1. Introduction
On 27 February 2010, a large part of Chile was hit by an 8.8 Mw earthquake and tsunami. Over two million people were directly affected and around 370 thousand homes (11% of all homes in the earthquake area) were damaged or destroyed [
1].
The World Health Organization defines a disaster as a serious disruption of the normal functioning of a system or community, whose effects on people, material, economic or environmental losses and damage exceed the capacity of that society or community to cope and recover from the situation [
2].
From a psychosocial perspective, natural disasters are a major source of stress as they pose a threat to life and they destroy social structures [
3]. However, in a study conducted by Vázquez, Cervellón, Pérez-Sales, Vidales and Gaborit [
4], on survivors of the El Salvador earthquake in 2001, it was shown that the majority of survivors who lived in shelters experienced positive emotions (e.g., enjoying recreation time), that they were capable of finding meaning in what had happened, and that they considered themselves to be better prepared for future negative events. This indicates that traumas do not always have negative consequences or result in disorders; in some cases positive processes may be triggered. Consequently, Tedeschi and Calhoun [
5] suggest that some people who have suffered a highly stressful life event could experience a positive and significant change as a result of their struggle, a concept that they define as Posttraumatic Growth (PTG).
Furthermore, the perception of these positive changes after a traumatic event does not depend solely on how much time has passed; it has been linked to the nature of the traumatic event [
6]. The meta-analysis by Helgeson, Reynols and Tomich [
7] found a positive relationship between the objective and perceived severity of the trauma and PTG,
r = 0.07 and
r = 0.14, respectively (using Pearson’s r as the effect size metric). Along the same lines, García, Jaramillo, Martínez, Valenzuela and Cova [
8] found that subjective severity predicted a high level of PTG in university students affected by the earthquake in Chile, partially mediated by deliberate rumination. In contrast, García, Reyes and Cova [
9] examined the impact of the objective and subjective severity of the earthquake on PTG in Chile. They found that objective severity, as measured by the loss of a home, injury and the death of a loved one, has a negative impact on PTG. However, the relationship with subjective severity, as measured by how the trauma is perceived or by major disruptions to life following the event, is less clear because it presents a negative bivariate correlation with PTG but, when interacting with optimism, predicts a higher level of PTG.
Some PTG models [
10,
11] postulate that it is not the event severity
per se, but rather the tendency of people to examine their core beliefs when encountering extreme experiences that fuels growth. In fact a study with earthquake victims in the same context [
8] found that negative changes in basic beliefs about the self and the world were associated to PTG as this model proposes.
The positive impact of subjective severity on PTG could be explained by the fact that there can only be growth if people interpret their experience as a shattering or traumatic one [
7,
12], as this makes it possible to learn from it. Therefore, a traumatic impact would be required for PTG because it is likely that the very severity of the event leads to serious questioning of beliefs and suffering, which would be conducive to growth [
7]). One of the major psychosocial factors shown to have a positive relationship with PTG is social support. In their explanatory model of PTG, Tedeschi and Calhoun [
11] refer specifically to the different forms of social bonding as means for facilitating PTG. Prati and Pietrantoni [
13] meta-analysis confirmed the positive relationship between PTG and social support. This suggests that a high level of social support (subjective, informational, emotional and instrumental), following a traumatic event reduces its cognitive impact, allowing an individual to regulate his/her negative emotion, control dysfunctional behaviors, increase distraction and rewarding activities and solve practical problems better.
At the end of the eighties, Pargament [
14] started developing his religious coping model, which describes the way of coping that uses religious beliefs and behaviors to prevent and/or mitigate the negative consequences of stressful life events and to help resolve problems. These religious coping strategies may be used individually (personal prayer), or collectively (praying in groups, taking part in spiritual rituals). Hence, adaptation mechanisms are triggered by a personal relationship with God or a higher power that can give them hope at times of crisis [
15].
People can use religion to cope with a crisis in many ways: finding meaning, obtaining an opportunity for intimacy with others, reinforcing identity, increasing the perception of control, decreasing anxiety and searching for the sacred or spiritual in themselves [
16]. Religion serves as a mechanism to reduce the impact of disasters and increase adaptation to them, as it gives meaning to unforeseeable and uncontrollable events [
17]. It is also associated with increased longevity, higher self-esteem, lower suicide rates, less substance abuse and greater satisfaction with married life [
18].
Campos
et al. [
19] assert that, during crisis situations, increasing private rituals (praying, meditating and reading sacred texts) and public rituals (increased attendance at church) are very common coping strategies; for example, after the earthquake in El Salvador in 2001, 87% of the people surveyed said that they had used religious beliefs to cope with the situation [
4]. Furthermore, most of the people surveyed found an explanation for what had happened, chiefly based on their religious beliefs. After the earthquake in Chile in 2010, one survivor who had been buried under rubble described how his faith in God had helped him to go through the most difficult moments in that episode, to cope with the uncertainty of what was going to happen to him, to comfort him and to give meaning to what he was experiencing [
20]:
I talked to God all night and told Him about my fears and recalled many passages from the Bible; I remembered some of the experiences of the early fathers of the faith; which did not always have happy endings. (…) Generally; being a Christian does not necessarily mean that you are only going to experience positive things; to say so is to misunderstand the gospel; what matters is how we deal with bad things; as Christians we have the ability to cope well with unpleasant experiences; things that hurt us; and I was experiencing a painful situation and; at that moment; I could feel within that God was with me; because I felt at peace.
Regarding PTG, the meta-analyses by Helgeson
et al. [
7] and by Prati and Pietrantoni [
13] identify religious coping and spirituality as one of the factors that enhance growth. In particular, religious coping was strongly linked to PTG in the latter meta-analysis,
r = 0.38. A study performed by Gasparre, Bosco and Bellelli [
21], explored the effect of participating in spiritual rituals on posttraumatic stress levels in genocide survivors in Guatemala and also examined the relationship between these variables and seeking social support. The results confirmed that there was a positive relationship between taking part in rituals, social support and PTG. Similar findings were obtained by Campos
et al. [
19] who found that the people who prayed the most in the week following the 11-M terrorist attack in Madrid also sought more social support and reported higher coping by positive reappraisal. A positive relationship has also been found between religious coping and PTG in cancer patients [
22] and in survivors of natural disasters [
23]. It is important to be aware that religious participation (e.g., involvement in religious networks, participation in religious rituals) is similar to objective social support and potentially related to coping by searching social support. Religious coping is also strongly related with deliberate cognitive work to find meaning or coping by positive reappraisal.
However, Pargament
et al. [
16] warn that religious coping is multivalent as it can also have harmful results and, therefore, research into religious aspects must acknowledge that there are both advantages and disadvantages of having a religious attitude. Hence, Pargament
et al. [
15] distinguish between positive and negative religious coping. Positive religious coping leads to spiritual psychological satisfaction, spiritual support, religious purification, seeking support from priests or members of the church and religious forgiveness. However, negative religious coping is associated with a punitive religious perception (punishment from God), spiritual discontent (questioning the existence and sense of divine beings) and interpersonal religious discontent (annoyance with co-religionists and priests). Furthermore, even positive religious coping may reinforce resignation and a more passive form of coping when faced with difficulties, such as certain illnesses [
24]. Some models postulate that voluntary rumination, similar to reevaluation or positive cognitive change, helps to find meaning in stressful experiences [
25]. Thus, positive religious coping could be framed within that context. In fact, voluntary positive rumination was related to PTG in another study in a similar sample [
8].
If it is accepted that, after a traumatic event or natural disaster, a person may develop PTG-with key influencing factors being perceived severity, social support and religious coping—the question arises of how these variables affect people who have lost their homes due to an earthquake and now live in transitional shelters. Furthermore, given that one traditional explanation offered for the positive impact of religious coping on well-being and health is that religious activity is a source of social support [
16,
19], perceived social support will be examined to verify the specific link between adaptation to trauma and religious coping, controlling for level of social integration. Another central point of the study will be to evaluate the mediating role that positive religious coping would play between subjective severity and PTG, because severity should fuel positive searching of meaning by religion in order to afford benefit finding after a potential traumatic event
3. Results
The range, mean, standard deviation, and reliability of each measure are listed in
Table 1.
Table 1.
Ranges, Means and Standard Deviations of study variables (N = 116).
Table 1.
Ranges, Means and Standard Deviations of study variables (N = 116).
| Variables | Range | Mean | SD |
|---|
| Subjective severity | 0 | 8 | 5.42 | 2.51 |
| Positive Religious Coping | 7 | 49 | 29.55 | 13.96 |
| Negative Religious Coping | 7 | 49 | 19.61 | 10.81 |
| Social support from family | 10 | 56 | 44.97 | 12.15 |
| Social support from friends | 4 | 28 | 20.34 | 6.59 |
| Social support—Total | 16 | 84 | 65.31 | 16.89 |
| Posttraumatic Growth Self-perception | 4 | 60 | 42.84 | 13.94 |
| Posttraumatic Growth Interpersonal Relationship | 2 | 35 | 25.38 | 7.80 |
| Posttraumatic Growth Life Philosophy | 0 | 10 | 6.19 | 3.05 |
| Posttraumatic Growth—Total | 6 | 105 | 74.41 | 23.68 |
Using the student’s T-test for independent samples, no significant differences were found between sexes for total PTG or any of its subscales. Using a single-factor ANOVA test, four age range groups were compared: 18–30 (25.9%), 31–40 (23.3%), 42–55 (25.9%) and 56–80 (25%), with no significant differences between the groups for total PTG or any of its subscales being found.
Bivariate correlations show that all variables included had a significant correlation with PTG, with the exception of negative religious coping—see
Table 2.
Then a multiple linear regression analysis was performed, using enter procedure [
34]. The regression model for total PTG had an
R2 coefficient of 0.53 (
R2adj = 0.51) and was significant (
F4,111 = 30.849,
p < 0.001). The model indicates that there is a direct linear relationship between the predictors—subjective severity, total social support and positive religious coping—and the posttraumatic growth scores; the model’s coefficient values are shown on
Table 3.
Table 2.
Pearson’s r correlations between the study variables (N = 116).
Table 2.
Pearson’s r correlations between the study variables (N = 116).
| Variable | PR | NR | SS-Fam | SS-Fri | SS | PTG-SP | PTG-IR | PTG-LP | PTG |
|---|
| Sev | 0.34 *** | 0.40 *** | 0.05 | 0.18 * | 0.04 | 0.22 * | 0.13 | 0.33 *** | 0.21 * |
| PR | | 0.58 *** | 0.21 * | 0.01 | 0.15 | 0.42 *** | 0.38 *** | 0.66 *** | 0.46 *** |
| NR | | | 0.00 | 0.12 | 0.05 | 0.08 | 0.08 | 0.39 *** | 0.12 |
| SS-Fam | | | | 0.59 *** | 0.95 *** | 0.59 *** | 0.64 *** | 0.36 *** | 0.60 *** |
| SS-Fri | | | | | 0.81 *** | 0.44 *** | 0.48 *** | 0.16 | 0.44 *** |
| SS | | | | | | 0.59 *** | 0.65 *** | 0.32 *** | 0.60 *** |
| PTG-SP | | | | | | | 0.93 *** | 0.73 *** | 0.99 *** |
| PTG-IR | | | | | | | | 0.68 *** | 0.96 *** |
| PTG-LP | | | | | | | | | 0.78 *** |
Table 3.
Coefficients, levels of significance and semi-partial correlations, for the MLR model scores for the posttraumatic growth variable (n = 116; R2 = 0.53).
Table 3.
Coefficients, levels of significance and semi-partial correlations, for the MLR model scores for the posttraumatic growth variable (n = 116; R2 = 0.53).
| Variable | Unstandardized Coefficients | Standardized Coefficients | T value | Semi-partial correlation |
|---|
| B | Standard error | Beta |
|---|
| (Constant) | 3.15 | 7.37 | | 0.43 | |
| Subjective Severity | 1.46 | 0.68 | 0.15 | 2.14 * | 0.14 |
| Positive Religious Coping | 0.70 | 0.14 | 0.41 | 4.94 *** | 0.32 |
| Negative Religious Coping | −0.34 | 0.18 | −0.15 | −1.84 | −0.12 |
| Total Support Social | 0.76 | 0.09 | 0.54 | 8.03 *** | 0.52 |
A multiple linear regression analysis was also performed with each subscale of PTG, showing that Social Support and Positive Religious Coping predict Interpersonal Relationship and Life Philosophy changes. Negative Religious Coping was a negative predictor of Self-perception (see
Table 4,
Table 5 and
Table 6).
Table 4.
Coefficients, levels of significance and semi-partial correlations, for the MLR model scores for the posttraumatic growth self-perception variable (n = 116; R2 = 0.50).
Table 4.
Coefficients, levels of significance and semi-partial correlations, for the MLR model scores for the posttraumatic growth self-perception variable (n = 116; R2 = 0.50).
| Variable | Unstandardized Coefficients | Standardized Coefficients | T value | Semi-partial correlation |
|---|
| B | Standard error | Beta |
|---|
| (Constant) | 2.20 | 4.46 | | 0.49 | |
| Subjective Severity | 1.01 | 0.41 | 0.18 | 2.45 * | 0.16 |
| Positive Religious Coping | 0.39 | 0.09 | 0.39 | 4.54 *** | 0.30 |
| Negative Religious Coping | −0.25 | 0.11 | −0.20 | −2.26 * | −0.15 |
| Total Support Social | 0.44 | 0.06 | 0.53 | 7.70 *** | 0.52 |
Table 5.
Coefficients, levels of significance and semi-partial correlations, for the MLR model scores for the posttraumatic growth interpersonal relationship variable (n = 116; R2 = 0.51).
Table 5.
Coefficients, levels of significance and semi-partial correlations, for the MLR model scores for the posttraumatic growth interpersonal relationship variable (n = 116; R2 = 0.51).
| Variable | Unstandardized Coefficients | Standardized Coefficients | T value | Semi-partial correlation |
|---|
| B | Standard error | Beta |
|---|
| (Constant) | 2.29 | 2.47 | | 0.93 | |
| Subjective Severity | 0.28 | 0.23 | 0.09 | 1.21 | 0.08 |
| Positive Religious Coping | 0.18 | 0.05 | 0.33 | 3.87 *** | 0.26 |
| Negative Religious Coping | −0.09 | 0.06 | −0.12 | −1.42 | −0.09 |
| Total Support Social | 0.27 | 0.03 | 0.59 | 8.68 *** | 0.58 |
Table 6.
Coefficients, levels of significance and semi-partial correlations, for the MLR model scores for the posttraumatic growth life philosophy variable (n = 116; R2 = 0.51).
Table 6.
Coefficients, levels of significance and semi-partial correlations, for the MLR model scores for the posttraumatic growth life philosophy variable (n = 116; R2 = 0.51).
| Variable | Unstandardized Coefficients | Standardized Coefficients | T value | Semi-partial correlation |
|---|
| B | Standard error | Beta |
|---|
| (Constant) | −1.35 | 0.97 | | −1.39 | |
| Subjective Severity | 0.17 | 0.09 | 0.14 | 1.93 | 0.13 |
| Positive Religious Coping | 0.13 | 0.02 | 0.58 | 6.78 *** | 0.45 |
| Negative Religious Coping | 0.00 | 0.02 | 0.00 | 0.03 | 0.00 |
| Total Support Social | 0.04 | 0.01 | 0.24 | 3.54 *** | 0.24 |
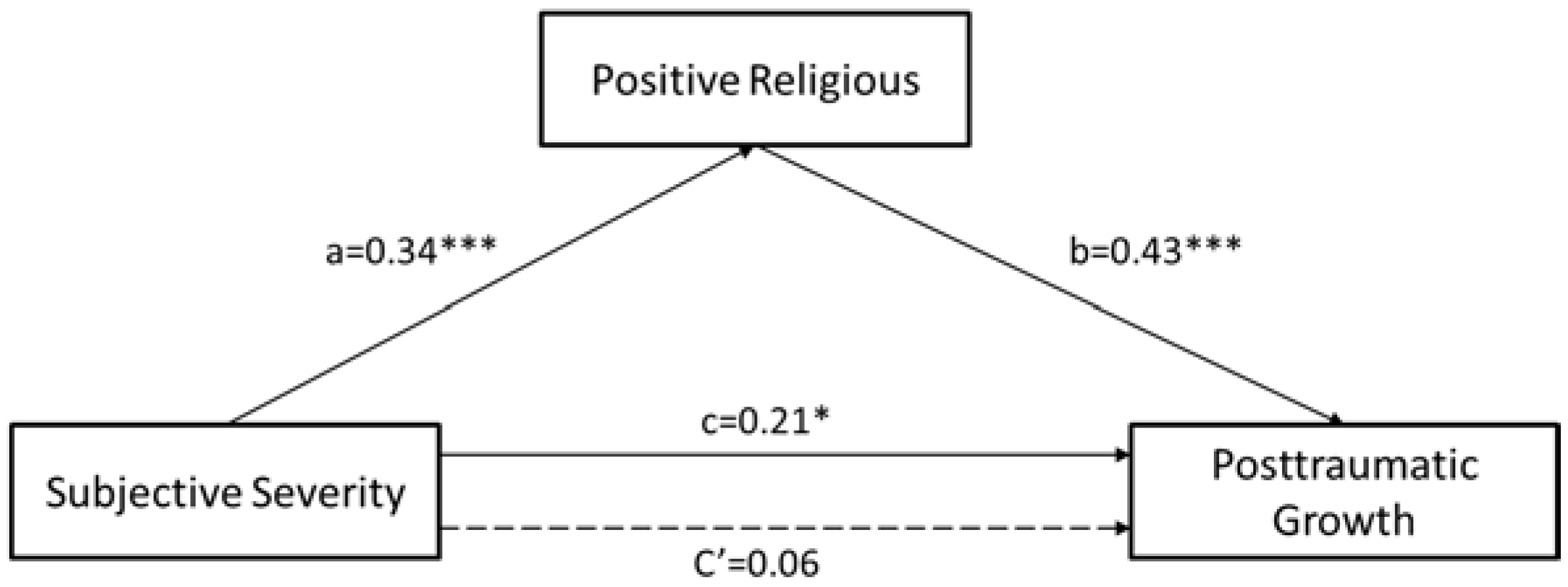
To contrast the mediation role of positive religious coping between subjective severity and PTG, a bias-corrected bootstrap estimate was performed with a confidence interval of 95%. Using 5000 bootstrap resamples [
35]. MacKinnon, Lockwood and Williams [
36] indicated that this method is the best statistical test to determine whether mediation is significant, compared with other alternative tests. In this case, mediation exists if the confidence interval does not contain zero. The true indirect effect was estimated to lie between 0.67 and 2.45 CI (
M = 1.40;
SE = 0.45). Since zero is not in the 95% confidence interval for the analyses, it can be concluded that the indirect effects were significantly different from zero at
p < 0.05 and that the relationship between PTG and severity is fully mediated by positive religious coping (see
Figure 1).
Figure 1.
Mediation model. Shown above are the standardized regression coefficients for each path of the model.
Figure 1.
Mediation model. Shown above are the standardized regression coefficients for each path of the model.
* p < 0.05; *** p < 0.001.
4. Discussion
Neither significant sex differences nor age differences were found. This differs from studies that show that women present higher levels of PTG than men, and young people have higher levels than adults (see [
7,
37]). Steward [
38] indicates that women report higher PTG for less intense events and men report higher PTG for more intense events. In turn, Cieslak
et al. [
39] find no relationship between the sex and age of the population affected by a natural disaster, so it can be concluded that in a community that has been hit by an earthquake and the loss of homes and whose precarious situation is still yet to be resolved three years after the disaster, the likelihood of experiencing growth is the same for men and women.
Regarding age, although the meta-analysis by Helgeson
et al. [
7] found an insignificant relationship with PTG, other studies have mixed results. For example, PTG has been shown to have a positive relationship with age in cases of abuse [
40], a negative relationship in catastrophic illnesses [
41] and no relationship in natural disasters [
39], so it appears that the relationship between these variables is affected by the type of event and its severity, among other criteria.
Correlations show that there are differences between the PTG subscales. Congruently, religious coping is strongly associated to PTG-LP, a more ideological form of growth, while social support show stronger correlations with PTG-IR, a form of growth intrinsically related to social integration. However, showing the importance of belongingness and social support for psychological well-being, PTG-SP or perception of positive changes in the self-concept is also strongly related to social support. Finally, negative religious coping is directly associated with PTG-LP, suggesting that religious doubt and critical reflection promote changes to life philosophies. Severity does not show a significant relationship with PTG-IR and social support from friends does not have a significant relationship with PTG-LP.
Additionally, excluding social support from the family, which is associated with positive religious coping, no relationship has been found between perceived social support and religious coping. Social support is most strongly associated with interpersonal growth, as discussed above, thus showing its importance for this type of growth, and it is less strongly associated with a growth in life philosophy.
The results show that all psychological variables included in the study show significant relationships with PTG, with the exception of negative religious coping, as expected. This makes it necessary to carefully examine other studies that show a relationship between religious coping and PTG because, if these studies do not take into account the attitude of a person or even a social group or culture towards religion—whether seen as a source of support and comfort or a source of punishment and persecution—the conclusions may be distorted. It is pertinent to compare inhabitants of Spain who were hit by an earthquake and for whom religious coping did not affect growth [
42], and the Chilean population in this study, for whom it did, but only where the attitude towards religious coping was positive. This intercultural difference may be due to the different levels of secularization in European and Latin American cultures [
4,
43], but it may also be a result of the attitude of civil society towards religious institutions, which is probably more negative in Spain than in Chile due to historical and political factors [
44].
The impact of perceived social support on growth has also been confirmed, as already found in other studies and meta-analyses [
7,
13]. However, the low correlation between social support and subjective severity and between social support and religious coping does not suggest that it performs a mediating role between them and PTG. Although it may be believed that social support could be performing a moderating role and that strong support would, for example, reduce the relationship between severity and growth, this was not confirmed (analyses not shown).
Objective and subjective resource loss are significant mediators of PTG. In this sample, objective index of resource loss was not available, but subjective severity could be conceived as proxy to subjective resource loss. Moreover, because the sample included only displaced people, basic resource loss (like the destruction of house) was a homogeneous phenomenon.
The findings are also important because they show that positive religious coping itself is specifically associated with PTG, even when social support is controlled, a process traditionally used to explain the beneficial effects of religious coping. However, the multivariate predictive coefficient of PTG was higher for social support than for religious coping—although the meta-analysis by Prati and Pietrantoni [
13] found the opposite. This shows that social support is an important factor in itself for PTG, much like religious coping.
It was also confirmed that the hypothesis of positive religious coping fully mediating between subjective severity and PTG. The relationship between severity and growth has been the subject of many studies, which have tried to explain why people who appraise an event as significant and unpleasant could develop posttraumatic growth after it. This study found that severity does not have a direct effect on growth but is mediated by psychological processes, such as positive religious coping, in addition to other mediators, such as deliberate rumination [
8], or moderators, such as optimism [
9].
There are some important limitations to the study, which must be considered when generalizing these findings. Firstly, the sample is small; three years after the event, there are not many shelters left and some of them have been over-evaluated and over-analyzed, thus limiting the population that could be surveyed for this study. Secondly, although this study hypothesizes on the relationships of influence between the variables, it must be remembered that this is a cross-sectional design, i.e., all instruments were used in a single moment of time, and so it is impossible to estimate causal relationships between the variables. Thirdly, the three years that have elapsed since the event may have affected the results, due to emotional factors associated with subjective memories of the event. Fourthly, another limitation of the study is the lack of a random sample, which limits the ability to make comparisons to studies that have used random samples from a population. Finally, the experience of the years since the disaster is another probable mediator of the estimation of loss, perception of support, and estimation of the severity of trauma. However in this sample years from the disaster was a constant because people were affected in the same period.
The findings of this study contribute to scientific knowledge regarding the influence of religious coping, severity and social support on the posttraumatic growth of people affected by natural disasters. Due to the frequency with which natural disasters occur in Chile and the world, it is important to gain scientific knowledge to make further progress and take steps to reduce the negative impact of these phenomena from a biopsychosocial perspective, thus enhancing protective factors.


{kind=link}
