

Empower Psychotherapy with mHealth Apps: The Design of “Safer”, an Emotion Regulation Application

Abstract
1. Introduction
- Information and education apps (the early 2000s–present): These apps provide users with health-related information, educational content, and guidelines. They may cover various topics, such as general health, nutrition, fitness, and disease-specific information. The emergence of these apps coincided with the early years of smartphone usage and the growing accessibility to the internet on mobile devices.
- Remote monitoring and telemedicine apps (mid-to-late 2000s–present): As mobile technology advanced, apps were developed to enable remote monitoring of patients, sharing health data with healthcare providers, and facilitating telemedicine consultations. These apps allow for better management of chronic conditions, such as diabetes or hypertension, and improved access to healthcare services, especially in remote or underserved areas.
- Personal health tracking and fitness apps (late 2000s–present): These apps gained popularity with the rise of wearable devices and sensors, such as fitness trackers and smartwatches. They help users monitor their physical activities, sleep patterns, heart rates, and other health parameters. They often provide personalized feedback, goal setting, and progress tracking to motivate users to maintain a healthy lifestyle.
- Mental health and well-being apps (2010s–present): Growing awareness of mental health issues and the increasing need for accessible mental health resources have led to the development of apps focusing on mental well-being. These apps typically offer services such as mood tracking, mindfulness exercises, cognitive-behavioral therapy (CBT) techniques, and stress reduction tools.
- Social networking and support group apps (2010s–present): With the ubiquity of social media platforms, mHealth apps started incorporating social networking features to create online communities and support groups. Users can share their experiences, provide mutual support, and connect with others dealing with similar health conditions or goals.
- Artificial intelligence (AI)-powered and personalized health apps (late 2010s–present): The latest generation of mHealth apps leverages AI, machine learning, and big data analytics to offer personalized health recommendations, symptom analysis, and treatment options. These apps can analyze a user’s health data and offer tailored suggestions, improving the overall user experience and effectiveness of the app.
2. An Overview of Mental Health Mobile Apps
2.1. Emotional Help Assistants
2.2. Mood Trackers
2.3. Mindfulness Apps
2.4. Self-Care Apps
2.5. Behavior Change Applications
2.6. Apps with Treatment Elements
3. Mobile App Adjunction to Psychotherapy
Challenges in the Use of mHealth Apps for Treatment
4. Integrating Mobile Technology in Psychotherapy and Vice Versa
5. The Design of an Emotion Regulation Application
5.1. Focus on Emotion Regulation
5.2. Theoretical Background
- Emotional awareness: The ability to recognize and identify emotions.
- Emotional regulation: The ability to manage emotions effectively and to use coping strategies to reduce emotional intensity.
- Acceptance: The ability to accept negative emotions without judgment or negative reaction.
- Stress tolerance skills: The ability to manage emotional stress without acting impulsively or engaging in self-harming behaviors.
5.3. Safer Design Pattern
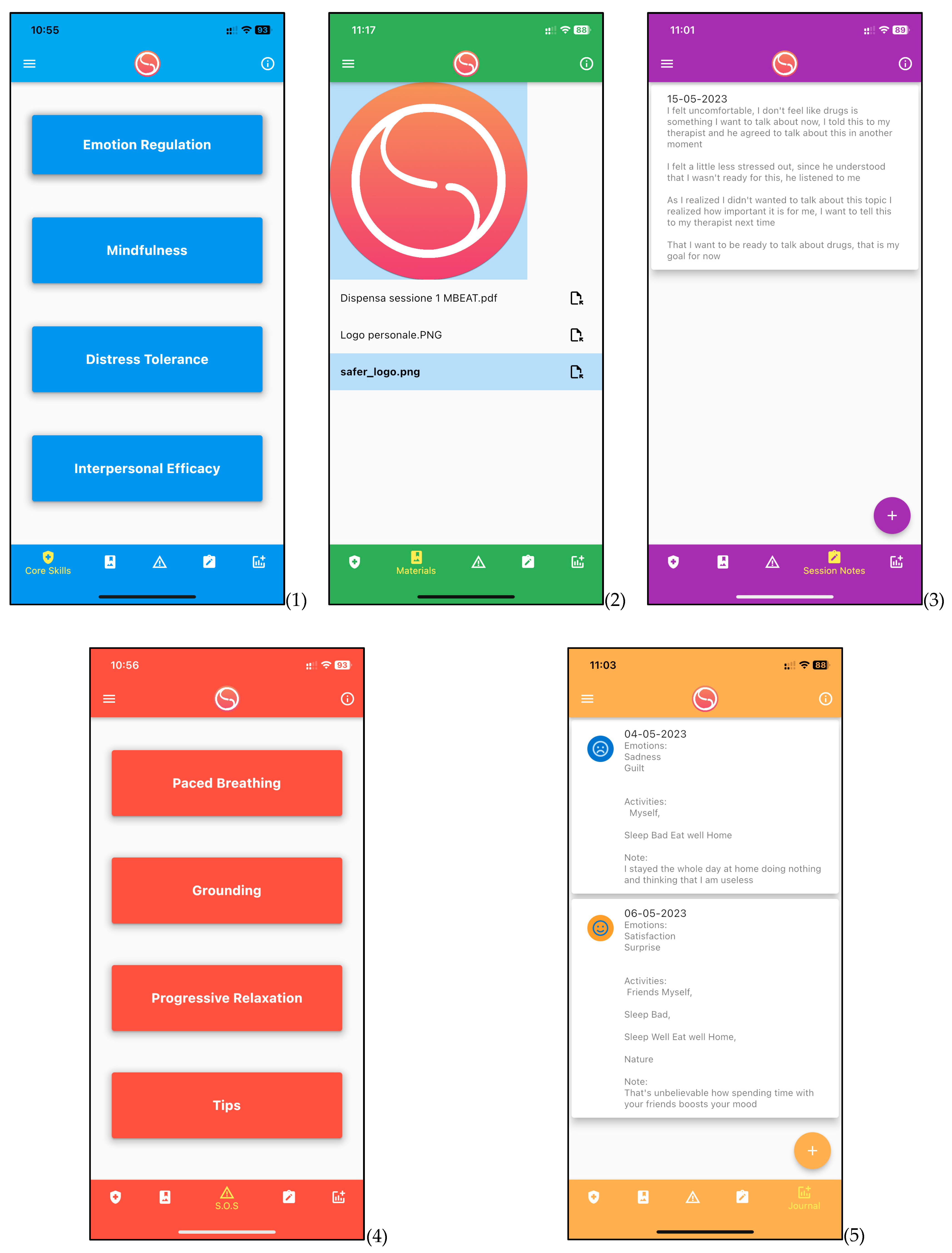
5.4. The Structure of the Application
- Distress tolerance: These skills help individuals endure and accept difficult or painful situations without reacting impulsively or in a self-destructive way. They include relaxation techniques, distraction, improvement of the present moment, and a reality check.
- Emotion regulation: These skills help individuals identify, understand and effectively manage their emotions. They include observing and describing emotions, reducing emotional vulnerability, increasing positive experiences, and modifying unwanted emotions.
- Interpersonal effectiveness: These skills help individuals establish and maintain healthy relationships, communicate effectively, and resolve conflicts. They include the ability to make requests, say no, set boundaries, and maintain self-esteem in social interactions.
- Mindfulness: These skills help individuals develop greater awareness of the present moment, of their emotions, thoughts, and bodily sensations. They include focused attention, non-judgmental observation, description, and full participation in the present experience and are presented both as self-reflection exercises and audio tracks of guided meditations.
6. Conclusions and Future Research
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
| Acronym | Description |
| ACT | Acceptance and Commitment Therapy |
| AI | Artificial Intelligence |
| BCA | Behavioral Change Applications |
| CBT | Cognitive Behavior Therapy |
| DBT | Dialectical Behavior Therapy |
| MBCT | Mindfulness-Based Cognitive Therapy |
| MBI | Mindfulness-Based Interventions |
| MBSR | Mindfulness-Based Stress Reduction |
| mHealth | Mobile Health |
| OAuth | Open Authorization |
| UI | User Interface |
| UX | User Experience |
References
- Phillips, E.A.; Himmler, S.; Schreyögg, J. Preferences of psychotherapists for blended care in Germany: A discrete choice experiment. BMC Psychiatry 2022, 22, 1–12. [Google Scholar] [CrossRef]
- Krebs, P.; Duncan, D.T. Health App Use Among US Mobile Phone Owners: A National Survey. JMIR Mhealth Uhealth 2015, 3, e101. [Google Scholar] [CrossRef]
- Torous, J.; Rodriguez, J.; Powell, A. The New Digital Divide For Digital Biomarkers. Digit. Psychiatry 2015, 2, 1–3. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Guideline 2020: Recommendations on Digital Interventions for Health System Strengthening. Available online: https://apps.who.int/iris/handle/10665/311941 (accessed on 27 April 2023).
- Singh, K.; Chandrasekaran, V.; Bhaumik, S.; Chandramouli, K. Mobile Health Apps for Self-management of COVID-19: A Scoping Review. J. Med. Syst. 2021, 45, 48. [Google Scholar] [CrossRef]
- Chandrashekar, P. Do Mental Health Mobile Apps Work: Evidence and Recommendations for Designing High-Efficacy Mental Health Mobile Apps. mHealth 2020, 6, 6. [Google Scholar] [CrossRef] [PubMed]
- Wac, K.; Tsiourti, C. The rise of mobile health. In Global Healthgrid; Wac, K., Ed.; Springer: Cham, Switzerland, 2014; pp. 3–20. [Google Scholar] [CrossRef]
- Steinhubl, S.R.; Muse, E.D.; Topol, E.J. The emerging field of mobile health. Sci. Transl. Med. 2015, 7, 283rv3. [Google Scholar] [CrossRef]
- Meskó, B.; Drobni, Z.; Bényei, É.; Gergely, B.; Győrffy, Z. Digital health is a cultural transformation of traditional healthcare. Mhealth 2017, 3, 38. [Google Scholar] [CrossRef]
- Laranjo, L.; Arguel, A.; Neves, A.; Gallagher, A.; Kaplan, R.; Mortimer, N.J.; Mendes, G.A.; Lau, A. The influence of social networking sites on health behavior change: A systematic review and meta-analysis. J. Am. Med. Inform. Assoc. 2015, 22, 243–256. [Google Scholar] [CrossRef]
- Free, C.; Phillips, G.; Watson, L.; Galli, L.; Felix, L.; Edwards, P.; Patel, V.; Haines, A. The effectiveness of mobile-health technologies to improve health care service delivery processes: A systematic review and meta-analysis. PLoS Med. 2013, 10, e1001363. [Google Scholar] [CrossRef]
- Pires, I.M.; Marques, G.; Garcia, N.M.; Flórez-Revuelta, F.; Ponciano, V.; Oniani, S. A research on the classification and applicability of the mobile health applications. J. Pers. Med. 2020, 10, 11. [Google Scholar] [CrossRef]
- Torous, J.; Andersson, G.; Bertagnoli, A.; Christensen, H.; Cuijpers, P.; Firth, J.; Haim, A.; Hsin, H.; Hollis, C.; Lewis, S.; et al. Towards a consensus around standards for smartphone apps and digital mental health. World Psychiatry Off. J. World Psychiatr. Assoc. (WPA) 2019, 18, 97–98. [Google Scholar] [CrossRef] [PubMed]
- Huckvale, K.; Nicholas, J.; Torous, J.; Larsen, M.E. Smartphone apps for the treatment of mental health conditions: Status and considerations. Curr. Opin. Psychol. 2020, 36, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Lui, J.H.L.; Marcus, D.K.; Barry, C.T. Evidence-based apps? A review of mental health mobile applications in a psychotherapy context. Prof. Psychol. Res. Pract. 2017, 48, 199–210. [Google Scholar] [CrossRef]
- Rathbone, A.L.; Clarry, L.; Prescott, J. Assessing the efficacy of mobile health apps using the basic principles of cognitive behavioral therapy: Systematic review. J. Med. Internet Res. 2017, 19, e399. [Google Scholar] [CrossRef] [PubMed]
- Linardon, J. Can acceptance, mindfulness, and self-compassion be learned by smartphone apps? A systematic and meta-analytic review of randomized controlled trials. Behav. Ther. 2019, in press. [Google Scholar] [CrossRef] [PubMed]
- Rizvi, S.L.; Dimeff, L.A.; Skutch, J.; Carroll, D.; Linehan, M.M. A pilot study of the DBT coach: An interactive mobile phone application for individuals with borderline personality disorder and substance use disorder. Behav. Ther. 2011, 42, 589–600. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, K.K.; Darcy, A.; Vierhile, M. Delivering cognitive behavior therapy to young adults with symptoms of depression and anxiety using a fully automated conversational agent (Woebot): A randomized controlled trial. JMIR Ment. Health 2017, 4, e19. [Google Scholar] [CrossRef] [PubMed]
- Diano, F.; Sica, L.S.; Ponticorvo, M. A Systematic Review of Mobile Apps as an Adjunct to Psychological Interventions for Emotion Dysregulation. Int. J. Environ. Res. Public Health 2023, 20, 1431. [Google Scholar] [CrossRef]
- Aldao, A.; Nolen-Hoeksema, S.; Schweizer, S. Emotion-regulation strategies across psychopathology: A meta-analytic review. Clin. Psychol. Rev. 2010, 30, 217–237. [Google Scholar] [CrossRef]
- Kring, A.M.; Sloan, D.M. (Eds.) Emotion Regulation and Psychopathology: A Transdiagnostic Approach to Etiology and Treatment; Guilford Press: New York, NY, USA, 2010. [Google Scholar]
- Rathbone, A.L.; Prescott, J. The use of mobile apps and SMS messaging as physical and mental health interventions: Systematic review. J. Med. Internet Res. 2017, 19, e295. [Google Scholar] [CrossRef]
- Torous, J.; Roberts, L.W. Needed innovation in digital health and smartphone applications for mental health: Transparency and trust validation. JAMA Psychiatry 2017, 74, 437–438. [Google Scholar] [CrossRef] [PubMed]
- Linehan, M.M. DBT Skills Training Manual, 2nd ed.; Guilford Publications: New York, NY, USA, 2014. [Google Scholar]
- Beck, J.S. Cognitive Behavior Therapy: Basics and Beyond, 2nd ed.; Guilford Press: New York, NY, USA, 2011. [Google Scholar]
- Firth, J.; Torous, J.; Nicholas, J.; Carney, R.; Pratap, A.; Rosenbaum, S.; Sarris, J. The efficacy of smartphone-based mental health interventions for depressive symptoms: A meta-analysis of randomized controlled trials. World Psychiatry 2017, 16, 287–298. [Google Scholar] [CrossRef]
- Schueller, S.M.; Neary, M.; O’ Loughlin, K.; Adkins, E.C. Discovery of and interest in health apps among those with mental health needs: Survey and focus group study. J. Med. Internet Res. 2018, 20, e10141. [Google Scholar] [CrossRef] [PubMed]
- Leahy, R.L. Cognitive Therapy Techniques: A Practitioner’s Guide; Guilford Publications: New York, NY, USA, 2017. [Google Scholar]
- Mak, W.W.; Tong, A.C.; Yip, S.Y.; Lui, W.W.; Chio, F.H.; Chan, A.T.; Wong, C.C. Efficacy and moderation of mobile app–based programs for mindfulness-based training, self-compassion training, and cognitive behavioral psychoeducation on mental health: Randomized controlled noninferiority trial. JMIR Ment. Health 2018, 5, e60. [Google Scholar] [CrossRef] [PubMed]
- Torous, J.; Levin, M.E.; Ahern, D.K.; Oser, M.L. Cognitive behavioral mobile applications: Clinical studies, marketplace overview, and research agenda. Cogn. Behav. Pract. 2017, 24, 215–225. [Google Scholar] [CrossRef]
- Torous, J.; Powell, A.C. Current research and trends in the use of smartphone applications for mood disorders. Internet Interv. 2015, 2, 169–173. [Google Scholar] [CrossRef]
- Kabat-Zinn, J.; Hanh, T.N. Full Catastrophe Living: Using the Wisdom of Your Body and Mind to Face Stress, Pain, and Illness; Random House Publishing Group: New York, NY, USA, 2009. [Google Scholar]
- Diano, F.; Ferrara, F.M.; Calabretta, R. The development of a mindfulness-based mobile application to learn emotional self-regulation. Psychobit 2019, 1. [Google Scholar]
- Shapiro, S.L.; Carlson, L.E.; Astin, J.A.; Freedman, B. Mechanisms of mindfulness. J. Clin. Psychol. 2006, 62, 373–386. [Google Scholar] [CrossRef]
- Hofmann, S.G.; Sawyer, A.T.; Witt, A.A.; Oh, D. The effect of mindfulness-based therapy on anxiety and depression: A meta-analytic review. J. Consult. Clin. Psychol. 2010, 78, 169. [Google Scholar] [CrossRef]
- van Emmerik, A.A.; Berings, F.; Lancee, J. Efficacy of a mindfulness-based mobile application: A randomized waiting-list controlled trial. Mindfulness 2018, 9, 187–198. [Google Scholar] [CrossRef]
- Khoury, B.; Sharma, M.; Rush, S.E.; Fournier, C. Mindfulness-based stress reduction for healthy individuals: A meta-analysis. J. Psychosom. Res. 2015, 78, 519–528. [Google Scholar] [CrossRef]
- van Emmerik, A.A.; Berings, F.; Lancee, J.; Eling, W.M. Mindfulness-based interventions for psychiatric disorders: A systematic review and meta-analysis. Clin. Psychol. Rev. 2019, 67, 117–131. [Google Scholar] [CrossRef]
- Dennis, M.J. Cultivating digital well-being and the rise of self-care Apps. In Ethics of Digital Well-Being; Springer: Cham, Switzerland, 2020; pp. 119–137. [Google Scholar]
- Riley, W.T.; Rivera, D.E.; Atienza, A.A.; Nilsen, W.; Allison, S.M.; Mermelstein, R. Health behavior models in the age of mobile interventions: Are our theories up to the task? Transl. Behav. Med. 2011, 1, 53–71. [Google Scholar] [CrossRef]
- Direito, A.; Carraça, E.; Rawstorn, J.; Whittaker, R.; Maddison, R. mHealth Technologies to Influence Physical Activity and Sedentary Behaviors: Behavior Change Techniques, Systematic Review and Meta-Analysis of Randomized Controlled Trials. Ann. Behav. Med. 2014, 49, 275–293. [Google Scholar] [CrossRef] [PubMed]
- Schoeppe, S.; Alley, S.; Van Lippevelde, W.; Bray, N.A.; Williams, S.L.; Duncan, M.J.; Vandelanotte, C. Efficacy of interventions that use apps to improve diet, physical activity and sedentary behaviour: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 127. [Google Scholar] [CrossRef]
- McKay, F.H.; Cheng, C.; Wright, A.; Shill, J.; Stephens, H.; Uccellini, M. Evaluating mobile phone applications for health behaviour change: A systematic review. J. Telemed. Telecare 2018, 24, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Orr, J.A.; King, R.J. Mobile phone SMS messages can enhance healthy behaviour: A meta-analysis of randomised controlled trials. Health Psychol. Rev. 2015, 9, 397–416. [Google Scholar] [CrossRef] [PubMed]
- Cuijpers, P.; Karyotaki, E.; Reijnders, M.; Huibers, M.J. Evidence-based psychotherapies for adult anxiety disorders: A meta-analysis of meta-analyses. J. Anxiety Disord. 2022, 84, 102474. [Google Scholar] [CrossRef]
- Strickland, E.L. An exploratory analysis of the smartphone application “kip”: mHealth progress monitoring and homework tracking as an adjunct to cognitive behavioral therapy treatment [ProQuest Information & Learning]. In Dissertation Abstracts International; Section B: The Sciences and Engineering; Ed. ProQuest: Ann Arbor, MI, USA, 2021; Volume 82, Issue 6-B. [Google Scholar]
- Faurholt-Jepsen, M.; Kessing, L.V. Apps for mental health care: The raise of digital psychiatry. Eur. Neuropsychopharmacol. 2021, 47, 51–53. [Google Scholar] [CrossRef] [PubMed]
- Kuhn, E.; McGee-Vincent, P. Using mobile apps in mental health practice. In Technology and Mental Health: A Clinician’s Guide to Improving Outcomes; Reger, G.M., Ed.; Routledge/Taylor & Francis Group: New York, NY, USA, 2021; pp. 56–74. [Google Scholar]
- Deady, M.; Johnston, D.A.; Glozier, N.; Milne, D.; Choi, I.; Mackinnon, A.; Mykletun, A.; Calvo, R.A.; Gayed, A.; Bryant, R.; et al. A smartphone application for treating depressive symptoms: Study protocol for a randomised controlled trial. BMC Psychiatry 2018, 18, 166. [Google Scholar] [CrossRef]
- Proudfoot, J.; Parker, G.; Hadzi Pavlovic, D.; Manicavasagar, V.; Adler, E.; Whitton, A. Community attitudes to the appropriation of mobile phones for monitoring and managing depression, anxiety, and stress. J. Med. Internet Res. 2010, 12, e64. [Google Scholar] [CrossRef]
- Torous, J.; Nicholas, J.; Larsen, M.E.; Firth, J.; Christensen, H. Clinical review of user engagement with mental health smartphone apps: Evidence, theory and improvements. Evid. Based Ment. Health 2018, 21, 116–119. [Google Scholar] [CrossRef] [PubMed]
- Fleming, T.; Bavin, L.; Lucassen, M.; Stasiak, K.; Hopkins, S.; Merry, S. Beyond the trial: Systematic review of real-world uptake and engagement with digital self-help interventions for depression, low mood, or anxiety. J. Med. Internet Res. 2018, 20, e199. [Google Scholar] [CrossRef]
- Bucci, S.; Schwannauer, M.; Berry, N. The digital revolution and its impact on mental health care. Psychol. Psychother. Theory Res. Pract. 2019, 92, 277–297. [Google Scholar] [CrossRef]
- Bakker, D.; Kazantzis, N.; Rickwood, D.; Rickard, N. Mental health smartphone apps: Review and evidence-based recommendations for future developments. JMIR Ment. Health 2016, 3, e7. [Google Scholar] [CrossRef] [PubMed]
- Larsen, M.E.; Huckvale, K.; Nicholas, J.; Torous, J.; Birrell, L.; Li, E.; Reda, B. Using science to sell apps: Evaluation of mental health app store quality claims. NPJ Digit. Med. 2019, 2, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Seitz, L. OAuth 2.0 Threat Landscape. IEEE Internet Comput. 2019, 23, 57–61. [Google Scholar]
- Hoffman, D. The Case for PKCE. IEEE Secur. Priv. 2020, 18, 96–101. [Google Scholar]
- Neary, M.; Schueller, S.M. State of the field of mental health apps. Cogn. Behav. Pract. 2018, 25, 531–537. [Google Scholar] [CrossRef]
- Karcher, N.R.; Presser, N.R. Ethical and legal issues addressing the use of mobile health (mHealth) as an adjunct to psychotherapy. Ethics Behav. 2018, 28, 1–22. [Google Scholar] [CrossRef]
- Borrelli, B.; Ritterband, L.M. Special issue on eHealth and mHealth: Challenges and future directions for assessment, treatment, and dissemination. Health Psychol. 2015, 34, 1205–1208. [Google Scholar] [CrossRef]
- Huckvale, K.; Torous, J.; Larsen, M.E. Assessment of the data sharing and privacy practices of smartphone apps for depression and smoking cessation. JAMA Netw. Open 2019, 2, e192542. [Google Scholar] [CrossRef] [PubMed]
- Robillard, J.; Illes, J.; Arcand, M.; Beattie, B.L.; Hayden, S.; Lawrence, P.; McGrenere, J.; Reiner, P.B.; Wittenberg, D.; Jacova, C. Scientific and ethical features of English-language online tests for Alzheimer’s disease. Alzheimer’s Dement. Diagn. Assess. Dis. Monit. 2018, 10, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Kiosses, D.N.; Monkovic, J.; Stern, A.; Czaja, S.J.; Alexopoulos, G.; Arslanoglou, E.; Ebo, T.; Pantelides, J.; Yu, H.; Dunefsky, J.; et al. An emotion regulation tablet app for middle-aged and older adults at high suicide risk: Feasibility, acceptability, and two case studies. Am. J. Geriatr. Psychiatry 2021, 30, 575–584. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Fagan, C.; Yu, C.L. Popular mental health apps (MH apps) as a complement to telepsychotherapy: Guidelines for consideration. J. Psychother. Integr. 2020, 30, 265. [Google Scholar] [CrossRef]
- Llorens-Vernet, P.; Miró, J. Standards for mobile health–related apps: Systematic review and development of a guide. JMIR Mhealth Uhealth 2020, 8, e13057. [Google Scholar] [CrossRef]
- Church, D.; Stapleton, P.; Sabot, D. App-based delivery of clinical Emotional Freedom Techniques: Cross-sectional study of app user self-ratings. JMIR Mhealth Uhealth 2020, 8, e18545. [Google Scholar] [CrossRef]
- Nicholas, J.; Larsen, M.E.; Proudfoot, J.; Christensen, H. Mobile apps for bipolar disorder: A systematic review of features and content quality. J. Med. Internet Res. 2015, 17, e198. [Google Scholar] [CrossRef]
- Proudfoot, J. The future is in our hands: The role of mobile phones in the prevention and management of mental disorders. Aust. New Zealand J. Psychiatry 2013, 47, 111–113. [Google Scholar] [CrossRef]
- Chan, S.; Torous, J.; Hinton, L.; Yellowlees, P. Towards a framework for evaluating mobile mental health apps. Telemed. E-Health 2015, 21, 1038–1041. [Google Scholar] [CrossRef]
- Deterding, S.; Dixon, D.; Khaled, R.; Nacke, L. From game design elements to gamefulness: Defining “gamification”. In Proceedings of the 15th International Academic MindTrek Conference: Envisioning Future Media Environments, Tampere, Finland, 28–30 September 2011; pp. 9–15. [Google Scholar]
- Nkambou, R.; Bourdeau, J.; Mizoguchi, R. Advances in Intelligent Tutoring Systems; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2010. [Google Scholar]
- Ponticorvo, M.; Rega, A.; Di Ferdinando, A.; Marocco, D.; Miglino, O. Approaches to Embed Bio-inspired Computational Algorithms in Educational and Serious Games. In CAID@ IJCAI; Ed. IJCAI: Melbourne, Australia, 2017; pp. 8–14. [Google Scholar]
- Ponticorvo, M.; Dell’Aquila, E.; Marocco, D.; Miglino, O. Situated psychological agents: A methodology for educational games. Appl. Sci. 2019, 9, 4887. [Google Scholar] [CrossRef]
- Wehmann, E.; Köhnen, M.; Härter, M.; Liebherz, S. Therapeutic alliance in technology-based interventions for the treatment of depression: Systematic review. J. Med. Internet Res. 2020, 22, e17195. [Google Scholar] [CrossRef]
- Bordin, E.S. The generalizability of the psychoanalytic concept of the working alliance. Psychother. Theory Res. Pract. 1979, 16, 252–260. [Google Scholar] [CrossRef]
- Sedgwick, O.; Hardy, A.; Greer, B.; Newbery, K.; Cella, M. ‘I wanted to do more of the homework!’—Feasibility and acceptability of blending app-based homework with group therapy for social cognition in psychosis. J. Clin. Psychol. 2021, 77, 2701–2724. [Google Scholar] [CrossRef] [PubMed]
- Ebert, D.D.; Van Daele, T.; Nordgreen, T.; Karekla, M.; Compare, A.; Zarbo, C.; Brugnera, A.; Øverland, S.; Trebbi, G.; Jensen, K.L.; et al. Internet- and mobile-based psychological interventions: Applications, efficacy, and potential for improving mental health: A report of the EFPA E-Health Taskforce. Eur. Psychol. 2018, 23, 167–187. [Google Scholar] [CrossRef]
- Bennett, C.B.; Ruggero, C.J.; Sever, A.C.; Yanouri, L. eHealth to redress psychotherapy access barriers both new and old: A review of reviews and meta-analyses. J. Psychother. Integr. 2020, 30, 188–207. [Google Scholar] [CrossRef]
- Kauer, S.; Reid, S.C. Mobile therapy: An overview of mobile device-assisted psychological therapy and prevention of mental health problems. In Mental Health in the Digital Age: Grave Dangers, Great Promise; Aboujaoude, E., Starcevic, V., Eds.; Oxford University Press: Oxford, UK, 2015; pp. 238–256. [Google Scholar] [CrossRef]
- Lindhiem, O.; Bennett, C.B.; Rosen, D.; Silk, J. Mobile technology boosts the effectiveness of psychotherapy and behavioral interventions: A meta-analysis. Behav. Modif. 2015, 39, 785–804. [Google Scholar] [CrossRef]
- Price, M.; Yuen, E.K.; Goetter, E.M.; Herbert, J.D.; Forman, E.M.; Acierno, R.; Ruggiero, K.J. mHealth: A mechanism to deliver more accessible, more effective mental health care. Clin. Psychol. Psychother. 2014, 21, 427–436. [Google Scholar] [CrossRef] [PubMed]
- Hayes, S.C.; Strosahl, K.D.; Wilson, K.G. Acceptance and Commitment Therapy; Guilford Press: New York, NY, USA, 1999; p. 6. [Google Scholar]
- Linehan, M.M. Skills Training Manual for Treating Borderline Personality Disorder; Guilford press: New York, NY, USA, 1993. [Google Scholar]
- Jacob, C.; Sanchez-Vazquez, A.; Ivory, C. Social, organizational, and technological factors impacting clinicians’ adoption of mobile health tools: Systematic literature review. JMIR Mhealth Uhealth 2020, 8, e15935. [Google Scholar] [CrossRef]
- Mohr, D.; Lyon, A.; Lattie, E.; Reddy, M.; Schueller, S. Accelerating Digital Mental Health Research From Early Design and Creation to Successful Implementation and Sustainment. J. Med. Internet Res. 2017, 19, e153. [Google Scholar] [CrossRef]
- ISO 9241-210:2019; Ergonomics of Human-System Interaction—Part 210: Human-Centred Design for Interactive Systems. International Organization for Standardization: Geneva, Switzerland, 2019.
- Nielsen, J. Usability Engineering; Morgan Kaufmann Publishers Inc.: Cambridge, MA, USA, 1993. [Google Scholar]
- Hollis, C.; Falconer, C.J.; Martin, J.L.; Whittington, C.; Stockton, S.; Glazebrook, C.; Davies, E.B. Annual Research Review: Digital health interventions for children and young people with mental health problems - a systematic and meta-review. J. Child Psychol. Psychiatry 2017, 58, 474–503. [Google Scholar] [CrossRef]
- Stawarz, K.; Preist, C.; Tallon, D.; Wiles, N.; Coyle, D. User Experience of Cognitive Behavioral Therapy Apps for Depression: An Analysis of App Functionality and User Reviews. J. Med. Int. Res. 2018, 20, e10120. [Google Scholar] [CrossRef]
- Cugelman, B. Gamification: What it is and why it matters to digital health behavior change developers. JMIR Serious Games 2013, 1, e3. [Google Scholar] [CrossRef]
- Hinyard, L.J.; Kreuter, M.W. Using narrative communication as a tool for health behavior change: A conceptual, theoretical, and empirical overview. Health Educ. Behav. 2007, 34, 777–792. [Google Scholar] [CrossRef]
- Stubbs, B.; Vancampfort, D.; Hallgren, M.; Firth, J.; Veronese, N.; Solmi, M.; Brand, S.; Cordes, J.; Malchow, B.; Gerber, M.; et al. EPA guidance on physical activity as a treatment for severe mental illness: A meta-review of the evidence and Position Statement from the European Psychiatric Association (EPA), supported by the International Organization of Physical Therapists in Mental Health (IOPTMH). Eur. Psychiatry 2018, 54, 124–144. [Google Scholar] [PubMed]
- Litvin, S.; Saunders, R.; Maier, M.; Lüttke, S. Gamification as an Approach to Improve Resilience and Reduce Attrition in Mobile Mental Health Interventions: A Randomized Controlled Trial. PLoS ONE 2021, 16, e0244400. [Google Scholar] [CrossRef] [PubMed]
- Gross, J.J. Emotion regulation: Affective, cognitive, and social consequences. Psychophysiology 2002, 39, 281–291. [Google Scholar] [CrossRef] [PubMed]
- Barlow, D.; Farchione, T.; Bullis, J.; Gallagher, M.; Murray-Latin, H.; Sauer-Zavala, S.; Bentley, K.; Thompson-Hollands, J.; Conklin, L.R.; Boswell, J.F.; et al. The unified protocol for transdiagnostic treatment of emotional disorders compared with diagnosis-specific protocols for anxiety disorders: A randomized clinical trial. JAMA Psychiatry 2017, 74, 875–884. [Google Scholar] [CrossRef]
- Folkman, S.; Lazarus, R.S.; Dunkel-Schetter, C.; DeLongis, A.; Gruen, R.J. Dynamics of a stressful encounter: Cognitive appraisal, coping, and encounter outcomes. J. Personal. Soc. Psychol. 1986, 50, 992. [Google Scholar] [CrossRef]
- Goldin, P.R.; Gross, J.J. Effects of mindfulness-based stress reduction (MBSR) on emotion regulation in social anxiety disorder. Emotion 2010, 10, 83. [Google Scholar] [CrossRef] [PubMed]
- Cole, P.M.; Hall, S.E. Emotion Dysregulation as a Risk Factor for Psychopathology. Wiley & Sons: Hoboken, NJ, USA, 2008. [Google Scholar]
- Sheppes, G.; Suri, G.; Gross, J.J. Emotion regulation and psychopathology. Annu. Rev. Clin. Psychol. 2015, 11, 379–405. [Google Scholar] [CrossRef] [PubMed]
- Beauchaine, T.P.; Cicchetti, D. Emotion dysregulation and emerging psychopathology: A transdiagnostic, transdisciplinary perspective. Dev. Psychopathol. 2019, 31, 799–804. [Google Scholar] [CrossRef] [PubMed]
- Farchione, T.; Fairholme, C.; Ellard, K.; Boisseau, C.L.; Thompson-Hollands, J.; Carl, J.; Gallagher, M.; Barlow, D. Unified protocol for transdiagnostic treatment of emotional disorders: A randomized controlled trial. Behav. Ther. 2012, 43, 666–678. [Google Scholar] [CrossRef] [PubMed]
- McRae, K.; Gross, J.J. Emotion regulation. Emotion 2020, 20, 1. [Google Scholar] [CrossRef]
- Gross, J.J. Emotion regulation: Current status and future prospects. Psychol. Inq. 2015, 26, 1–26. [Google Scholar] [CrossRef]
- Bridges, L.J.; Denham, S.A.; Ganiban, J.M. Definitional issues in emotion regulation research. Child Dev. 2004, 75, 340–345. [Google Scholar] [CrossRef]
- Hu, T.; Zhang, D.; Wang, J.; Mistry, R.; Ran, G.; Wang, X. Relation between emotion regulation and mental health: A meta-analysis review. Psychol. Rep. 2014, 114, 341–362. [Google Scholar] [CrossRef]
- Marroquín, B.; Tennen, H.; Stanton, A.L. Coping, emotion regulation, and well-being: Intrapersonal and interpersonal processes. In The Happy Mind: Cognitive Contributions to Well-Being; Springer: New York, NY, USA, 2017; pp. 253–274. [Google Scholar]
- Cludius, B.; Mennin, D.; Ehring, T. Emotion regulation as a transdiagnostic process. Emotion 2020, 20, 37. [Google Scholar] [CrossRef] [PubMed]
- Gross, J.J.; Jazaieri, H. Emotion, emotion regulation, and psychopathology: An affective science perspective. Clin. Psychol. Sci. 2014, 2, 387–401. [Google Scholar] [CrossRef]
- Wang, K.; Varma, D.S.; Prosperi, M. A systematic review of the effectiveness of mobile apps for monitoring and management of mental health symptoms or disorders. J. Psychiatr. Res. 2018, 107, 73–78. [Google Scholar] [CrossRef]
- Jones, N.; Moffitt, M. Ethical guidelines for mobile app development within health and mental health fields. Prof. Psychol. Res. Pract. 2016, 47, 155. [Google Scholar] [CrossRef]
- Rathus, J.H.; Miller, A.L. DBT Skills Manual for Adolescents; Guilford press: New York, NY, USA, 2014. [Google Scholar]
- Alomari, H.W.; Ramasamy, V.; Kiper, J.D.; Potvin, G. A User Interface (UI) and User eXperience (UX) evaluation framework for cyberlearning environments in computer science and software engineering education. Heliyon 2020, 6, e03917. [Google Scholar] [CrossRef]
- Alqahtani, F.; Orji, R. Insights from user reviews to improve mental health apps. Health Inform. J. 2020, 26, 2042–2066. [Google Scholar] [CrossRef]
- Lemon, C.; Huckvale, K.; Carswell, K.; Torous, J. A narrative review of methods for applying user experience in the design and assessment of mental health smartphone interventions. Int. J. Technol. Assess. Health Care 2020, 36, 64–70. [Google Scholar] [CrossRef]
- Smith, A.C.; Fowler, L.A.; Graham, A.K.; Jaworski, B.K.; Firebaugh, M.-L.; Monterubio, G.E.; Vázquez, M.M.; DePietro, B.; Sadeh-Sharvit, S.; Balantekin, K.; et al. Digital overload among college students: Implications for mental health app use. Soc. Sci. 2021, 10, 279. [Google Scholar] [CrossRef]
- Elhai, J.D.; Dvorak, R.D.; Levine, J.C.; Hall, B.J. Problematic smartphone use: A conceptual overview and systematic review of relations with anxiety and depression psychopathology. J. Affect. Disord. 2017, 207, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Kushlev, K.; Dunn, E.W. Checking email less frequently reduces stress. Comput. Hum. Behav. 2015, 43, 220–228. [Google Scholar] [CrossRef]
- Terry, N.P.; Gunter, T.D. Regulating mobile mental health apps. Behav. Sci. Law 2018, 36, 136–144. [Google Scholar] [CrossRef]
- Sharon, T. Self-tracking for health and the quantified self: Re-articulating autonomy, solidarity, and authenticity in an age of personalized healthcare. Philos. Technol. 2017, 30, 93–121. [Google Scholar] [CrossRef]
- Henson, P.; Wisniewski, H.; Hollis, C.; Keshavan, M.; Torous, J. Digital mental health apps and the therapeutic alliance: Initial review. BJPsych Open 2019, 5, e15. [Google Scholar] [CrossRef] [PubMed]
- Tremain, H.; McEnery, C.; Fletcher, K.; Murray, G. The therapeutic alliance in digital mental health interventions for serious mental illnesses: Narrative review. JMIR Ment. Health 2020, 7, e17204. [Google Scholar] [CrossRef] [PubMed]
- Flutter. Available online: https://flutter.dev (accessed on 26 April 2023).
- Wadhwa, B.; Verma, A.K. Flutter & Firebase: An enhanced mobile application development. Int. J. Adv. Sci. Technol. 2020, 29, 3815–3821. [Google Scholar]
- Firebase. Available online: https://firebase.google.com (accessed on 26 April 2023).
- Fowler, M. Firebase: The new mobile app development platform. J. Mob. Technol. Med. 2016, 5, 43–45. [Google Scholar]



{kind=link}
{kind=link}
| Opportunities | Challenges |
|---|---|
| Improved accessibility to mental health resources | Privacy and data security concerns |
| Cost-effective interventions for mental health | Limited access to smartphones or the internet for some populations |
| Personalized care through data-driven insights | Reinforcement of therapeutic approaches (e.g., DBT, CBT) |
| Reduction of the stigma associated with seeking help | Lack of user engagement or sustained usage |
| Promotion of self-monitoring and self-awareness | Difficulty in navigating the vast number of available apps |
| Facilitation of peer support and social networking | Regulatory and ethical concerns |
| Design Element | Description |
|---|---|
| User interface (UI) and user experience (UX) | Simple layout for easy navigation and reduced anxiety. UI refers to visual and interactive elements, while UX focuses on user satisfaction and ease of use. |
| Notifications | Properly managed notifications to avoid information overload, interruptions, or addiction. Customization options for frequency and content are necessary. |
| Progress charts | Use tracking charts with caution to avoid stress, anxiety, or distortion of users’ perceptions. Consider showing charts to therapists instead of users directly. Be aware of potential negative effects, such as addiction, oversimplification of emotions, or plateau effects. Offer the option to enable or disable progress charts for the user. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Diano, F.; Sica, L.S.; Ponticorvo, M. Empower Psychotherapy with mHealth Apps: The Design of “Safer”, an Emotion Regulation Application. Information 2023, 14, 308. https://doi.org/10.3390/info14060308
Diano F, Sica LS, Ponticorvo M. Empower Psychotherapy with mHealth Apps: The Design of “Safer”, an Emotion Regulation Application. Information. 2023; 14(6):308. https://doi.org/10.3390/info14060308
Chicago/Turabian StyleDiano, Federico, Luigia Simona Sica, and Michela Ponticorvo. 2023. "Empower Psychotherapy with mHealth Apps: The Design of “Safer”, an Emotion Regulation Application" Information 14, no. 6: 308. https://doi.org/10.3390/info14060308
APA StyleDiano, F., Sica, L. S., & Ponticorvo, M. (2023). Empower Psychotherapy with mHealth Apps: The Design of “Safer”, an Emotion Regulation Application. Information, 14(6), 308. https://doi.org/10.3390/info14060308