
Online Religious Involvement, Spiritual Support, Depression, and Anxiety during the COVID-19 Pandemic


Abstract
1. Introduction
1.1. Religious Involvement, Spiritual Support, Depression, and Anxiety
1.2. The Present Study
2. Methods
2.1. Procedure and Participants
2.2. Measurement
2.2.1. Online Religious Involvement
2.2.2. Spiritual Support
2.2.3. Depression
2.2.4. Anxiety
2.3. Data Analysis
3. Results
3.1. Descriptive Statistics
3.2. Construct Validity Test and Fitness Test of the Model
3.3. Construct Equivalence Test
3.4. Latent Mean Analysis
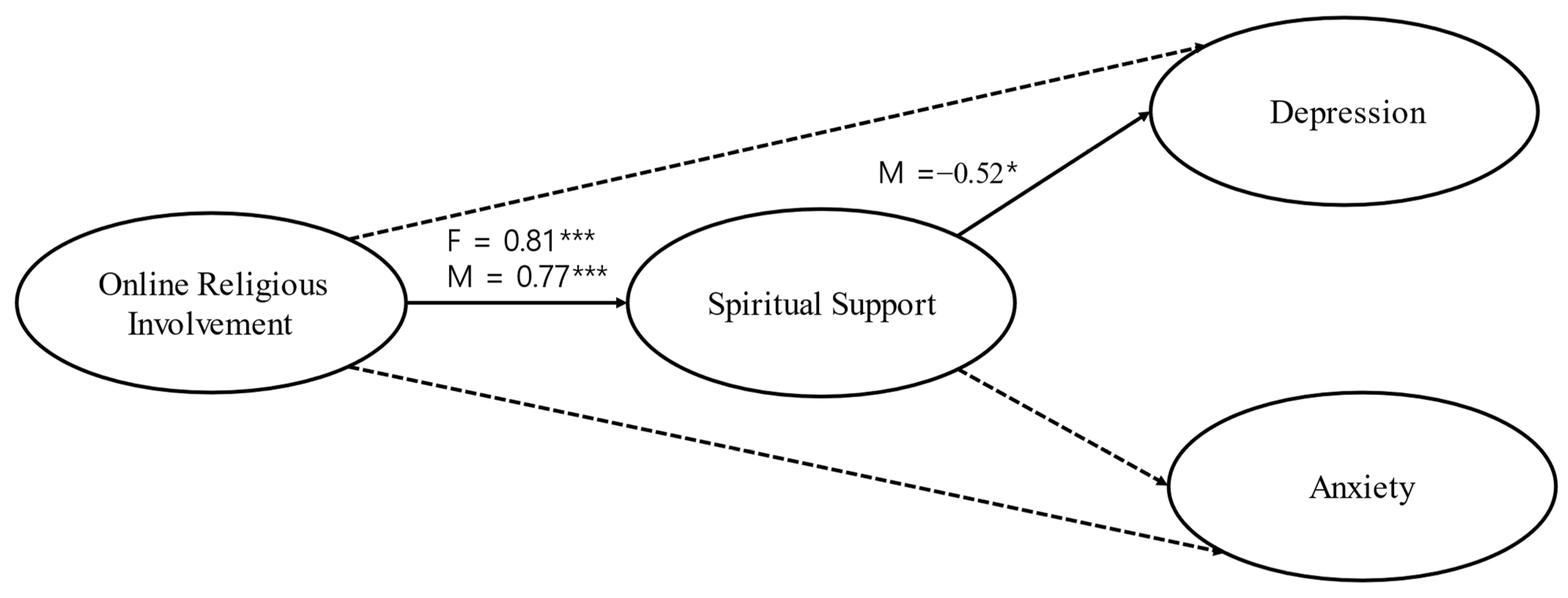
3.5. Multigroup Structural Model Analysis
4. Discussion
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abdel-Khalek, Ahmed M., Laura Nuño, Juana Gómez-Benito, and David Lester. 2019. The relationship between religiosity and anxiety: A meta-analysis. Journal of Religion and Health 58: 1847–56. [Google Scholar] [CrossRef] [PubMed]
- Ai, Ai L., Terrence N. Tice, Christopher Peterson, and Bu Huang. 2005. Prayers, spiritual support, and positive attitudes in coping with the September 11 national crisis. Journal of Personality 73: 763–92. [Google Scholar] [CrossRef] [PubMed]
- Algahtani, Fahad D., Mohamed Ali Alzain, Najoua Haouas, Khadijah Angawi, Bandar Alsaif, Adel Kadri, Mohamed A. Dkhil, Mejdi Snoussi, and Rafat Zrieq. 2021. Coping during COVID-19 Pandemic in Saudi Community: Religious Attitudes, Practices and Associated Factors. International Journal of Environmental Research and Public Health 18: 8651. [Google Scholar] [CrossRef] [PubMed]
- Andrade, Laura, Jorge J. Caraveo-anduaga, Patricia Berglund, Rob V. Bijl, Ron De Graaf, Wilma Vollebergh, Eva Dragomirecka, Robert Kohn, Martin Keller, Ronald C. Kessler, and et al. 2003. The epidemiology of major depressive episodes: Results from the International Consortium of Psychiatric Epidemiology (ICPE) Surveys. International Journal of Methods in Psychiatric Research 12: 3–21. [Google Scholar] [CrossRef] [PubMed]
- Bahk, Yong-Chun, Kiho Park, Naeun Kim, Lee Joohee, Chosurin Cho, Jihee Jang, Dawoon Jung, Eun Jin Chang, and Kee-Hong Choi. 2021. Psychological Impact of COVID-19 in South Korea: A Preliminary Study. Korean Journal of Clinical Psychology 39: 355–67. [Google Scholar] [CrossRef]
- Bahrami, Fatemeh, and Naser Yousefi. 2011. Females are more anxious than males: A metacognitive perspective. Iranian Journal of Psychiatry and Behavioral Sciences 5: 83–90. [Google Scholar] [PubMed]
- Balboni, Tracy A., Lauren Vanderwerker, Susan Block, M. ElizabethPaulk, Christopher LathanJohn Peteet, and Holly Prigerson. 2007. Religiousness and spiritual support among advanced cancer patients and associations with end-of-life treatment preferences and quality of life. Journal of Clinical Oncology 25: 555–60. [Google Scholar] [CrossRef]
- Bolton, James, Brian Cox, Tracie Afifi, Murray Enns, O. Joseph Bienvenu, and Jitender Sareen. 2008. Anxiety disorders and risk for suicide attempts: Findings from the Baltimore Epidemiologic Catchment area follow-up study. Depress Anxiety 25: 477–81. [Google Scholar] [CrossRef]
- Byrne, Barbara. 2010. Structural Equation Modeling with Amos: Basic Concepts, Applications, and Programming, 2nd ed. New York: Taylor and Francis Group. [Google Scholar]
- Cho, Maeng Je, Su Jeong Seong, Jee Eun Park, In-Won Chung, Young Moon Lee, Ahn Bae, Joon Ho Ahn, Dong-Woo Lee, Jae Nam Bae, Seong-Jin Cho, and et al. 2015. Prevalence and Correlates of DSM-IV Mental Disorders in South Korean Adults: The Korean Epidemiologic Catchment Area Study 2011. Psychiatry Investigation 12: 164–70. [Google Scholar] [CrossRef]
- Cohen, Jacob. 1988. Statistical Power Analysis of the Behavioral Sciences, 2nd ed. Hillsdale, NJ: Erlbaum. [Google Scholar]
- de Vaus, David, and Ian McAllister. 1987. Gender Differences in Religion: A Test of the Structural Location Theory. American Sociological Review 52: 472–81. [Google Scholar] [CrossRef]
- Desrosiers, Alethea, and Lisa Miller. 2007. Relational spirituality and depression in adolescent girls. Journal of Clinical Psychology 63: 1021–37. [Google Scholar] [CrossRef] [PubMed]
- Ellison, Christopher. 1991. Religious involvement and subjective wellbeing. Journal of Health and Social Behavior 32: 80–99. [Google Scholar] [CrossRef] [PubMed]
- Ellison, Christopher, and Kevin Flannelly. 2009. Religious involvement and risk of major depression in a prospective nationwide study of African American adults. The Journal of Nervous and Mental Disease 197: 568–73. [Google Scholar] [CrossRef] [PubMed]
- Fiala, William, Jeffrey Bjorck, and Richard Gorsuch. 2002. The religious support scale: Construction, validation, and cross-validation. American Journal of Community Psychology 30: 761–86. [Google Scholar] [CrossRef]
- Fornell, Claes, and David Larcker. 1981. Evaluating structural equation models with unobservable variables and measurement error. Journal of Marketing Research 18: 39–50. [Google Scholar] [CrossRef]
- George, Linda, Christopher Ellison, and David Larson. 2002. Explaining the relationships between religious involvement and health. Psychological Inquiry 13: 190–200. [Google Scholar] [CrossRef]
- Głaz, Stanisław. 2022. The Relationship between Meaning in Life, Life Satisfaction and Job Satisfaction with Religious Experience in the Life of Polish Nurses. Journal of Religion and Health. [Google Scholar] [CrossRef]
- Hadianfard, Habib. 2005. Subjective well-being and religious activity in a group of Muslims. Iranian Journal of Psychiatry and Clinical Psychology (Thinking and Behavior) 11: 224–32. [Google Scholar]
- Hair, Joseph, Jr., William Black, Barry Babin, and Rolph Anderson. 2010. Multivariate Data Analysis: A Global Perspective, 7th ed. Upper Saddle River: Pearson Education. [Google Scholar]
- Hakamata, Yuko, Mikio Iwase, Hiroshi Iwata, Toshiki Kobayashi, Tsuneo Tamaki, Masami Nishio, Hiroshi Matsuda, Norio Ozaki, and Toshiya Inada. 2009. Gender difference in relationship between anxiety-related personality traits and cerebral brain glucose metabolism. Psychiatry Research: Neuroimaging 173: 206–11. [Google Scholar] [CrossRef]
- Hall, Daniel, Harold Koenig, and Keith Meador. 2008. Hitting the target: Why existing measures of “religiousness” are really reverse-scored measures of “secularism”. Explore 4: 368–73. [Google Scholar] [CrossRef]
- Han, Nae. 2002. An empirical study on the effects of religiosity on the mental health. Korean Journal of Sociology 36: 157–82. [Google Scholar]
- Harris, J. Irene, Sean Schoneman, and Stephanie Carrera. 2002. Approaches to religiosity related to anxiety among college students. Mental Health, Religion and Culture 5: 253–65. [Google Scholar] [CrossRef]
- Holmes, Emily A., Rory C. O’Connor, V. Hugh Perry, Irene Tracey, Simon Wessely, Louise Arseneault, Clive Ballard, Helen Christensen, Roxane Cohen Silver, Ian Everall, and et al. 2020. Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. The Lancet Psychiatry 7: 547–60. [Google Scholar] [CrossRef]
- Hong, Sehee, Mary Malik, and Min-Kyu Lee. 2003. Testing configural, metric, scalar, and latent mean invariance across genders in sociotropy and autonomy using non-western sample. Educational and Psychological Measurement 63: 636–54. [Google Scholar] [CrossRef]
- Hu, L. Litze, and Peter Bentler. 1999. Cutoff criteria for fit indexes in covariance structure analyses: Conventional criteria versus new alternatives. Structural Equation Modeling 6: 1–55. [Google Scholar] [CrossRef]
- Jansen, Kate, Rebecca Motley, and Joseph Hovey. 2010. Anxiety, depression and students’ religiosity. Mental Health, Religion & Culture 13: 267–71. [Google Scholar]
- Kang, Sung-Bong, and Sung-Sook Cho. 2013. Effects of Religious Activities and Faith Attitudes on Depression and Ego-Integrity of the Elderly. The Journal of the Korea Contents Association 13: 325–46. [Google Scholar] [CrossRef]
- Kang, Piljoo, and Laura Romo. 2011. The role of religious involvement on depression, risky behavior, and academic performance among Korean American adolescents. Journal of Adolescence 34: 767–78. [Google Scholar] [CrossRef]
- Kanwar, Amrit, Shaista Malik, Larry Prokop, Leslie Sim, David Feldstein, Zhen Wang, and M. Hassan Murad. 2013. The association between anxiety disorders and suicidal behaviors: A systematic review and meta-analysis. Depression and Anxiety 30: 917–29. [Google Scholar] [CrossRef]
- Keshavarz, Keshavarz Amir, Hossein Ali Mehrabi, and Mohammad Soltanizadeh. 2009. Psychological predictors of life satisfaction. Journal of Developmental Psychology 22: 159–68. [Google Scholar]
- Kim, Joo, Min Kim, and Sehee Hong. 2009. Structural Equation Modeling in Dissertation. Seoul: Communication Books. [Google Scholar]
- Koenig, Harold. 2007. Religion and remission of depression in medical inpatients with heart failure/pulmonary disease. Journal of Nervous and Mental Disease 195: 389–95. [Google Scholar] [CrossRef] [PubMed]
- Koenig, Harold. 2012. Religion, spirituality, and health: The research and clinical implications. ISRN Psychiatry 2012: 278730. [Google Scholar] [CrossRef] [PubMed]
- Koenig, Harold, Dana King, and Verna Carson. 2012. Handbook of Religion and Health, 2nd ed. New York: Oxford University Press. [Google Scholar]
- Kowalczyk, Oliwia, Krzysztof Roszkowski, Xavier Montane, Wojciech Pawliszak, Bartosz Tylkowski, and Anna Bajek. 2020. Religion and Faith Perception in a Pandemic of COVID-19. Journal of Religion and Health 59: 2671–77. [Google Scholar] [CrossRef] [PubMed]
- Lee, Bruce, and Andrew Newberg. 2005. Religion and health: A review and critical analysis. Zygon 40: 443–68. [Google Scholar] [CrossRef]
- Lee, Kang Ho, Chang Ho Chae, Young Ouk Kim, Jun Seok Son, Ja-Hyun Kim, Chan Woo Kim, Hyoung Ouk Park, Jun Ho Lee, and Young Saeng Jung. 2015. Anxiety symptoms and occupational stress among young Korean female manufacturing workers. Annals of Occupational and Environmental Medicine 27: 24. [Google Scholar] [CrossRef]
- Lee, Sang-Ahm, Han Uk Ryu, Eun-Ju Choi, Myung-Ah Ko, Ji-Ye Jeon, Su-Hyun Han, Gha-Hyun Lee, Moon Kyu Lee, and Kwang-Deog Jo. 2017. Associations between religiosity and anxiety, depressive symptoms, and well-being in Korean adults living with epilepsy. Epilepsy & Behavior 75: 246–51. [Google Scholar]
- Leonardi, Angeliki, and Vasilios Gialamas. 2009. Religiosity and psychological well- being. International Journal of Psychology 44: 241–48. [Google Scholar]
- Levin, Jeffrey. 1994. Religion and health: Is there an association, is it valid, and is it causal? Social Science & Medicine 38: 1475–82. [Google Scholar] [CrossRef]
- Levin, Jeffrey, Robert Taylor, and Linda Chatters. 1995. A multidimensional measure of religious involvement for African American. Sociological Quarterly 36: 157–73. [Google Scholar] [CrossRef]
- Lindemann, Carol. 1996. Handbook of the Treatment of the Anxiety Disorders. London: Jason Aronsoninc. [Google Scholar]
- Mackenzie, Elizabeth, Doris Rajagopal, Margaret Meilbohm, and Risa Lavizzo-Mourey. 2000. Spiritual support and psychological well-being: Older adults’ perceptions of the religion and health connection. Alternative Therapies in Health and Medicine 6: 37. [Google Scholar]
- Maier, Maier, Wolfgang, Michael Gänsicke, Richard Gater, Murat Rezaki, Bea G. Tiemens, and Ramón Florenzano Urzúa. 1999. Gender differences in the prevalence of depression: A survey in primary care. Journal of Affective Disorders 53: 241–52. [Google Scholar] [CrossRef]
- Maton, Kenneth. 1989. The stress-buffering role of spiritual support: Cross-sectional and prospective investigations. Journal for the Scientific Study of Religion 28: 310–23. [Google Scholar] [CrossRef]
- McCullough, Michael, and David Larson. 1999. Religion and depression: A review of the literature. Twin Research and Human Genetics 2: 126–36. [Google Scholar] [CrossRef]
- McFarland, Michael. 2010. Religion and mental health among older adults: Do the effects of religious involvement vary by gender? Journals of Gerontology Series B: Psychological Sciences and Social Sciences 65: 621–30. [Google Scholar] [CrossRef] [PubMed]
- Mirola, William. 1999. A Refuge for Some: Gender Differences in the Relationship between Religious Involvement and Depression. Sociology of Religion 60: 419–37. [Google Scholar] [CrossRef]
- Nikkei Asia. 2021. South Korea Unemployment Rate Soars to 21-Year High. Available online: https://asia.nikkei.com/Economy/South-Korea-unemployment-rate-soars-to-21-year-high (accessed on 10 February 2021).
- Oh, Kyung. N. 2015. A Comparative Study on Religiosity of Christian Women and Men in Korea. Christian Education & Information Technology 44: 221–52. [Google Scholar]
- Paine, David, and Steven Sandage. 2017. Religious involvement and depression: The mediating effect of relational spirituality. Journal of Religion and Health 56: 269–83. [Google Scholar] [CrossRef]
- Panchal, Nirmita, Rabah Kamal, Cynthia Cox, and Rachel Garfield. 2021. The Implications of COVID-19 for Mental Health and Substance Use. Available online: https://www.kff.org/coronavirus-covid-19/issue-brief/the-implications-of-covid-19-for-mental-health-and-substance-use/ (accessed on 10 February 2022).
- Park, Crystal, and Crystal Cohen. 1993. Religious and non religious coping with the death of a friend. Cognitive Therapy and Research 17: 561–77. [Google Scholar] [CrossRef]
- Pew Research Center. 2016a. The Gender Gap in Religion around the World; Women Are Generally More Religious Than Men, Particularly among Christians. March 22. Available online: https://www.pewforum.org/2016/03/22/the-gender-gap-in-religion-around-the-world/ (accessed on 22 March 2022).
- Pew Research Center. 2016b. The Gender Gap in Religion around the World; 7. Theories Explaining Gender Differences in Religion. March 22. Available online: https://www.pewforum.org/2016/03/22/theories-explaining-gender-differences-in-religion/ (accessed on 22 March 2022).
- Price, Linda. 2006. Gender differences and similarities in online courses: Challenging stereotypical views of women. Journal of Computer Assisted Learning 22: 349–59. [Google Scholar] [CrossRef]
- Radloff, Lenore. 1977. The CES-D Scale: A self-report depression scale for research in the general population. Applied Psychological Measurement 1: 385–401. [Google Scholar] [CrossRef]
- Roth, David, Isaac Mwase, Cheryl L. Holt, Eddie M. Clark, Susan N. Lukwago, and Matthew Kreuter. 2012. Religious involvement measurement model in a national sample of African Americans. Journal of Religion and Health 51: 567–78. [Google Scholar] [CrossRef] [PubMed]
- Rovai, Alfred, and Jason Baker. 2005. Gender differences in online learning: Sense of community, perceived learning, and interpersonal interactions. Quarterly Review of Distance Education 6: 31. [Google Scholar]
- Schnittker, Jason. 2001. When is Faith Enough? The Effects of Religious Involvement on Depression. Journal for the Scientific Study of Religion 40: 393–411. [Google Scholar] [CrossRef]
- Shreve-Neiger, Andrea, and Barry Edelstein. 2004. Religion and anxiety: A critical review of the literature. Clinical Psychology Review 24: 379–97. [Google Scholar] [CrossRef]
- Sloan, Richard, Emilia Bagiella, and Tia Powell. 1999. Religion, spirituality, and medicine. Lancet 353: 664–67. [Google Scholar] [CrossRef]
- Spitzer, Robert, Kurt Kroenke, Janet Williams, and Bernd Löwe. 2006. A brief measure for assessing generalized anxiety disorder: The GAD-7. Archives of Internal Medicine 166: 1092–97. [Google Scholar] [CrossRef]
- Stark, Rodney. 2002. Physiology and Faith: Addressing the “Universal” Gender Difference in Religious Commitment. Journal for the Scientific Study of Religion 41: 495–507. [Google Scholar] [CrossRef]
- Statistics Korea. 2016. Cause of Death Statistics. May 30. Available online: http://kosis.kr/common/meta_onedepth.jsp?vwcd=MT_OTITLE&listid=MT_CTITLE_1 (accessed on 22 September 2021).
- Swinyard, William, Ah-Keng Kau, and Hui-Yin Phua. 2001. Happiness, materialism, and religious experience in the U.S. and Singapore. Journal of Happiness Studies 2: 13–32. [Google Scholar] [CrossRef]
- Thoresen, Carl, and Alex Harris. 2004. Spirituality, religion, and health: A scientific perspective. In Handbook of Clinical Health Psychology. Edited by James Raczynski and Laura Leviton. Washington, DC: American Psychological Association, pp. 269–98. [Google Scholar]
- Trzebiatowska, Marta, and Steve Bruce. 2012. Why Are Women More Religious Than Men? Oxford: Oxford University Press. [Google Scholar]
- Van Voorhees, Benjamin W, David Paunesku, Sachiko A. Kuwabara, Anirban Basu, Jackie Gollan, Benjamin L. Hankin, Stephanie Melkonian, and Mark Reinecke. 2008. Protective and vulnerability factors predicting new-onset depressive episode in a representative of U.S. adolescents. Journal of Adolescent Health 42: 605–16. [Google Scholar] [CrossRef]
- Vasegh, Sasan, and Mohammad-Reza Mohammadi. 2007. Religiosity, Anxiety, and Depression among a Sample of Iranian Medical Students. The International Journal of Psychiatry in Medicine 37: 213–27. [Google Scholar] [CrossRef]
- Vasilescu, Bogdan, Andrea Capiluppi, and Alexander Serebrenik. 2012. Gender, representation and online participation: A quantitative study of stackoverflow. Paper presented at the 2012 International Conference on Social Informatics, Alexandria, VA, USA, December 14–16; New York: IEEE, pp. 332–38. [Google Scholar]
- Wnuk, Marcin, and Jerzy Marcinkowski. 2014. Do existential variables mediate between religious-spiritual facets of functionality and psychological wellbeing. Journal of Religion & Health 53: 56–67. [Google Scholar]
- Woodhead, Linda. 2012. Gender Differences in Religious Practice and Significance. Travail, Genre et Sociétés 1: 33–54. [Google Scholar] [CrossRef]
- Yoo, Jieun. 2017. The Effect of Religious Involvement on Life Satisfaction among Korean Christians: Focused on the Mediating Effect of Spiritual Well-Being and Self-Esteem. The Journal of Pastoral Care & Counseling: JPCC 71: 257–66. [Google Scholar] [CrossRef]
- You, Sukkyung, and Jieun Yoo. 2016. Prayer and subjective well-being: The moderating role of religious support. Archive for the Psychology of Religion 38: 301–15. [Google Scholar] [CrossRef]
- You, Sukkyung, Jieun Yoo, and Yunsung Koh. 2019. Religious practices and mental health outcomes among Korean adults. Personality and Individual Differences 142: 7–12. [Google Scholar] [CrossRef]
- Zhang, Wei. 2010. Religious participation, gender differences, and cognitive impairment among the oldest-old in China. Journal of Aging Research 2010: 160294. [Google Scholar] [CrossRef]
- Zohra, Nosheen, and Erum Irshad. 2012. Religiosity and anxiety disorder in Peshawar. FWU Journal of Social Sciences 6: 57. [Google Scholar]


{kind=link}
| Variables | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| 1. Online Religious Involvement | 1 | 0.708 ** | 0.151 * | 0.097 |
| 2. Spiritual Support | 0.680 ** | 1 | 0.054 | 0.047 |
| 3. Depression | −0.224 * | −0.382 ** | 1 | 0.763 ** |
| 4. Anxiety | −0.252 * | −0.360 ** | 0.678 ** | 1 |
| M(SD) | 3.60(0.821) | 3.85(1.138) | 1.78(0.697) | 1.85(0.744) |
| Skewness | −0.647 | −1.115 | 0.539 | 0.511 |
| Kurtosis | −0.621 | 0.490 | 0.334 | 0.334 |
| Model | χ² | df | p | TLI | CFI | RMSEA |
|---|---|---|---|---|---|---|
| Configural invariance (baseline model): Model 1 | 679.525 | 366 | 0.000 | 0.915 | 0.926 | 0.064 |
| Metric invariance: Model 2 | 704.144 | 383 | 0.000 | 0.917 | 0.924 | 0.063 |
| Metric & scalar invariance: Model 3 | 749.433 | 404 | 0.000 | 0.915 | 0.918 | 0.064 |
| Metric, scalar, & factor variance invariance: Model 4 | 763.559 | 408 | 0.000 | 0.914 | 0.916 | 0.065 |
| Latent Variables | Female (n = 138) | Male (n = 72) | Effect Size | Total M | ||
|---|---|---|---|---|---|---|
| Latent M | M | Latent M | M | |||
| Online Religious Involvement | 0 | 3.490 | 0.431 *** | 3.819 | 0.69 | 3.603 |
| Spiritual Support | 0 | 3.676 | 0.569 *** | 4.191 | 0.53 | 3.852 |
| Depression | 0 | 1.822 | 0.356 *** | 1.726 | 0.95 | 1.789 |
| Anxiety | 0 | 1.893 | 0.427 *** | 1.767 | 0.95 | 1.850 |
| Parameter | Female | Male |
|---|---|---|
| Online Religious Involvement → Spiritual Support | 1.089 ***(0.809) | 0.857 ***(0.771) |
| Online Religious Involvement → Depression | 0.236(0.325) | 0.154(0.165) |
| Online Religious Involvement → Anxiety | 0.175(0.219) | −0.014(−0.014) |
| Spiritual Support → Depression | −0.110(−0.204) | −0.435 *(−0.518) |
| Spiritual Support → Anxiety | −0.077(−0.131) | −0.336(−0.365) |
| Path with Equality Constraint on Path Coefficient | Δdf | Δχ² | ΔTLI |
|---|---|---|---|
| Online Religious Involvement → Spiritual Support | 1 | 1.921 | 0.000 |
| Online Religious Involvement → Depression | 1 | 0.093 | 0.000 |
| Online Religious Involvement → Anxiety | 1 | 0.409 | 0.000 |
| Spiritual Support → Depression | 1 | 2.275 | 0.000 |
| Spiritual Support → Anxiety | 1 | 1.182 | 0.000 |
| All constrained | 5 | 14.389 | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoo, J. Online Religious Involvement, Spiritual Support, Depression, and Anxiety during the COVID-19 Pandemic. Religions 2022, 13, 1052. https://doi.org/10.3390/rel13111052
Yoo J. Online Religious Involvement, Spiritual Support, Depression, and Anxiety during the COVID-19 Pandemic. Religions. 2022; 13(11):1052. https://doi.org/10.3390/rel13111052
Chicago/Turabian StyleYoo, Jieun. 2022. "Online Religious Involvement, Spiritual Support, Depression, and Anxiety during the COVID-19 Pandemic" Religions 13, no. 11: 1052. https://doi.org/10.3390/rel13111052
APA StyleYoo, J. (2022). Online Religious Involvement, Spiritual Support, Depression, and Anxiety during the COVID-19 Pandemic. Religions, 13(11), 1052. https://doi.org/10.3390/rel13111052