Factor Structure of the Spiritual Needs Questionnaire (SpNQ) in Persons with Chronic Diseases, Elderly and Healthy Individuals

 ,
,  ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Factorial Structure of the SpNQ in Persons with Chronic Diseases, Elderly and Healthy Persons
3. Materials and Methods
3.1. Participants
3.2. Methods
3.3. Spiritual Needs Questionnaire
3.4. Factor Structure in the Different Samples
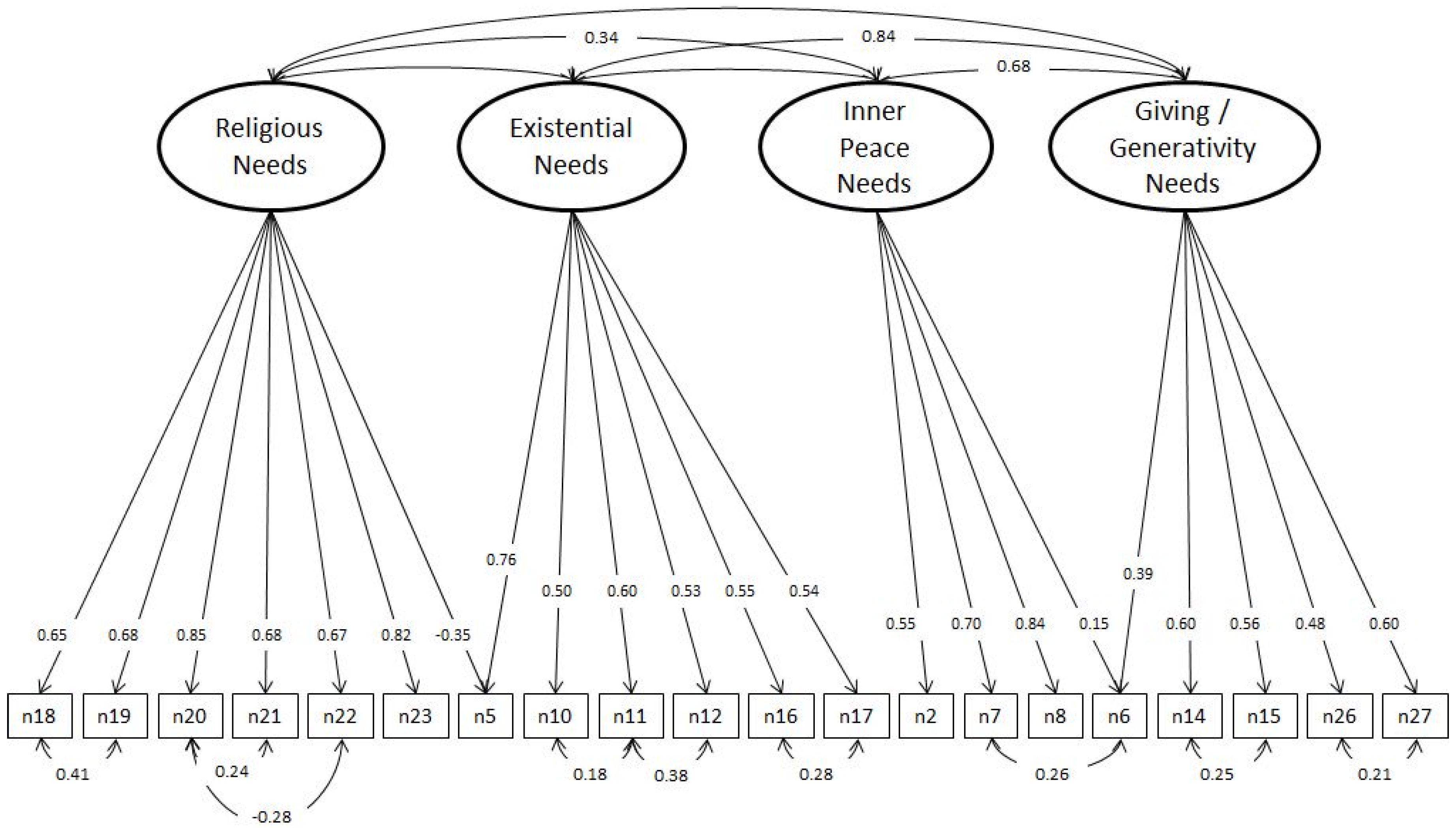
3.5. Structured Equation Modelling
3.6. Differences between the Mean Scores of Previous and Current Version of the SpNQ
3.7. Profiles of Unmet Needs
- For Religious Needs, there were age (F = 23.8; p < 0.0001) and gender (F = 13.4; p < 0.0001) differences, but not disease/healthy differences (F = 2.2; p = 0.139). No significant interaction effects were present.
- For Existential Needs, there were significant gender (F = 13.6; p < 0.0001) and disease/healthy (F = 7.8; p = 0.005) differences, but differences in age were only at the trend level (F = 3.0; p = 0.010). There was a difference at the trend level for the combined effect of all three variables (F = 2.9; p = 0.013).
- For Inner Peace Needs, there were significant gender (F = 13.8; p < 0.0001) and disease/healthy (F = 9.8; p = 0.002) differences, but not for age (F = 1.9; p = 0.096). Again, there was a difference at the trend level for the combined effects of all three variables (F = 2.7; p = 0.018).
- For Giving/Generativity Needs, only a significant difference was found for age (F = 7.9; p < 0.0001), not for gender (F = 3.5; p = 0.062) or disease/healthy (F = 1.7; p = 0.197). There were no significant interaction effects for these three variables (F = 2.1; p = 0.064).
4. Discussion
5. Associations with Spirituality and Quality of Life
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Asparouhov, Tihomir, and Bengt Muthén. 2009. Exploratory structural equation modeling. Structural Equation Modeling 16: 397–438. [Google Scholar] [CrossRef]
- Balboni, Tracy A., Lauren C. Vanderwerker, Susan D. Block, M. Elizabeth Paulk, Christopher S. Lathan, John R. Peteet, and Holly G. Prigerson. 2007. Religiousness and spiritual support among advanced cancer patients and associations with end-of-life treatment preferences and quality of life. Journal of Clinical Oncology 25: 555–60. [Google Scholar] [CrossRef] [PubMed]
- Büssing, Arndt. 2010. Measures of Spirituality in Health Care. In Oxford Textbook of Spirituality in Healthcare. Edited by Mark R. Cobb, Christina M. Puchalski and Bruce Rumbold. Oxford: Oxford University Press, pp. 323–31. ISBN 978-0-19-957139-0. [Google Scholar]
- Büssing, Arndt, and Harold G. Koenig. 2010. Spiritual Needs of Patients with Chronic Diseases. Religions 1: 18–27. [Google Scholar] [CrossRef]
- Büssing, Arndt, and Daniela Rodrigues Recchia. 2016. Spiritual and Non-spiritual Needs Among German Soldiers and their Relation to Stress Perception, PTDS Symptoms, and Life Satisfaction—Results from a Structural Equation Modeling Approach. Journal of Religion and Health 55: 747–64. [Google Scholar]
- Büssing, Arndt, Hans-Joachim Balzat, and Peter Heusser. 2009. Spirituelle Bedürfnisse von Patienten mit chronischen Schmerz- und Tumorerkrankungen. Perioperative Medizin 1: 248. [Google Scholar] [CrossRef]
- Büssing, Arndt, Hans-Joachim Balzat, and Peter Heusser. 2010. Spiritual needs of patients with chronic pain diseases and cancer—Validation of the spiritual needs questionnaire. European Journal of Medical Research 15: 266–73. [Google Scholar]
- Büssing, Arndt, Annina Janko, Andreas Kopf, Eberhard Albert Lux, and Eckhard Frick. 2012. Zusammenhänge zwischen psychosozialen und spirituellen Bedürfnissen und Bewertung von Krankheit bei Patienten mit chronischen Erkrankungen. Spiritual Care 1: 57–73. [Google Scholar]
- Büssing, Arndt, Annina Janko, Klaus Baumann, Niels Christian Hvidt, and Andreas Kopf. 2013a. Spiritual Needs among Patients with Chronic Pain Diseases and Cancer Living in a Secular Society. Pain Medicine 14: 1362–73. [Google Scholar]
- Büssing, Arndt, Zhai Xiao-Feng, Wen-bo Peng, and Chang-quan Ling. 2013b. Psychosocial and spiritual needs of patients with chronic diseases: Validation of the Chinese version of the Spiritual Needs Questionnaire. Journal of Integrative Medicine 11: 106–15. [Google Scholar] [CrossRef] [PubMed]
- Büssing, Arndt, Iwoan Pilchowska, and Janusz Surzykiewicz. 2015. Spiritual Needs of Polish patients with chronic diseases. Journal of Religion and Health 54: 1524–42. [Google Scholar] [CrossRef] [PubMed]
- Büssing, Arndt, Undine Wassermann, Niels Christian Hvidt, Alfred Längler, and Michael Thiel. 2017. Spiritual needs of mothers with sick new born or premature infants. Woman and Birth. [Google Scholar] [CrossRef] [PubMed]
- Erichsen, Nora Beata, and Arndt Büssing. 2013. Spiritual Needs of Elderly living in Retirement/Nursing Homes. Evidence-Based Complementary and Alternative Medicine, 913247. [Google Scholar] [CrossRef]
- Frick, Eckhard, Carola Riedner, Martin J. Fegg, S. Hauf, and Gian Domenico Borasio. 2006. A clinical interview assessing cancer patients’ spiritual needs and preferences. European Journal of Cancer Care 15: 238–43. [Google Scholar] [CrossRef] [PubMed]
- Glavas, Andrijana, Karin Jors, Arndt Büssing, and Klaus Baumann. 2017. Spiritual needs of PTSD patients in Croatia and Bosnia-Herzegovina: A quantitative pilot study. Psychiatria Danubina 29: 282–90. [Google Scholar] [CrossRef] [PubMed]
- Hatamipour, Khadijeh, Maryam Rassouli, Farideh Yaghmaie, Kazem Zendedel, and Hamid Alavi Majd. 2018. Development and Psychometrics of a ‘Spiritual Needs Assessment Scale of Patients with Cancer’: A mixed exploratory study. International Journal of Cancer Management. in press. [Google Scholar]
- Haußmann, Annette, Norbert Schäffeler, Martin Hautzinger, Birgit Weyel, Thomas Eigentler, Stephan Zipfel, and Martin Teufel. 2017. Religiöse/spirituelle Bedürfnisse und psychosoziale Belastung von Patienten mit malignem Melanom. Psychotherapie, Psychosomatik, Medizinische Psychologie 67: 413–19. [Google Scholar] [CrossRef] [PubMed]
- Höcker, Anja, Andreas Krüll, Uwe Koch, and Anja Mehnert A. 2014. Exploring spiritual needs and their associated factors in an urban sample of early and advanced cancer patients. European Journal of Cancer Care 23: 786–94. [Google Scholar] [CrossRef] [PubMed]
- Man-Ging, Carlos Ignacio, Jülyet Öven Uslucan, Martin Fegg, Eckhard Frick, and Arndt Büssing. 2015. Reporting Spiritual Needs of Older Adults Living in Bavarian Residential and Nursing Homes. Journal of Mental Health, Religion and Spirituality 18: 809–21. [Google Scholar] [CrossRef]
- Munirruzzaman, Muhammad, Yuni Sapto Edi R, and Ahus Prasetyo. 2017. Gambaran Tingkat Kebutuhan Spiritual Pada Pasien Gagal Ginjal Kronik Yang Menjalani Hemodialisis Di Ruang Hemodialisa Rsud Cilacap. In Proceeding Management Communication in Health Team Collaboration of Giving High Alert for Patient Safety. Cilacap: STIKES Al-Irsyad Al-Islamiyyah Cilacap, pp. 1–8. ISBN 978-602-60725-1-1. [Google Scholar]
- Nejat, Nazi, Lisa Whitehead, and Marie Crowe. 2016. Exploratory Psychometric Properties of the Farsi and English Versions of the Spiritual Needs Questionnaire (SpNQ). Religions 7: 84. [Google Scholar] [CrossRef]
- Nuraeni, Aan, Ikeu Nurhidayah, Nuroktavia Hidayati, Citra Windani Mambang Sari, and Ristina Mirwanti. 2015. Kebutuhan Spiritual pada Pasien Kanker. Jurnal Keperawatan Padjadjaran 3: 57–66. Available online: http://jkp.fkep.unpad.ac.id/index.php/jkp/article/view/101 (accessed on 10 December 2017). [CrossRef]
- Offenbaecher, Martin, Nico Kohls, Loren L. Toussaint, Claudia Sigl, Andreas Winkelmann, Robin Hieblinger, Albrecht Walther, and Arndt Büssing. 2013. Spiritual needs in patients suffering from fibromyalgia. Evidence-Based Complementary and Alternative Medicine, 178547. [Google Scholar] [CrossRef] [PubMed]
- Puchalski, Christina, Betty Ferrell, Rose Virani, Shirley Otis-Green, Pamela Baird, Janet Bull, Harvey Chochinov, George Handzo, Holly Nelson-Becker, Maryjo Prince-Paul, and et al. 2009. Improving the quality of spiritual care as a dimension of palliative care: The report of the Consensus Conference. Journal of Palliative Medicine 12: 885–904. [Google Scholar] [CrossRef] [PubMed]
- Seddigh, Ruohollah, Amir-Abbas Keshavarz-Akhlaghi, and Somayeh Azarnik. 2016. Questionnaires Measuring Patients’ Spiritual Needs: A Narrative Literature Review. Iranian Journal of Psychiatry and Behavioral Sciences 10: e4011. [Google Scholar] [CrossRef] [PubMed]
- Valente, Tania Christina de Oliveira, Ana Paula R. Cavalcanti, Arndt Büssing, and Clóvis Pereira da Costa Júnior. 2018. Transcultural adaptation and psychometric properties of Portuguese version of the Spiritual Needs Questionnaire among HIB positive patients in Brasil. Paper presented at 6th European Conference on Religion, Spirituality and Health and 5th International Conference of the British Association for the Study of Spirituality, Coventry, UK, May 17–19. forthcoming. [Google Scholar]


{kind=link}
| Patients with Chronic Diseases | Healthy Persons | Elderly in Retirement Homes | All Persons | ||
|---|---|---|---|---|---|
| Number of persons | 627 | 1158 | 313 | 2095 | |
| Gender | Women | 65.5% | 18.0% | 76.0% | 40.4% |
| Men | 34.5% | 82.0% | 24.0% | 59.6% | |
| All | 100.0% | 100.0% | 100.0% | 100.0% | |
| Age groups | <31 years | 6.5% | 39.1% | 0.0% | 24.5% |
| 31–40 years | 9.0% | 36.2% | 0.0% | 23.4% | |
| 41–50 years | 23.1% | 19.1% | 0.0% | 17.1% | |
| 51–60 years | 27.6% | 5.6% | 0.6% | 10.5% | |
| 60–70 years | 19.0% | 0.0% | 3.9% | 5.5% | |
| >70 years | 14.9% | 0.0% | 95.5% | 18.9% | |
| All | 100.0% | 100.0% | 100.0% | 100.0% | |
| Persons with Chronic Diseases (n = 627) | Persons with Chronic Diseases + Elderly (n = 940) | Healthy Persons (n = 1468) | All Persons (n = 2095) | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 1 | 2 | 3 | 4 | 5 | 1 | 2 | 3 | 4 | 5 | 1 | 2 | 3 | 4 | |
| Cronbach’s alpha | 0.88 | 0.77 | 0.75 | 0.74 | 0.87 | 0.66 | 0.71 | 0.68 | 0.70 | 0.87 | 0.66 | 0.69 | 0.64 | 0.60 | 0.87 | 0.73 | 0.74 | 0.71 |
| N20 pray for yourself | 0.797 | 0.824 | 0.837 | 0.828 | ||||||||||||||
| N23 turn to a higher presence (i.e., God, Allah, Angels) | 0.745 | 0.773 | 0.780 | 0.784 | ||||||||||||||
| N21 participate at a religious ceremony (i.e., service) | 0.812 | 0.816 | 0.772 | 0.764 | ||||||||||||||
| N18 pray with someone | 0.782 | 0.744 | 0.765 | 0.755 | ||||||||||||||
| N19 someone prays for you | 0.775 | 0.747 | 0.746 | 0.746 | ||||||||||||||
| N22 read religious/spiritual books | 0.603 | 0.335 | 0.605 | 0.618 | 0.642 | |||||||||||||
| N17 be forgiven | 0.313 | 0.534 | 0.707 | 0.769 | 0.682 | |||||||||||||
| N16 forgive someone from a distinct period of your life | 0.503 | 0.348 | 0.639 | 0.731 | 0.641 | 0.349 | ||||||||||||
| N5 dissolve open aspects of your life | 0.515 | 0.381 | 0.666 | 0.670 | 0.563 | |||||||||||||
| N11 talk about the question of meaning in life | 0.758 | 0.752 | 0.801 | 0.316 | 0.364 | 0.541 | ||||||||||||
| N12 talk about the possibility of life after death | 0.351 | 0.644 | 0.706 | 0.745 | 0.381 | 0.534 | ||||||||||||
| N10 find meaning in illness and/or suffering | 0.608 | 0.592 | 0.335 | 0.441 | 0.457 | 0.371 | ||||||||||||
| N7 dwell at a place of quietness and peace | 0.801 | 0.369 | 0.713 | 0.766 | 0.762 | |||||||||||||
| N6 plunge into beauty of nature | 0.755 | 0.363 | 0.702 | 0.470 | 0.469 | 0.590 | ||||||||||||
| N8 find inner peace | 0.381 | 0.721 | 0.478 | 0.653 | 0.743 | 0.721 | 0.408 | |||||||||||
| N2 talk with someone about fears and worries | 0.390 | 0.373 | 0.483 | 0.301 | 0.313 | 0.610 | 0.576 | 0.337 | ||||||||||
| N26 pass own life experiences to others | 0.789 | 0.668 | 0.565 | 0.626 | ||||||||||||||
| N27 assured that your life was meaningful and of value | 0.730 | 0.613 | 0.459 | 0.534 | ||||||||||||||
| N15 give solace to someone | 0.599 | 0.338 | 0.646 | 0.719 | 0.698 | |||||||||||||
| N14 give away something from yourself | 0.365 | 0.520 | 0.317 | 0.631 | 0.729 | 0.661 | ||||||||||||
| Religious Needs | Existential Needs | Inner Peace Needs | Giving/Generativity Needs | |||||
|---|---|---|---|---|---|---|---|---|
| Version 2.1 | New SpNQ-20 | Version 2.1 | New SpNQ-20 | Version 2.1 | New SpNQ-20 | Version 2.1 | New SpNQ-20 | |
| Mean | 0.51 | 0.51 | 0.55 | 0.48 | 1.21 | 1.23 | 1.09 | 1.00 |
| SD | 0.74 | 0.74 | 0.62 | 0.61 | 0.79 | 0.90 | 0.87 | 0.82 |
| Religious Needs | Existential Needs | Inner Peace Needs | Giving/Generativity Needs | ||
|---|---|---|---|---|---|
| Healthy/Diseased | |||||
| Non-diseased (healthy) persons (n = 1468) | Mean | 0.46 | 0.36 | 1.05 | 0.90 |
| SD | 0.71 | 0.49 | 0.82 | 0.76 | |
| Chronically diseased persons (n = 627) | Mean | 0.61 | 0.77 | 1.64 | 1.28 |
| SD | 0.80 | 0.75 | 0.93 | 0.89 | |
| All persons (n = 2085) | Mean | 0.51 | 0.48 | 1.23 | 1.01 |
| SD | 0.74 | 0.61 | 0.90 | 0.82 | |
| F value | 17.3 | 213.6 | 208.5 | 99.3 | |
| p value | <0.0001 | <0.0001 | <0.0001 | <0.0001 | |
| Gender | |||||
| Women (n = 826) | Mean | 0.78 | 0.64 | 1.49 | 1.18 |
| SD | 0.84 | 0.67 | 0.87 | 0.85 | |
| Men (n = 1219) | Mean | 0.32 | 0.37 | 1.04 | 0.88 |
| SD | 0.60 | 0.53 | 0.86 | 0.77 | |
| All persons (n = 2045) | Mean | 0.51 | 0.48 | 1.22 | 1.00 |
| SD | 0.74 | 0.60 | 0.89 | 0.81 | |
| F value | 209.2 | 103.3 | 137.0 | 66.8 | |
| p value | <0.0001 | <0.0001 | <0.0001 | <0.0001 | |
| Age groups | |||||
| <31 years (n = 482) | Mean | 0.78 | 0.64 | 1.49 | 1.18 |
| SD | 0.23 | 0.31 | 0.92 | 0.71 | |
| 31–40 years (n = 462) | Mean | 0.48 | 0.45 | 0.78 | 0.68 |
| SD | 0.30 | 0.38 | 1.18 | 0.83 | |
| 41–50 years (n = 338) | Mean | 0.56 | 0.53 | 0.87 | 0.73 |
| SD | 0.44 | 0.49 | 1.28 | 1.03 | |
| 51–60 years (n = 207) | Mean | 0.69 | 0.65 | 0.98 | 0.84 |
| SD | 0.56 | 0.72 | 1.62 | 1.25 | |
| 61–70 years (n = 109) | Mean | 0.74 | 0.76 | 0.95 | 0.85 |
| SD | 0.80 | 0.75 | 1.62 | 1.49 | |
| >70 years (n = 373) | Mean | 0.86 | 0.77 | 0.85 | 0.88 |
| SD | 1.06 | 0.54 | 1.25 | 1.27 | |
| All ages (n = 1971) | Mean | 0.89 | 0.57 | 0.82 | 0.81 |
| SD | 0.51 | 0.47 | 1.22 | 1.00 | |
| F value | 80.2 | 22.8 | 25.3 | 39.9 | |
| p value | <0.0001 | <0.0001 | <0.0001 | <0.0001 | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Büssing, A.; Recchia, D.R.; Koenig, H.; Baumann, K.; Frick, E. Factor Structure of the Spiritual Needs Questionnaire (SpNQ) in Persons with Chronic Diseases, Elderly and Healthy Individuals. Religions 2018, 9, 13. https://doi.org/10.3390/rel9010013
Büssing A, Recchia DR, Koenig H, Baumann K, Frick E. Factor Structure of the Spiritual Needs Questionnaire (SpNQ) in Persons with Chronic Diseases, Elderly and Healthy Individuals. Religions. 2018; 9(1):13. https://doi.org/10.3390/rel9010013
Chicago/Turabian StyleBüssing, Arndt, Daniela Rodrigues Recchia, Harold Koenig, Klaus Baumann, and Eckhard Frick. 2018. "Factor Structure of the Spiritual Needs Questionnaire (SpNQ) in Persons with Chronic Diseases, Elderly and Healthy Individuals" Religions 9, no. 1: 13. https://doi.org/10.3390/rel9010013
APA StyleBüssing, A., Recchia, D. R., Koenig, H., Baumann, K., & Frick, E. (2018). Factor Structure of the Spiritual Needs Questionnaire (SpNQ) in Persons with Chronic Diseases, Elderly and Healthy Individuals. Religions, 9(1), 13. https://doi.org/10.3390/rel9010013