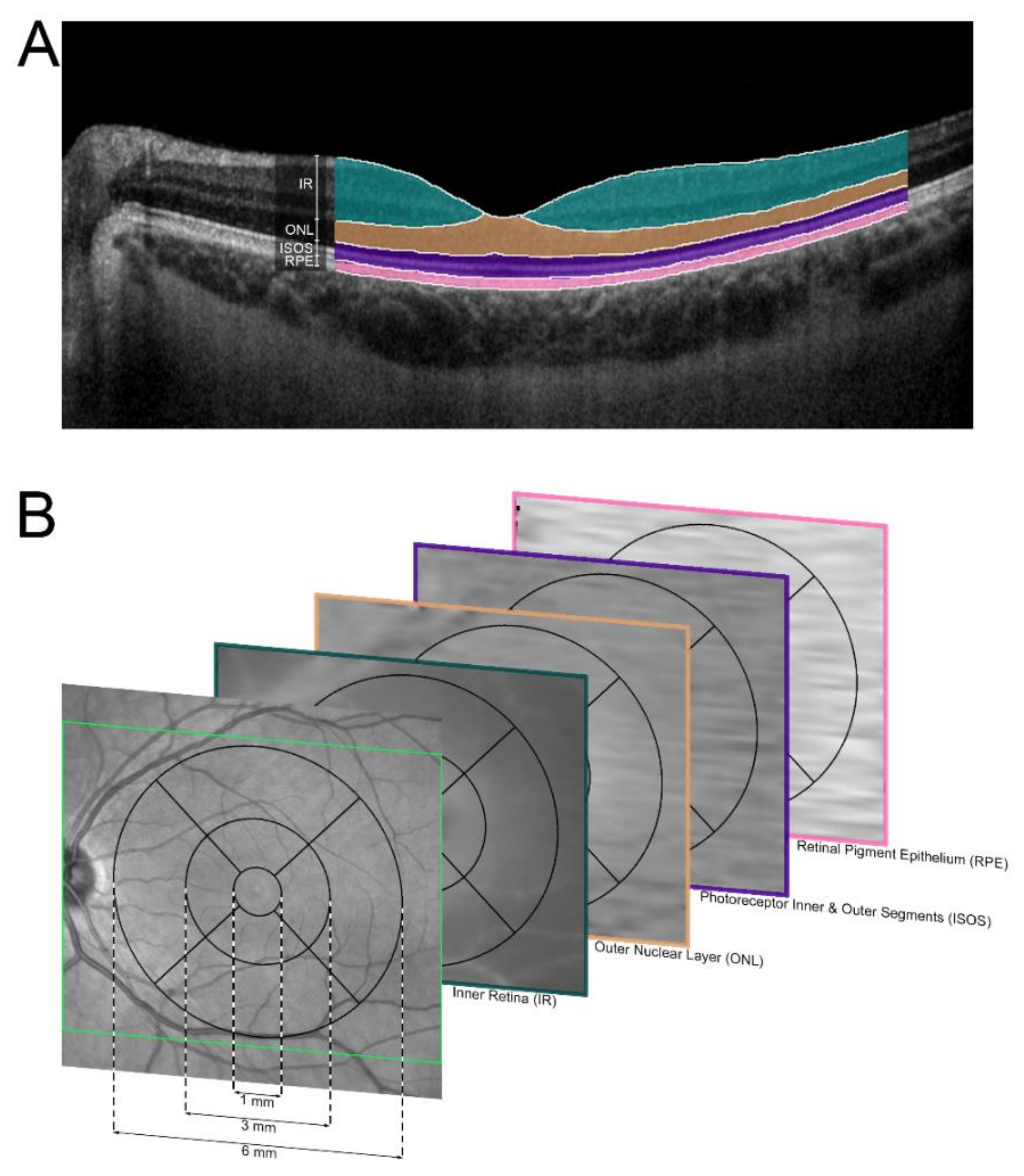
2.2. Imaging and Functional Testing
2.3. Classification
2.4. Machine Learning Analysis
2.5. Statistical Analysis
3. Results
3.1. Cohort Characteristics
3.2. Retinal Layer Thickness
3.3. Prediction of Panretinal Function
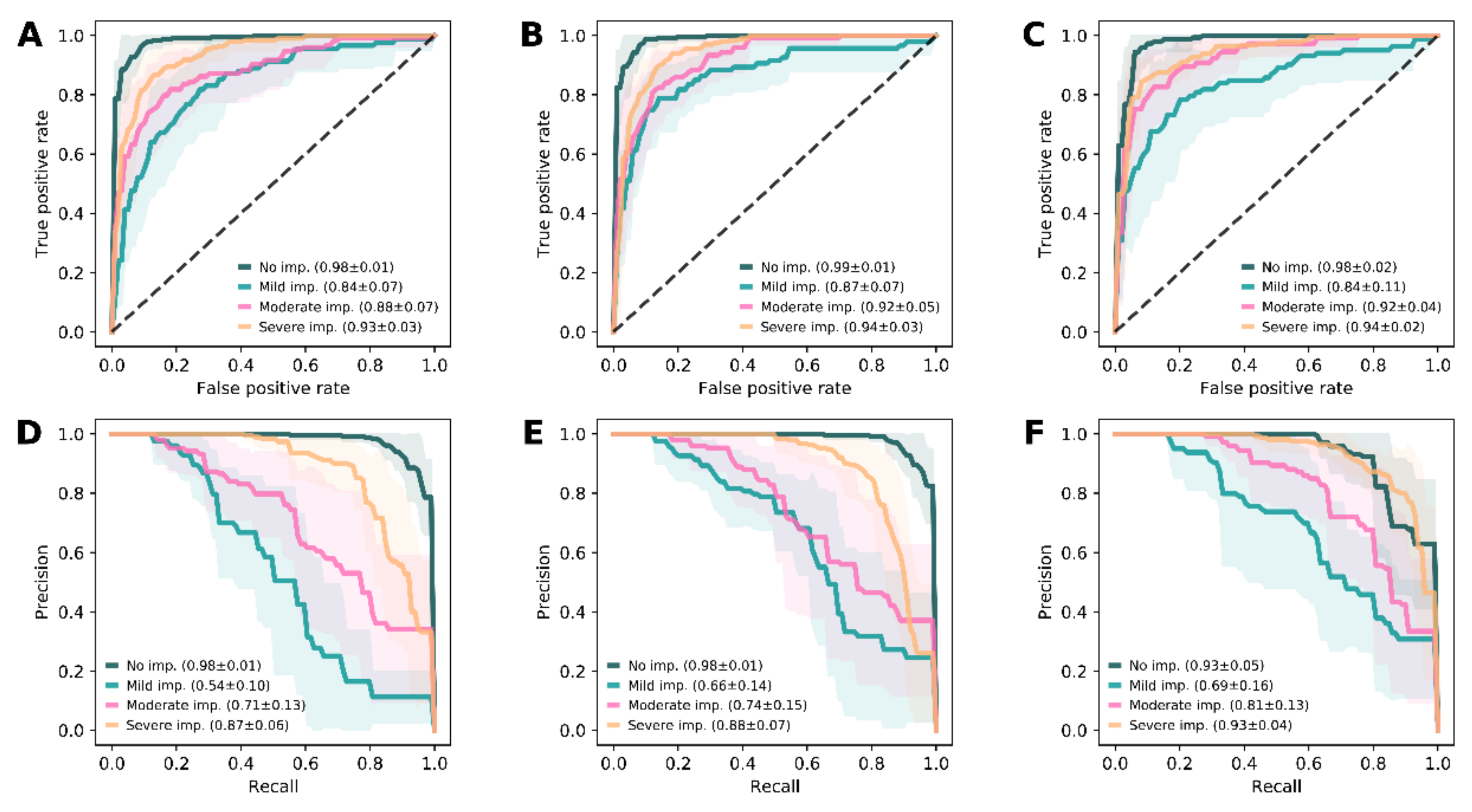
3.4. Prediction of Visual Impairment
3.5. Prediction of Best Corrected Visual Acuity
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hanany, M.; Rivolta, C.; Sharon, D. Worldwide carrier frequency and genetic prevalence of autosomal recessive inherited retinal diseases. Proc. Natl. Acad. Sci. USA 2020, 117, 2710–2716. [Google Scholar] [CrossRef] [PubMed]
- Koenekoop, R.K. The gene for Stargardt disease, ABCA4, is a major retinal gene: A mini-review. Ophthalmic Genet. 2003, 24, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Müller, P.L.; Gliem, M.; Mangold, E.; Bolz, H.J.; Finger, R.P.; McGuinness, M.; Betz, C.; Jiang, Z.; Weber, B.H.F.; MacLaren, R.E.; et al. Monoallelic ABCA4 Mutations Appear Insufficient to Cause Retinopathy: A Quantitative Autofluorescence Study. Invest. Ophthalmol. Vis. Sci. 2015, 56, 8179–8186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Müller, P.L.; Birtel, J.; Herrmann, P.; Holz, F.G.; Charbel Issa, P.; Gliem, M. Functional Relevance and Structural Correlates of Near Infrared and Short Wavelength Fundus Autofluorescence Imaging in ABCA4 -Related Retinopathy. Transl. Vis. Sci. Technol. 2019, 8, 46. [Google Scholar] [CrossRef] [Green Version]
- Ho, A.; Kuehlewein, L.; Hariri, A.; Wolfson, Y.; Strauss, R.W.; Scholl, H.P.; Sadda, S.R. ProgSTAR Study Group Quantitative Characteristics of Spectral-Domain Optical Coherence Tomography (SDOCT) in Corresponding Areas of Decreased Autofluorescence in Patients with Stargardt Disease. Investig. Opthalmol. Vis. Sci. 2015, 56, 5924. [Google Scholar]
- Klevering, B.J.; Deutman, A.F.; Maugeri, A.; Cremers, F.P.M.; Hoyng, C.B. The spectrum of retinal phenotypes caused by mutations in the ABCA4 gene. Graefes Arch. Clin. Exp. Ophthalmol. 2005, 243, 90–100. [Google Scholar] [CrossRef]
- Müller, P.L.; Pfau, M.; Treis, T.; Pascual-Camps, I.; Birtel, J.; Lindner, M.; Herrmann, P.; Holz, F.G. Progression of abca4-related retinopathy-prognostic value of demographic, functional, genetic, and imaging parameters. Retina 2020, 1. [Google Scholar] [CrossRef] [PubMed]
- Müller, P.L.; Pfau, M.; Mauschitz, M.M.; Möller, P.T.; Birtel, J.; Chang, P.; Gliem, M.; Schmitz-Valckenberg, S.; Fleckenstein, M.; Holz, F.G.; et al. Comparison of Green Versus Blue Fundus Autofluorescence in ABCA4 -Related Retinopathy. Transl. Vis. Sci. Technol. 2018, 7, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lois, N.; Holder, G.E.; Bunce, C.; Fitzke, F.W.; Bird, A.C. Phenotypic subtypes of Stargardt macular dystrophy-fundus flavimaculatus. Arch. Ophthalmol. 2001, 119, 359–369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujinami, K.; Lois, N.; Mukherjee, R.; McBain, V.A.; Tsunoda, K.; Tsubota, K.; Stone, E.M.; Fitzke, F.W.; Bunce, C.; Moore, A.T.; et al. A Longitudinal Study of Stargardt Disease: Quantitative Assessment of Fundus Autofluorescence, Progression, and Genotype Correlations. Investig. Opthalmol. Vis. Sci. 2013, 54, 8181–8190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zahid, S.; Jayasundera, T.; Rhoades, W.; Branham, K.; Khan, N.; Niziol, L.M.; Musch, D.C.; Heckenlively, J.R. Clinical phenotypes and prognostic full-field electroretinographic findings in Stargardt disease. Am. J. Ophthalmol. 2013, 155, 465–473.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCulloch, D.L.; Marmor, M.F.; Brigell, M.G.; Hamilton, R.; Holder, G.E.; Tzekov, R.; Bach, M. ISCEV Standard for full-field clinical electroretinography (2015 update). Doc. Ophthalmol. 2015, 130, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Caixinha, M.; Nunes, S. Machine Learning Techniques in Clinical Vision Sciences. Curr. Eye Res. 2017, 42, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Rohm, M.; Tresp, V.; Müller, M.; Kern, C.; Manakov, I.; Weiss, M.; Sim, D.A.; Priglinger, S.; Keane, P.A.; Kortuem, K. Predicting Visual Acuity by Using Machine Learning in Patients Treated for Neovascular Age-Related Macular Degeneration. Ophthalmology 2018, 125, 1028–1036. [Google Scholar] [CrossRef] [PubMed]
- Von der Emde, L.; Pfau, M.; Dysli, C.; Thiele, S.; Möller, P.T.; Lindner, M.; Schmid, M.; Fleckenstein, M.; Holz, F.G.; Schmitz-Valckenberg, S. Artificial intelligence for morphology-based function prediction in neovascular age-related macular degeneration. Sci. Rep. 2019, 9, 11132. [Google Scholar] [CrossRef] [PubMed]
- Džeroski, S.; Ženko, B. Is combining classifiers with stacking better than selecting the best one? Mach. Learn. 2004, 54, 255–273. [Google Scholar] [CrossRef] [Green Version]
- Strauss, R.W.; Ho, A.; Muñoz, B.; Cideciyan, A.V.; Sahel, J.-A.; Sunness, J.S.; Birch, D.G.; Bernstein, P.S.; Michaelides, M.; Traboulsi, E.I.; et al. The Natural History of the Progression of Atrophy Secondary to Stargardt Disease (ProgStar) Studies. Ophthalmology 2016, 123, 817–828. [Google Scholar] [CrossRef]
- Müller, P.L.; Pfau, M.; Möller, P.T.; Nadal, J.; Schmid, M.; Lindner, M.; de Sisternes, L.; Stöhr, H.; Weber, B.H.F.; Neuhaus, C.; et al. Choroidal Flow Signal in Late-Onset Stargardt Disease and Age-Related Macular Degeneration: An OCT-Angiography Study. Invest. Ophthalmol. Vis. Sci. 2018, 59, AMD122–AMD131. [Google Scholar] [CrossRef] [Green Version]
- Birtel, J.; Eisenberger, T.; Gliem, M.; Müller, P.L.; Herrmann, P.; Betz, C.; Zahnleiter, D.; Neuhaus, C.; Lenzner, S.; Holz, F.G.; et al. Clinical and genetic characteristics of 251 consecutive patients with macular and cone/cone-rod dystrophy. Sci. Rep. 2018, 8, 4824. [Google Scholar] [CrossRef]
- Staurenghi, G.; Sadda, S.; Chakravarthy, U.; Spaide, R.F. International Nomenclature for Optical Coherence Tomography (IN•OCT) Panel Proposed Lexicon for Anatomic Landmarks in Normal Posterior Segment Spectral-Domain Optical Coherence Tomography. Ophthalmology 2014, 121, 1572–1578. [Google Scholar] [CrossRef]
- Sayegh, R.G.; Sacu, S.; Dunavölgyi, R.; Kroh, M.E.; Roberts, P.; Mitsch, C.; Montuoro, A.; Ehrenmüller, M.; Schmidt-Erfurth, U. Geographic Atrophy and Foveal-Sparing Changes Related to Visual Acuity in Patients With Dry Age-Related Macular Degeneration Over Time. Am. J. Ophthalmol. 2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Virtanen, P.; Gommers, R.; Oliphant, T.E.; Haberland, M.; Reddy, T.; Cournapeau, D.; Burovski, E.; Peterson, P.; Weckesser, W.; Bright, J.; et al. Author Correction: SciPy 1.0: Fundamental algorithms for scientific computing in Python. Nat. Methods 2020, 17, 352. [Google Scholar] [PubMed] [Green Version]
- Varoquaux, G.; Buitinck, L.; Louppe, G.; Grisel, O.; Pedregosa, F.; Mueller, A. Scikit-learn. GetMobile Mob. Comput. Commun. 2015, 19, 29–33. [Google Scholar] [CrossRef]
- Chen, T.; Guestrin, C. XGBoost: A scalable tree boosting system. In Proceedings of the 22nd ACM SIGKDD International Conference on Knowledge Discovery and Data Mining, San Francisco, CA, USA, 13–17 August 2016; Association for Computing Machinery: New York, NY, USA, 2016; pp. 785–794. [Google Scholar]
- MIT ELI5. Available online: https://eli5.readthedocs.io/en/latest/index.html (accessed on 23 March 2020).
- Müller, P.L.; Treis, T.; Pfau, M.; Esposti, S.D.; Alsaedi, A.; Maloca, P.; Balaskas, K.; Webster, A.; Egan, C.; Tufail, A. Progression of Retinopathy Secondary to Maternally Inherited Diabetes and Deafness—Evaluation of Predicting Parameters. Am. J. Ophthalmol. 2020, 213, 134–144. [Google Scholar] [CrossRef]
- Vabalas, A.; Gowen, E.; Poliakoff, E.; Casson, A.J. Machine learning algorithm validation with a limited sample size. PLoS ONE 2019, 14, e0224365. [Google Scholar] [CrossRef]
- Kotsiantis, S.B.; Zaharakis, I.D.; Pintelas, P.E. Machine learning: A review of classification and combining techniques. Artif. Intell. Rev. 2006, 26, 159–190. [Google Scholar] [CrossRef]
- Dey, A. Machine Learning Algorithms: A Review. Int. J. Comput. Sci. Inf. Technol. 2016, 7, 1174–1179. [Google Scholar]
- Uddin, S.; Khan, A.; Hossain, M.E.; Moni, M.A. Comparing different supervised machine learning algorithms for disease prediction. BMC Med. Inform. Decis. Mak. 2019, 19, 1–16. [Google Scholar] [CrossRef]
- Azar, A.T.; El-Metwally, S.M. Decision tree classifiers for automated medical diagnosis. Neural Comput. Appl. 2013, 23, 2387–2403. [Google Scholar] [CrossRef]
- Sesmero, M.P.; Ledezma, A.I.; Sanchis, A. Generating ensembles of heterogeneous classifiers using Stacked Generalization. Wiley Interdiscip. Rev. Data Min. Knowl. Discov. 2015, 5, 21–34. [Google Scholar] [CrossRef]
- Varma, S.; Simon, R. Bias in error estimation when using cross-validation for model selection. BMC Bioinformatics 2006, 7, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samuel, A.L. Some Studies in Machine Learning Using the Game of Checkers. IBM J. Res. Dev. 1959, 3, 210–229. [Google Scholar] [CrossRef]
- De Fauw, J.; Keane, P.; Tomasev, N.; Visentin, D.; van den Driessche, G.; Johnson, M.; Hughes, C.O.; Chu, C.; Ledsam, J.; Back, T.; et al. Automated analysis of retinal imaging using machine learning techniques for computer vision. F1000Research 2016, 5, 1573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davidson, B.; Kalitzeos, A.; Carroll, J.; Dubra, A.; Ourselin, S.; Michaelides, M.; Bergeles, C. Automatic Cone Photoreceptor Localisation in Healthy and Stargardt Afflicted Retinas Using Deep Learning. Sci. Rep. 2018, 8, 7911. [Google Scholar] [CrossRef]
- Parodi, M.B.; Iacono, P.; Triolo, G.; La Spina, C.; Zucchiatti, I.; Cicinelli, M.V.; Borrelli, E.; Manitto, M.P.; Martina, E.; Bandello, F. Morpho-functional correlation of fundus autofluorescence in Stargardt disease. Br. J. Ophthalmol. 2015, 99, 1354–1359. [Google Scholar] [CrossRef]
- Ergun, E.; Hermann, B.; Wirtitsch, M.; Unterhuber, A.; Ko, T.H.; Sattmann, H.; Scholda, C.; Fujimoto, J.G.; Stur, M.; Drexler, W. Assessment of central visual function in Stargardt’s disease/fundus flavimaculatus with ultrahigh-resolution optical coherence tomography. Invest. Ophthalmol. Vis. Sci. 2005, 46, 310–316. [Google Scholar] [CrossRef]
- Von der Emde, L.; Pfau, M.; Thiele, S.; Moller, P.T.; Hassenrik, R.; Fleckenstein, M.; Holz, F.G.; Schmitz-Valckenberg, S. Mesopic and Dark-Adapted Two-Color Fundus-Controlled Perimetry in Choroidal Neovascularization Secondary to Age-Related Macular Degeneration. Transl. Vis. Sci. Technol. 2019, 8, 7. [Google Scholar] [CrossRef] [Green Version]
- Huang, W.C.; Cideciyan, A.V.; Roman, A.J.; Sumaroka, A.; Sheplock, R.; Schwartz, S.B.; Stone, E.M.; Jacobson, S.G. Inner and Outer Retinal Changes in Retinal Degenerations Associated With ABCA4 Mutations. Investig. Opthalmol. Vis. Sci. 2014, 55, 1810. [Google Scholar] [CrossRef]
- Hendriks, M.; Verhoeven, V.J.M.; Buitendijk, G.H.S.; Polling, J.R.; Meester-Smoor, M.A.; Hofman, A.; Kamermans, M.; Ingeborgh van den Born, L.; Klaver, C.C.W.; van Huet, R.A.; et al. Development of Refractive Errors—What Can We Learn From Inherited Retinal Dystrophies? Am. J. Ophthalmol. 2017, 182, 81–89. [Google Scholar] [CrossRef] [Green Version]
- Müller, P.L.; Wolf, S.; Dolz-Marco, R.; Tafreshi, A.; Schmitz-valckenberg, S.; Holz, F.G. Ophthalmic Diagnostic Imaging: Retina. In High Resolution Imaging in Microscopy and Ophthalmology: New Frontiers in Biomedical Optics; Bille, J.F., Ed.; Springer International Publishing: Berlin/Heidelberg, Germany, 2019; pp. 87–106. ISBN 978-3-030-16637-3. [Google Scholar]
- International Conference on Harmonisation E9 Expert Working Group ICH Harmonised Tripartite Guideline. Statistical principles for clinical trials. Stat. Med. 1999, 18, 1905–1942. [Google Scholar]
- Zernant, J.; Schubert, C.; Im, K.M.; Burke, T.; Brown, C.M.; Fishman, G.A.; Tsang, S.H.; Gouras, P.; Dean, M.; Allikmets, R. Analysis of the ABCA4 gene by next-generation sequencing. Invest. Ophthalmol. Vis. Sci. 2011, 52, 8479–8487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burke, T.R.; Rhee, D.W.; Smith, R.T.; Tsang, S.H.; Allikmets, R.; Chang, S.; Lazow, M.A.; Hood, D.C.; Greenstein, V.C. Quantification of peripapillary sparing and macular involvement in Stargardt disease (STGD1). Invest. Ophthalmol. Vis. Sci. 2011, 52, 8006–8015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nassisi, M.; Mohand-Saïd, S.; Andrieu, C.; Antonio, A.; Condroyer, C.; Méjécase, C.; Dhaenens, C.M.; Sahel, J.A.; Zeitz, C.; Audo, I. Peripapillary sparing with near infrared autofluorescence correlates with electroretinographic findings in patients with Stargardt disease. Investig. Ophthalmol. Vis. Sci. 2019, 60, 4951–4957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pfau, M.; Holz, F.G.; Müller, P.L. Retinal light sensitivity as outcome measure in recessive Stargardt disease. Br. J. Ophthalmol. 2020, 4. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient-Level Data | Controls | All Patients | Group 1 | Group 2 | Group 3 |
|---|---|---|---|---|---|
| Patients (n) | 54 | 156 | 71 | 55 | 30 |
| Sex (F/M) | 35/19 | 101/55 | 46/25 | 36/19 | 19/11 |
| Age at Exam (Y)A | 39.24 ± 16.00 | 38.77 ± 18.23 | 33.76 ± 15.17 | 45.03 ± 19.521 | 39.15 ± 18.79 |
| Age of Onset (Y)A | --- | 26.39 ± 17.16 | 24.75 ± 15.48 | 32.91 ± 18.93 | 18.30 ± 12.59 |
| Disease Duration (Y)A | --- | 12.39 ± 12.45 | 9.01 ± 9.55 | 12.12 ± 12.00 | 20.85 ± 15.07 |
| Eye-Level Data | |||||
| Eyes (n) | 108 | 311 | 142 | 109 | 60 |
| BCVA (LogMAR)A | 0.00 ± 0.00 | 0.68 ± 0.47 | 0.57 ± 0.44 | 0.62 ± 0.43 | 1.06 ± 0.4 |
| Refractive Error (Dpt)A | −0.80 ± 2.05 | −1.15 ± 1.99 | −1.23 ± 2.05 | −0.64 ± 1.95 | −1.88 ± 1.67 |
| Foveal Status (FI/FNI) | --- | 197/114 | 79/63 | 65/44 | 53/7 |
| Maximal Deviation from Truth [LogMAR] | Feature Sets [%] A | ||
|---|---|---|---|
| A | B | C | |
| −0.5 To 0.5 | 92.10 | 96.37 | 95.82 |
| −0.4 To 0.4 | 85.15 | 92.42 | 89.35 |
| −0.3 To 0.3 | 72.67 | 85.31 | 83.92 |
| −0.2 To 0.2 | 59.24 | 75.36 | 67.64 |
| −0.1 To 0.1 | 35.39 | 53.55 | 39.87 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Müller, P.L.; Treis, T.; Odainic, A.; Pfau, M.; Herrmann, P.; Tufail, A.; Holz, F.G. Prediction of Function in ABCA4-Related Retinopathy Using Ensemble Machine Learning. J. Clin. Med. 2020, 9, 2428. https://doi.org/10.3390/jcm9082428
Müller PL, Treis T, Odainic A, Pfau M, Herrmann P, Tufail A, Holz FG. Prediction of Function in ABCA4-Related Retinopathy Using Ensemble Machine Learning. Journal of Clinical Medicine. 2020; 9(8):2428. https://doi.org/10.3390/jcm9082428
Chicago/Turabian StyleMüller, Philipp L., Tim Treis, Alexandru Odainic, Maximilian Pfau, Philipp Herrmann, Adnan Tufail, and Frank G. Holz. 2020. "Prediction of Function in ABCA4-Related Retinopathy Using Ensemble Machine Learning" Journal of Clinical Medicine 9, no. 8: 2428. https://doi.org/10.3390/jcm9082428
APA StyleMüller, P. L., Treis, T., Odainic, A., Pfau, M., Herrmann, P., Tufail, A., & Holz, F. G. (2020). Prediction of Function in ABCA4-Related Retinopathy Using Ensemble Machine Learning. Journal of Clinical Medicine, 9(8), 2428. https://doi.org/10.3390/jcm9082428